Ambulatory Surgery Centers (ASCs) are transforming outpatient healthcare, with billing complexity increasing as well. Today, more than 6,300 Medicare-certified ASCs treat approximately 3.4 million fee-for-service beneficiaries annually. Outpatient settings perform over 80% of the total surgeries. The U.S. ASC market exceeds $50 billion, with nearly 18,000 operating rooms nationwide, with 95% of centers operating as for-profit organizations.
Medicare payments to ASCs have surpassed $6 billion in recent years, as procedure volume has been rising. This is because CMS continues to expand the Covered Procedures List, resulting in more acuity cases being transferred to the ASC setting.
In this high-volume sector, ASC billing accuracy directly affects the revenue of ambulatory surgery centers. This ASC billing guide will help you understand the ASC billing process, commonly used codes, documentation requirements, challenges, and best practices for ASC billing.
What is Ambulatory Surgery Center?
Ambulatory Surgery Center (ASC) is a licensed, Medicare-certified healthcare facility that provides same-day surgical care, including diagnostic and preventive procedures that don’t require an overnight hospital stay. Centers for Medicare & Medicaid Services (CMS) requires that ASCs meet specific Conditions for Coverage to operate and get reimbursement.
ASC billing is the process of submitting claims for ASC services provided in the ambulatory surgery center, aside from the surgeon’s billing. ASC billing includes reporting CPT/HCPCS procedure codes, appropriate modifiers, revenue codes, and compliance with payer-specific reimbursement policies. The CMS ASC payment system assigns procedures to payment groups with predetermined rates.
What are the Common ASC Procedures?
Ambulatory Surgery Centers (ASCs) perform low-risk outpatient procedures that do not require an overnight hospital stay. Below are the most common services performed in ASCs:
- Gastroenterology procedures: Colonoscopies and upper endoscopies are commonly performed under the ASC Covered Procedures List with CPT coding.
- Orthopedic surgeries: Arthroscopy and minimally invasive joint repairs qualify for ASC payment groups.
- Ophthalmology procedures: Cataract removal and related eye surgeries are among the highest-volume ASC services.
- Pain management procedures: Epidural steroid injections and nerve blocks have payer coverage as ASC procedures.
- ENT surgeries: Sinus surgery and other otolaryngology procedures are suited for outpatient settings and have ASC payment classifications.
- Urology procedures: Cystoscopy and related minimally invasive interventions are commonly approved under ASC reimbursement policies.
Why ASC Medical Billing Is Different: Key Components and Challenges
Understanding what makes ASC medical billing different is essential for ASCs to maximize reimbursements. Unlike standard hospital billing, ASC billing focuses on the facility component of outpatient procedures. This requires strict adherence to specialized coding and reimbursement policies for ASCs. Following ASC medical billing guidelines ensures compliance with CMS regulations for ambulatory surgery centers.
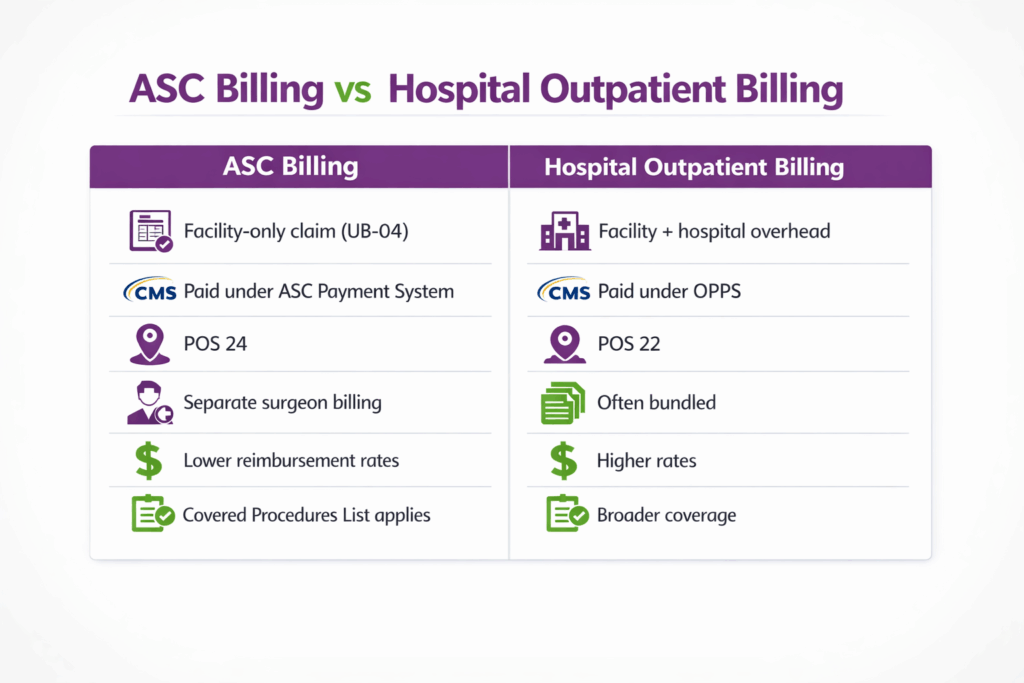
- Separate Facility vs. Professional Billing
ASC claims cover only the facility portion, while surgeons bill their professional services separately. Proper coordination helps to prevent coding errors and delayed payments.
