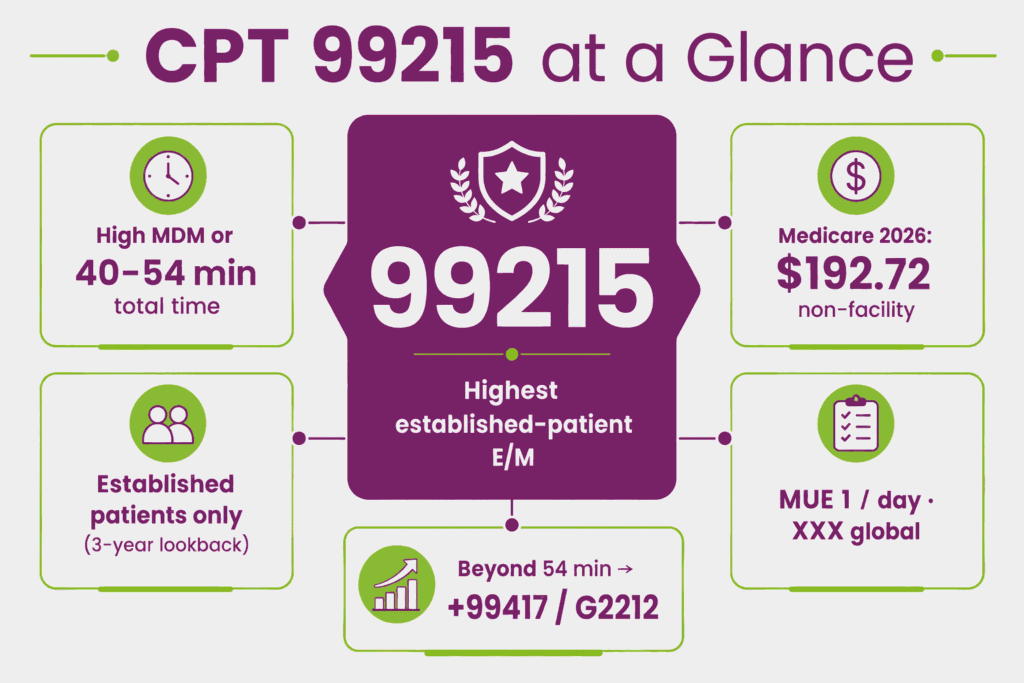
CPT code 99215 is an evaluation and management code used to report an office or outpatient visit for an established patient that requires either high-complexity medical decision making or 40–54 minutes of total time on the date of the encounter. Procedure code 99215 represents the highest-level established patient office visit code.
This E/M process code is reserved for patients with severe exacerbations of chronic conditions, multiple high-risk comorbidities, or management decisions involving significant risk to life or bodily function. Under the 2021 AMA E/M guidelines, code 99215 CPT may be selected based on either MDM or total time. History and physical exam no longer determine the code level, though they must remain medically appropriate to the visit.
What Is the Description of CPT Code 99215?
99215 CPT code description as defined by the AMA is: “Office or other outpatient visit for the evaluation and management of an established patient, which requires a medically appropriate history and/or examination and high level of medical decision making. When using total time on the date of the encounter for code selection, 40-54 minutes of total time is spent on the date of the encounter.”
99215 CPT code applies only to established patients. The ones who have received professional services from the physician or another physician of the same specialty in the same group practice within the past three years. Comparable-complexity new patient visits are reported under the CPT 99205 code.
What Are the Two Pathways to Qualify for CPT Code 99215: MDM vs. Total Time?
Per the 2021 AMA E/M guidelines, CPT code 99215 may be selected using either of two independent pathways:
- Medical Decision Making (MDM) Pathway: The visit qualifies for procedure code 99215 when the overall MDM level reaches “high” complexity, based on the three MDM elements (problems addressed, data reviewed, and risk). History and examination are performed as medically appropriate, but do not determine the code level.
- Total Time Pathway: The visit qualifies for CPT code 99215 when the physician or qualified health care professional spends 40–54 minutes of total time on the date of the encounter, regardless of the MDM level. Total time includes both face-to-face and non-face-to-face time personally spent by the billing provider on the date of the encounter. This includes pre-visit chart review, history-taking, examination, counseling, ordering, documentation, and care coordination.
Only one pathway needs to be met. A visit reaching high MDM but with shorter time spent, or a lengthy visit with lower MDM, may still qualify for code 99215 CPT under whichever pathway is satisfied.
What Are the Three Elements of High Medical Decision Making for CPT Code 99215?
