")
Neurology practices face higher billing risk than most specialties, with claim denial rates averaging 18% compared to the 5–10% industry average, according to the Medical Group Management Association (MGMA). These denials are often driven by documentation gaps, incorrect modifier use, and failure to meet payer rules around medical necessity.
This guide covers every major code category, billing rule, and compliance update that directly impacts reimbursement. The content aligns with guidance from the Centers for Medicare & Medicaid Services and coding standards from the American Medical Association.
What Are Neurology CPT Codes?
Neurology CPT codes are standardized medical billing codes used to report and document neurological services provided by physicians and specialists. These codes come from the American Medical Association and are part of the Current Procedural Terminology (CPT) system, which ensures consistent communication between healthcare providers, insurers, and billing teams.
CPT procedure codes cover diagnostic studies, therapeutic procedures, and patient visits. High-volume services such as EMG, nerve conduction studies, EEGs, Botox injections, and chronic care visits generate high revenue when coded accurately.
How Neurology CPT Codes Are Structured?
Neurology coding follows a defined structure that combines procedure codes, evaluation services, and payer rules. Most neurology CPT codes fall within a specific procedural range, but accurate billing depends on how these codes interact with documentation, diagnosis linkage, and payer policies. Understanding this structure helps reduce denials and ensures correct reimbursement under guidelines set by the Centers for Medicare & Medicaid Services and the American Medical Association.
What Is the CPT Code Range for Neurology?
Neurology and neuromuscular procedures are primarily reported under CPT codes 95700–96020. This includes diagnostic testing and monitoring services commonly performed in neurology practices.
Within this range, key subcategories include:
- EEG studies (95812–95836)
- EMG services (95860–95886)
- Nerve conduction studies (95907–95913)
In addition to procedural codes, neurologists frequently bill E&M services (99202–99215) for patient visits, along with HCPCS drug codes when applicable. Modifiers are often required to reflect technical vs. professional components or distinct procedural services.
What Governs Neurology Code Selection in 2026?
The Medicare Physician Fee Schedule governs code selection, the American Medical Association CPT manual, and payer-specific policies such as Local Coverage Determinations (LCDs). Payer LCD policies define medical necessity criteria for neurology services such as EEG, EMG, and nerve conduction studies, and must be reviewed alongside NCCI edits for full compliance.
Accurate code selection directly affects reimbursement and denial risk, making it critical to align procedure codes with documented medical necessity and diagnosis codes.
What Are the Most Common Neurology CPT Codes?
They cover a wide range of services related to the diagnosis, evaluation, and treatment of nervous system disorders, including conditions affecting the brain, spinal cord, nerves, and muscles.
Neurology E&M CPT Codes
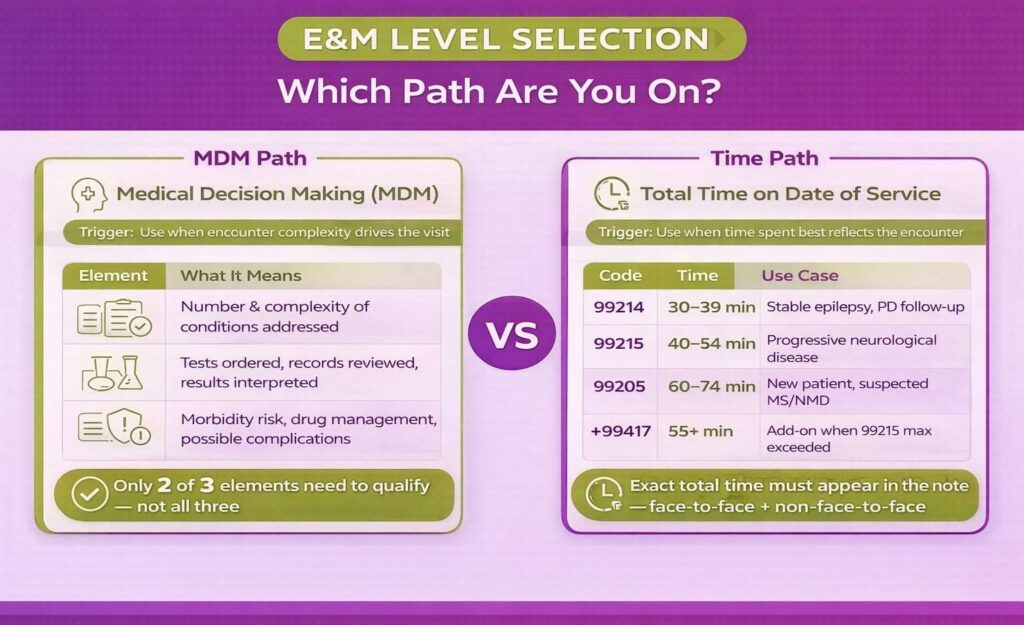
Evaluation and Management (E&M) coding is a major driver of revenue in Neurology. However, incorrect level selection is also a leading cause of denials and audits. According to the Centers for Medicare & Medicaid Services, E&M levels must be supported by either medical decision making (MDM) or total time spent on the date of service, not both.