- ASC Payment System Rules
Reimbursement follows the CMS ASC payment methodology, assigning procedures to payment groups with predetermined rates. Misclassification can cause revenue loss.
- Compliance with Covered Procedures List
Only procedures approved under the CMS ASC Covered Procedures List are reimbursable. Verifying eligibility before billing is critical to avoid denials.
- Complex Modifiers and Bundling Guidelines
Correct use of CPT/HCPCS modifiers and adherence to NCCI edits ensure that bundled procedures are billed accurately.
- High Audit and Regulatory Compliance
Documentation must support medical necessity, device use, and implant billing. Compliance with federal, state, and payer-specific rules reduces the risk of audits.
What Is the Step-by-Step Process for ASC Billing?
The ASC billing process follows a step-by-step workflow to ensure that all facility charges for outpatient procedures are properly documented, coded, and submitted. Each step is critical for compliance, revenue optimization, and minimizing claim denials.
Step 1: Patient Registration and Insurance Verification
The process begins with the patient’s registration and verification of their insurance coverage. The ASC team checks for prior authorizations and confirms eligibility for the scheduled procedure.
Practical example: Suppose a patient’s GI plan requires pre-approval for non-emergency colonoscopies. The ASC front desk should upload the colonoscopy order and patient records to the insurer’s portal before the procedure date. If the insurer denies coverage, the surgery is postponed or billed as a self-pay procedure. Conversely, a properly documented approval means no last-minute denials. See Transcure’s GI Prior Authorization Expansion alert for details on evolving GI pre-auth rules.
Step 2: Procedure Documentation and Coding
After the procedure, all facility-related services such as operating room use, supplies, implants, and anesthesia are carefully documented. This information is then converted into CPT/HCPCS codes, revenue codes, and modifiers in accordance with CMS ASC payment rules and NCCI. Use proper modifiers (e.g., -50, -59, -73, 74) for laterality, distinct services, or discontinued procedures; incorrect modifiers are a top cause of denials. For example, Medicare requires the “SG” modifier on the ASC claim line for facility services.
Practical example: After a knee arthroscopy, the surgeon’s note indicates a meniscectomy. An ASC coder using an integrated EHR will assign CPT 29880 (arthroscopy with meniscectomy) and attach the appropriate ICD-10 code for the diagnosis. The EHR then auto-includes charges for anesthesia and any implants used, reducing manual entry errors. All supporting details (patient history, consent, implants listed) are kept in the chart to substantiate the bil
Step 3: Claim Preparation and Scrubbing
Claims are prepared using the documented services. Scrubbing helps to detect coding errors, missing information, or bundling conflicts. This quality check improves first-pass claim approval rates and reduces denials. ASCs generally bill on the CMS-1500 (HCFA 1500) form with a Place of Service code of “24” (ASC). Unlike hospitals (UB-04/APC), ASC facility claims are submitted on the CMS-1500 form, as are physician claims from the same case (when applicable).
