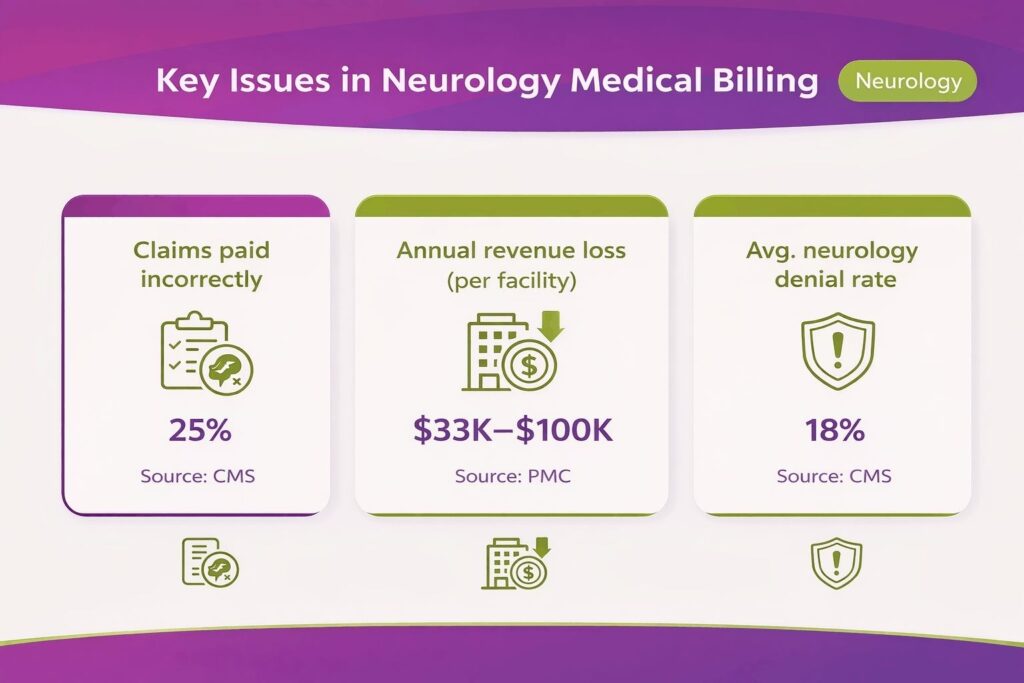
Neurology practices in the U.S. perform complex and high-volume procedures, including EEGs, EMGs, and nerve conduction studies. Accurate coding for these procedures is critical for timely claim submission. According to the Centers for Medicare & Medicaid Services (CMS), 25% Neurology claims are paid incorrectly due to documentation, coding, or wrong modifiers.
Inaccuracies in Neurology billing have a significant financial impact on providers. According to PMC, documentation and coding errors in Neurology practices can cause annual revenue losses of $33,000–$100,000 per medium-sized facility.
With growing patient volumes and strict payer requirements, Neurology billing requires attention at every step. This is why many providers are turning to specialized Neurology billing services to streamline payments and reduce costly errors.
This guide explains the Neurology billing process step by step, outlines common billing challenges, and provides updated CPT and ICD-10-CM code cheat sheets for 2026. We will also share practical tips and provide extensive guidelines to help your practice minimize write‑offs.
What Makes Neurology Billing Different From Other Specialties
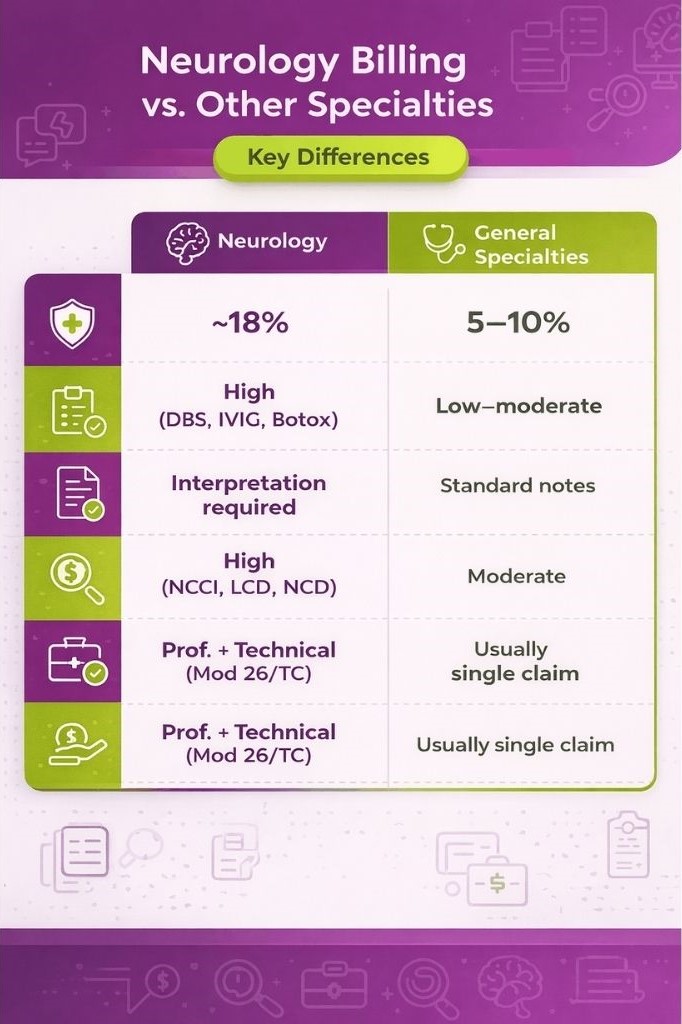
Neurology billing is more detailed than many other medical specialties because it involves complex testing, ongoing patient care, and closer insurance review. Conditions are often long-term, and diagnostic tests require careful reporting, which makes accurate documentation and coding essential for every claim.
High Procedure Complexity and Documentation Burden
Neurology includes several specialized diagnostic tests that require detailed interpretation, not just procedure coding. Tests like electroencephalogram (EEG), electromyography (EMG), and nerve conduction study (NCS) must always include a written interpretation report. Without this report, payers may deny the claim even if the test was performed.
Neurologists also treat long-term conditions such as multiple sclerosis, epilepsy, and Parkinson’s disease. These conditions require repeated visits and updated clinical notes at each encounter. Even if the diagnosis is already known, each visit must clearly show why the care or testing is still needed. This is known as medical necessity documentation.
Because care continues over time and involves repeated testing and monitoring, Neurology billing depends heavily on consistent and complete documentation at every step.