Practices that struggle with E&M level selection often benefit from working with a dedicated neurology billing services provider that specializes in MDM documentation and audit defense.
MDM vs. Time-Based Selection for Neurology Visits
Under 2026 guidelines from the Centers for Medicare & Medicaid Services, providers can select the E&M level based on:
- MDM complexity, or
- Total time on the date of service (including face-to-face and non-face-to-face work)
Providers should select either MDM or total time based on which method most accurately reflects the complexity of the encounter. When using MDM, it is evaluated across three elements: the number and complexity of problems addressed, the amount and complexity of data reviewed, and the risk of complications or morbidity.
The final E&M level is determined by meeting at least two of these three elements at the same level, not all three. This “two-of-three” rule is often misunderstood and is a common source of both undercoding and audit risk in neurology billing.
New Patient vs. Established Patient E&M Codes
These codes are defined and maintained by the American Medical Association and reimbursed based on the Medicare Physician Fee Schedule.
| CPT Code | Description |
|---|---|
| 64642 | Chemodenervation, 1 extremity |
| 64643 | Each additional extremity |
When Should You Bill Prolonged Service Add-On Code 99417?
Use CPT code 99417 when the total provider time exceeds the maximum time threshold for 99215. This add-on code is only valid when:
- Time-based billing is used
- Total time clearly exceeds the highest E&M level
- Exact total time is documented in the note
Failure to document time explicitly can result in denials under the Centers for Medicare & Medicaid Services audit rules.
What Are the Most Common E&M Errors in Neurology Billing?
- Upcoding without documented MDM complexity
- Billing E&M with a same-day procedure without the appropriate modifier use
- Using time-based billing without a clear, verifiable time record
- Missing linkage to ICD-10-CM diagnosis codes
EEG CPT Codes: Routine, Long-Term, and Ambulatory
EEG billing is one of the most commonly used CPT codes in neurology. Most claims fall within the 95700–95726 series, and errors often occur due to missing time documentation, incorrect component billing, or incomplete interpretation reports.
Routine EEG CPT Codes (95812–95836)
Routine EEG codes are used for short-duration diagnostic studies. The patient’s state (awake, drowsy, or asleep) must always be documented, along with a signed interpretation report.
| CPT Code | Description |
|---|---|
| 96365 | Initial IV infusion, up to 1 hour |
| 96366 | Each additional hour |
| 96367 | Sequential infusion (additional drug/substance) |
| 96368 | Concurrent infusion |
Each claim must include a formal, signed physician interpretation report. Missing or unsigned interpretation documentation is a frequent denial trigger under CMS medical necessity enforcement standards.
Long-Term EEG Monitoring CPT Codes (95700–95726)
Long-term EEG (LTM) replaced older EEG monitoring codes (95950–95953) after CPT restructuring in 2020. These codes are time-tiered, meaning accurate start/stop time tracking is required for compliance.
| CPT Code | Description | Notes |
|---|---|---|
| 95700 | LTM setup, patient education, takedown | Billed once per monitoring period |
| 95711 | LTM technical recording, 2–12 hours | Time-based |
| 95712 | LTM technical recording, 12–26 hours | Time-based |
| 95714 | LTM technical recording, 24–48 hours | Time-based |
| 95716 | LTM technical recording, >48 hours | Extended monitoring |
| 95718–95726 | Professional interpretation codes | Tiered by duration |
In LTM billing:
- 95700 is billed once per episode
- Recording codes represent the technical component
- Interpretation codes represent the professional component
Incorrect separation of components is a major denial driver in payer audits under the Centers for Medicare & Medicaid Services.
Ambulatory and Video EEG CPT Codes
Ambulatory EEG is used for outpatient seizure monitoring outside the clinical setting, typically over 24–72 hours. Video EEG is commonly used in pre-surgical epilepsy evaluation. These studies must clearly document:
- Whether monitoring was remote or in-clinic
- Whether the physician’s interpretation was a continuous or delayed review
- Device setup and patient instructions
Pre-surgical epilepsy evaluation often involves extended EEG or video EEG monitoring and requires strong medical necessity documentation to support surgical planning.
