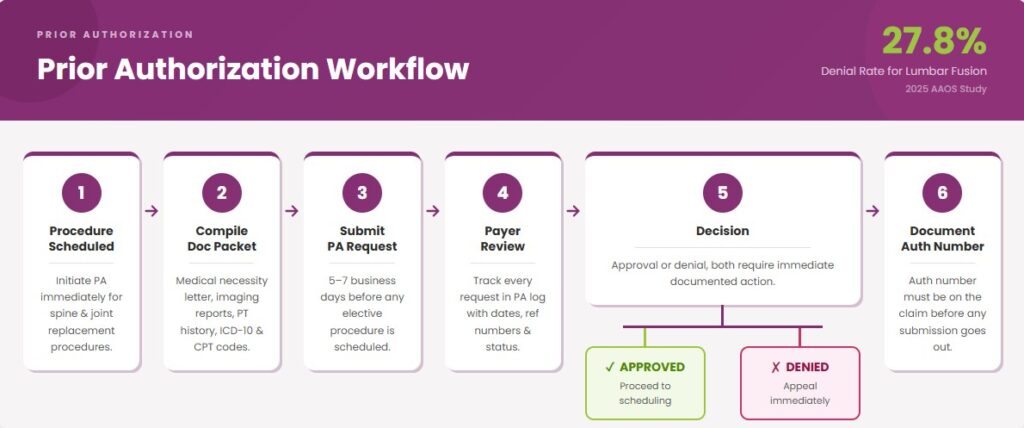
Orthopedic practices today face a billing environment that is more demanding than ever. According to a 2025 AAOS Annual Meeting study, prior authorization delays are causing higher denials. Insurers denied nearly 7% of elective spine surgeries, with denial rates reaching 27.8% for lumbar fusion procedures.
To make the situation more complex, CMS expanded its mandatory prior authorization list to include orthopedic braces and osteogenesis stimulators, adding a new compliance layer overnight. Meanwhile, the coding behind every orthopedic claim is uniquely complex.
Laterality errors, 90-day global period violations, and CMS’s quarterly NCCI edit updates mean a single miscoded claim can trigger a denial. This is why healthcare providers need to know everything about orthopedic medical billing services. From coding fundamentals to compliance requirements, this guide helps practices protect their revenue and reduce audit risks.
What Makes Orthopedic Billing Unique?
Orthopedic medical billing sits in a different category from most medical specialties. The combination of surgical complexity, implantable devices, and strict payer rules is the answer to what makes orthopedic medical billing hard.
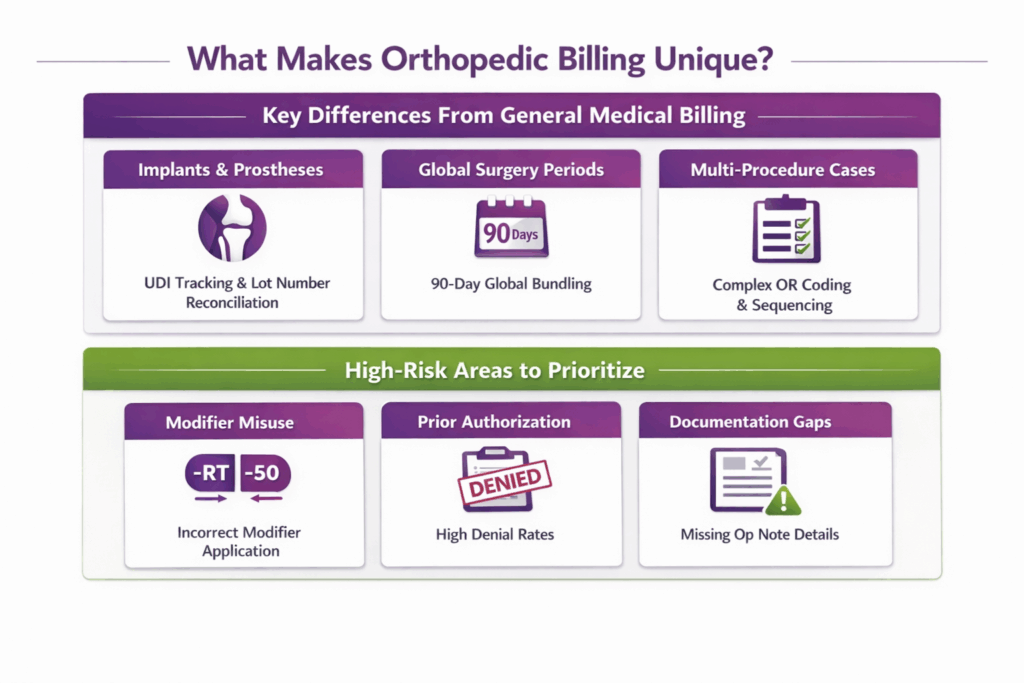
Key Differences From General Medical Billing
| Area | What It Means in Practice |
|---|---|
| Implants and Prostheses | Every implantable device requires a UDI, a unique code capturing device identifier and lot/batch number per FDA rule (21 CFR 801.20). Billing staff must reconcile this against operative notes before submission. |
| Global Surgery Periods | Per CMS, major orthopedic procedures carry a 90-day global period. All related post-op E/M visits within that window are bundled. Billing them separately is one of the most common orthopedic billing errors. |
| Multi-Procedure OR Cases | A single session can generate 3 to 5 CPT codes, like decompression, fusion, and instrumentation across multiple levels. Each requires correct sequencing, modifier application, and supply reconciliation before the claim goes out. |
High-Risk Areas to Prioritize
- Modifier misuse: Laterality (-RT/-LT), bilateral (-50), and distinct procedural service (-59) modifiers are heavily used and heavily audited in orthopedics. A wrong or missing modifier changes the reimbursement outcome entirely.
- Prior Authorization Failures: A 2025 AAOS study found denial rates for lumbar fusion reached 27.8%. Each unresolved denial means stalled revenue and delayed patient care.
- Documentation Gaps: Missing surgical approach, anatomical site, or implant details in the operative note leaves every associated CPT code vulnerable. This is regardless of whether the procedure was performed correctly.