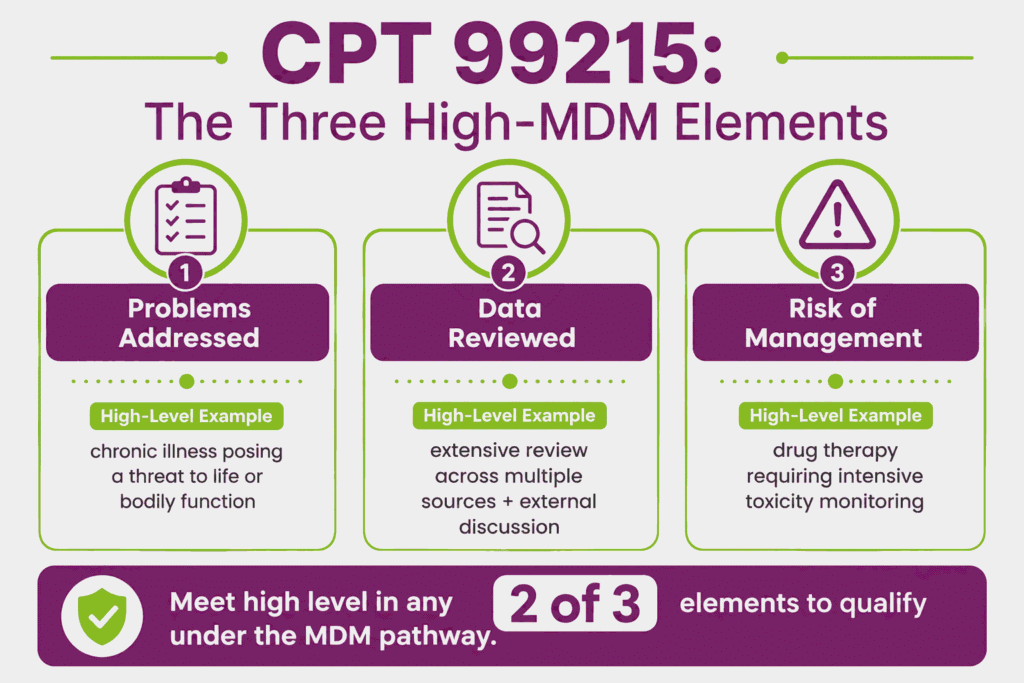
High MDM supporting CPT code 99215 is determined by meeting or exceeding the high level in at least two of the following three elements:
- Number and Complexity of Problems Addressed: Typically reflects one or more chronic illnesses with severe exacerbation, progression, or side effects of treatment, or a chronic illness or injury that poses a threat to life or bodily function
- Amount and/or Complexity of Data Reviewed and Analyzed: Typically reflects extensive review and analysis of data from multiple sources. Combinations of test ordering/review, independent test interpretation, and discussion of management with external physicians or other qualified sources
- Risk of Complications, Morbidity, or Mortality of Patient Management: Typically reflects drug therapy requiring intensive monitoring for toxicity, decision regarding elective major surgery with identified patient or procedure risk factors, decision regarding emergency major surgery, decision regarding hospitalization, or a decision not to resuscitate or to de-escalate care because of poor prognosis
Meeting high-level criteria in at least two of the three elements supports CPT code 99215 under the MDM pathway. The “risk” element most commonly distinguishing 99215 from the E/M code 99214 is the drug therapy requiring intensive toxicity monitoring (e.g., warfarin with INR monitoring, certain immunosuppressants), which is a frequently cited example supporting the high-risk threshold.
How Much Total Time Is Required for CPT Code 99215 Under the Time-Based Pathway?
Under the time-based pathway, CPT code 99215 requires 40–54 minutes of total time spent by the billing physician or qualified health care professional on the date of the encounter. This is the upper-bound code in the established patient E/M family. There is no higher-level established patient office visit code.
When total time exceeds 54 minutes, prolonged service add-on codes such as the CPT code 99417 or G2212 apply rather than a higher base E/M code. Total time must be personally performed by the billing provider and clearly documented, including the total minutes spent and a description of the activities performed. Time spent by clinical staff is not counted toward the billing provider’s total time for procedure code 99215.
How Does CPT Code 99215 Differ From CPT 99214 and New Patient Code 99205?
These codes are distinguished by patient status, MDM level, and total time:
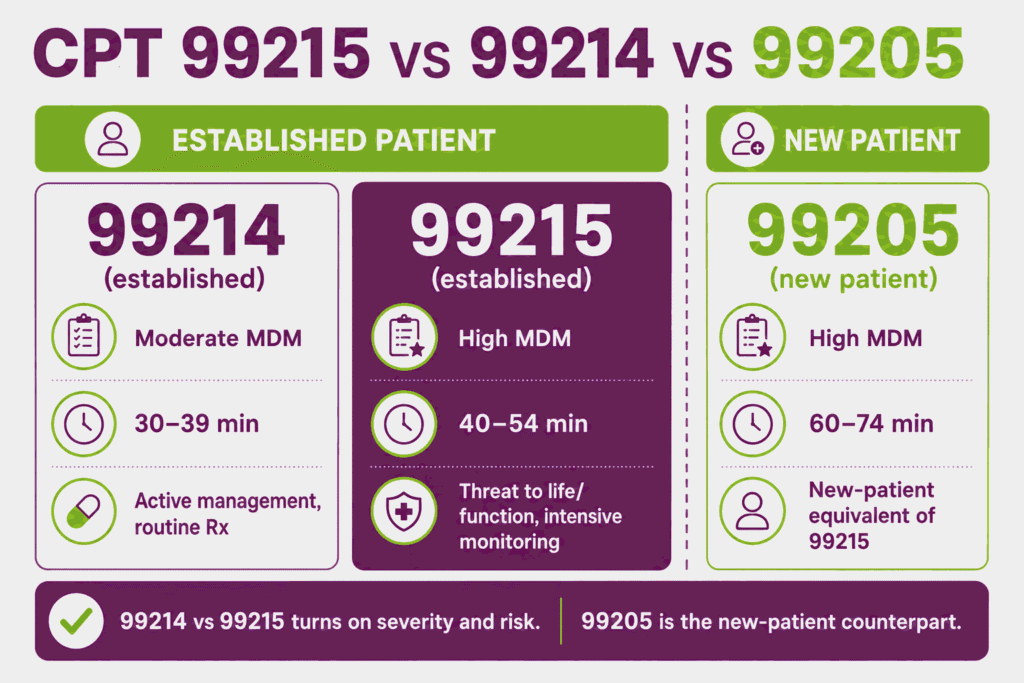
- CPT Code 99214: Moderate-complexity MDM or 30–39 minutes total time. Used for established patients with chronic conditions requiring active management or prescription drug management without intensive monitoring requirements
- CPT Code 99215: High-complexity MDM or 40–54 minutes total time. Used for established patients with severe exacerbations, conditions threatening life or bodily function, or drug therapy requiring intensive toxicity monitoring
- CPT Code 99205: The new patient equivalent of the 99215 CPT code. Used when the patient has not received professional services from the physician or a same-specialty physician in the same group within the past three years, with comparable high-complexity MDM or 60–74 minutes total time (note the longer time threshold reflecting the additional work of a new patient encounter)
The defining distinction between 99214 and procedure code 99215 is typically the severity and risk dimension. A chronic illness that is merely “exacerbated” (99214) versus one that “poses a threat to life or bodily function” (99215), or prescription management (99214) versus drug therapy requiring intensive monitoring for toxicity (99215).