Global vs. Professional vs. Technical EEG Billing: POS Rules
EEG reimbursement depends heavily on component separation and place of service (POS). Misclassification leads to underpayment or denials.
| Scenario | Modifier | Place of Service | Who Bills What |
|---|---|---|---|
| Practice owns equipment + physician interprets | None (global) | POS 11 (office) | Full fee schedule |
| Hospital owns equipment; physician interprets only | Modifier -26 | POS 21/22 | Professional component only |
| Practice owns equipment; no physician interpretation | Modifier -TC | POS 11 | Technical component only |
Incorrect modifier usage between -26 and -TC is a high-risk denial trigger under payer audit rules from the Centers for Medicare & Medicaid Services.
Category III CPT Codes for AI-Assisted EEG Analysis
Category III EEG codes are used for emerging technologies and advanced analytics. These are typically considered investigational until payer adoption is confirmed.
Relevant 2026 codes include:
- X461T–X466T — Continuous EEG monitoring services
- X504T — AI-supported EEG waveform analysis
These codes often require prior authorization, strong documentation of clinical utility, and verification of payer coverage before submission. A key compliance requirement is that AI-generated interpretations alone do not meet documentation standards. The treating provider must review the output and document the final clinical decision. This distinction is actively audited by payers in 2026.
EMG and Nerve Conduction Study CPT Codes
EMG and NCS services are core revenue drivers in neurology, but they are also frequently audited due to bundling errors, incomplete documentation, and incorrect modifier use. Neuromuscular diagnostic coding must clearly reflect anatomical specificity and clinical justification to support reimbursement for EMG and related procedures.
Needle EMG CPT Codes (95860–95886)
Needle EMG codes measure muscle electrical activity and vary by anatomical complexity and number of muscles studied.
| CPT Code | Description | wRVU (2026) |
|---|---|---|
| 95860 | Needle EMG, 1 extremity | 0.90 |
| 95861 | Needle EMG, 2 extremities | 1.10 |
| 95885 | EMG, same day as NCS, limited | 0.90 |
| 95886 | EMG, 5+ muscles, 3+ nerves or 4+ spinal levels | 1.56 |
CPT 95886 is the most commonly reported EMG code nationally. It is most appropriate for comprehensive studies, such as evaluation of suspected ALS or motor neuron disease requiring multi-extremity and bulbar testing, and for generalized myopathy or polyneuropathy workups involving multiple nerves and muscle groups.
When supported by documentation and medical necessity, 95886 justifies higher reimbursement due to its broader diagnostic scope and higher work RVU (1.56).
Nerve Conduction Study CPT Codes (95907–95913)
NCS testing evaluates nerve signal conduction and is billed based on the number and type of studies performed.
| CPT Code | Description | wRVU (2026) |
|---|---|---|
| 95907 | 1–2 studies | 0.65 |
| 95908 | 3–4 studies | 0.85 |
| 95909 | 5–6 studies | 1.05 |
| 95910 | 7–8 studies | 1.25 |
| 95911 | 9–10 studies | 1.45 |
| 95912 | 11–12 studies | 1.65 |
| 95913 | 13+ studies | 1.85 |
Each direction of testing (motor, sensory, F-wave, or reflex study) counts as a separate study, which directly impacts code selection and reimbursement accuracy.
How To Bill EMG and NCS Together Without Triggering NCCI Edits?
EMG and NCS are commonly billed together, but improper documentation can trigger National Correct Coding Initiative (NCCI) denials.
Use Modifier -59 only when:
- EMG and NCS are performed on different anatomical regions
- Each service has clearly separate documentation
- Medical necessity supports both procedures independently
Improper use of modifiers is a leading cause of denials under Centers for Medicare & Medicaid Services edit rules.
Chemodenervation and Botox Injection CPT Codes
Chemodenervation is a high-volume, high-scrutiny service in neurology, especially for migraine, spasticity, and dystonia management. These services are governed by CPT rules from the American Medical Association and reimbursement policies enforced by the Centers for Medicare & Medicaid Services. Accurate documentation and correct separation of drug vs. procedure billing are essential for compliance and reimbursement.
CPT 64615: Botox for Chronic Migraine
CPT 64615 is used for chemodenervation of facial, neck, or scalp muscles for chronic migraine treatment. This is one of the most commonly billed neurology injection procedures. The documentation for CPT 64615 must include:
- Confirmed diagnosis of chronic migraine
- History of failed preventive therapies (e.g., beta-blockers, anticonvulsants, or CGRP inhibitors when applicable)
- Injection sites and muscle groups treated
- Total units administered and distribution pattern
Incomplete documentation is a common denial trigger under payer-enforced medical necessity standards. Frequency limits are a key compliance requirement. Most payers, including Centers for Medicare & Medicaid Services, restrict onabotulinumtoxinA (Botox) for chronic migraine to one treatment every 12 weeks.