Step 4: Claim Submission to Payers
Once verified, claims are submitted to Medicare or commercial payers. ASC billing focuses on facility charges, while the surgeon submits separate fees. Timely submission helps ASCs to maintain cash flow.
Be sure to submit facility charges (nursing, facility fee, supplies) under the ASC facility’s name, and have the physician submit professional charges separately on their National Provider Identifier (NPI).
Step 5: Claim Tracking and Denial Management
Submitted claims are monitored for approval. Rejections or denials are reviewed and appealed so the facility receives full reimbursement for services.
Practical example: If a colonoscopy claim is denied due to “no pre-authorization on file,” the billing staff should immediately contact the physician’s office to verify whether pre-authorization was obtained. If it was, submit a reconsideration with the auth approval attached. If not, quickly appeal with clinical justification or arrange for patient self-pay. Over time, tracking these outcomes reduces repeated errors.
Step 6: Payment Posting and Reconciliation
Payments are posted and reconciled against expected reimbursements. Any discrepancies are identified to maintain accurate revenue reporting. Maintain strict compliance as well. ASCs must bill only for procedures on the CMS ASC Covered List; any facility claim for a non-ASC-approved procedure will be denied. Likewise, follow all CMS billing policies.
ASCs can optimize revenue, reduce denials, and maintain regulatory compliance by following these ASC billing guidelines.
What are the Common ASC Coding and Billing Codes?
Ambulatory Surgery Centers (ASCs) use a combination of standardized code sets for accurate billing and reimbursement. These include ICD-10 codes for diagnoses, ASC CPT codes for procedures, HCPCS codes for supplies and medications, and modifiers to clarify services performed. Understanding how these coding systems work together is critical for maintaining compliance. This ASC billing guide shows the most common ICD-10, CPT, HCPCS, and modifier codes used in ASC billing, with ASC billing coding cheat sheet.
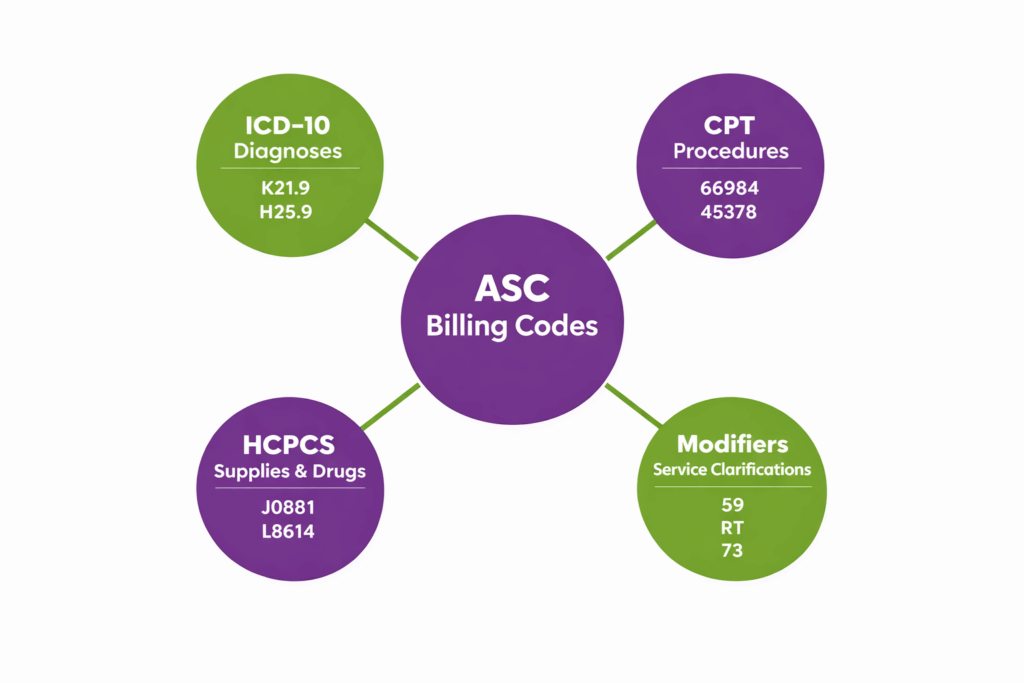
Common ASC ICD-10 Codes
These ICD-10 codes show frequently billed diagnoses in Ambulatory Surgery Centers (ASCs).