When Should CPT 99417 or G2212 Be Added for Prolonged Services Beyond 54 Minutes?
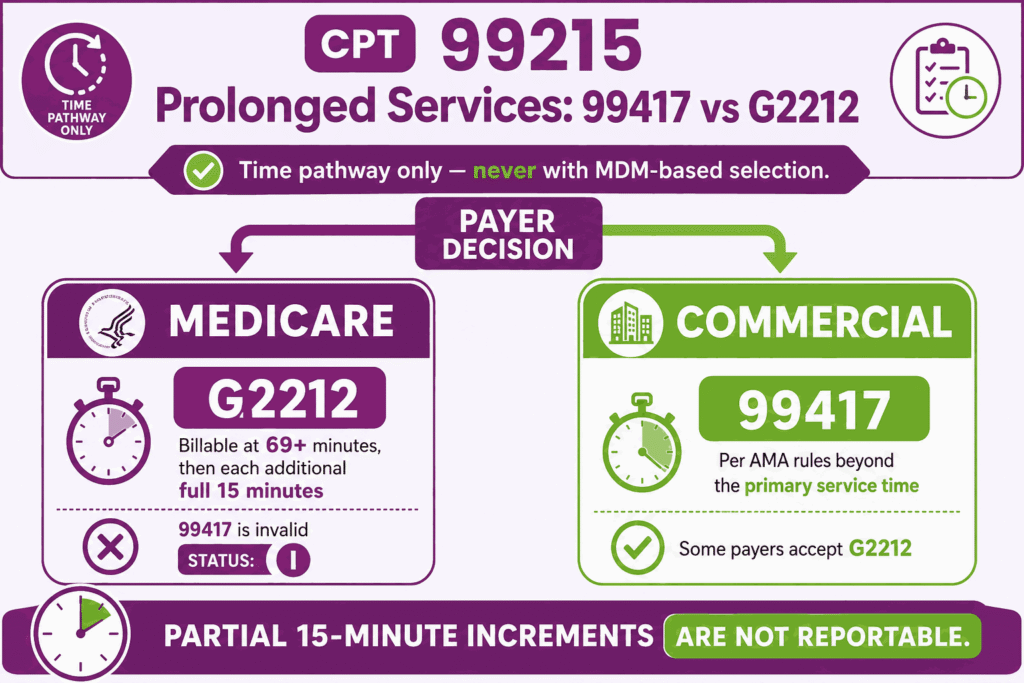
When total time on the date of the encounter exceeds the 54-minute maximum for CPT code 99215, prolonged service add-on codes may be reported, but the correct code depends on the payer:
Per Noridian MAC (citing CMS IOM Publication 100-04, Chapter 12, §30.6.15), CPT code 99417 carries Medicare status indicator “I” and is not valid for Medicare billing. For Medicare, HCPCS code G2212 is the correct add-on code, reportable only when the total time exceeds the maximum time for 99215 (54 minutes) by at least 15 minutes. This means G2212 becomes billable starting at 69 minutes of total time, and again for each additional full 15-minute increment thereafter. Partial 15-minute increments are not reportable.
For commercial payers following AMA CPT guidelines, the CPT 99417 code is the correct prolonged service add-on code, reported in conjunction with CPT code 99215 when total time exceeds the typical time of the primary service by 15 minutes or more. Some commercial payers may also accept G2212. So, verify payer-specific policy.
Prolonged service add-on codes apply only when CPT code 99215 is selected using the total-time pathway. If the code level was selected based on MDM rather than time, neither 99417 nor G2212 may be reported, regardless of how much additional time was spent.
Why CPT Code 99215 Is Restricted to Established Patients Only
CPT code 99215 is part of the established patient office visit code family (99211–99215) and cannot be billed for a patient being seen by the practice for the first time. The AMA defines an established patient as one who has received professional services from the physician or qualified health care professional, or another physician or qualified health care professional of the same specialty in the same group practice, within the past three years.
If the three-year lookback finds no qualifying prior encounter, the visit must be reported using the corresponding new patient code 99205. That code carries a higher work RVU and a longer time threshold (60–74 minutes) reflecting the additional work of establishing a new patient record and comprehensive history. Billing procedure code 99215 for a new patient or vice versa is a documented compliance and audit risk.
How Does CPT 99215 Differ From Transitional Care Management Code 99496?