Claims billed outside this interval without a clear clinical justification are commonly denied. Documentation must include the date of the previous treatment cycle to support each claim.
Chemodenervation for Spasticity and Dystonia (64642–64643)
| CPT Code | Description |
|---|---|
| 64642 | Chemodenervation, 1 extremity |
| 64643 | Each additional extremity |
64643 cannot be billed as a standalone code. It must always be reported with a primary chemodenervation code. Incorrect standalone billing is a frequent audit trigger under Centers for Medicare & Medicaid Services compliance reviews.
Why Billing J0585 (OnabotulinumtoxinA) Is Billed Separately From The Procedure Code?
HCPCS code J0585 represents onabotulinumtoxinA (Botox) and must always be billed separately from the injection procedure code (e.g., 64615).
Key billing rules:
- J0585 must appear on a separate line item from CPT 64615
- Units must be billed precisely: 1 unit billed = 1 unit administered
- Drug wastage policies must follow payer-specific documentation requirements
Improper bundling of drugs and procedures is a high-frequency denial reason in neurology injection billing under the Centers for Medicare & Medicaid Services guidelines.
What is The Modifier -25 Rule in Practice For Same-Day Botox + E&M?
When an Evaluation & Management (E&M) service is performed on the same day as a Botox injection, modifier -25 may be used only when the E&M service is separately identifiable from the procedure.
Correct use requires:
- A distinct clinical evaluation beyond the injection decision
- Separate documentation supporting the E&M service
- Clear indication that E&M was not part of the routine pre-procedure assessment
Incorrect use occurs when providers bill E&M solely for routine injection visits without additional clinical work. This remains one of the most common audit issues flagged by the Centers for Medicare & Medicaid Services.
Infusion Therapy CPT Codes in Neurology
Infusion therapy is used for conditions like multiple sclerosis (MS), autoimmune neuropathies, and neuroinflammatory disorders. These services are tightly regulated by the Centers for Medicare & Medicaid Services and must strictly follow CPT coding rules from the American Medical Association. Documentation accuracy, especially time tracking and drug linkage, directly impacts reimbursement under medical necessity standards.
IV Infusion Administration Codes (96365–96368)
These CPT codes are used for therapeutic, prophylactic, or diagnostic infusion services.
| CPT Code | Description |
|---|---|
| 96365 | Initial IV infusion, up to 1 hour |
| 96366 | Each additional hour |
| 96367 | Sequential infusion (additional drug/substance) |
| 96368 | Concurrent infusion |
All infusion claims must include start time and stop time for each infusion session for the documentation requirement. Missing time documentation is a frequent denial trigger under CMS audit guidelines.
Specialty Biologic Infusion Code (96413)
CPT 96413 is used for the administration of high-cost biologic agents commonly used in neurology, including MS disease-modifying therapies.
Key use cases include:
- Multiple sclerosis infusion therapy
- Monoclonal antibody treatments
- Other specialty biologic neurologic therapies
Accurate reporting requires linkage between the infusion administration code and the corresponding drug code to support reimbursement under medical necessity.
Chronic Care Management (CCM) Codes in Neurology
Chronic Care Management services represent a significant billing opportunity for neurology practices managing long-term conditions such as multiple sclerosis, Parkinson’s disease, and epilepsy.
| CPT Code | Service Type | Description | Typical Neurology Use |
|---|---|---|---|
| 99490 | CCM | 20 min/month of clinical staff time | MS, Parkinson’s, epilepsy |
| 99439 | CCM add-on | Each additional 20 minutes | Complex chronic patients |
CCM billing requires patient consent, a documented care plan, and at least 20 minutes of non-face-to-face clinical management time per calendar month. These codes are frequently underutilized in neurology despite high eligibility rates among chronic disease populations.
Neurology Diagnostic CPT Codes: Neuroimaging and Sleep Studies
Diagnostic testing is a core part of neurology workflows, especially for stroke, epilepsy, dementia, and sleep disorders. Correct coding, interpretation, and modifier use directly affect reimbursement and the risk of denial.
Neuroimaging CPT Codes Commonly Used in Neurology
| CPT Code | Procedure | Clinical Use Case | Modifier Notes |
|---|---|---|---|
| 70551 | MRI brain without contrast | Seizures, multiple sclerosis, lesion detection | Use Modifier -26 when billing professional interpretation only |
| 70553 | MRI brain with and without contrast | Tumors, inflammatory disease, complex lesion evaluation | Use Modifier -26 when billing professional interpretation only |
| 70450 | CT head without contrast | Stroke, trauma, acute headache, hemorrhage evaluation | Use Modifier -26 when billing professional interpretation only |
| 78608 | PET brain scan | Alzheimer’s disease, dementia evaluation, neurodegenerative disorders | Use Modifier -26 when billing professional interpretation only |
When neurologists interpret imaging without owning equipment, Modifier -26 must be applied. Incorrect modifier use is a frequent denial trigger under medical necessity enforcement rules.