| ICD-10 Code | Description | Common ASC Procedure |
|---|---|---|
| K21.9 | Gastroesophageal reflux disease without esophagitis | Upper GI endoscopy |
| N40.0 | Enlarged prostate (benign prostatic hyperplasia) | TURP, prostate procedures |
| H25.9 | Age-related cataract, unspecified | Cataract surgery |
| M17.9 | Osteoarthritis of knee, unspecified | Knee arthroscopy |
| L40.0 | Psoriasis vulgaris | Dermatology procedures, excisions |
| I83.90 | Varicose veins of lower extremities, unspecified | Vein ablation or ligation |
| N81.4 | Pelvic organ prolapse, unspecified | Gynecology procedures |
| K80.20 | Calculus of gallbladder without cholecystitis | Laparoscopic cholecystectomy |
| M51.36 | Lumbar disc degeneration, lumbar region | Spine procedures, discectomy |
| H52.4 | Presbyopia | LASIK or refractive procedures |
Common ASC CPT Codes
These ASC CPT codes represent some of the most frequently billed procedures in Ambulatory Surgery Centers (ASCs).
| CPT Code | Description | Common ASC Procedure |
|---|---|---|
| 66984 | Extracapsular cataract removal with intraocular lens | Cataract surgery |
| 47562 | Laparoscopic cholecystectomy | Gallbladder removal |
| 29881 | Arthroscopy, knee, surgical; with meniscectomy | Knee arthroscopy |
| 52440 | Cystourethroscopy, with removal of ureteral calculus | Urology procedures |
| 36415 | Collection of venous blood | Phlebotomy, lab draws |
| 45378 | Colonoscopy, flexible, diagnostic | GI endoscopy |
| 64721 | Neuroplasty and/or transposition; median nerve at carpal tunnel | Carpal tunnel release |
| 20610 | Arthrocentesis, small joint | Joint injections |
| 58571 | Hysteroscopy, surgical, with biopsy | Gynecology procedures |
| 12001 | Simple repair of superficial wounds, 2.5 cm or less | Minor dermatology surgery |
Common HCPCS Codes in ASC Billing
HCPCS codes in ASC billing are primarily used for supplies, implants, and injectable medications that accompany procedures.
| HCPCS Code | Description | Common ASC Use |
|---|---|---|
| J0881 | Injection, epoetin alfa, 1,000 units | Anemia management, pre-op optimization |
| J2270 | Injection, ketorolac tromethamine, per 15 mg | Pain management, post-op analgesia |
| A4206 | Catheter, intermittent, each | Urology procedures, post-op supplies |
| L8614 | Intraocular lens, single-piece | Cataract surgery implants |
| J3010 | Injection, fentanyl citrate, per 100 mcg | Anesthesia or pain management |
| A9524 | Injection, skin test antigen, tuberculin | Pre-op screening |
| J7350 | Injection, denosumab, 1 mg | Orthopedic/osteoporosis-related procedures |
| A4550 | Infusion set for insulin pump | Diabetes management supplies |
| L8699 | Implantable device, prosthetic, other | Orthopedic or cardiac implants |
| J1094 | Injection, dexamethasone, up to 4 mg | Anti-inflammatory post-op injections |
Common ASC Modifiers
Modifiers in ASC billing provide additional information about how a procedure was performed. They clarify reduced services, laterality (right/left), or billing anomalies, such as the wrong patient/body part.
