
CPT code 99213 is an evaluation and management code used to report an office or outpatient visit for an established patient that requires either low-complexity medical decision making or 20–29 minutes of total time on the date of the encounter. Procedure code 99213 is the most frequently billed E/M code across primary care.
The code is used for established patients with stable chronic conditions, minor acute illnesses, or routine follow-up visits that do not involve significant medication management decisions or new problem evaluation.
Under the 2021 AMA E/M guidelines, code 99213 CPT may be selected based on either MDM or total time. History and physical exam no longer determine the code level, though they must remain medically appropriate to the visit.
What Is the Description of CPT Code 99213?
99213 CPT code description defined by the AMA is: “Office or other outpatient visit for the evaluation and management of an established patient, which requires a medically appropriate history and/or examination and low level of medical decision making. When using total time on the date of the encounter for code selection, 20-29 minutes of total time is spent on the date of the encounter.”
99213 CPT code applies only to established patients, those who have received professional services from the physician or another physician of the same specialty in the same group practice within the past three years. Comparable-complexity new patient visits are reported under code CPT 99203.
What Are the Two Pathways to Qualify for CPT Code 99213: MDM vs. Total Time?
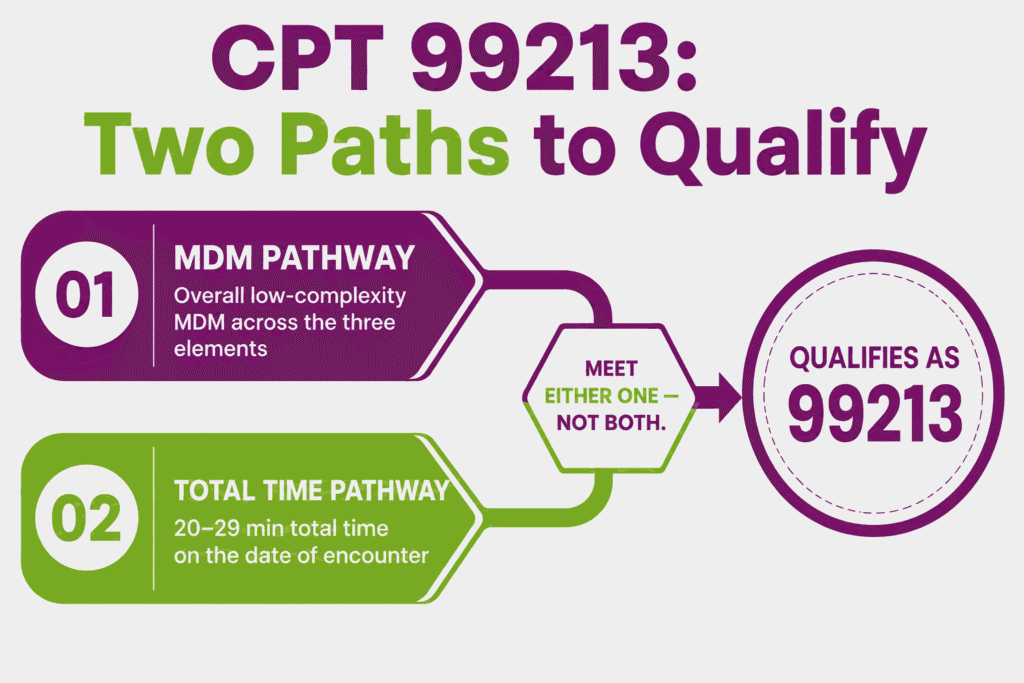
Per the 2021 AMA E/M guidelines, CPT code 99213 may be selected using either of two independent pathways:
- Medical Decision Making (MDM) Pathway: The visit qualifies for procedure code 99213 when the overall MDM level reaches “low” complexity, based on the three MDM elements (problems addressed, data reviewed, and risk). History and examination are performed as medically appropriate, but do not determine the code level.
- Total Time Pathway: The visit qualifies for CPT code 99213 when the physician or qualified health care professional spends 20–29 minutes of total time on the date of the encounter, regardless of the MDM level. Total time includes both face-to-face and non-face-to-face time personally spent by the billing provider on the date of the encounter. This includes pre-visit chart review, history-taking, examination, counseling, ordering, documentation, and care coordination.
Only one pathway needs to be met. A visit with lower MDM complexity but extensive time spent or vice versa may still qualify for code 99213 CPT under whichever pathway is satisfied.