Stricter Payer Scrutiny Compared to Other Specialties
Neurology claims are reviewed more closely by insurance companies because many services involve high-cost procedures and long-term treatment plans. Payers such as Medicare, Medicaid, and commercial payers like UnitedHealthcare often apply stricter rules before approving or paying claims.
Some procedures, such as deep brain stimulation (DBS), chemodenervation (Botox for chronic migraine), and lumbar puncture, usually require prior authorization before the service is done. Neurology claims are also frequently checked under NCCI edits, which help ensure correct coding and prevent billing mistakes. Small errors in coding or missing approvals can lead to denials.
As a result, Neurology tends to have a higher denial rate, around 18%, compared to the average 5–10% seen in many other specialties. This makes payer rules and approvals especially important in Neurology billing.
Volume and Billing Environment (Private Practice vs. Hospital Setting)
Neurology billing also depends on where the service is provided, as billing rules change between private clinics and hospitals. In private practice, billing is usually handled under professional billing (PB). The neurologist or clinic submits the full claim directly to insurance for both evaluation and treatment services.
Whereas, in hospital settings, billing is often split between the hospital and the physician. The hospital handles the facility or technical part of the service, while the neurologist bills for the professional work. This is known as hospital billing (HB).
Because of this split, billing may use specific modifiers such as Modifier 26 for the professional portion and Modifier TC for the technical portion. The place of service code also becomes important because it tells the payer where the service was performed.
A Comprehensive Neurology Billing and Coding Workflow
Neurology billing requires precise coding and proper documentation. High-volume procedures, chronic patient management, and payer-specific requirements make accurate billing essential to avoid revenue loss. We have enlisted the steps in the Neurology medical billing process to help your practice maximize reimbursements.
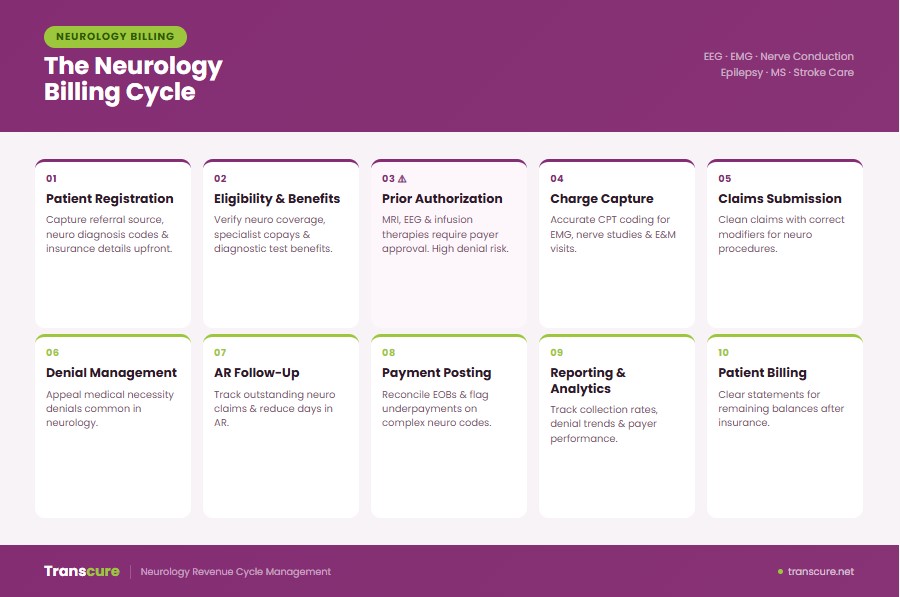
Step 1: Patient Registration and Insurance Intake
Neurology billing begins at patient registration, not at the claim submission stage. This is one of the most error-prone points in the entire revenue cycle because incomplete or incorrect intake data directly leads to claim denials later.
What Information Must Be Captured at Registration
Accurate intake ensures that the claim can move through insurance verification and payment without avoidable interruptions. At registration, the following information must be captured:
- Primary insurance and secondary insurance
- Coordination of benefits (COB) details when multiple insurers are involved
- Insurance plan type, such as HMO, PPO, or managed care plan
- Complete patient demographics (name, date of birth, address, contact details)
- Referring to the provider details, including the NPI (National Provider Identifier)
- Referral source when required by the payer
- Completed the intake form with all required administrative fields
In Neurology billing, scheduling teams must also identify services that may require prior approval. Procedures or diagnostic tests should be flagged early so authorization can be started before the visit. This is especially important for high-cost or high-review services commonly seen in Neurology practices.
How Incomplete Intake Creates Downstream Billing Failures
Errors at registration do not stay isolated; they create a chain reaction that affects the entire billing cycle. According to insights from AHIMA (American Health Information Management Association), a large portion of claim issues originates at the front end of the revenue cycle. In many cases, about 60% of returned claims are never resubmitted, resulting in permanent revenue leakage and lowering the overall clean claim rate.
Most of these problems are not caused by coding mistakes but by administrative errors made before the claim is even created.
Digital Intake Tools and EHR Integration in Neurology
To reduce intake errors, many Neurology practices use digital systems that connect registration directly to billing workflows. Modern Neurology EHR systems, such as AdvancedMD and PlusNeuro, help automate intake validation. These systems are often connected to a practice management system, keeping clinical and billing data aligned.
Automated eligibility verification ensures that insurance coverage issues are identified early, helping prevent avoidable claim denials and improving overall billing accuracy in Neurology workflows.
Step 2: Insurance Eligibility Verification
Insurance eligibility verification is a separate step from prior authorization, although the two are often confused in day-to-day Neurology billing workflows. Eligibility verification confirms whether the patient’s insurance is active and what benefits are available at the time of service. Prior authorization, in contrast, determines whether a specific procedure or service is approved in advance. When eligibility checks are skipped, claims can be denied even if prior authorization has already been obtained.
What to Verify Before Every Neurology Appointment
Before every Neurology appointment, eligibility verification ensures that the visit and related services will be reimbursed correctly. It is important to confirm whether the patient has active coverage and whether the provider is considered an in-network provider or out-of-network under the plan. The patient’s deductible, including how much has been met or remains, should be checked along with applicable copay and coinsurance amounts for both office visits and procedures.
It is also necessary to confirm any coverage limits that apply specifically to Neurology services, especially diagnostic testing or repeated evaluations. For HMO plans, HMO referral requirements must be verified before the visit to avoid non-payment. In addition, plan-specific exclusions should be reviewed through plan benefits verification to ensure the scheduled service is not restricted.