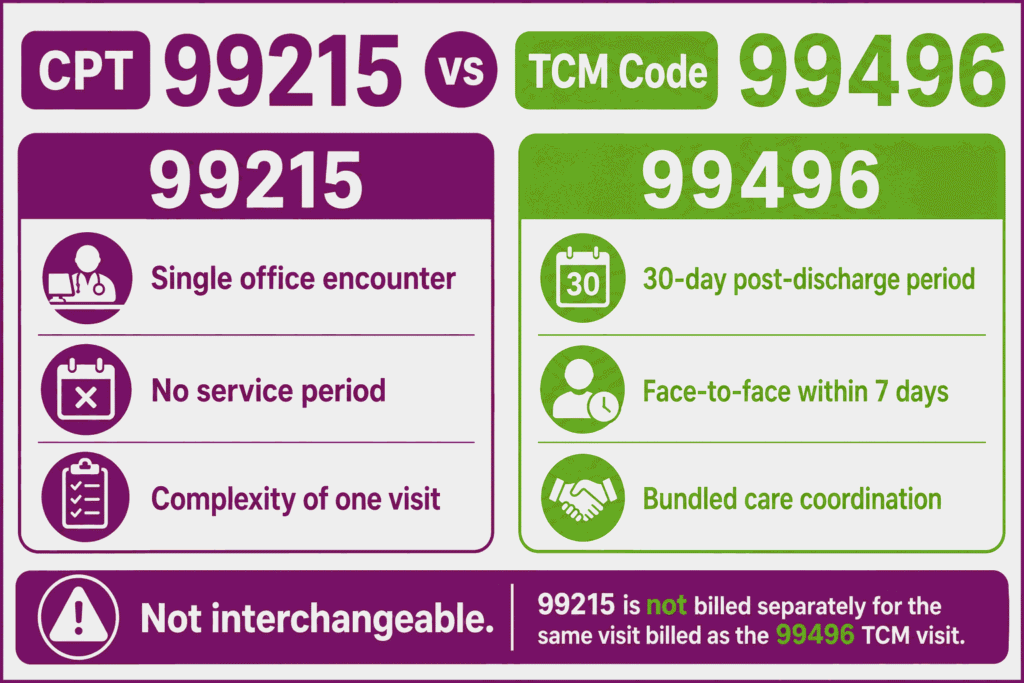
CPT code 99496 is a high-complexity Transitional Care Management (TCM) code. It is used to report the management of a patient’s care during the 30-day period following discharge from an inpatient hospital, observation, or skilled nursing facility stay, requiring a face-to-face visit within 7 calendar days of discharge.
CPT 99496 code is a bundled service that includes non-face-to-face care coordination activities (medication reconciliation, communication with the patient and other providers, referrals) in addition to the required face-to-face visit, all reported as a single code for the 30-day period.
CPT code 99215, by contrast, is a single-encounter E/M code reflecting the complexity of one office visit, with no bundled 30-day service period and no discharge-related requirement. If a patient is seen within 7 days of hospital discharge and TCM criteria are met, 99496 may be the more appropriate and more highly valued code.
However, the two codes are not interchangeable, and procedure code 99215 is not reported separately for the same face-to-face visit that is being billed as the required TCM visit under 99496.
Can CPT 99215 Be Billed by Non-Physician Practitioners Under Incident-To Rules?
Yes, CPT code 99215 may be billed by non-physician practitioners (NPPs). These include nurse practitioners and physician assistants. They use either under their own NPI at the standard NPP payment rate (typically 85% of the physician fee schedule for Medicare), or under “incident-to” billing rules at 100% of the physician rate when all incident-to requirements are met.
Incident-to billing for procedure code 99215 requires that the service be part of a course of treatment initiated by the supervising physician. Plus, the supervising physician must be physically present in the office suite at the time the service is rendered, and the visit must not involve a new problem requiring independent physician evaluation.
Given the high-complexity nature of visits qualifying for CPT code 99215, practices should carefully assess whether the visit truly meets the incident-to criteria. The reason being high-risk visits often involve new problems or significant management decisions that may exceed the scope of incident-to billing.
What Are the Telehealth Billing Rules for CPT Code 99215?
CPT code 99215 remains on the Medicare telehealth services list and may be billed for visits delivered via real-time telecommunications technology. Per current 2026 telehealth billing guidance, Medicare beneficiaries can receive telehealth services from any location through December 31, 2027:
- Modifier 95 is appended to CPT code 99215 for synchronous audio-video telehealth visits, paired with Place of Service 02 (other location) or POS 10 (patient’s home)
- Modifier 93 is appended for synchronous audio-only telehealth visits where the payer permits audio-only billing for the 99215 CPT code
- The visit must still meet either the high MDM or 40–54 minute total-time requirement for CPT code 99215, regardless of delivery modality, and documentation must reflect the technology platform used and confirm the encounter was conducted via live communication
- Given the complexity threshold required for procedure code 99215, documentation for telehealth visits at this level must be especially thorough. Payers scrutinize high-level telehealth E/M claims for whether the complexity genuinely warranted the highest code level in a remote setting
Telehealth policy for E/M codes changes based on Congressional extensions of Medicare telehealth flexibilities. Providers should verify current-year telehealth eligibility for the 99215 CPT code with their MAC before billing.
What are the Modifiers for CPT code 99215?