Neurology Biomarker & Dementia Diagnostic Lab Codes
| CPT Code | Procedure | Clinical Use Case | Billing Notes |
|---|---|---|---|
| 81479 (commonly used) or PLA codes | Beta-amyloid testing (Aβ42/Aβ40, plasma or CSF) | Alzheimer’s disease evaluation, amyloid pathology assessment | No universal CPT Category I code; often requires prior authorization; payer-specific coverage |
| 81479 (commonly used) or PLA codes | Tau protein testing (total tau, phosphorylated tau) | Alzheimer’s disease staging and differential dementia diagnosis | Coverage highly variable; often investigational; prior authorization commonly required |
| 81479 (or lab-specific immunoassay codes) | Neurofilament light chain (NfL) testing | Neurodegeneration monitoring (MS, ALS, dementia research/adjunct use) | No Category I CPT; often non-covered or investigational depending on payer |
Sleep Study CPT Codes in a Neurology Context (95810, 95811)
| CPT Code | Description | Clinical Use Case | Key Requirement |
|---|---|---|---|
| 95810 | Attended overnight polysomnography | Sleep apnea, parasomnias, REM disorders | Full-night sleep study with interpretation |
| 95811 | Polysomnography with CPAP titration | Sleep apnea treatment optimization | CPAP titration documentation required |
Neurostimulator Implantation CPT Codes for Parkinson’s and Epilepsy
| CPT Code | Procedure | Clinical Use Case | Risk Level |
|---|---|---|---|
| 61850 | Intracranial electrode placement | Epilepsy monitoring, DBS planning | High |
| 61886 | Neurostimulator pulse generator implantation | Parkinson’s disease, movement disorders | High |
| 61889 | Revision or removal of neurostimulator system | Device adjustment or complications | High |
These procedures are considered high audit-risk due to cost and complexity. Prior authorization is typically required, and documentation must clearly establish medical necessity under CMS rules.
Remote Patient Monitoring CPT Codes in Neurology
Remote Patient Monitoring (RPM) is increasingly used in neurology for seizure tracking, headache management, and chronic disease follow-up. These codes are regulated under billing frameworks from the Centers for Medicare & Medicaid Services. Practices must meet strict time, device, and documentation requirements to ensure reimbursement under medical necessity rules.
RPM Setup and Device Supply Codes
| CPT Code | Description | Key Requirement |
|---|---|---|
| 99453 | RPM setup and patient education | One-time setup per episode |
| 99454 | Device supply, daily recordings | 16+ days of data in a 30-day period required |
A key 2026 compliance rule is that RPM billing must clearly document device supply duration and active monitoring days. Failure to specify the number of monitored days is now one of the most common denial triggers.
Treatment Management Time
| CPT Code | Description | Time Requirement |
|---|---|---|
| 99457 | First 20 minutes of clinical management per month | Interactive communication required |
| 99458 | Each additional 20 minutes | Must be linked to care management |
Time must be clearly documented and tied to a clinical decision, a care plan update, or an intervention, not just to a passive review of incoming device data. Unclear documentation, such as “reviewed monitoring,” is insufficient for reimbursement under payer audit standards from the Centers for Medicare & Medicaid Services.
What Are Neurology RPM Use Cases?
RPM is commonly used in neurology for:
- Seizure tracking through wearable or implantable devices
- Chronic migraine monitoring via digital health platforms
- Post-treatment response tracking in medication adjustments
However, payer coverage for RPM varies significantly across plans and regions. Practices must verify eligibility and authorization requirements before enrolling patients in RPM programs. Incorrect assumptions about coverage often lead to preventable denials under medical necessity enforcement rules.
Tele-Neurology CPT Codes and Modifier Requirements
Tele-neurology has become a standard care delivery model in neurology, especially for follow-ups, medication management, and chronic disease monitoring. Correct use of modifiers and place of service codes is essential to avoid claim rejections.