When to Re-Verify Eligibility for Chronic Neurology Patients
Eligibility cannot be treated as a one-time check in Neurology because patients with chronic conditions often stay under care for long periods. Patients with conditions such as Parkinson’s disease and multiple sclerosis, which fall under chronic disease management, are particularly likely to experience insurance changes during treatment. This includes switching employers, changing plans, or experiencing a temporary loss of coverage.
For this reason, eligibility should be re-verified at every visit for active patients. It should also be checked 48 to 72 hours before any scheduled procedure to confirm coverage is still valid. Failure to do so can result in an insurance lapse or a coverage gap, which often leads to denied claims in recurring patient billing scenarios.
Common Eligibility Errors That Cause Claim Denials
Many claim denials in Neurology billing occur due to eligibility errors that could have been prevented at the front end. One common issue is policy termination not being identified before the visit, which results in a direct claim rejection once the service is billed.
Another frequent problem is incorrect or outdated subscriber ID information, which leads to an eligibility mismatch during payer verification. Errors in the coordination of benefits, especially when primary and secondary insurance are reversed, also cause claims to fail during processing.
In some cases, services are billed without confirming whether they are excluded under the patient’s plan. These issues are often identified too late unless real-time eligibility (RTE) verification is used consistently at the point of scheduling and check-in.
Step 3: Prior Authorization in Neurology
Prior authorization is one of the most critical and high-friction parts of Neurology billing. Many Neurology services cannot be performed or reimbursed without payer approval, making this step essential for revenue protection and avoiding preventable denials.
Which Neurology Services Require Prior Authorization in 2026
In Neurology, prior authorization is most commonly required for high-cost or high-complexity services. Advanced imaging, such as CT angiography and MRI (especially MRI with contrast), typically requires approval before scheduling.
Interventional procedures like deep brain stimulation, spinal cord stimulator implantation, and diagnostic procedures such as lumbar puncture often require authorization due to strict payer medical necessity review.
Infusion-based therapies are also heavily regulated. Treatments such as natalizumab, ocrelizumab, intravenous immunoglobulin (IVIG), and other infusion therapy protocols usually require prior approval with documentation of prior treatment failure or disease progression.
Even Botox/onabotulinumtoxinA for chronic migraine requires authorization in most cases, often with frequency limits that trigger re-authorization rules. Missing these limits is a common cause of denial.
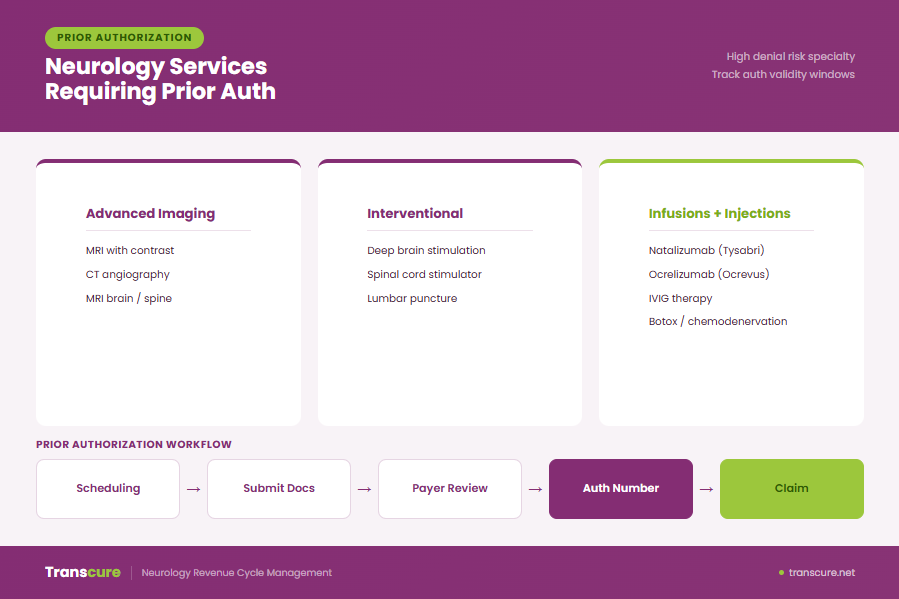
The Prior Authorization Workflow
The workflow begins at scheduling, where staff identify whether prior authorization is required based on payer rules. Clinical staff then submit clinical documentation and diagnosis details through the payer portal, supported by medical records.
Payers evaluate requests using medical necessity criteria and local coverage determination (LCD) guidelines. If approved, an authorization number is issued.
This authorization number must be attached to the claim during billing. Without it, the claim will typically be denied even if the service is medically appropriate. Ownership is shared: scheduling identifies need, clinical staff submits documentation, and billing ensures correct claim submission.
What Happens When Prior Auth Expires Before the Procedure
Each authorization has a defined validity window set by the payer timeline. If the procedure is delayed beyond this period, the authorization expiration leads to automatic claim denial.
This is a common hidden revenue loss point in Neurology billing. To prevent it, teams must actively track expiration dates and request re-authorization before the window closes when delays occur.
How to Reduce Prior Authorization Denials Operationally
Reduction starts with standardizing authorization templates that include payer-aligned clinical language. Integrating LCD (Local Coverage Determination) and NCD (National Coverage Determination) criteria into documentation improves approval rates.
Tracking authorization turnaround times by payer helps predict delays and schedule more accurately. When denials occur, peer-to-peer review is often the most effective escalation path.
A centralized authorization tracking dashboard ensures visibility of all pending, approved, and expiring authorizations, reducing missed approvals and improving revenue consistency.
Step 4: Charge Capture Workflow
In a typical Neurology workflow, charge capture begins with provider documentation during the patient encounter. The provider records the clinical note, which includes the services performed, assessments, and treatment decisions. These clinical notes then act as the foundation for identifying billable services through charge capture triggers.
How Charges Are Captured in Neurology Practices
The coding team reviews the documentation and translates the encounter into billable items, which are then prepared for submission. These charges are entered into the practice management system, where they are eventually converted into claims for payer submission. In many modern setups, the EHR is integrated with billing systems so that documentation flows directly into charge creation with fewer manual steps.
Some practices still use paper-based encounter forms or superbills, where providers manually mark services performed. This approach increases the risk of errors and delays. In contrast, EHR-integrated workflows significantly reduce charge lag.
Common Charge Capture Failures in Neurology
Charge capture errors are a major source of revenue leakage in Neurology practices. One of the most common issues is undercoding, where services provided are not fully captured or billed correctly, resulting in lost revenue.