What Qualifies as Low Medical Decision Making for CPT Code 99213?
Low MDM supporting CPT code 99213 is determined by meeting or exceeding the low level in at least two of the following three elements:
- Number and Complexity of Problems Addressed: Typically reflects two or more self-limited or minor problems, or one stable chronic illness, or one acute, uncomplicated illness or injury
- Amount and/or Complexity of Data Reviewed and Analyzed: Typically reflects review of the results of one or two unique tests, or a limited review of external notes, or an assessment requiring an independent historian
- Risk of Complications, Morbidity, or Mortality of Patient Management: Typically reflects over-the-counter medication management, or minor treatments without significant risk factors, such as a recommendation for rest, ice, or a non-prescription remedy
Meeting low-level criteria in at least two of the three elements supports CPT code 99213 under the MDM pathway. If the visit involves prescription drug management or addresses a chronic illness with exacerbation, the MDM level typically rises to moderate, supporting the CPT 99214 code instead.
How Much Total Time Is Required for CPT Code 99213 Under the Time-Based Pathway?
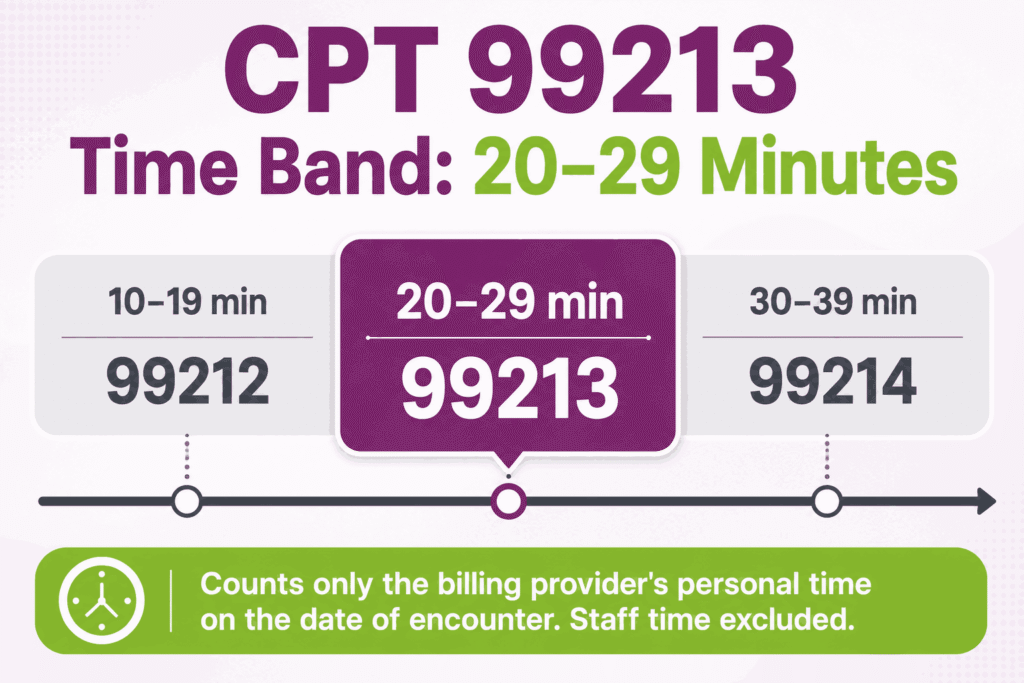
Under the time-based pathway, CPT code 99213 requires 20–29 minutes of total time spent by the billing physician or qualified health care professional on the date of the encounter. This is a defined band. Visits totaling 10–19 minutes fall to CPT 99212, while visits totaling 30–39 minutes qualify for CPT 99214.
Total time must be personally performed by the billing provider and clearly documented, including the total minutes spent and a description of the activities performed. Time spent by clinical staff (e.g., rooming, vitals) is not counted toward the billing provider’s total time for procedure code 99213.
How Does CPT Code 99213 Differ From CPT 99212 and CPT 99214?