How Should Front-Desk and Pre-Visit Workflows Operate?
What happens before a patient arrives directly determines whether a claim gets paid. Most orthopedic denials trace back to errors made at registration, eligibility, or authorization, not in the OR.
Patient Registration: Fields That Must Be Accurate
A single wrong digit in an insurance ID or a transposed date of birth will reject a claim before it is ever reviewed. Every patient record must capture and verify:
- Insurance ID and Group Number: Exactly as printed on the insurance card
- Subscriber Name and Relationship to Patient: Especially critical when the patient is a dependent
- Date of Birth: Must match the payer’s records precisely
- Policy Type: HMO, PPO, EPO, or HDHP, as each carries different referral and authorization rules
- Out-of-Network Indicators: Confirm whether the treating orthopedic surgeon and facility are both in-network; a mismatch between the two is a common surprise billing trigger under the No Surprises Act
Registration staff should verify this information at every visit, not just the first. Insurance changes mid-treatment are common, and orthopedic cases often span multiple visits within a single global period.
Eligibility and Benefits Check: What To Capture
A real-time eligibility check through EDI 270/271 transaction should run at least 72 hours before any scheduled orthopedic procedure. The check must confirm more than just active coverage. Capture all of the following:
| Field | Why It Matters in Orthopedics |
|---|---|
| Prior auth requirement | Many orthopedic procedures, especially spine and joint replacement, require authorization before scheduling |
| Deductible status | High-deductible plans shift significant cost to the patient; knowing the remaining balance prevents billing surprises |
| Co-insurance percentage | Orthopedic procedures carry high allowed amounts. Even a 20% patient share can be substantial |
| Outpatient vs. inpatient benefit rules | Total joint replacements are increasingly performed in ASCs; coverage rules differ sharply by setting |
| Out-of-network coverage | Confirms patient liability if any provider in the care team is OON |
Save a copy of the eligibility response. Payers can retroactively deny claims by claiming coverage was inactive on the date of service. So, a timestamped eligibility record is your documentation defense.
Prior Authorization: Who, When, and Timeline Checklist
Prior authorization for orthopedic procedures must be initiated early. Per a 2025 AAOS study, patients waiting on overturned PA denials had measurably worse outcomes by the time surgery was approved. This means delays are not just a billing problem, they are a clinical one.