Another frequent problem is incorrect or missing documentation for time-based billing, where the time spent on patient care is not clearly recorded, making the service non-billable or reduced in value. Missing interpretation reports, especially for procedures like EEG or EMG, can also prevent billing entirely because the service is not considered complete without documented interpretation.
How to Audit Your Charge Capture Process
Auditing charge capture is essential to ensure that all services provided are being billed correctly and on time. One of the most effective methods is running a monthly charge lag report, which measures the time between the date of service and when the charge is entered into the billing system. Longer delays often indicate workflow issues.
On a broader level, practices should perform quarterly reconciliation between procedure logs and billing records to ensure all services performed are reflected in the claims submitted. Regular billing audit processes help identify patterns of missed or delayed charges, improve workflow efficiency, and reduce long-term revenue loss in Neurology billing systems.
Step 5: Claims Submission
Claims submission is the stage where all prior steps come together into a finalized claim sent to the payer. In Neurology billing, the focus is not just submitting claims, but ensuring they are “clean” the first time so they pass payer systems without correction, delay, or rejection.
What Makes a Clean Neurology Claim
A clean claim is one that can be processed by the payer without any manual intervention or request for additional information. For Neurology billing, a clean CMS-1500 form (or UB-04 (hospital) when applicable) must include correct patient demographics, valid insurance details, and accurate provider identifiers such as NPI for both the individual neurologist and the group practice. The place of service (POS) code must accurately reflect where the service was performed, as this directly impacts reimbursement.
The claim must also include a correct diagnosis-to-procedure linkage, ensuring the clinical reason supports the service billed. Any required authorization number must be present and valid. Modifier usage must align with payer rules, and all supporting documentation should be available if requested.
Electronic vs. Paper Claims Submission in Neurology
Most Neurology practices now rely on electronic claim submission using EDI (Electronic Data Interchange) systems. Over 95% of Neurology claims are submitted electronically because this method is faster, more accurate, and less prone to manual errors.
Paper claims are still used in limited cases but typically take 2–3 times longer to process and have significantly higher rejection rates. The clearinghouse performs claim scrubbing, which identifies formatting errors, missing fields, or invalid data before submission. The most common electronic format used is the 837P transaction, which standardizes professional claims for payer systems.
How to Increase First-Pass Acceptance Rate
The first-pass acceptance rate measures how many claims are accepted and processed by the payer without needing correction. Improving this rate depends heavily on pre-submission validation. Claim scrubbing tools identify issues such as demographic mismatches, incorrect NPI entries, or modifier conflicts before claims are sent. Many practices also use a payer rules engine inside their practice management system to enforce payer-specific requirements automatically.
It is also important to distinguish between rejection vs. denial. Rejections occur before processing due to errors, while denials occur after processing due to coverage or policy issues.
Payer-Specific Submission Rules Neurology Practices Must Follow
Different payers apply different submission rules, and Neurology practices must follow them carefully to avoid delays. For example, Medicare typically enforces a 12-month timely filing limit, while many commercial payers may have limits ranging from 90 to 180 days.
Some payers require additional documentation or paper attachments for neurodiagnostic services, especially for complex testing. Understanding each payer’s timely filing limit, claim attachment rules, and payer portal requirements is essential for reducing submission errors.
Step 6: Denial Management
Denial management is one of the most financially important parts of Neurology billing. Many Neurology practices lose revenue here, not because services are not payable, but because denied claims are not properly followed up, corrected, and appealed. A structured denial workflow is essential to prevent silent revenue leakage.
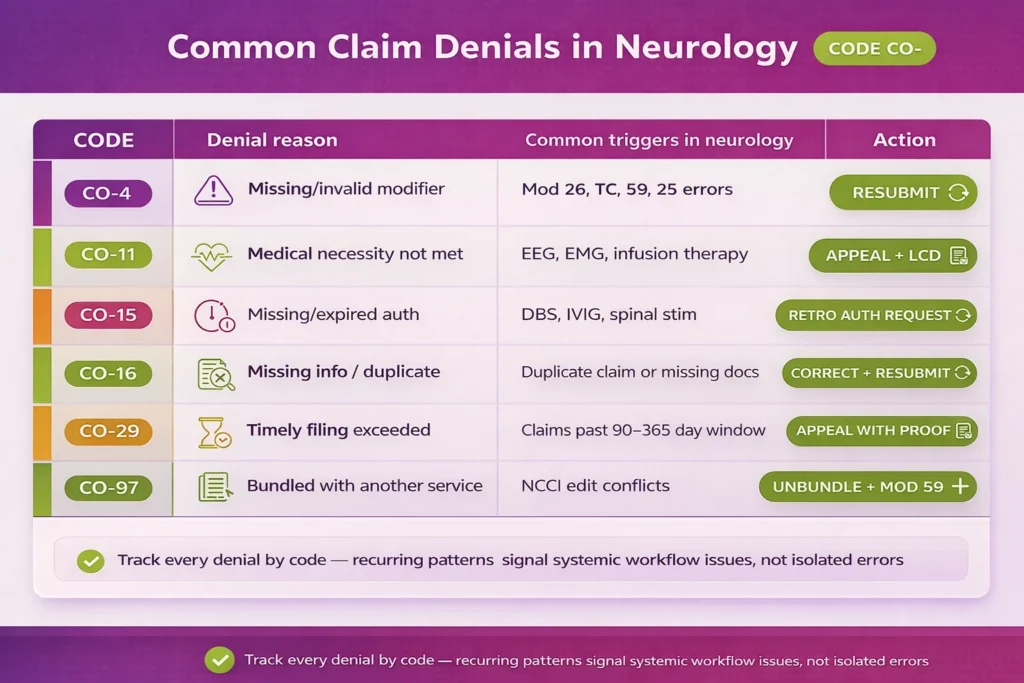
Most Common Denial Reasons in Neurology Billing
Neurology denials usually fall into predictable categories, often linked to specific procedures or documentation gaps. One of the most common issues is missing or expired prior authorization, especially for interventional procedures where approval is required before service delivery. These are typically categorized under CO-4 or CO-15 denial reason codes.
Another frequent issue is insufficient medical necessity denial, particularly for services like electroencephalogram (EEG), electromyography (EMG), and infusion therapy. These often appear as CO-11 or CO-16 denials, depending on payer classification.
Other common denial types include timely filing denial, where claims are submitted after the payer deadline, duplicate claim submissions under CO-16, and incorrect or missing modifiers. Some claims are denied simply because the service is considered a non-covered service under the patient’s plan.