Tele-Neurology CPT Codes
| CPT Code | Description | Clinical Use Case | Billing Notes |
|---|---|---|---|
| 99202–99215 | Office/Outpatient E/M (Telehealth) | Real-time video visits for conditions like migraine, epilepsy, or Parkinson’s follow-up | Append modifier 95 (or payer-required equivalent); use POS 10 or 02 |
| 99421–99423 | Online Digital E/M | Patient portal evaluation and management over a 7-day period | Time-based; established patients only |
| 99441–99443 | Telephone E/M | Audio-only neurology visits when video is unavailable | Coverage varies by payer; may require modifier 93 |
| 99457–99458 | Remote Physiologic Monitoring (RPM) | Monitoring neurologic conditions (e.g., movement disorders, MS symptoms) | Requires device data + interactive communication |
What Is The Difference Between Modifier 95 vs. Modifier 93
| Modifier | Service Type | When to Use | 2026 Note |
|---|---|---|---|
| -95 | Synchronous audio-video telehealth | Standard telehealth visits | Widely accepted across most payers |
| -93 | Audio-only telehealth | Used when video is unavailable and payer allows it | Must verify Appendix T eligibility before use |
Modifier selection must match the actual delivery method. Incorrect pairing of service type and modifier is a common cause of telehealth claim denials under Centers for Medicare & Medicaid Services audit rules.
Place of Service Codes for Tele-Neurology
| POS Code | Description | Use Case |
|---|---|---|
| POS 02 | Telehealth provided other than patient’s home | Clinic-to-clinic or non-home telehealth |
| POS 10 | Telehealth provided in patient’s home | Most modern tele-neurology visits |
A key compliance issue in 2026 is misalignment between the POS code, the telehealth modifier, and the payer telehealth indicator. This mismatch often triggers automatic claim rejections or downcoding during CMS claims processing.
Which Neurology Services Qualify for Audio-Only Billing?
Audio-only billing is limited and must follow payer-specific Appendix T rules under the CPT framework from the American Medical Association.
Common eligible neurology services include:
- Follow-up E&M visits when video is unavailable and allowed by payer policy
- Medication management for stable chronic neurological conditions
- Patient counseling and care coordination visits
An often-missed eligibility category includes neuropsychological testing codes (96130–96133), which are recognized under Appendix T for audio-only allowances in specific payer policies. Many practices fail to bill these correctly, resulting in lost revenue opportunities despite eligibility.
What Are Common Neurology Modifiers?
Modifiers are one of the highest-impact elements in neurology CPT coding. In Neurology, most denials are not caused by incorrect CPT selection but by incorrect or unsupported modifier use. These rules are governed by CPT standards from the American Medical Association and enforced through claim edits by the Centers for Medicare & Medicaid Services.
Neurology Modifiers Quick-Reference Table
| Modifier | Meaning | When Used | Audit Risk |
|---|---|---|---|
| -25 | Significant, separately identifiable E&M | E&M + procedure same day | High |
| -59 | Distinct procedural service | EMG/NCS separation, nerve blocks | Very High |
| -26 | Professional component only | Interpretation only services | Medium |
| -TC | Technical component only | Equipment + technician services | Medium |
| -51 | Multiple procedures | Multiple services in same session | Medium |
This table serves as a quick compliance reference for neurology billing teams to reduce denial risk and improve consistency across claims submitted to the Centers for Medicare & Medicaid Services.
NCCI Bundling Edits in Neurology Billing: How To Prevent Denials Before They Happen
Neurology has the highest exposure to NCCI bundling denials of any specialty due to the frequency of multi-service encounters. National Correct Coding Initiative (NCCI) edits are one of the leading causes of neurology claim denials and underpayments. These edits define which procedure codes can be billed together and which are bundled into a single payable service.
In neurology, procedures like EEG, EMG, nerve conduction studies, and chemodenervation are frequently performed together. Practices that fail to follow NCCI rules can face automatic denials, partial payments, or audit risk. Many practices partner with specialized neurology billing companies to manage NCCI compliance, since multi-service encounters require pre-submission scrubbing that in-house teams often lack the capacity to perform.
What Are NCCI Edits and Why Do They Matter?
NCCI edits are published by CMS to prevent:
- Unbundling (billing components separately when they should be grouped)
- Duplicate billing for overlapping services
- Improper modifier usage
There are two key edit types:
- Column 1 / Column 2 Edits — Column 2 codes are bundled into Column 1 and not separately payable unless a valid modifier (e.g., -59) is applied.
- Medically Unlikely Edits (MUEs) — Limit the maximum units of a service billable per patient per day.