| Modifier | Description | Common Use in ASC Billing |
|---|---|---|
| 52 | Reduced services | Procedure performed with less intensity or incomplete service |
| 59 | Distinct, separate procedure | Identifies procedures that are separate from other procedures performed |
| 73 | Procedure discontinued after prepping for surgery | Surgery started but stopped before anesthesia or incision |
| 74 | Procedure finished following anesthesia administration | Surgery completed after anesthesia started |
| RT | Right side | Denotes procedure performed on the right side of the body |
| LT | Left side | Denotes procedure performed on the left side of the body |
| TC | Technical component | Billed when only the technical component of a service is performed (e.g., imaging) |
| FB | Device furnished at no cost/full credit | Indicates device provided at no charge or full credit to payer |
| FC | Device provided at partial credit | Indicates device provided with partial credit adjustment |
| PT | Screening service changed to diagnostic or therapeutic service | Screening converted to diagnostic/therapeutic service during procedure |
| PA | Wrong body part | Used when surgery was mistakenly performed on the incorrect body part |
| PB | Surgery wrong patient | Surgery performed on the incorrect patient |
| PC | Wrong surgery on a patient | Incorrect procedure performed on the correct patient |
What Are the Most Common ASC Billing and Coding Mistakes?
Accurate ASC billing and coding help Ambulatory Surgery Centers (ASCs) ensure compliance, maximize reimbursement, and prevent audits. By understanding ASC billing guidelines, practices can reduce claim denials and avoid revenue loss. However, even experienced staff can make common mistakes that lead to claim denials. Here are some common billing and coding mistakes ASC billers and coders make:
1. Coding for Non-Covered Procedures
Submitting claims for procedures that are not covered by the patient’s insurance or Medicare is a common error. This can lead to immediate denials and compliance issues. ASCs should verify coverage and document medical necessity before billing.
2. Failing to Document Properly
Proper documentation supports medical necessity and the services provided. Missing operative notes, incomplete histories, or absent signatures can trigger denials. Accurate, timely documentation is the key to ASC billing and coding compliance.
3. Upcoding
Upcoding occurs when a procedure or service is reported at a higher level than was actually performed. This can result in overpayment requests or penalties. Staff should strictly follow CPT, ICD-10, and HCPCS coding guidelines.
4. Unbundling
Unbundling is the incorrect separation of services that should be billed as a single bundled code. This practice can trigger denials for fraudulent billing. ASCs must accurately review payer rules and codes to avoid unbundling.
5. Incorrect Use of Modifiers
Modifiers, such as RT/LT, 52, 59, or TC, are frequently misapplied in ASC billing. Using the wrong modifier can cause denials, underpayment, or audit triggers. Staff should ensure modifiers accurately reflect the procedure and service for ASC billing and coding.
6. Failing to Verify Payer-Specific Rules
Every insurance payer has different rules for coverage, prior authorization, or bundled services. Failing to follow these guidelines can result in claim denials or delayed reimbursement. ASCs should maintain an updated payer policy for all commonly performed procedures.
How Can ASCs Ensure Accurate and Compliant ASC Billing?
Ensuring accurate billing in Ambulatory Surgery Centers (ASCs) requires a mix of regulatory knowledge, coding accuracy, and payer rule compliance. The following ASC billing guidelines help ASCs maintain compliance and reduce audit risk:
1. Follow CMS Billing and Coding Guidelines
The Centers for Medicare & Medicaid Services (CMS) provides detailed instructions for ASC billing. Staff should regularly review CMS updates to ensure claims have the correct procedures and payment rules
2. Coding Compliance with ICD-10, CPT, and HCPCS
Accurate coding is the backbone of ASC billing. ICD-10 codes capture diagnoses, CPT codes document procedures, and HCPCS codes cover supplies, drugs, and implants. Staff should use official code sets and avoid errors like upcoding, unbundling, or incorrect modifiers.
3. Anti-Kickback Statute and Stark Law
Compliance with the Anti-Kickback Statute (AKS) and Stark Law is critical. ASCs need to avoid improper financial arrangements with physicians or vendors. Any violations can result in fines, audits, and exclusion from federal programs.
4. Understand ASC Payment Groupings
ASCs are reimbursed based on Ambulatory Payment Classifications (APCs) or Medicare ASC payment groups. Understanding how procedures are grouped and reimbursed helps optimize revenue and prevent underpayment.