How to Build a Denial Tracking Workflow
Effective denial management starts with structured tracking. Every denial should be recorded in a denial log that captures the denial reason code, payer name, procedure involved, and provider responsible for the service. This allows practices to identify recurring issues instead of treating each denial as an isolated event.
A denial management dashboard should be reviewed weekly to monitor trends and identify high-risk patterns. Denials must also be categorized based on responsibility, such as administrative denials and clinical denials.
The Neurology Claims Appeal Process: Step by Step
When a claim is denied, a structured appeal process improves the chance of recovery. The first step is identifying the exact denial reason code and understanding why the payer rejected the claim. Next, supporting documentation must be collected, including clinical notes, prior authorization records, and applicable LCD criteria when relevant.
An appeal letter is then prepared using payer-specific language that directly addresses the reason for denial. In cases involving clinical judgment, a peer-to-peer review may be required between the neurologist and the payer’s medical reviewer.
The appeal must be submitted within the defined appeal deadline, and the outcome should be tracked until resolution. In Medicare cases, this process may escalate through redetermination (Medicare), followed by reconsideration, and eventually an external appeal if necessary.
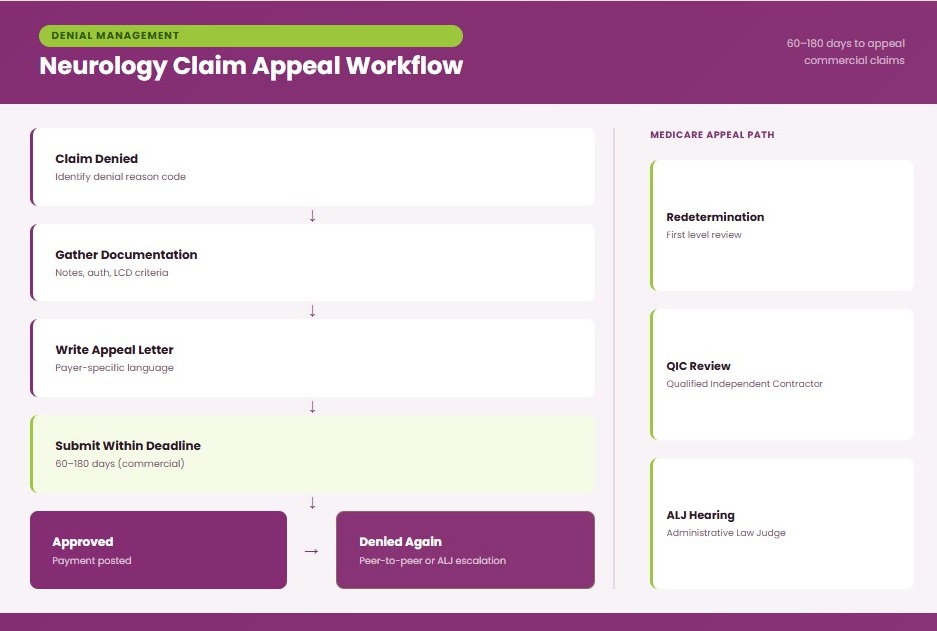
Payer Appeal Timelines and Deadlines Neurology Practices Must Know
Appeal timelines vary significantly by payer, and missing these deadlines is one of the most common reasons appeals fail in Neurology billing. For Medicare, the process follows a structured multi-level system that includes redetermination, review by a Qualified Independent Contractor (QIC), and potentially escalation to an Administrative Law Judge (ALJ) hearing.
Commercial payers such as Aetna, Cigna, and UnitedHealthcare typically allow appeal submission windows ranging from 60 to 180 days after the denial date, depending on plan rules. Failure to meet these appeal deadlines results in automatic loss of reimbursement rights, even if the claim was otherwise valid.
Step 7: Accounts Receivable (AR) Management
Accounts Receivable (AR) management is where Neurology billing performance becomes financially visible. Even if claims are submitted correctly and initially paid, poor AR follow-up leads to delayed or lost revenue. Key performance indicator in Neurology billing is Days in AR, which measures how long it takes for a claim to be paid after being submitted. For Neurology practices, a healthy benchmark is typically under 35 days.
Another important metric is AR aging, which categorizes unpaid claims based on how long they have been outstanding. These categories are known as AR aging buckets, commonly divided into 0–30 days, 31–60 days, 61–90 days, and 90+ days.
Two additional performance indicators that help measure efficiency are net collection rate and gross collection rate, both of which reflect how effectively a practice converts billed services into actual revenue. Together, these form core revenue cycle KPI benchmarks.
When to Escalate vs. Write Off a Neurology Claim
Not all unpaid claims can be collected, but decisions to write off must be structured and policy-driven. A write-off policy should clearly define when adjustments are appropriate, starting with contractual adjustments.
Other categories include bad debt, which applies when patient responsibility is uncollectible, and small balance threshold write-offs, typically used for very low-value amounts under a defined limit. However, no claim should be written off without at least one attempt at appeal or follow-up, especially in Neurology billing, where high-value procedures are common.
Step 8: Payment Posting and Reconciliation
Payment posting and reconciliation ensure that what payers approve is actually what gets recorded and collected. In Neurology billing, this step is especially important because claims often include multiple services per visit, and small mismatches between payment and expected reimbursement can quickly accumulate into significant revenue loss.
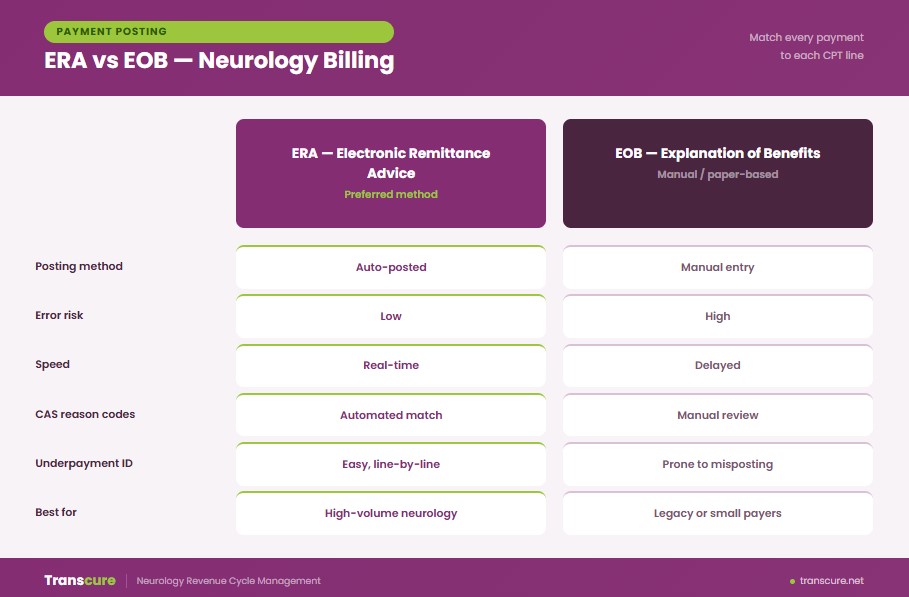
ERA vs. EOB Posting
Payment posting can be done through either ERA (Electronic Remittance Advice) or EOB (Explanation of Benefits). E A (Electronic Remittance Advice) allows payments and adjustments to be automatically posted to the correct claims, significantly reducing manual work and posting errors.