Who Submits: Designated PA coordinator, not clinical staff.
When to Initiate: Minimum 5 to 7 business days before elective procedures. Immediately upon scheduling for spine surgery or total joint replacement.
Documentation Packet Typically Required:
- Physician’s letter of medical necessity
- Relevant diagnostic imaging reports (X-ray, MRI, CT)
- Conservative treatment history (PT notes, injection records, medication trials)
- ICD-10 diagnosis codes matching the procedure
- CPT codes for all planned procedures
- Operative plan or surgical notes from prior related procedures
Trigger Chart: Procedures That Almost Always Require Prior Auth:
| Procedure | Typical Auth Requirement |
|---|---|
| Total knee/hip arthroplasty | Yes, all major payers |
| Lumbar spinal fusion | Yes, all major payers |
| Arthroscopic knee surgery | Varies by payer |
| Rotator cuff repair | Varies by payer |
| Orthopedic braces/orthoses | Yes, CMS mandatory since August 2024 |
Financial Counseling and Estimates
For insured patients, provide a plain-language cost estimate before the visit. Cover three things: what insurance is expected to pay, what the patient’s estimated share is, and when payment is due.
For uninsured and self-pay patients, a Good Faith Estimate (GFE) is legally required under the No Surprises Act (45 CFR § 149.610). Per CMS, providers must give uninsured or self-pay individuals an estimate for the cost of their health care when scheduling the item or service or upon request. If the patient is billed $400 or more above the good faith estimate, they may dispute the bill through the federal patient-provider dispute resolution process.
Short Front-Desk Script For Self-Pay Patients:
“Based on the procedure planned, your estimated cost is $[amount]. This is an estimate, not a final bill. If your actual bill comes in $400 or more above this figure, you have the right to dispute it through a federal process. This estimate is not a contract. You are not required to use this facility.”
Per CMS, the GFE must be written in clear and understandable language and must include a disclaimer informing the patient of their right to initiate the dispute resolution process if billed charges are substantially in excess of the estimate.
Technology and Checklists: Front Desk Toolkit
Core tools every orthopedic front desk should use:
- EDI 270/271 Eligibility Transactions: Real-time insurance verification integrated into the practice management system
- Pre-Bill Edit Software: Flags missing auth numbers, diagnosis-procedure mismatches, and modifier errors before claim submission
- PA Tracking Log: A shared, date-stamped record of every authorization request, response, appeal, and expiration date
Pre-Visit Front Desk Checklist:
- Insurance card scanned and ID verified against payer records
- Eligibility check run and saved with timestamp
- Prior auth confirmed with reference number documented
- Patient cost estimate provided and signed
- GFE issued if patient is self-pay or uninsured
- Correct ICD-10 and CPT codes confirmed against the planned procedure
- OON status of all treating providers verified
How Must Clinical Documentation Support Claims?
A claim is only as strong as the documentation behind it. In orthopedic medical billing, where procedures are complex and audit scrutiny is high, the operative report and clinical notes are also the legal defense for every dollar billed.
Operative Reports: Minimum Elements to Defend a Claim
Every orthopedic operative report must contain the following before a claim is submitted:
- Procedure Description: What was performed, in clinical detail, not a templated macro. Per CMS, it is insufficient documentation if physicians only use macros.
- Surgical Approach: Open vs. arthroscopic, anterior vs. posterior. This determines the CPT code. A mismatch between the approach in the report and the code billed is an automatic audit flag.
- Laterality: Right, left, or bilateral, stated explicitly. Required for correct modifier application (-RT, -LT, -50).
- Implant Data: Device name, manufacturer, UDI, lot number, and serial number for every implantable device used, per FDA 21 CFR 801.20.
- Procedure Duration: Required for time-based anesthesia billing and for defending against unbundling queries.
- Surgeon’s Signature: CMS requires a dated, legible signature. An unsigned operative report is an unsupported claim.
Office Notes and E/M Documentation: Linking Diagnosis to Procedure
Office notes must do more than describe a visit. They must build a medical necessity case that justifies the procedure billed. For orthopedic claims, three things must be present and traceable across visit notes:
Medical Necessity Narrative: The note must state why this procedure is necessary for this patient at this time. Vague language like “patient requests surgery” is not sufficient. The note should document functional limitation, pain level, and impact on daily activity.
