
Chronic kidney disease (CKD) is one of the highest-volume diagnoses in nephrology and primary care. It is also one of the most frequently miscoded. The ICD-10-CM framework for CKD is stage-driven. The correct code depends on the GFR-based stage documented by the provider.
One missing stage assignment can trigger a risk-adjustment error or a payer denial. This guide covers every billable CKD ICD-10 code, combination codes for hypertension and diabetes, dialysis and transplant status rules, documentation requirements, and the most common denial patterns. Understanding these core nephrology billing ICD-10 codes is essential for maintaining compliance and preventing revenue leakage at every stage of renal care.
CKD ICD-10 Quick Reference Card
Primary CKD Stage Codes (N18 Family)
| Code | Description | Key Rule |
|---|---|---|
| N18.1 | CKD, Stage 1 | GFR 90 or above; kidney damage markers present. Provider must document. |
| N18.2 | CKD, Stage 2 (mild) | GFR 60 to 89; mild reduction with kidney damage markers present. |
| N18.30 | CKD, Stage 3 (unspecified) | GFR 30 to 59; use when provider does not specify 3a or 3b. |
| N18.31 | CKD, Stage 3a | GFR 45 to 59; requires provider documentation of 3a. |
| N18.32 | CKD, Stage 3b | GFR 30 to 44; requires provider documentation of 3b. |
| N18.4 | CKD, Stage 4 (severe) | GFR 15 to 29; often precedes ESRD planning. |
| N18.5 | CKD, Stage 5 | GFR below 15; not on dialysis. Do not use N18.6 unless dialysis is active. |
| N18.6 | End-stage renal disease (ESRD) | CKD requiring chronic dialysis. Add Z99.2. Do not use N18.5 alongside. |
| N18.9 | CKD, unspecified | Use only when stage is not documented. Avoid in risk-adjusted models. |
Combination Codes: Comorbidity-Driven Sequencing
| Code | Description | Key Rule |
|---|---|---|
| I12.9 | Hypertensive CKD, stages 1 to 4 or unspecified | Assumed causal link. Code I12.9 first, then N18 stage code. |
| I12.0 | Hypertensive CKD with stage 5 or ESRD | Code I12.0 first, then N18.5 or N18.6, then Z99.2 if on dialysis. |
| I13.x | Hypertensive heart and CKD | Use I13 when hypertension, heart disease, and CKD are all present. |
| E11.22 | Type 2 diabetes with diabetic CKD | Code E11.22 first; add N18.x stage second. Assumed causal link applies. |
Status and Manifestation Codes
| Code | Description | Key Rule |
|---|---|---|
| Z99.2 | Dependence on renal dialysis | Always pair with N18.6. Never use Z99.2 without N18.6 for ESRD. |
| Z94.0 | Kidney transplant status | Add alongside N18.x when CKD persists after transplant. Not a complication code. |
| D63.1 | Anemia in CKD | Manifestation code. Never first-listed. Always follows N18.x. |
| N25.81 | Secondary hyperparathyroidism of renal origin | Code after N18.x. Common in stage 4 and 5 CKD and ESRD patients. |
What Is the ICD-10 Code for CKD?
The ICD-10-CM parent category for chronic kidney disease (CKD) is N18, which represents chronic kidney disease in the ICD-10-CM classification system. However, N18 itself is a non-billable parent code and must never be submitted on a claim. Instead, coders must report the appropriate stage-specific subcode ranging from N18.1 through N18.9 based on the provider’s documentation of CKD severity.
CKD code selection is both GFR-based and provider-documented. Although estimated glomerular filtration rate (eGFR) values help determine CKD severity clinically, coders cannot assign a CKD stage from lab values alone. The provider must explicitly document the clinical CKD stage and link it to the patient’s renal findings. If the stage is not documented, the only reportable option is N18.9 for unspecified CKD.
Within ICD-10-CM, CKD falls under Chapter 14: Diseases of the Genitourinary System (N00–N99). This chapter also includes related renal conditions such as acute kidney failure (N17) and unspecified kidney failure (N19), which are coded separately depending on the provider’s documentation and clinical presentation.
| CODING RULE: N18.9 (CKD, unspecified) is billable but carries the lowest specificity. It undercounts disease severity in risk-adjusted payment models such as Medicare Advantage and ACO programs. Coders should query the provider when no stage is documented before defaulting to N18.9. |
Complete CKD ICD-10 Code Table — 2026 Edition
The 2026 ICD-10-CM edition retains all N18 codes from the prior year. No additions or deletions were made to the N18 family. The stage 3 subcodes (N18.31 and N18.32) introduced in prior editions remain active for 2026.
The N18 Code Family: Stage-Specific CKD Codes
Stage selection maps directly to GFR ranges as defined by KDIGO guidelines. The provider must document the CKD stage. Coders cannot assign a stage from a lab result alone. Following a structured nephrology billing guide ensures that your clinical staff captures the precise terminology required to back up these codes during an audit.