These three established patient E/M codes are distinguished by MDM level and total time:
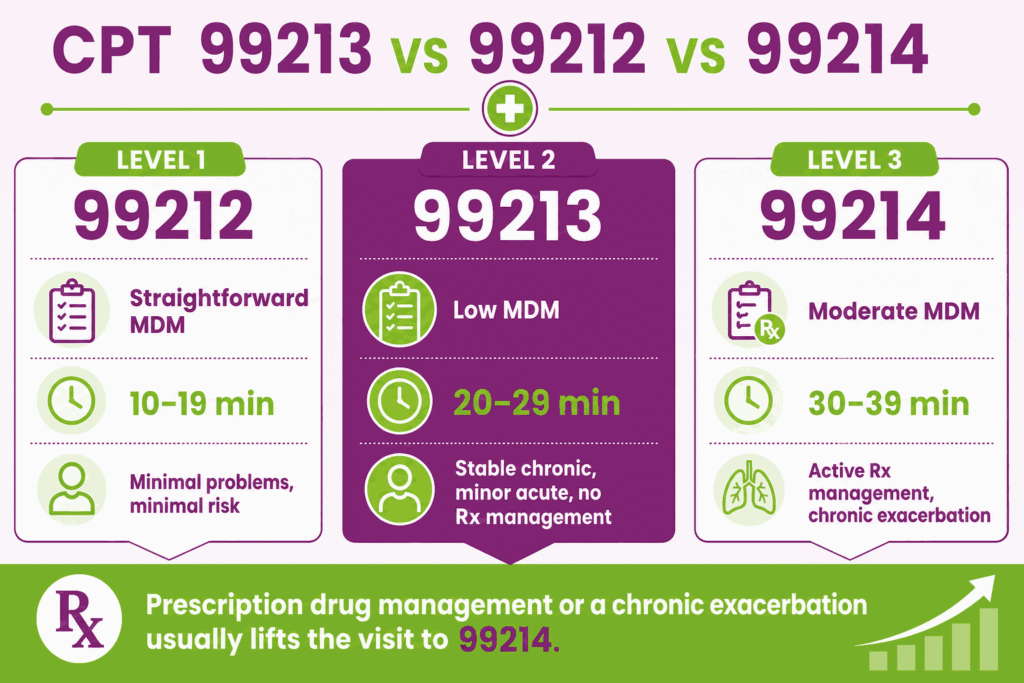
- CPT Code 99212: Straightforward MDM or 10–19 minutes total time. Procedure code 99212 Used for established patients with minimal problems and minimal risk
- CPT Code 99213: Low-complexity MDM or 20–29 minutes total time. Used for established patients with stable chronic conditions, minor acute illnesses, or routine follow-up not involving prescription drug management
- CPT Code 99214: Moderate-complexity MDM or 30–39 minutes total time. Used for established patients with chronic conditions requiring active management, prescription drug management, or new problems with moderate risk
The defining distinction between the 99213 CPT code and the 99214 is typically the presence of prescription drug management or a chronic illness with exacerbation, progression, or treatment side effects. Either of these generally elevates the visit from low to moderate MDM, supporting 99214 instead of 99213.
Why CPT Code 99213 Is Restricted to Established Patients Only
CPT code 99213 is part of the established patient office visit code family (99211–99215) and cannot be billed for a patient being seen by the practice for the first time. The AMA defines an established patient as one who has received professional services from the physician or qualified health care professional, or another physician or qualified health care professional of the same specialty in the same group practice, within the past three years.
If the three-year lookback finds no qualifying prior encounter, the visit must be reported using the corresponding new patient code (99202–99205), which carry higher RVU values reflecting the additional work of establishing a new patient record, comprehensive history, and initial care planning. Billing procedure code 99213 for a new patient or vice versa is a documented compliance and audit risk.
Can CPT 99213 Be Billed by Non-Physician Practitioners Under Incident-To Rules?