Failed Conservative Care: Most major orthopedic procedures, like joint replacement, spinal fusion, and rotator cuff repair, require documented evidence that conservative treatment was tried and failed. This means dated entries showing physical therapy, corticosteroid injections, oral medications, or activity modification were attempted before surgical intervention was recommended.
Imaging and Diagnostic Correlation. The ICD-10 diagnosis code on the claim must be directly supported by imaging or diagnostic findings in the record. An MRI report showing a torn meniscus must appear in the chart before CPT 29880 is billed.
Special Documentation: Injections, DME, Casts and Therapy Referrals
These service categories carry their own documentation requirements beyond the standard operative note.
| Service | Required Supporting Documentation |
|---|---|
| Joint/spinal injections | Consent form, fluoroscopy or imaging confirmation if applicable, and prior injection history |
| DME (braces, orthoses) | Signed physician order, diagnosis supporting medical necessity, conservative treatment trial per CMS LCD |
| Casts and splints | Clinical indication documented in the office note; if applied during a global period, confirm it is not bundled |
| Therapy referrals | Referral order with diagnosis, frequency, and duration; required if billing under a therapy benefit |
Audit-Ready File: What To Keep and For How Long
Per CMS regulation (42 CFR § 424.516(f)), Medicare providers and suppliers are required to maintain medical records for 7 years from the date of service. Failure to produce records on request can result in revocation of Medicare enrollment, not just repayment of a single claim.
An audit-ready orthopedic file should contain, at a minimum:
| Document | Retention Period |
|---|---|
| Operative reports | 7 years from DOS (CMS minimum) |
| Office and E/M notes | 7 years from DOS |
| Prior authorization approvals and denials | 7 years from DOS |
| Eligibility verification records (timestamped) | 7 years from DOS |
| Implant documentation / UDI records | 7 years from DOS; longer if state law requires |
| EOBs and claim remittances | 7 years from DOS |
| Good Faith Estimates (self-pay) | 7 years from DOS |
Two Practical Rules For Audit Readiness:
- Store timestamped eligibility responses alongside the claim. Payers can retroactively claim coverage was inactive on the date of service, and a dated verification record is your rebuttal.
- Never rely solely on EHR auto-populated fields. CMS auditors review for specificity. A note that reads identically across multiple visits, a clear sign of copy-paste, is a documentation integrity red flag.
How Do You Code Procedures and Apply Modifiers Correctly?
Correct coding in orthopedics is all about picking the right CPT number. It is about making a series of connected decisions, about medical necessity, modifier logic, global period rules, and procedure sequencing, where each one affects whether the claim pays. For a full procedure-by-procedure code reference, see our Orthopedic Medical Billing and Coding Cheat Sheet.
Common Procedure Buckets and Representative CPTs
Orthopedic CPT codes fall across five core procedure buckets. Each carries its own coding rules and documentation requirements:
| Procedure Bucket | Representative CPTs | Key Coding Variable |
|---|---|---|
| Arthroplasty | 27447 (TKA), 27130 (THA) | Approach, revision vs. primary |
| Arthroscopy | 29880 (knee meniscectomy), 29827 (rotator cuff repair) | Open vs. arthroscopic = different codes |
| Fracture fixation | 25607–25609 (distal radius), 27236 (femoral neck) | Complexity, internal vs. external fixation |
| Spine | 63047 (laminectomy), 22612 (posterior lumbar fusion) | Level, approach, instrumentation |
| Injections | 20610 (major joint), 62322 (lumbar epidural) | Anatomical site, imaging guidance |
ICD-10 to CPT Pairing: Medical Necessity Examples
Every CPT code on an orthopedic claim must be supported by an ICD-10 diagnosis that justifies it. Payers review this pairing, not just the procedure code, to determine whether the service was medically necessary.
| ICD-10 | Diagnosis | Paired CPT | Medical Necessity Logic |
|---|---|---|---|
| M17.11 | Primary osteoarthritis, right knee | 27447 | Conservative care failed; functional limitation documented |
| M75.120 | Complete rotator cuff tear, right shoulder | 29827 | Imaging confirmed; PT trial documented |
| M51.16 | Intervertebral disc degeneration, lumbar | 63047 | Neurological symptoms, failed conservative management |
The ICD-10 code alone is not enough. The office note must contain the narrative that connects the diagnosis to the procedure, such as failed conservative care, imaging correlation, and documented functional impact. Without that narrative, even a correctly paired code will face a medical necessity denial.