5. Conduct Regular Internal Audits
Routine audits of claims, documentation, and coding help identify errors early. These ensure compliance and reduce the risk of denials or audits. Audits should focus on high-volume procedures, modifier use, and payer-specific rules to maximize impact.
What Types of Payers Do Ambulatory Surgery Centers Work With?
Understanding the types of payers that ASCs bill is important for compliance with payer-specific requirements. Each payer type has unique rules, coverage policies, and documentation requirements that ASC staff need to consider.
1. Medicare
Medicare is the main payer for many ASC procedures. ASCs must follow Medicare payment rules, coverage policies, and Ambulatory Payment Classifications (APCs) to ensure accurate reimbursement. ASC claims must include correct CPT, HCPCS, ICD-10 codes, and any required modifiers.
2. Commercial Insurers
Commercial insurance plans vary widely in coverage and prior authorization requirements. ASCs should maintain updated contracts, verify coverage before procedures, and submit claims according to each insurer’s specific rules.
3. Medicaid
Medicaid programs differ by state, with unique billing requirements and payment rates. ASCs must comply with state-specific Medicaid regulations and get prior authorizations when necessary.
4. Self-Pay Patients
Self-pay patients require clear communication about costs and payment. Practices should provide itemized estimates and payment plans to reduce ASC billing confusion and ensure timely collection.
Why Should ASCs Outsource Their ASC Billing?
Ambulatory Surgery Centers (ASCs) face complex billing challenges. These include strict compliance requirements, payer-specific rules, and frequent claim denials. Outsourcing ASC billing has several benefits for ASC, such as:
1. Expertise in ASC-Specific Coding and Compliance
ASCs get access to professionals trained in ICD-10, CPT, HCPCS, and ASC-specific modifiers. Their knowledge of CMS guidelines, commercial payer rules, and state-specific regulations ensures accurate claims, which reduces the risk of denials.
2. Improved Revenue Cycle Management
Outsourced billing providers streamline claim submission, follow-ups, and denial management. With specialized tools and analytics, they can identify missed charges and reduce accounts receivable days, leading to higher revenue collection.
3. Reduced Administrative Burden
ASC billing is time-consuming and requires continuous updates on coding rules and payer policies. By outsourcing, ASC staff can focus on patient care, while experts handle ASC billing and coding.
4. Access to Advanced Technology
Many ASC billing companies use AI-driven billing platforms and automation tools. Such tools minimize errors, track claims in real time, and ensure timely reporting. This reduces human errors and increases billing accuracy.
5. Scalability and Cost Efficiency
Outsourcing provides flexibility as ASCs grow or perform more procedures. Instead of hiring and training additional in-house staff, ASC operators can scale billing resources efficiently, at a lower cost.
How to Choose the Right ASC Medical Billing Company
Selecting the right ASC billing partner is an important decision for Ambulatory Surgery Centers. The right ASC billing company not only ensures accurate claims but also helps maintain compliance with payer CMS regulations. You should consider the following factors when choosing an ASC billing partner:
1. Experience with ASC Billing
You should look for a medical billing company with proven experience in ASC-specific billing. Experience across multiple specialties, such as ophthalmology, orthopedics, and urology, is also a good sign.
2. Compliance and Regulatory Knowledge
Make sure they follow CMS guidelines, Stark Law, Anti-Kickback Statute, and state regulations. With a compliant partner, your practice minimizes the risk of audits, fines, or denied claims.
3. Technology and Automation
Top ASC medical billing companies use advanced billing software and reporting tools. Technology helps reduce errors, monitor claims, and improve overall efficiency.
4. Denial Management and Follow-Up
Right billing partners actively manage denials, submit appeals, and follow up with payers. This results in higher first-pass claim approval rates and maximizes revenue.
5. Scalability and Flexibility
Choose an ASC medical billing company that can adapt to you handle high volumes of ASC procedures. Also, ensure it can scale resources as needed without compromising service quality.