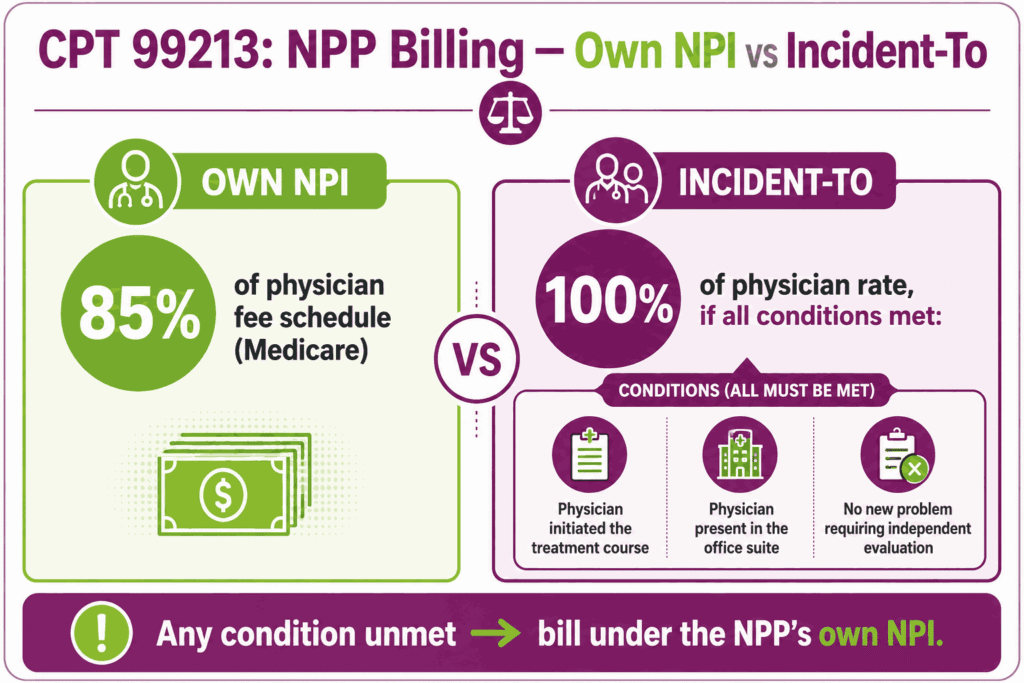
Yes, CPT code 99213 may be billed by non-physician practitioners (NPPs), including nurse practitioners and physician assistants. They do it either under their own NPI at the standard NPP payment rate (typically 85% of the physician fee schedule for Medicare), or under “incident-to” billing rules at 100% of the physician rate when all incident-to requirements are met.
Incident-to billing for procedure code 99213 requires that the service be part of a course of treatment initiated by the supervising physician, the supervising physician must be physically present in the office suite at the time the service is rendered, and the visit must not involve a new problem requiring independent physician evaluation. When incident-to requirements are not met, CPT code 99213 must be billed under the NPP’s own NPI.
What Are the Telehealth Billing Rules for CPT Code 99213?
CPT code 99213 remains on the Medicare telehealth services list and may be billed for visits delivered via real-time, interactive audio-video technology. Per current 2026 telehealth billing guidance:
- Modifier 95 is appended to CPT code 99213 to indicate the service was delivered via synchronous audio-video telecommunications technology
- Place of Service 10 is used when the patient is located in their home at the time of the telehealth visit; Place of Service 02 is used when the patient is located somewhere other than home
- Audio-only visits require modifier 93, where the payer permits audio-only billing for the 99213 CPT code. Medicare has historically not adopted audio-only E/M billing for established patient office visits and may deny claims billed this way; verify current MAC policy before billing audio-only
- The visit must still meet either the MDM or total-time requirement for CPT code 99213, regardless of delivery modality. Also, documentation must reflect the technology platform used and confirm the encounter was conducted via live audio-video communication
Telehealth policy for E/M codes changes frequently based on Congressional extensions of Medicare telehealth flexibilities. Providers should verify current-year telehealth eligibility for procedure code 99213 with their MAC before billing.
What are the Modifiers for CPT Code 99213?
CPT code 99213 may be reported with modifiers to indicate special circumstances.
Modifier 25: Significant, Separately Identifiable E/M on Same Day as Procedure
Modifier 25 is appended to CPT code 99213 when a significant, separately identifiable E/M service is performed on the same day as a minor procedure by the same provider. The E/M service must address a problem or complexity beyond the routine pre- and post-procedure work bundled into the procedure code. Append modifier 25 to the 99213 CPT code and ensure documentation clearly distinguishes the E/M work from the procedure-related work.
Modifier 24: Unrelated E/M During Post-Op Global Period
Modifier 24 is appended to CPT code 99213 when the established patient visit is unrelated to a prior surgical procedure and occurs during that procedure’s postoperative global period. Append modifier 24 and document that the condition addressed during the visit is clinically unrelated to the surgery, to support separate reimbursement for procedure code 99213 despite the active global period.
Modifier 95: Synchronous Telehealth Service
Modifier 95 is appended to CPT code 99213 to indicate the visit was conducted via real-time, interactive audio and video telecommunications technology. Modifier 95 is the most widely accepted telehealth modifier across Medicare and commercial payers for code 99213 CPT delivered via live video visit, paired with the appropriate POS code (02 or 10).