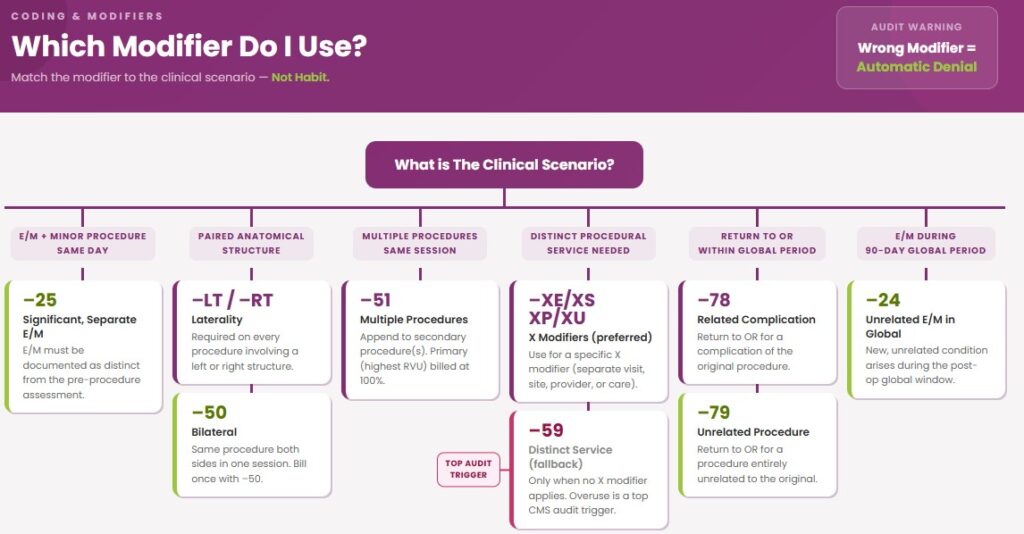
Modifier Guidance: Decision Trees
Modifiers are where orthopedic claims most commonly go wrong. Apply them based on the clinical scenario, not habit.
Modifier 25 for E/M Same Day As Procedure: Was a separately identifiable evaluation and management service performed on the same day as a minor procedure? If yes, append -25 to the E/M code. The E/M must be documented as distinct from the pre-procedure assessment. Do not use -25 on the same day as a major surgical procedure with a 90-day global period.
Modifier 59 vs. X Modifiers (XE, XS, XP, XU): Use -59 to indicate a distinct procedural service only when no other modifier more precisely describes the situation. CMS introduced the X modifiers to be more specific: -XE (separate encounter), -XS (separate structure), -XP (separate practitioner), -XU (unusual non-overlapping service). When one of the X modifiers fits, use it instead of -59. Applying -59 broadly without clinical justification is a common audit trigger.
Modifier 51 for Multiple Procedures: Append -51 to the secondary procedure(s) when multiple surgeries are performed in the same session. The primary procedure (highest RVU) is billed at 100%. Secondary procedures are typically reimbursed at 50%. Do not use -51 on add-on codes or codes exempt from multiple procedure reduction.
Modifiers 78/79 for Return to OR: Use -78 when the patient returns to the OR for a complication of the original procedure within the global period. Use -79 when the return is for an unrelated procedure entirely.
Modifiers LT/RT for Laterality: Required on every orthopedic procedure involving a paired anatomical structure. Missing laterality on a bilateral joint claim is a direct denial. If the same procedure is performed on both sides in the same session, use -50 (bilateral) rather than separate claims with -LT and -RT.
Global Surgical Periods and Post-Op Visits
CMS assigns every surgical CPT code a global period: 0 days, 10 days, or 90 days. Major orthopedic procedures carry 90-day globals. Minor procedures like injections and small joint aspirations carry 0 or 10.