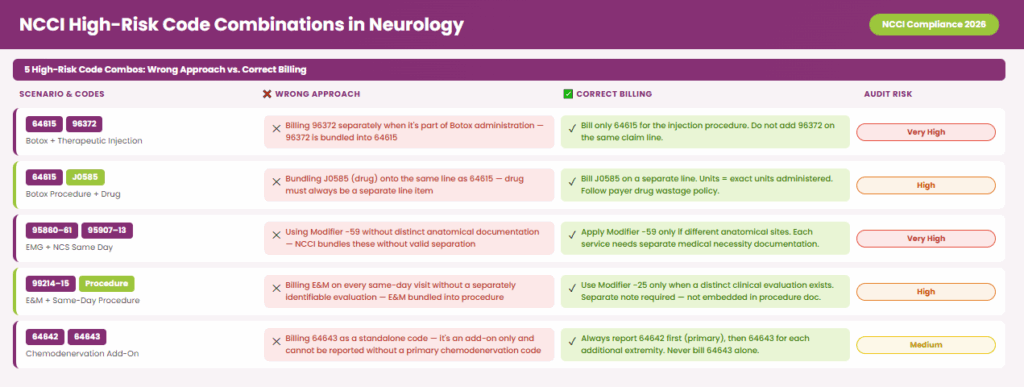
What Are High-Risk NCCI Bundling Scenarios in Neurology (2026)
The following CPT combinations commonly trigger NCCI edits in neurology billing:
| Scenario | What Happens | Correct Billing Approach |
|---|---|---|
| Chemodenervation (64615) + Therapeutic Injection (96372) | 96372 is bundled into 64615 | Do not bill 96372 separately when performed as part of Botox administration |
| J0585 (Botox drug) + 64615 | Drug must be billed separately | Always bill J0585 on a separate line item with correct units |
| EMG (95860–95861) + NCS (95907–95913) | Often bundled without modifier | Use Modifier -59 only if performed on different anatomical sites with separate documentation |
| E/M (99214–99215) + Procedure Same Day | E/M bundled into procedure | Use Modifier -25 only if a separate, significant evaluation is documented |
| Multiple Nerve Blocks (64450, etc.) | Subject to multiple procedure reduction | Apply Modifier -51 where appropriate; ensure documentation supports each service |
Step-by-Step: How to Avoid NCCI Denials in Neurology Billing
Clean claim submission in neurology requires front-end validation of CPT codes, ICD-10 linkage, and modifiers before submission to maximize first-pass acceptance rates. To consistently submit clean claims, implement this pre-submission NCCI check workflow:
- Run CPT Code Pair Check: Validate all procedure combinations against the current NCCI edit tables.
- Verify Modifier Necessity: Flag all same-day procedures and confirm if -25 or -59 is required.
- Check Documentation Support: Ensure separate procedure notes exist, distinct anatomical sites are documented, and medical necessity is justified for each service.
- Validate Drug and Procedure Separation: Always bill HCPCS drug codes (e.g., J0585) separately from procedure CPT codes.
- Apply Claim Scrubbing Tools: Use neurology EHR systems with built-in claim scrubbing or clearinghouse edits to catch bundling issues before submission.
NCCI bundling edits are not just a compliance requirement; they are a revenue protection mechanism. Neurology revenue cycle management is increasingly dependent on documentation accuracy, payer policy alignment, and automated claim validation systems.
By understanding high-risk code combinations, applying modifiers correctly, and implementing a proactive claim review process, neurology practices can significantly reduce denials, capture full reimbursement, and stay audit-ready in 2026.
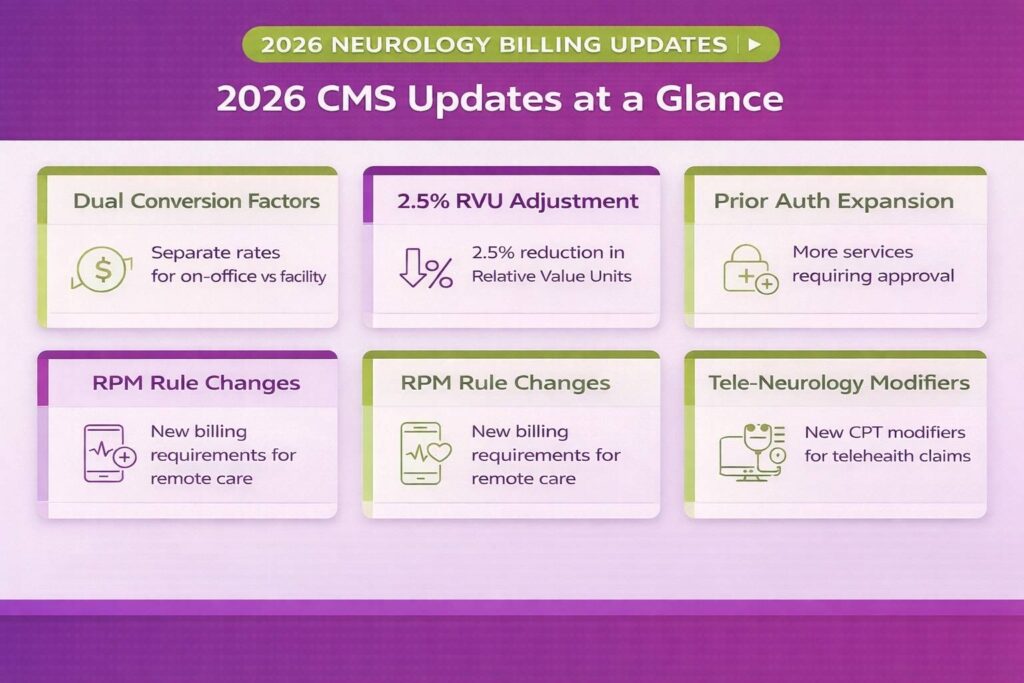
2026 Neurology Billing Updates
This section includes important 2026 CMS and payer updates impacting neurology billing. Neurology practices need to keep up with these updates to avoid facing unexpected claim denials or rejection.