In contrast, EOB (Explanation of Benefits) is typically paper-based or manually entered, which increases the risk of misposting and delays in reconciliation. Once payments are received, they must be accurately matched to each CPT line item. It is critical in Neurology because a single encounter may include multiple services, each with separate billing lines. Adjustments are often communicated using CAS reason code, which explains why a payment differs from the billed amount.
Identifying Underpayments in Neurology Claims
Underpayments occur when a payer reimburses less than the contracted rate outlined in the provider agreement. To identify underpayments, practices must compare posted payments against the contracted fee schedule on a line-by-line basis. This comparison helps detect systematic underpayment, where certain services are consistently reimbursed below expected levels. Neurology procedures that involve both professional and technical components are particularly vulnerable to underpayment.
Secondary Insurance Billing and Coordination of Benefits
After the primary payer processes and posts a claim, any remaining balance may be billed to a secondary insurance. Th s process is known as coordination of benefits (COB) and must follow correct sequencing rules to avoid denials.
In Neurology billing, the primary payer’s EOB must always be attached when submitting the secondary claim. If claims are submitted out of order or if the primary payer is incorrectly identified, both insurers may deny the claim due to COB sequencing errors.
Special rules apply when Medicare Secondary Payer (MSP) rules are involved. In these cases, accurate identification of secondary payer responsibility is essential to ensure proper reimbursement.
Step 9: Patient Billing and Collections
Patient billing and collections in Neurology billing begin after insurance has processed the claim and posted its payment. Th s step focuses on collecting the remaining patient responsibility in a clear, timely, and compliant way.
When and How to Send Patient Statements After Insurance Payment
Patient statements should be sent within 5 business days after insurance payment is posted. Each patient statement should clearly break down what the insurance paid, what adjustments were applied, and what amount is now the patient’s responsibility.
It is important not to send statements while a claim is still pending with insurance, as this can result in incorrect balance billing and unnecessary patient confusion. Many practices also use a patient portal to provide real-time access to billing updates for consistency across the billing statement cycle.
Neurology billing is not a single task but a connected workflow where each step directly affects the next. From patient intake and eligibility verification to charge capture, claims submission, denial management, AR follow-up, payment posting, and patient collections, every stage builds on the accuracy of the one before it. The goal is not just to submit claims, but to maintain accuracy and accountability across the entire revenue cycle so that nothing is lost between service delivery and final payment.
How Does the Tele-Neurology Billing Process Work?
Tele-Neurology billing follows the same revenue cycle principles as in-person Neurology care, but the billing rules, documentation requirements, and payer expectations differ in key ways. Because services are delivered remotely, compliance depends heavily on correct visit classification, consent documentation, and payer-specific telehealth rules.
How the Tele-Neurology Billing Workflow Differs From In-Person
Tele-Neurology billing starts with confirming that the service is eligible for telehealth delivery under the payer’s policy. Unlike in-person visits, telehealth requires documented patient consent before the encounter, which must be recorded in the medical chart prior to or during the visit.
The type of virtual encounter also determines billing accuracy. A synchronous audio-video visit is treated differently from an audio-only encounter. The elehealth platform used must also be documented in the clinical record to support compliance and audit readiness.
Correct assignment of place of service code 02 (telehealth outside the patient’s home) or place of service code 10 (telehealth in the patient’s home) is essential for proper reimbursement. Not all Neurology services are covered under telehealth rules, so payer coverage must always be confirmed before scheduling to avoid denials.
What Documentation Is Required Before a Virtual Neurology Visit
Proper documentation must be completed before or at the time of a tele-neurology encounter to ensure claim validity. This includes confirmed telehealth consent, which may be verbal or written depending on payer requirements, and must be clearly documented in the chart.
One of the most common causes of tele-neurology claim denials is missing or incomplete pre-visit documentation. The elehealth platform used for the visit must be recorded, along with confirmation that the encounter was conducted through synchronous communication (real-time interaction). Patient location at the time of service must also be documented, as state licensure rules and cross-state telehealth regulations directly affect billing eligibility.
How Payer Rules for Telehealth Differ Across Medicare, Medicaid, and Commercial Plans
Telehealth reimbursement rules vary significantly across payers, making it unsafe to apply a single billing rule across all tele-neurology services.
Medicare telehealth policies have historically included originating site requirements, although many of these were relaxed during the Public Health Emergency (PHE). Medi id telehealth coverage varies by state, meaning each jurisdiction may have different rules for eligible services, modalities, and documentation requirements. In contrast, commercial payer telehealth policy is set individually by insurers such as UnitedHealthcare, Aetna, and Cigna, and may include additional restrictions or prior authorization requirements.
RCM Reporting and Billing KPIs Every Neurology Practice Should Track
Strong neurology billing performance depends on consistent tracking of revenue cycle metrics. RCM reporting gives visibility into where revenue is being lost, whether in coding, claims submission, denials, or collections.
Key Performance Indicators for Neurology Billing
Every neurology practice should actively monitor a core set of billing KPIs to measure financial health and operational efficiency. These indicators should be visible in a centralized KPI dashboard and reviewed regularly.
- Days in AR should stay below 35 days. Anything higher than signals slow collections or backlog in follow-up activity.
- Clean claim rate should be above 90%, meaning most claims are accepted without correction on the first submission.
- Denial rate should remain under 5%, as higher levels indicate upstream issues in coding, eligibility, or authorization.
- Net collection rate should exceed 95%, reflecting how effectively the practice collects contracted reimbursement.
- First-pass acceptance rate measures how many claims are accepted without edits or rework and directly reflects front-end accuracy.
- Cost to collect shows how much it costs to collect each dollar of revenue and helps evaluate billing efficiency.
When any KPI falls below target, it should trigger a structured review of the revenue cycle stage responsible, rather than isolated claim fixes. Persistent underperformance usually indicates a systemic workflow issue rather than individual errors.