What is Bundled in the 90-day Global: All routine post-op E/M visits, suture removal, and follow-up directly related to the surgery. Billing any of these separately within the global period triggers an automatic denial.
When You Can Bill Separately Within a Global:
- A new, unrelated condition arises: use -24 on the E/M
- A complication requiring a return to the OR: use -78
- An unrelated procedure is performed: use -79
- The surgeon did not perform the post-op care: use -54/-55 to split the global
Multiple Procedures, Bilateral Services, and Correct Sequencing
When multiple procedures are performed in the same OR session, claim construction matters as much as code selection.
Sequencing Rule: List the procedure with the highest relative value unit (RVU) first. Payers apply multiple procedure reductions to everything listed after the primary code. Incorrect sequencing can reduce reimbursement on your highest-value procedure.
Bilateral Procedures: Bill CPT 27447-50 for bilateral total knee replacement in a single session, not two separate claims. Payers that accept modifier -50 typically reimburse at 150% of the single-procedure rate.
NCCI Edits: CMS updates the National Correct Coding Initiative edits quarterly. These specify which orthopedic code pairs cannot be billed together. Always run claims through a pre-bill edit tool before submission.
How Should Implants, Supplies, and UDIs Be Billed?
Implants and prostheses are among the highest-cost line items in orthopedic billing. They are also among the most frequently denied. Documentation requirements are stricter, billing rules differ by setting, and the gap between device cost and payer reimbursement directly affects practice margins.
What Payers Expect: UDI, Serial/Lot, and Prosthesis HCPCS Rules
Per FDA 21 CFR 801.20, every implantable device requires a UDI (device identifier plus production identifier, lot/serial number) that is reconcilable against the claim. In practice:
- UDI, lot, and serial number must appear in the operative note before claim submission
- HCPCS Level II L-codes for prostheses must match the device type exactly
- Some commercial payers require UDI as a claim attachment
OR Charge Capture and Inventory Reconciliation Best Practices
Charge capture errors on implants are common because OR teams are focused on the procedure, not the billing record. Three controls close most of the gap:
- Real-Time Logging: Record device name, manufacturer, UDI, and quantity at implantation, not reconstructed post-op
- Post-OP Reconciliation: Charge capture record, operative report, and vendor packing slip must all agree before submission
- Cost-to-Charge Matching: Implant cost on the vendor invoice must match the billed charge as unbilled or underbilled devices are a direct margin loss
Billing Scenarios: Vendor-Supplied vs. Practice-Owned Implants
The ownership arrangement for an implant changes both the documentation trail and the compliance exposure. Each scenario carries a distinct set of requirements:
| Scenario | Key Billing Consideration |
|---|---|
| Vendor consignment | Packing slip must match the operative report. Confirm that consignment pricing does not create Anti-Kickback exposure |
| Practice-owned inventory | Billed charge must reflect the actual acquisition cost. Internal inventory logs must reconcile to the claim |
| Loaner sets | Confirm device is on the payer’s approved list before use as loaner components can carry different HCPCS codes |