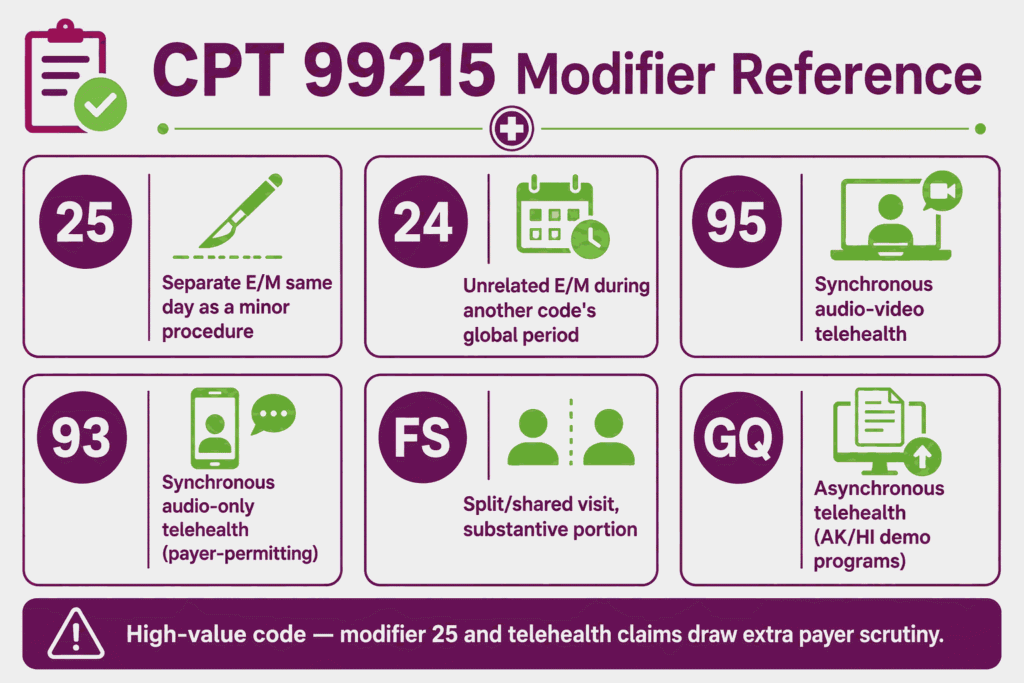
CPT code 99215 may be reported with modifiers that clarify same-day procedures, unrelated post-op care, telehealth delivery, or when the visit led to a decision for surgery.
Modifier 25: Significant, Separately Identifiable E/M on Same Day as Procedure
Modifier 25 is appended to CPT code 99215 when a significant, separately identifiable E/M service is performed on the same day as a minor procedure by the same provider. The E/M service must address a problem or complexity beyond the routine pre- and post-procedure work bundled into the procedure code. Given the high complexity required for 99215 CPT code, documentation must clearly demonstrate that the E/M work, not just the procedure’s inherent evaluation, independently meets the high MDM or time threshold.
Modifier 24: Unrelated E/M During Post-Op Global Period
Modifier 24 is appended to CPT code 99215 when the established patient visit is unrelated to a prior surgical procedure and occurs during that procedure’s postoperative global period. Append modifier 24 and document that the condition addressed during the visit is clinically unrelated to the surgery, to support separate reimbursement for procedure code 99215 despite the active global period.
Modifier 95: Synchronous Telehealth Service (Audio-Video)
Modifier 95 is appended to CPT code 99215 to indicate the visit was conducted via real-time, interactive audio and video telecommunications technology. Modifier 95 is paired with the appropriate POS code (02 or 10) for telehealth delivery of code 99215 CPT.
Modifier 93: Synchronous Telehealth Service (Audio-Only)
Modifier 93 is appended to CPT code 99215 to indicate the visit was conducted via real-time audio-only telecommunications technology, without video. Append modifier 93 to procedure code 99215 only when the payer’s telehealth policy permits audio-only billing for high-level established patient E/M visits. Verify before submission, as audio-only coverage policy varies by payer and has historically been more restricted for higher-complexity E/M codes.
Modifier FS: Split or Shared E/M Visit
Modifier FS is appended to CPT code 99215 when the visit is performed as a split (or shared) E/M service between a physician and a non-physician practitioner in a facility setting, where both providers from the same group jointly perform the visit. Modifier FS identifies that the substantive portion of the visit, as defined by CMS as either more than half of the total time or the performance of the MDM, was performed by the billing practitioner. Given the high-complexity threshold for 99215 CPT code, documentation should clearly establish which provider performed the high-risk decision-making component.
Modifier GQ: Asynchronous Telehealth Service
Modifier GQ is appended to CPT code 99215 to indicate the service was delivered via an asynchronous (store-and-forward) telecommunications system. Modifier GQ has historically been limited to use under federal telemedicine demonstration programs in Alaska and Hawaii. Providers outside these programs should verify with their MAC whether modifier GQ is applicable before appending it to procedure code 99215, as most payers require synchronous (modifier 95 or 93) telehealth for established patient E/M visits, and the high complexity required for 99215 makes asynchronous delivery clinically uncommon.
Which Documents Are Required For CPT Code 99215?
Documentation for CPT code 99215 must support either the high MDM pathway or the 40–54 minute total-time pathway, and must reflect medically appropriate history and examination commensurate with the visit’s complexity.
Required documents checklist:
- Chief complaint and history of present illness reflecting the severity of the condition(s) addressed
- Medically appropriate review of systems and physical examination findings consistent with high-acuity presentation
- Documentation of the number and status of problems addressed, specifically identifying severe exacerbation, progression, or threat to life or bodily function
- Documentation of extensive data review. Multiple unique tests, independent test interpretation, and/or discussion of management with external physicians or other qualified sources
- Documentation of high risk, specifically identifying drug therapy requiring intensive toxicity monitoring, decisions regarding major surgery, hospitalization decisions, or de-escalation of care decisions
- Assessment and plan reflecting the clinical reasoning for each high-complexity decision made
- If billing under the time pathway: total time spent on the date of encounter (40–54 minutes) with a description of activities performed
- If prolonged services apply: documentation of total time exceeding 54 minutes and selection of the time-based pathway, supporting G2212 (Medicare, at 69+ minutes) or 99417 (commercial, per payer policy)
- If telehealth: documentation of the technology platform used (audio-video or audio-only), patient location, and confirmation of synchronous communication
- If split/shared visit: documentation identifying which provider performed the substantive portion of the visit, including the high-risk decision-making component
What is the Cost of CPT Code 99215?
The cost of CPT code 99215 varies by place of service, payer, geographic location, and whether the billing provider is a Qualifying APM Participant (QP).