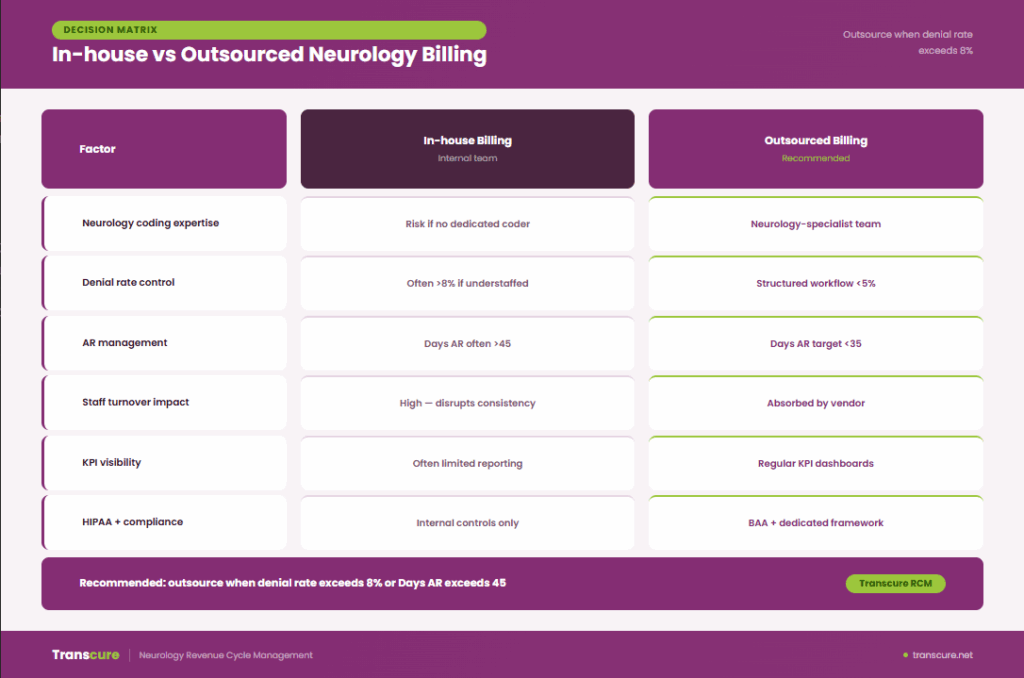
In-House Billing vs. Outsourcing Neurology Billing
Neurology practices often reach a point where neurology billing becomes too complex to manage internally. Choosing between in-house billing and outsourcing is less about cost alone and more about performance, compliance, and scalability of the revenue cycle.
Signs Your In-House Neurology Billing Is Underperforming
An in-house billing setup should deliver predictable performance. When it starts failing, the signs usually show up clearly in revenue cycle KPIs and staff workload.
A denial rate benchmark above 8% is a strong indicator that claims are not being submitted correctly or payer rules are not being consistently applied. Similarly, AR days benchmark exceeding 45 days suggests delays in follow-up, slow posting, or unresolved denials impacting cash flow.
A lack of specialized expertise, such as no dedicated neurology coder within the billing department, often leads to coding inaccuracies for complex procedures. High staff turnover further destabilizes consistency and increases error rates.
What to Look for in a Neurology Billing Company
Strong neurology billing companies should function as a true RCM partner, not just a claims processor. The most important factor is proven experience specifically in neurology billing workflows, not general medical billing. The provider should offer billing transparency through regular KPI reporting, including denial rates, AR trends, and collections performance.
Technology compatibility with your existing EHR system is essential to avoid workflow disruption during claims processing. A HIPAA compliance framework must be in place, including secure handling of patient data and proper documentation of processes. Finally, there should be a dedicated account manager responsible for communication between your practice and the outsourced billing team.
Neurology Billing Compliance and Payer Audit
Neurology billing is frequently reviewed under payer and federal audit programs due to the high volume of complex procedures and diagnostic testing. Strong compliance practices reduce exposure to OIG (Office of Inspector General) scrutiny and other audit programs.
Top Audit Triggers for Neurology Practices in 2026
Common audit triggers in neurology billing are usually linked to documentation gaps or utilization patterns that appear inconsistent. Frequent issues include EEG or EMG bundling errors that conflict with NCCI edits or improper billing of same-day services. High-frequency chemodenervation frequency for procedures like Botox can also raise red flags if not clinically justified.
Another major trigger is E/M upcoding without proper medical necessity documentation or clear MDM support. Incrementally, AI-assisted diagnostics are being reviewed when physician interpretation is not clearly documented.
Procedures such as infusion therapy without proper justification or inconsistent coding patterns may lead to RAC audit or CERT audit selection for review.
Pre-Audit Documentation Checklist for High-Risk Neurology Procedures
Audit readiness depends on having complete documentation available for high-risk procedures before any review occurs.
For EEG procedures, a signed interpretation report must be present in the chart. Infusion therapy requires a complete infusion log, along with supporting medical necessity letter documentation. For advanced procedures like DBS, records must include prior authorization confirmation and a detailed operative report.
A structured documentation checklist helps ensure consistency across providers and reduces audit risk significantly.
HIPAA Compliance in Neurology Billing Operations
Compliance with HIPAA is essential in all neurology billing operations due to the handling of sensitive patient data classified as PHI (Protected Health Information). Billing teams must ensure secure handling of PHI during claim submission, including restricted access within EHR systems.
All third-party billing vendors must operate under a valid BAA (Business Associate Agreement) that clearly defines responsibilities for data protection. Systems should include encryption and secure transmission protocols to reduce breach risk.
What Are the Most Common Neurology Billing Challenges
Neurology practices operate in a high-risk billing environment, with complex diagnostics, strict payer policies, and documentation-intensive services. This creates unique medical billing challenges not commonly seen in other specialties.
1. High Denial Rates For EEG, EMG, And NCS Procedures
Neurology claims for diagnostic testing are frequently denied due to missing documentation, incorrect code selection, or failure to meet payer-specific medical necessity criteria. EEGs, EMGs, and nerve conduction studies often require detailed clinical notes, test interpretations, and accurate CPT code sequencing.
2. Authorization Delays And Payer Restrictions
Many neurology procedures, such as Lumbar Puncture (CPT 62270, 62272) and Deep Brain Stimulation (DBS) implantation (CPT 61863), require prior authorization. Delay or missing authorizations can result in claim denials or extended reimbursement timelines, affecting cash flow.