ASC vs. Hospital Billing Differences for Implants
The billing treatment of implants changes significantly depending on the care setting. This distinction matters most in orthopedics, where device costs are high relative to the procedure payment:
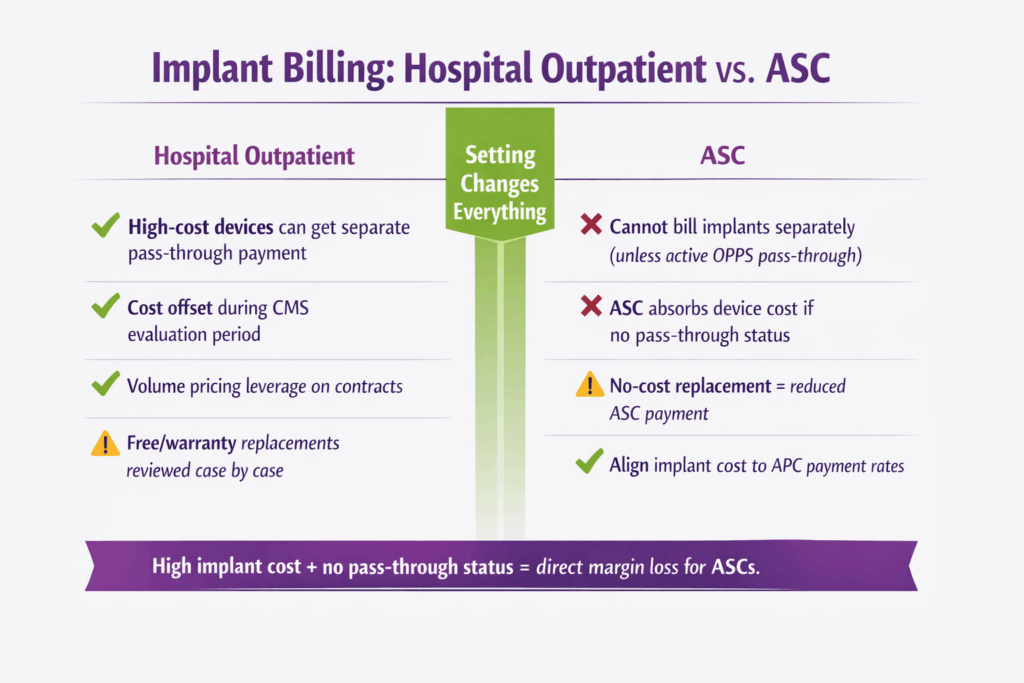
| Area | Hospital Outpatient | ASC |
|---|---|---|
| Separate device billing | High-cost devices can receive separate pass-through payment | Cannot be billed separately unless device holds active OPPS pass-through status |
| Device cost absorption | Offset by pass-through during CMS evaluation period | ASC absorbs device cost if no pass-through status |
| Free/warranty replacements | Reviewed case by case | A no-cost replacement device triggers a reduction in the procedure’s ASC payment |
| Contract negotiation priority | Volume pricing on implants | Align implant cost thresholds to APC payment rates. Negotiate tiered pricing for high-volume categories |
How Can You Prevent Denials and Run an Effective Appeals Workflow?
Denial prevention and appeals management are two sides of the same problem. A strong pre-submission process reduces denials at the front end. A structured appeals workflow recovers revenue when denials still get through.
Top Denial Reasons and Early Detection
Most orthopedic denials fall into four categories. Tracking each one as a distinct metric, not a combined denial rate, is what makes early detection possible:
| Denial Reason | What to Monitor |
|---|---|
| Missing or invalid prior auth | Auth number absent on claim; auth expired before DOS |
| Modifier errors | Claims rejected for unbundling, laterality mismatch, or -59 overuse |
| Inadequate documentation | Medical necessity not established; operative note missing required elements |
| Timely filing | Per CMS, Medicare claims must be received within one calendar year of the date of service. A denial for late filing is not an initial determination and is not subject to appeal |
Clean-Claim Checklist (Pre-Submission)
Every orthopedic claim should pass through automated pre-bill edits before submission. The checklist below covers the minimum gates:
- ICD-10 diagnosis code present and supports medical necessity for the billed CPT code
- CPT code matches the surgical approach documented in the operative report
- All required modifiers applied: laterality, bilateral, distinct service, global period
- Prior authorization number present and confirmed active on the date of service
- UDI and lot/serial number reconciled for all implants
- Attachments required by payer uploaded (operative note, imaging, consent)
- Claim submission date confirmed within the payer’s timely filing window
Denial Triage and Ownership
When a denial comes in, the first decision is who owns it. Routing the wrong denial type to the wrong team adds days to resolution. Use this escalation matrix:
| Denial Type | Owner | SLA for Rework |
|---|---|---|
| Missing or invalid prior auth | Billing: PA coordinator | 24 hours |
| Modifier error | Coding | 48 hours |
| Medical necessity/documentation | Clinical + Coding jointly | 48 to 72 hours |
| Timely filing | Billing manager review | Immediate |
| Implant / UDI mismatch | Billing + OR charge capture | 48 hours |
Every denial must have a timestamp, an assigned owner, and a resolution deadline logged in the denial tracking system. Unassigned denials age, and aged denials become write-offs.