RVUs & Medicare Payment
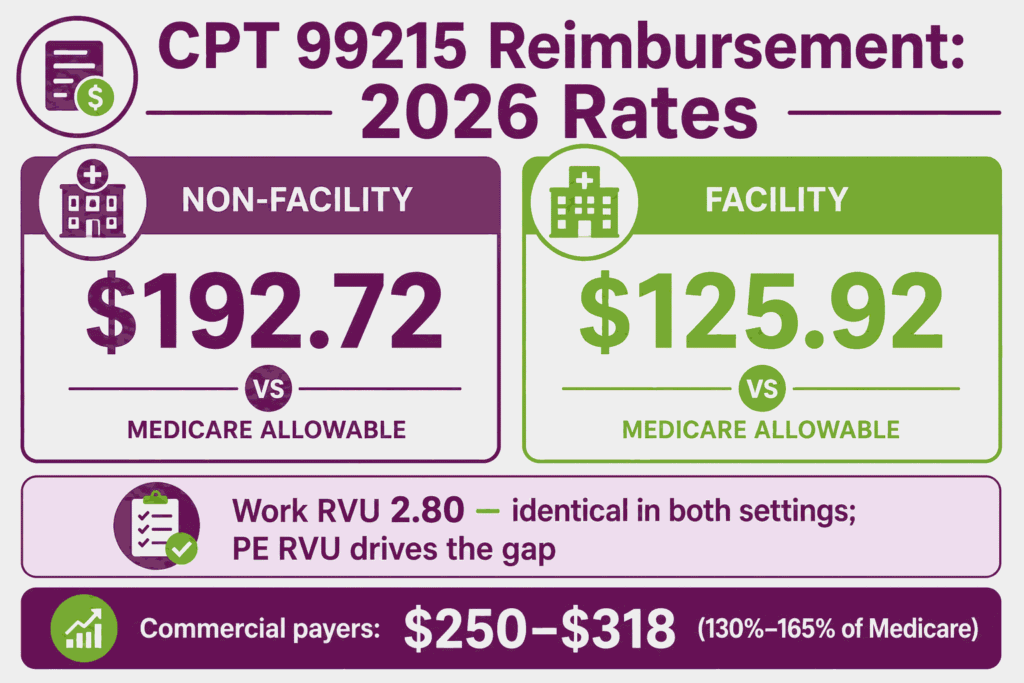
Medicare calculates reimbursement for CPT code 99215 by compounding work intensity, liability risk, and physical overhead. For 2026, the Work RVU (wRVU) is held firmly at 2.80, recognizing the intense cognitive workload required to manage severe or unstable conditions. RVU weighting and the annual conversion factor set the baseline for reimbursement of E/M CPT codes across the office visit family before payer adjustments.
To combat private practice inflation, CMS substantially escalated the non-facility practice expense allocation, pushing the Total Non-Facility RVU up to 5.77. Multiplied by the standard 2026 conversion factor of $33.4009, the national unadjusted office payout is $192.72. In contrast, because the clinical overhead is absorbed by the institution rather than the physician, the Total Facility RVU settles at 3.77, yielding a professional fee of $125.92.
Commercial Payers
Commercial health insurance networks typically price the 99215 CPT code at 130% to 165% of the standard Medicare baseline, resulting in regional market allowable rates ranging between $250 and $318 for a single office encounter. Because this code represents a top-tier primary and specialty care expense, private carriers in 2026 are heavily auditing documentation thresholds.
If a practice selects this code level based on time rather than medical decision-making (MDM), failure to explicitly document a minimum of 40 minutes of total provider care on the exact date of the encounter will spark an automated downcode to a 99214, creating immediate revenue leakage.
Place-of-Service & Geographic Adjustments
CPT code 99215 carries substantially different payment rates by place of service. Furthermore, the Place of Service (POS) defines the distribution of payment. In an independent or private practice setting (POS 11), the group captures the full $192.72 global allowance to satisfy their operational overhead.
If the encounter occurs within an institutional environment like a hospital outpatient clinic (POS 22), the physician collects the lower professional allocation of $125.92, leaving the hospital system to file a separate institutional claim to offset space and support staff pricing.
What Are Example Clinical Scenarios or Use Cases for CPT Code 99215?
CPT code 99215 applies to established patient visits involving high-complexity medical decision making or 40–54 minutes of total time. This commonly involves severe exacerbations of chronic conditions, drug therapy requiring intensive toxicity monitoring, or decisions involving significant risk to life or bodily function.
Scenario 1: Acute-on-Chronic Systolic Heart Failure With Volume Status Reassessment
ICD-10: I50.23 (Acute on chronic systolic (congestive) heart failure)
An established patient with chronic systolic heart failure presents with worsening dyspnea, lower extremity edema, and a 5-pound weight gain over one week. The physician addresses a chronic illness with severe exacerbation posing risk of hospitalization (problem addressed, high), reviews recent BNP labs, an EKG, and a chest X-ray, and discusses findings with the patient’s cardiologist (data reviewed, extensive), and makes the decision to intensify diuretic therapy with close outpatient monitoring as an alternative to hospitalization, while documenting the hospitalization decision considered (risk, high). This meets high MDM in at least two of three elements, supporting CPT code 99215.
Scenario 2: Multiple Chronic Conditions With Severe Exacerbation Requiring Urgent Treatment Changes
ICD-10: E11.65 (Type 2 diabetes mellitus with hyperglycemia)
An established patient with type 2 diabetes, chronic kidney disease, and hypertension presents with a markedly elevated point-of-care glucose and new-onset blurred vision. The physician addresses multiple chronic illnesses, with the diabetes exacerbation posing a threat to bodily function (problem addressed, high), reviews point-of-care glucose, recent A1C, and renal function labs (data reviewed, extensive), and initiates urgent insulin therapy adjustment requiring close monitoring for hypoglycemia risk given the patient’s renal impairment (risk, high, drug therapy requiring intensive monitoring). Procedure code 99215 is reported.