Modifier FS: Split or Shared E/M Visit
Modifier FS is appended to CPT code 99213 when the visit is performed as a split (or shared) E/M service between a physician and a non-physician practitioner in a facility setting, where both providers from the same group jointly perform the visit. Modifier FS identifies that the substantive portion of the visit, defined by CMS as either more than half of the total time or the performance of the MDM, was performed by the billing practitioner. Append modifier FS to procedure code 99213 when billing a split/shared visit in an institutional setting.
Modifier GQ: Asynchronous Telehealth Service
Modifier GQ is appended to CPT code 99213 to indicate the service was delivered via an asynchronous (store-and-forward) telecommunications system, an interaction in which information is transmitted for review at a later time rather than in real time. Modifier GQ has historically been limited to use under federal telemedicine demonstration programs in Alaska and Hawaii. Providers outside these programs should verify with their MAC whether modifier GQ is applicable before appending it to the 99213 CPT code, as most payers require synchronous (modifier 95) telehealth for established patient E/M visits.
Which Documents Are Required For CPT Code 99213?
Documentation for CPT code 99213 must support either the MDM pathway or the total-time pathway, and must reflect medically appropriate history and examination.
Required documents checklist:
- Chief complaint and history of present illness relevant to the visit
- Medically appropriate review of systems and physical examination findings
- Documentation of the number and status of problems addressed (e.g., stable chronic illness, minor self-limited problem, acute uncomplicated illness)
- Documentation of data reviewed. Results of one or two unique tests, limited external record review, or use of an independent historian
- Documentation of risk, over-the-counter medication recommendations, or minor treatments without significant risk factors
- Assessment and plan reflecting the medical decision-making for each problem addressed
- If billing under the time pathway: total time spent on the date of encounter, with a description of activities performed
- If telehealth: documentation of the technology platform used, patient location, and confirmation of synchronous audio-video communication
- If split/shared visit: documentation identifying which provider performed the substantive portion of the visit
What is the Cost of CPT Code 99213?
The cost of CPT code 99213 varies by place of service, payer, geographic location, and whether the billing provider is a Qualifying APM Participant (QP).
RVUs & Medicare Payment
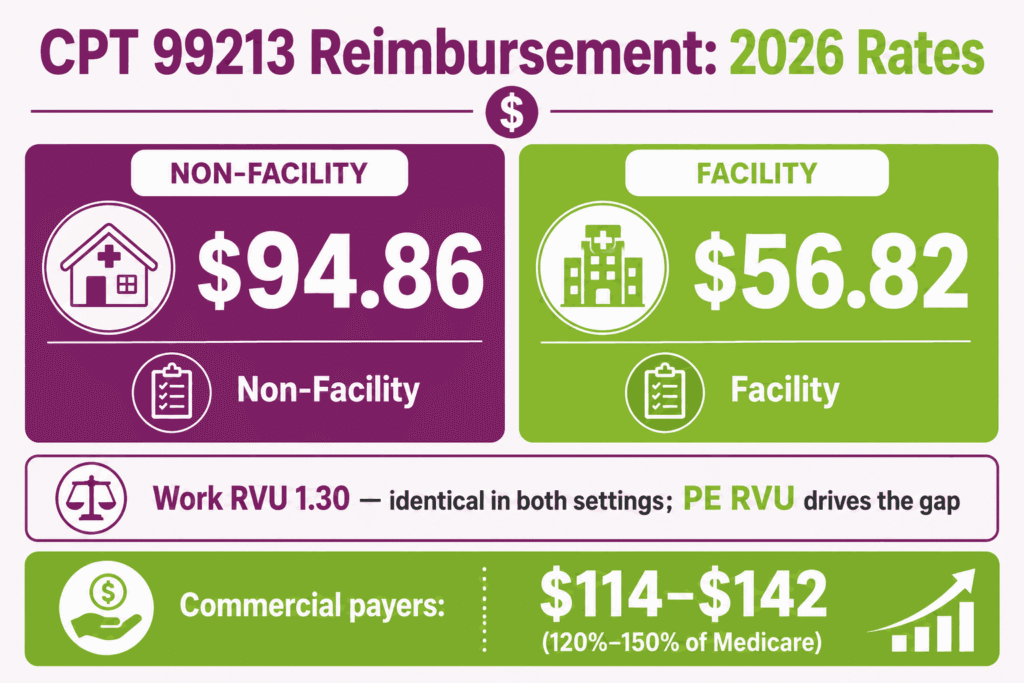
Reimbursement for CPT code 99213 is driven by a precise formula multiplying relative value weights by the standard 2026 non-QP conversion factor of $33.4009. The Work RVU (wRVU) is locked at 1.30, completely shielded from the -2.5% efficiency cuts that impacted radiology and surgical specialties.