6. Cost Structure
Understand whether their pricing model is percentage-based, per-claim, or flat fee. Make sure it aligns with your ASC’s finances.
Conclusion:
ASC billing requires precise ICD-10, CPT, and HCPCS coding, accurate modifier usage, and strict compliance with CMS ASC payment rules and the Covered Procedures List. A structured ASC billing process reduces errors and improves clean claim rates. By outsourcing to ASC billing experts, ambulatory surgery centers can maximize reimbursements and maintain regulatory compliance.
FAQs
What is ASC billing?
ASC billing is the process of submitting facility claims for outpatient procedures performed in an Ambulatory Surgery Center. It includes reporting ASC CPT codes, HCPCS codes, ICD-10 codes, modifiers, and complying with payer-specific reimbursement rules.
How do ASCs manage coding for multi-specialty procedures?
ASCs use accurate CPT, ICD-10, and HCPCS codes with proper modifiers to bill multi-specialty procedures. Clear documentation of each provider’s service ensures compliance, reduces denials, and maximizes reimbursement.
How do ASCs handle out-of-network billing and coding?
Out-of-network ASC billing requires verifying patient benefits, submitting claims with medical necessity, and communicating patient financial responsibility. Proper coding ensures faster reimbursement and compliance with payer rules.
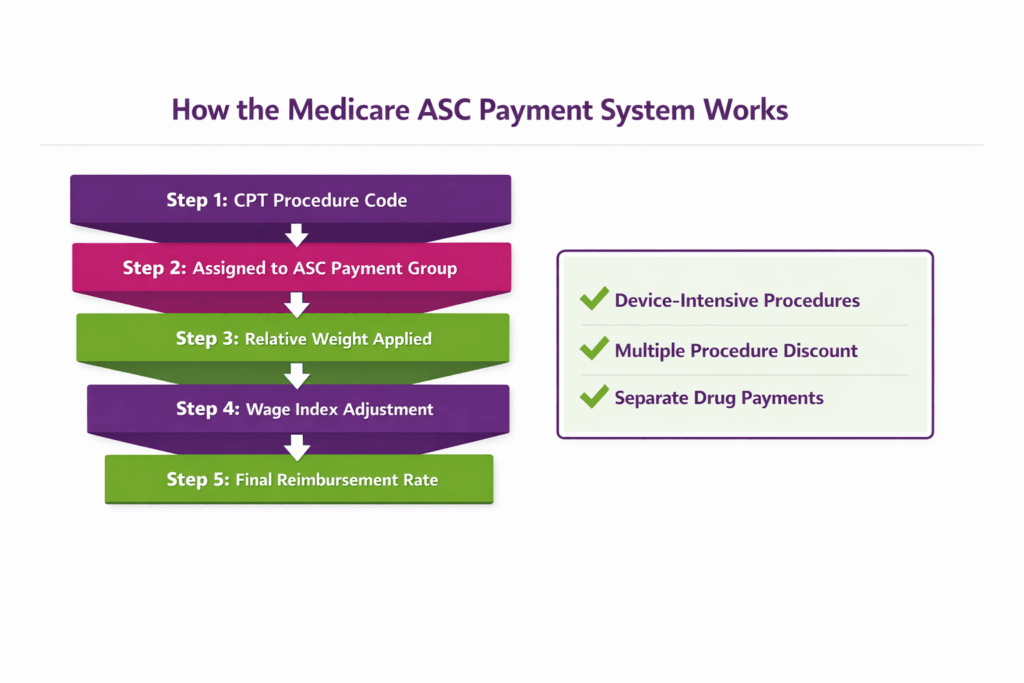
How do ASCs get paid by Medicare?
Medicare pays ASCs under the ASC payment system, assigning procedures to payment groups with predetermined rates based on Ambulatory Payment Classifications (APCs).
What are the reasons for ASC claim denials?
Common reason of ASC denials include incorrect modifiers, unbundling, lack of medical necessity documentation, coding errors, and failure to follow payer-specific rules.
What is the ASC Covered Procedures List?
The ASC Covered Procedures List identifies procedures approved for reimbursement in the ASC setting under CMS guidelines.