KPIs to Track for Denials and Appeals
These four metrics give a complete picture of denial and appeals performance. Track them monthly, by denial category:

| KPI | What It Measures | Target Benchmark |
|---|---|---|
| Denial rate | % of claims denied on first submission | Below 5% |
| First-pass clean claim rate | % of claims paid without rework | Above 95% |
| Days to appeal resolution | Average time from denial to payment or write-off | Under 30 days |
| Appeal success rate | % of appealed claims that result in payment | Above 70% |
Which KPIs and RCM Metrics Should You Track?
Tracking the right numbers is what separates a practice that reacts to revenue problems from one that prevents them. In orthopedics, where a single denied TJA claim can represent thousands of dollars, the metrics you monitor and how often directly determine financial outcomes.
Essential RCM Metrics for Orthopedics
These six metrics form the core of any orthopedic RCM dashboard. Each one flags a different failure point in the revenue cycle:
| Metric | What It Measures | Target |
|---|---|---|
| Days in A/R | Average time from claim submission to payment | Under 40 days |
| A/R over 90 days | Claims aging beyond the recovery risk threshold | Below 15% of total A/R |
| Net collection rate | % of collectible revenue actually collected | Above 95% |
| Denial rate | % of claims denied on first submission | Below 5% |
| Clean claim rate | % of claims paid without rework | Above 95% |
| Cash per procedure | Average reimbursement per CPT family | Tracked monthly by procedure bucket |
Procedure-Level Profitability: How to Calculate
A high collection rate on a low-margin procedure is not the same as a profitable one. Procedure-level profitability requires accounting for all cost layers:
Net Margin per Procedure = Reimbursed Amount − Implant Cost − OR/Facility Cost Allocation − Professional Fee − Billing and Admin Cost
Track this monthly, by CPT family, like arthroplasty, spine, arthroscopy, and injections. A procedure that looks high-volume on the schedule may be underwater once implant costs and OR time are factored in. That is a contracting and scheduling decision, not just a billing one.
Reporting Cadence and Dashboard Fields
Different metrics need different review cycles. Mixing them into a single monthly report delays decisions that need to be made in days.
| Cadence | What to Review |
|---|---|
| Weekly | Claims pipeline, pending authorizations, new denials by category, A/R aging movement |
| Monthly | Net collection rate, denial rate by CPT family, procedure-level profitability, appeal resolution rate |
| Quarterly | Clean claim rate trend, A/R over 90 days, implant cost-to-reimbursement variance |
How Transcure Supports Orthopedic Practices
Every workflow in this guide, from registration, eligibility, prior auth and documentation to coding, implant billing, and denials, must execute correctly, across every claim, every day. Getting anyone wrong does not produce a single bad claim.
It produces a pattern of revenue loss that compounds quietly until it shows up as a cash flow problem. Transcure is built specifically for that problem.
What Transcure Brings to Orthopedic Practices:
| Capability | What It Means in Practice |
|---|---|
| 1,100+ certified billers and coders | Orthopedic-specialist staff, not generalists reassigned to your account |
| 98% clean claim rate | Fewer denials from day one, less rework, faster cash |
| 24-day average A/R recovery | Compared to a 40-day industry benchmark |
| 25% reduction in admin overhead | Clinical staff freed from billing tasks |
| 30+ EHR integrations | Epic, Athenahealth, eClinicalWorks, so no workflow disruption |
What Transcure Manages So Your Team Does Not Have To:
- Prior authorization for joint replacements, spine fusions, injections, and CMS-mandated orthotic braces
- UDI, lot, and serial number reconciliation on every implant claim
- Quarterly NCCI edit monitoring and CPT update implementation
- Denial triage, appeal writing, and payer follow-up across all orthopedic CPT families
- ICD-10 to CPT pairing and medical necessity documentation review before submission
Where It Starts:
Every Transcure engagement begins with a complimentary 21-KPI RCM audit worth $2000+. It is a baseline assessment that identifies exactly where revenue is leaking before it becomes a write-off. No commitment required.
For a practice collecting $1M annually, the difference between a 90% and 95% net collection rate is $50,000 in recovered revenue. The audit shows where your practice currently sits. Moreover, there are no hidden costs as Transcure charges only 5% of total collections for end-to-end medical billing services with complementary credentialing.