In an office setting, the Total Non-Facility RVU has increased to 2.84, bringing the unadjusted national payment to $94.86. Conversely, due to a severe 2026 reduction in indirect facility practice expenses, the Total Facility RVU dropped to 1.70, driving the institutional physician fee down to $56.82.
Commercial Payers
Commercial health plans typically align their fee structures between 120% and 150% of the Medicare schedule, resulting in market allowable rates of $114 to $142 for an office encounter. In 2026, private payers are heavily auditing high-volume 99213 usage to verify compliance with the 20-minute threshold when billing strictly by time.
Additionally, commercial networks have widely implemented the dual conversion factor model, meaning non-participating providers who fail to enter value-based tracks face stagnant commercial updates compared to those in Advanced APMs.
Place-of-Service & Geographic Adjustments
The finalized payment is further modified by the Geographic Practice Cost Index (GPCI), which causes the base rate to climb significantly in high-overhead metropolitan hubs to match regional labor and real estate costs. Furthermore, the Place of Service (POS) choice drastically dictates the revenue split.
In an independent practice (POS 11), the provider collects the maximum $94.86 allowance to absorb all clinical overhead. If the exact same evaluation takes place within a hospital outpatient department (POS 22), the physician’s payout is capped at $56.82, while the hospital system separately bills an institutional facility fee to offset its own programmatic costs.
What Are Example Clinical Scenarios or Use Cases for CPT Code 99213?
CPT code 99213 applies to established patient visits involving low-complexity medical decision making or 20–29 minutes of total time, commonly involving stable chronic disease follow-up, minor acute illnesses, or routine rechecks without medication changes.
Scenario 1: Acute Upper Respiratory Infection With Symptomatic Treatment Plan
ICD-10: J06.9 (Acute upper respiratory infection, unspecified)
An established patient presents with nasal congestion, sore throat, and mild cough for three days, with no fever and no signs of bacterial infection on examination. The physician addresses one acute, uncomplicated illness (problem addressed), performs a focused exam without ordering tests (minimal data), and recommends over-the-counter decongestants and rest (low risk). This meets low MDM in at least two of three elements, supporting CPT code 99213.
Scenario 2: Stable Hypothyroidism Follow-Up With TSH Review and Dose Adjustment
ICD-10: E03.9 (Hypothyroidism, unspecified)
An established patient with hypothyroidism, stable on levothyroxine, presents for routine follow-up. The physician reviews the recent TSH result, which is within the target range (data reviewed with one unique test). This confirms the patient remains stable on the current dose (one stable chronic illness, problem addressed), and continues the current regimen without adjustment (low risk, no prescription change). CPT code 99213 is reported.
Scenario 3: Controlled Hypertension Recheck With No Medication Changes Required
ICD-10: I10 (Essential hypertension)
An established patient with hypertension returns for a routine blood pressure recheck. Home readings and the in-office reading are within the patient’s target range. The physician addresses one stable chronic illness (problem addressed), reviews the patient’s home BP log (data reviewed), and continues the current antihypertensive regimen without any dosage change or new prescription (low risk). Procedure code 99213 is reported, as no prescription drug management decision was made during this visit.
Scenario 4: Minor Skin Condition Follow-Up With Topical Treatment Modification
ICD-10: L30.9 (Dermatitis, unspecified)
An established patient returns for follow-up of a mild contact dermatitis previously treated with an over-the-counter hydrocortisone cream. The rash has partially improved. The physician addresses one self-limited problem (problem addressed), performs a brief visual examination (minimal data), and recommends continuing the over-the-counter topical treatment with minor application adjustments (low risk, no prescription medication involved). CPT code 99213 is reported.
What Are the CPT Code 99213 Rules To Ensure Successful Reimbursement?