CMS Dual Conversion Factors For Physician Fee Schedule
CMS has introduced dual conversion factors for 2026, with approximately $33.57 for APM participants and $33.40 for non-APM providers. While the difference is small, it has a noticeable impact in high-volume neurology practices.
EMG (95860–95886), nerve conduction studies (95907–95913), and EEG services, such as 95812 and 95816, are directly affected because reimbursement is RVU-driven. Even minor adjustments can accumulate across frequent diagnostic testing, making accurate coding and documentation more important than ever.
2.5% Efficiency Adjustment
The 2.5% efficiency adjustment reduces non-time-based work RVUs, impacting common neurology services such as EMG, NCS, EEG interpretation, and botulinum toxin injections.
Because these services rely heavily on work RVUs, the adjustment results in incremental reimbursement reductions that must be offset through precise coding, documentation, and correct modifier usage.
Prior Authorization Tightening for High-Cost Procedures
Prior authorization requirements continue to expand for neurology services, including MRI brain, PET scans, EMG/NCS in select payer regions, and procedures like deep brain stimulation.
Most denials result from administrative issues, such as missing authorization, expired approvals, or mismatched documentation, rather than clinical errors. Prior authorization is now a required front-end billing step, not an optional safeguard.
Category III CPT Codes for AI-Assisted Neurology Diagnostics
Category III codes now support AI-assisted EEG analysis and advanced neuroimaging tools. These codes are considered experimental and require strong documentation of clinical necessity and methodology. Coverage varies widely by payer, and improper use can lead to denials or audit risk.
Remote Patient Monitoring (RPM) Rule Updates
RPM codes 99453 and 99454 now require clear documentation of device setup and at least two days of data collection within a 30-day period. Short-duration RPM refers to emerging CMS-supported monitoring models typically ranging from 2–15 days, used for episodic neurological conditions such as seizures and migraines. Codes 99457 and 99458 require clinically meaningful treatment management time.
A key 2026 update is that device supply duration must be clearly documented, as missing timeframes are a leading cause of RPM denials in neurology.
Tele-Neurology Expansion and Modifier Updates
Modifier 95 applies to audio-video telehealth visits, while Modifier 93 is used for audio-only services when allowed by payer policy. POS 02 and POS 10 must align correctly with the telehealth delivery location.
Any mismatch between POS, modifier, and telehealth indicator is now a common cause of claim rejection. Some neuropsychological testing codes (96130–96133) may qualify for audio-only billing under Appendix T, depending on payer rules.
Increased Focus on Denial Prevention and Compliance
Payers are increasingly strict about documentation quality, modifier accuracy, and medical necessity. High-risk areas include Modifier 25, Modifier 59, EMG/NCS documentation, EEG justification, and prior authorization alignment.
Even correctly coded claims may be denied without strong supporting documentation, making pre-bill review and audit workflows essential in 2026.
What These Updates Mean for Neurology Practices
Overall, 2026 reinforces a shift toward documentation-heavy, compliance-driven neurology billing. Practices that update coding systems, strengthen documentation, and improve authorization workflows will reduce denials and stabilize reimbursement in an increasingly strict payer environment. For a full breakdown of how claims move from documentation to payment, see our neurology billing process guide. It covers the complete revenue cycle workflow aligned with 2026 CMS requirements.
How to Ensure Accuracy When Billing for Specific Neurology Procedures?
Correct coding requires matching precise procedure codes with the latest documentation and modifier rules. For a complete breakdown of specific codes and billing standards, see our comprehensive guide for CPT Codes in medical billing.