Scenario 3: High-Risk Medication Management Requiring Extensive Data Review and Specialist Coordination
ICD-10: Z79.01 (Long term (current) use of anticoagulants)
An established patient on warfarin for a mechanical heart valve presents with an INR significantly outside the therapeutic range. The physician addresses a chronic condition where the medication itself poses a threat to life if mismanaged (problem addressed, high), reviews the INR trend, recent labs, and discusses the dose adjustment plan with the patient’s cardiologist (data reviewed, extensive, external discussion), and adjusts the warfarin dose with intensive INR monitoring instructions (risk, high, drug therapy requiring intensive toxicity monitoring). CPT code 99215 is reported.
Scenario 4: Complex Psychiatric Visit With Imminent Risk Assessment and Crisis Safety Planning
ICD-10: F33.2 (Major depressive disorder, recurrent severe without psychotic features)
An established patient with recurrent severe major depressive disorder presents with worsening symptoms and newly disclosed passive suicidal ideation without active plan. The physician addresses a chronic illness with severe exacerbation posing a threat to bodily function (problem addressed, high), conducts an extensive risk assessment incorporating review of the patient’s medication history and discussion with a covering crisis counselor (data reviewed, extensive), and develops a safety plan with close follow-up while considering. And documenting the rationale against a higher level of care (risk, high, decision regarding hospitalization considered). Procedure code 99215 is reported, supported by 45 minutes of total time spent on assessment, safety planning, and documentation.
What Are the CPT Code 99215 Rules To Ensure Successful Reimbursement?
Follow CMS and payer rules for bundling, frequency, code-level accuracy, and split/shared billing. Meeting these rules reduces denials and supports defensible coding for the 99215 CPT code.
Bundling / NCCI / Same-Day Procedure Rules
CPT code 99215 may be billed alongside a minor procedure on the same date only when a significant, separately identifiable E/M service is performed and modifier 25 is appended. If the E/M work is limited to the routine pre- and post-procedure assessment bundled into the procedure code, procedure code 99215 must not be separately reported.
NCCI edits will bundle CPT code 99215 with same-day procedures absent modifier 25 and supporting documentation demonstrating a distinct, medically necessary high-complexity E/M service beyond the procedure’s inherent evaluation component. Given the high reimbursement associated with 99215 CPT code, claims billing this code with modifier 25 alongside a same-day procedure are subject to elevated payer scrutiny.
Units, MUEs & E/M Frequency Rules
CPT code 99215 is billed as one unit per patient per day. Medicare’s MUE for this code is 1. Per CMS policy:
- Only one E/M visit per patient per day may be billed by the same provider or group/specialty, except when modifier 25 supports a separately identifiable second E/M or procedure
- CPT code 99215 carries a 0-day global period (XXX). There is no global surgical package associated with this code, and it may be billed independently of any procedure’s global period using modifier 24 when applicable
- Established patient status must be verified. The patient must have received a professional service from the same physician or a physician of the same specialty in the same group within the past three years. Otherwise, the appropriate new patient code (99205) applies
- Prolonged service add-on codes (G2212 for Medicare at 69+ minutes, 99417 for commercial payers) may only accompany procedure code 99215 when the time-based pathway was used for code selection
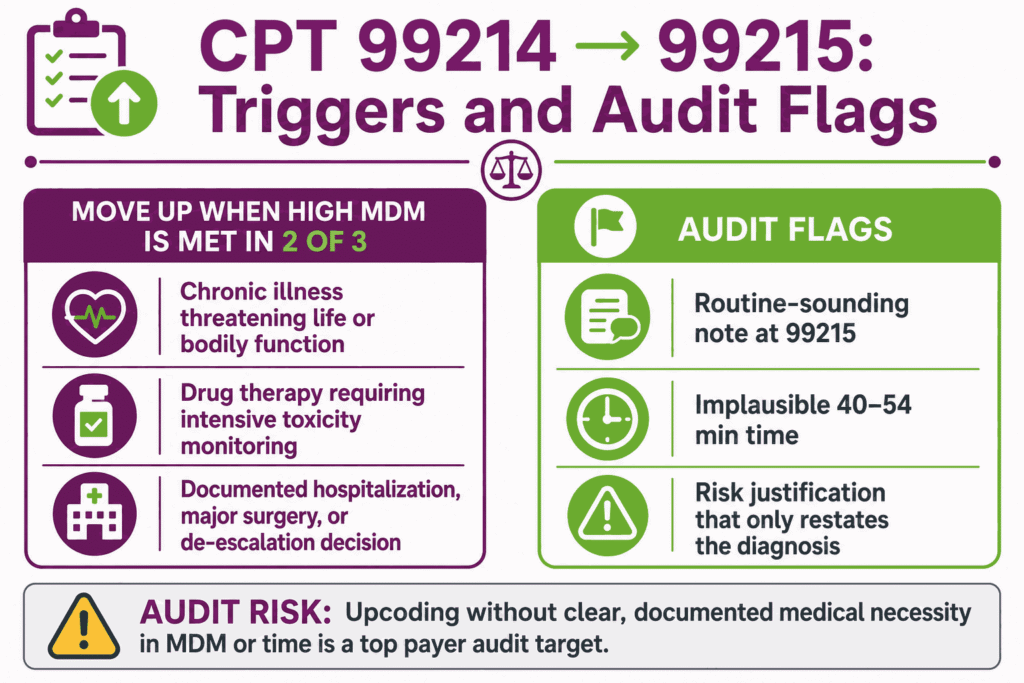
When to Upgrade From CPT 99214 to 99215 and Audit Risk of High-Frequency 99215 Billing
CPT code 99215 should be selected over CPT 99214 when documentation supports high MDM in at least two of the three elements. It is most commonly triggered by a chronic illness that poses a threat to life or bodily function (rather than merely an exacerbation), drug therapy requiring intensive toxicity monitoring (rather than routine prescription management), or a documented decision regarding hospitalization, major surgery, or de-escalation of care.