Follow CMS and payer rules for bundling, frequency, code-level accuracy, and split/shared billing. Meeting these rules reduces denials and supports defensible coding for the 99213 CPT code, highlighting the importance of CPT codes and insurance billing.
Bundling / NCCI / Same-Day Procedure Rules
CPT code 99213 may be billed alongside a minor procedure on the same date only when a significant, separately identifiable E/M service is performed and modifier 25 is appended. If the E/M work is limited to the routine pre- and post-procedure assessment bundled into the procedure code, procedure code 99213 must not be separately reported.
NCCI edits will bundle CPT 99213 code with same-day procedures absent modifier 25 and supporting documentation demonstrating a distinct, medically necessary E/M service beyond the procedure’s inherent evaluation component.
Units, MUEs & E/M Frequency Rules
CPT code 99213 is billed as one unit per patient per day. Medicare’s MUE for this code is 1. Per CMS policy:
- Only one E/M visit per patient per day may be billed by the same provider or group/specialty, except when modifier 25 supports a separately identifiable second E/M or procedure
- CPT code 99213 carries a 0-day global period (XXX). There is no global surgical package associated with this code, and it may be billed independently of any procedure’s global period using modifier 24 when applicable
- Established patient status must be verified. The patient must have received a professional service from the same physician or a physician of the same specialty in the same group within the past three years; otherwise, the appropriate new patient code (99203) applies
When to Upgrade From CPT 99213 to 99214 and Avoiding Downcoding Risk
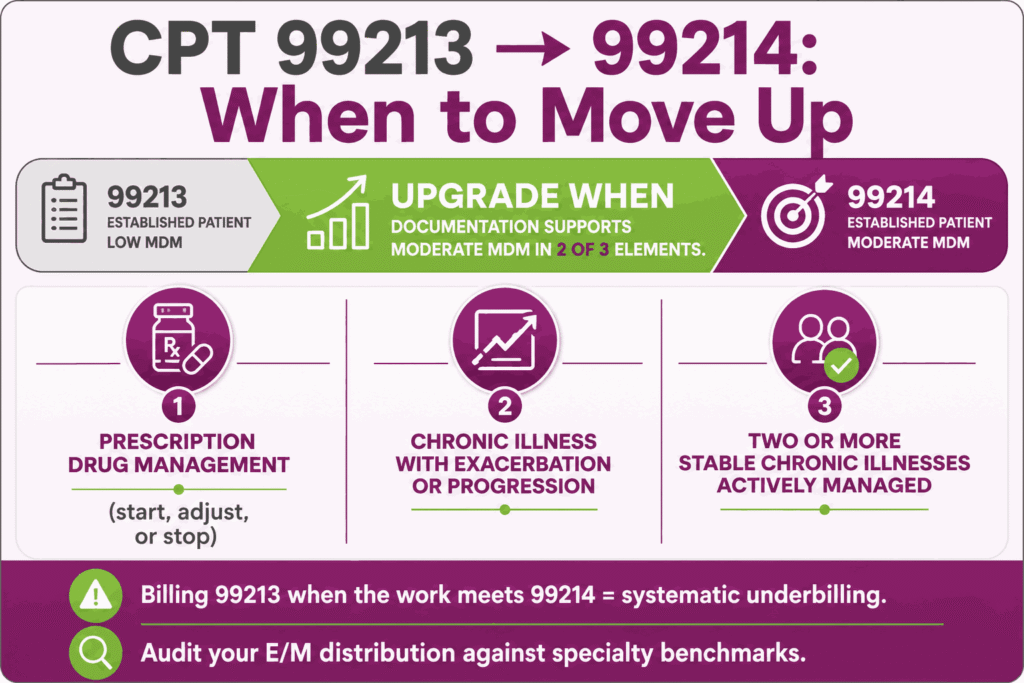
CPT code 99213 is frequently the subject of both upcoding and downcoding scrutiny. The visit should be upgraded to CPT 99214 when documentation supports moderate MDM in at least two of the three elements. Most commonly triggered by prescription drug management (initiating, continuing with dose adjustment, or discontinuing a prescription medication), a chronic illness with exacerbation or progression, or two or more stable chronic illnesses being actively managed.
Conversely, downcoding risk arises when a visit that genuinely meets moderate MDM criteria. For example, an active medication dose change for a chronic condition is billed as procedure code 99213 out of caution. This results in systematic underbilling relative to the work performed.