3. Modifier Misuse and Incorrect Application
Neurology billing relies heavily on modifiers such as 25, 26, TC, and 59. Inconsistent or incorrect modifier usage can result in bundling issues, partial payments, or claim rejections.
4. Underpayment And Bundling Challenges
Payers might bundle neurology procedures incorrectly or reimburse only the technical or professional ones. This leads to underpayments when claims are not carefully reviewed and appealed.
5. Complex Documentation For Multi-Visit Neurology Care
Neurology often involves ongoing, multi-visit management of chronic conditions. Capturing all relevant symptoms, assessments, and treatment decisions for accurate coding is difficult, and omissions can lead to claim denials or audits.
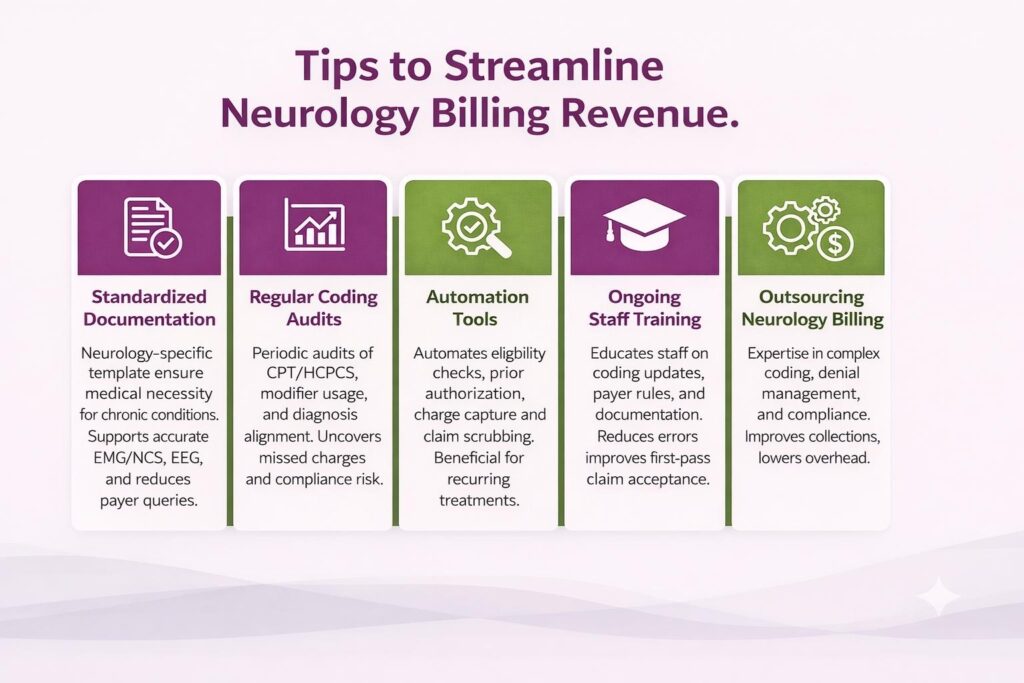
How Can Neurology Practices Streamline Billing and Increase Revenue
- Standardized Documentation: Implement neurology-specific documentation templates to capture medical necessity for chronic conditions, diagnostic testing, and time-based procedures. Consistent documentation supports accurate coding for EMG/NCS, EEG, infusion therapies, Botox injections, and high-level E/M services while reducing payer queries.
- Regular Coding Audits: Conduct periodic audits focused on neurology CPT and HCPCS usage, modifier application, and diagnosis-to-procedure alignment. Audit helps uncover missed charges, compliance risks, and denial patterns tied to high-ticket neurology services.
- Automation Tools: Use automation for eligibility checks, prior authorization tracking, charge capture, and claim scrubbing. Automated transcription is especially valuable for neurology practices due to recurring treatments and authorization-heavy procedures.
- Ongoing Staff Training: Train billing and clinical staff on neurology-specific coding updates, payer rules, and documentation standards. Continuous education reduces errors and improves first-pass claim acceptance.
- Outsourcing Neurology Billing: Partnering with a neurology-focused billing company such as Transcure provides expertise in complex coding, denial management, and payer compliance. It improves collections, lowers overhead, and allows providers to focus on patient care.
Conclusion
Accurate neurology medical billing is important for maximizing revenue, minimizing denials, and ensuring compliance across complex procedures. By following a structured medical billing process from pre-authorization and precise coding to claims submission and payment posting, neurology practices can streamline operations and improve cash flow. Using CPT and ICD-10-CM codes correctly helps practices reduce errors, improve reimbursements, and focus on delivering high-quality patient care.
Which CPT codes are commonly used for neurology procedures?
The most common CPT codes for neurology procedures include 95907–95913 for nerve conduction studies, 64615 for chemodenervation for chronic migraine, 64642–64643 for chemodenervation of extremity muscles, 96365–96368 for intravenous infusion therapy, and 99214–99215 for established patient E/M office visits.
What CPT Codes are Used for Botox and Chemodenervation in Neurology Billing?
Chemodenervation in neurology is billed using CPT 64615 for chronic migraine and 64642–64643 for extremity-based injections, along with HCPCS J0585 for onabotulinumtoxinA dosing.
Why are Neurology Claims Denied Even When Correct Codes are Submitted?
Neurology claims are denied due to missing prior authorizations, insufficient medical necessity documentation, incorrect modifier usage, or payer-specific billing rules, even when CPT and diagnosis codes are accurate.
How Do Modifiers Affect Reimbursement in Neurology Billing?
Modifiers such as 25, 26, TC, and 59 clarify service circumstances in neurology billing. Incor ect modifier application can result in bundling issues, partial payments, or claim rejections.
What is the CPT Code for a Neurology Appointment?
Neurology appointments use E/M CPT codes such as 99202–99205 for new patients and 99212–99215 for established patients, based on medical decision-making or time.
Can Teleneurology Visits be Billed Using Standard E/M Codes?
Yes, most 99204–99215 codes can be used if the visit meets time and complexity requirements, even when delivered virtually.
How Long Does it Take to Get Paid for Neurology Claims?
Clean neurology claims submitted electronically are typically paid within 14–30 days by commercial payers and within 14 days by Medicare. Claim requiring prior authorization review, manual processing, or correction after denial can extend to 45–90 days.
Should Neurology Practices Outsource Billing?
Outsourcing is worth considering if your denial rate exceeds 8%, Days in AR is consistently above 45, or you lack a dedicated neurology coder in-house. A medical billing services provider that supports neurology practices typically improves clean claim rates, reduces denials, and lowers cost-to-collect without the overhead of in-house training and turnover.