99215 CPT code is one of the most heavily audited E/M codes because it represents the highest payment in the established patient code family. Practices with a 99215 utilization rate significantly above specialty-specific benchmarks face elevated audit risk from Medicare contractors and commercial payers.
Common audit findings include documentation that describes a stable or routine visit while billing at the 99215 level, time documentation that does not plausibly support 40–54 minutes given the visit’s actual content. Plus, risk-element justifications that restate the diagnosis without describing the specific high-risk management decision made.
Conversely, genuinely high-complexity visits should not be systematically downcoded to 99214. Both directions of miscoding carry compliance and revenue implications, and documentation should drive code selection rather than the reverse.
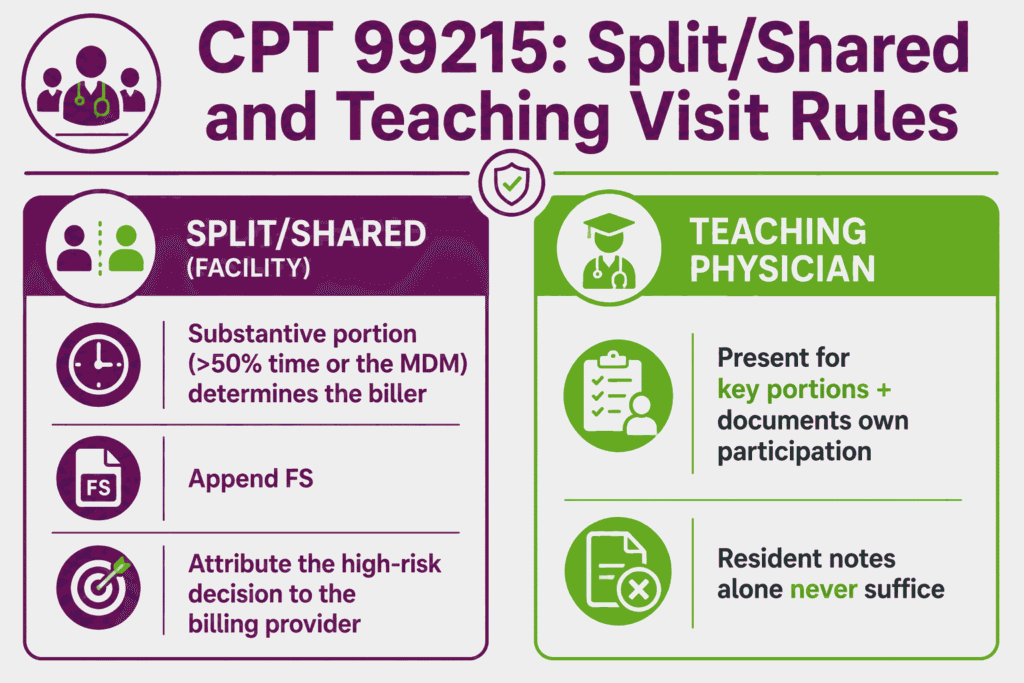
Split/Shared Visit Rules and Teaching Physician Requirements
When CPT code 99215 is performed as a split (or shared) visit between a physician and a non-physician practitioner in a facility setting. CMS requires that the “substantive portion” of the visit, defined as either more than half of the total time spent or the performance of the medical decision-making, determine which provider bills the service.
Modifier FS is appended to identify the visit as split/shared. Given the high-complexity threshold for procedure code 99215, the documentation should clearly attribute the high-risk decision-making component (the element most likely to drive the code level) to the billing provider.
For teaching physician settings, CPT code 99215 billed under a resident’s involvement requires the teaching physician to be physically present for the key portions of the service and to document their own participation, findings, and management decisions. It is particularly for the high-risk decision-making that justifies the 99215 level.
A resident’s documentation alone, even if thorough, does not support billing under the teaching physician’s NPI without the required attestation. Benchmarking 99215 utilization against specialty norms and defending it in audit is detailed work, which is why many practices lean on professional medical billing services.
Top Reasons For Denials Specific To 99215 & Quick Remedies
- Insufficient MDM Documentation to Support High Complexity: Prevent by ensuring the assessment and plan documents at least two of the three MDM elements at the high level. With specific clinical detail identifying threat to life/bodily function, extensive data review, or high-risk management decisions, rather than restating the diagnosis alone.
- Time-Based Billing Without Adequate Time Documentation: Prevent by documenting the total minutes spent on the date of the encounter (40–54 minutes) along with a description of the specific activities performed.
- Incorrect Prolonged Service Code (99417 Billed to Medicare): Prevent by confirming payer type before selecting the prolonged service add-on code. Per Noridian MAC, CPT 99417 has Medicare status indicator “I” and is invalid for Medicare. Use G2212 instead, reportable only at 69+ minutes total time.
- Telehealth Claims Rejected for POS/Modifier Mismatch: Prevent by confirming modifier 95 (audio-video) or modifier 93 (audio-only) is paired with the correct POS code and that the payer’s policy permits the modality billed for 99215 CPT code.