Practices should periodically audit their E/M code distribution against specialty-specific benchmarks. A 99213-heavy distribution relative to peers may indicate either appropriately lower-acuity patient mix or a pattern of defensive downcoding that should be reviewed against actual documentation. Periodic E/M distribution audits against specialty benchmarks catch both patterns, which is why many practices route coding review through professional medical billing services.
Split/Shared Visit Rules and Teaching Physician Requirements
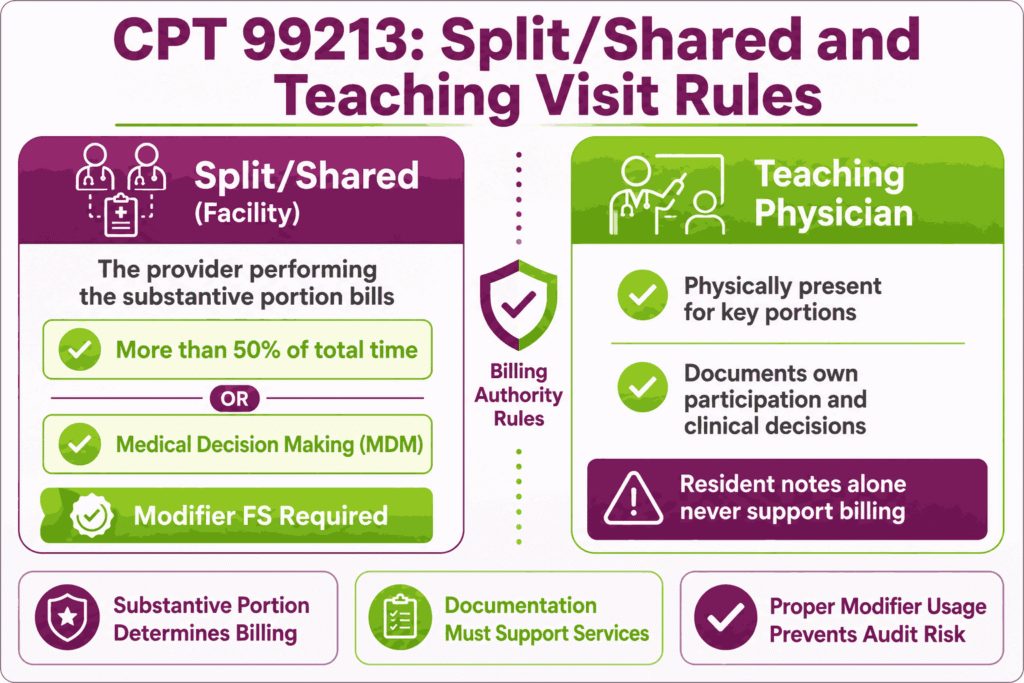
When CPT code 99213 is performed as a split (or shared) visit between a physician and a non-physician practitioner in a facility setting, CMS requires that the “substantive portion” of the visit, which is defined as either more than half of the total time spent or the performance of the medical decision making. This portion determines which provider bills the service.
Modifier FS is appended to identify the visit as split/shared. The billing provider (physician or NPP) must be identified based on who performed the substantive portion, and documentation must clearly attribute the relevant time or MDM components to that provider.
For teaching physician settings, CPT code 99213 billed under a resident’s involvement requires the teaching physician to be physically present for the key portions of the service and to document their own participation, findings, and management decisions. A resident’s documentation alone, even if thorough, does not support billing under the teaching physician’s NPI without the required attestation.
Top Reasons For Denials Specific To 99213 & Quick Remedies
- Insufficient MDM Documentation to Support Even Low Complexity: Prevent by ensuring the assessment and plan documents at least two of the three MDM elements at the low level, problem complexity, data reviewed, and risk, with specific clinical detail rather than generic statements.
- Time-Based Billing Without Adequate Time Documentation: Prevent by documenting the total minutes spent on the date of the encounter, along with a description of the activities performed, when billing under the 20–29 minute time pathway.
- Modifier 25 Used Without Separately Identifiable E/M Documentation: Prevent by ensuring the note clearly distinguishes the E/M service from the routine pre/post work of any same-day procedure before appending modifier 25 to CPT code 99213.
- Telehealth Claims Rejected for POS/Modifier Mismatch: Prevent by confirming modifier 95 is paired with the correct POS code (10 for patient at home, 02 for other locations) and that the documentation confirms synchronous audio-video technology was used.