| Code | Description | GFR Range | Billable? | Stage Note |
|---|---|---|---|---|
| N18 | CKD, parent category | N/A | No — do not bill | Non-specific. Code subcategory only. |
| N18.1 | CKD, Stage 1 | 90 or above | Yes | Kidney damage markers required. |
| N18.2 | CKD, Stage 2 (mild) | 60 to 89 | Yes | Mild reduction with damage markers. |
| N18.30 | CKD, Stage 3 (unspecified) | 30 to 59 | Yes | Use when 3a or 3b is not specified. |
| N18.31 | CKD, Stage 3a | 45 to 59 | Yes | Provider must document 3a specifically. |
| N18.32 | CKD, Stage 3b | 30 to 44 | Yes | Provider must document 3b specifically. |
| N18.4 | CKD, Stage 4 (severe) | 15 to 29 | Yes | Pre-ESRD planning stage. |
| N18.5 | CKD, Stage 5 | Below 15 | Yes | Not on dialysis. Do not use with N18.6. |
| N18.6 | ESRD — end-stage renal disease | Below 10 to 15 | Yes | Requires chronic dialysis. Add Z99.2. |
| N18.9 | CKD, unspecified | Not documented | Yes | Last resort. Query provider before assigning. |
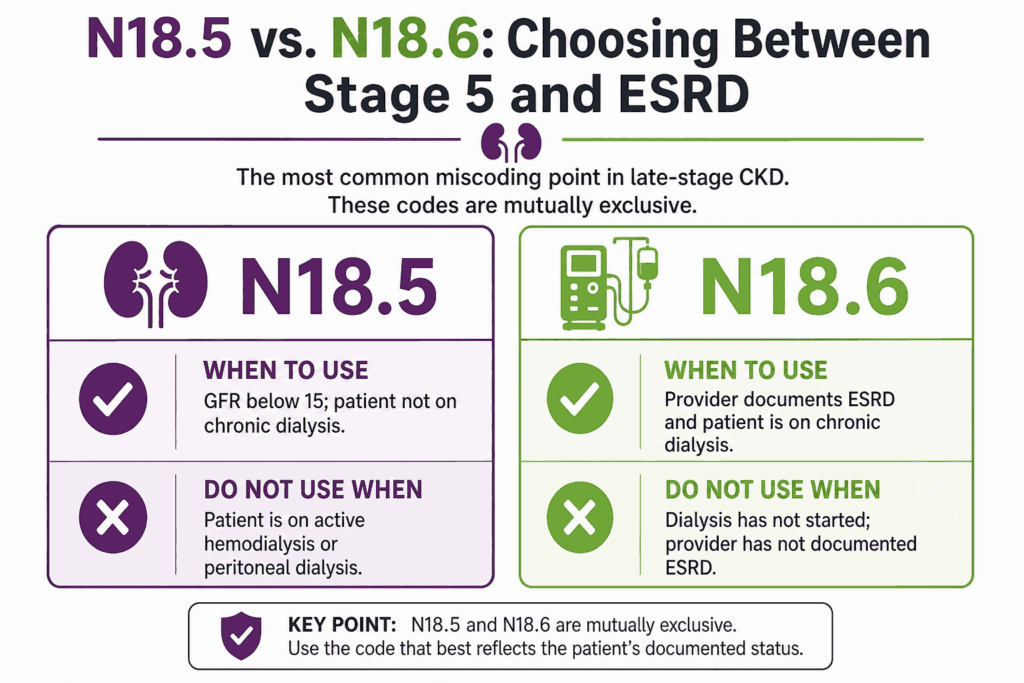
N18.5 vs N18.6: Choosing Between Stage 5 and ESRD
This is the most common miscoding point in late-stage CKD. N18.5 and N18.6 are mutually exclusive.
| Code | When to Use | Do Not Use When |
|---|---|---|
| N18.5 | GFR below 15; patient not on chronic dialysis | Patient is on active hemodialysis or peritoneal dialysis |
| N18.6 | Provider documents ESRD and patient is on chronic dialysis | Dialysis has not started; provider has not documented ESRD |
| DENIAL SCENARIO: A nephrologist documents CKD stage 5 in the encounter note. The patient is on twice-weekly hemodialysis. The coder assigns N18.5. The claim is reviewed for dialysis-related CPT codes but the diagnosis lacks ESRD status. Payer denies medical necessity for dialysis. The fix: when chronic dialysis is active and the provider has documented ESRD, N18.6 is required, not N18.5. |
Combination Codes: CKD with Hypertension and Diabetes
CKD rarely exists in isolation. ICD-10-CM uses combination codes and assumed causal relationships for CKD with hypertension and diabetes. These rules govern most nephrology and primary care claims.
CKD with Hypertension: The I12 and I13 Code Families
ICD-10-CM assumes a causal relationship between hypertension and CKD whenever both are documented together. This assumption applies unless the provider explicitly states that the conditions are unrelated. When that assumed link is present, I10 (essential hypertension) must never be coded alongside a standalone N18 code. The I12 combination code replaces both.
| Code | Description | Sequence First? | Additional Codes Required |
|---|---|---|---|
| I12.9 | Hypertensive CKD, stages 1 to 4 or unspecified | Yes — I12.9 is sequenced before N18.x | N18.1 through N18.4 or N18.9 to specify stage |
| I12.0 | Hypertensive CKD, stage 5 or ESRD | Yes — I12.0 before N18.5 or N18.6 | Z99.2 added when patient is on dialysis |
| I13.0 | Hypertensive heart and CKD with heart failure, stages 1 to 4 | Yes — I13.0 first | I50.x for heart failure type; N18.x for CKD stage |
| I13.2 | Hypertensive heart and CKD with heart failure and stage 5 or ESRD | Yes — I13.2 first | I50.x, N18.5 or N18.6, Z99.2 if on dialysis |
| CRITICAL RULE — Hypertension with CKD: Never code I10 (essential hypertension) alongside N18.x when both hypertension and CKD are documented in the same encounter. ICD-10-CM mandates the I12 combination code when the assumed causal link applies. Coding I10 plus N18.x as separate standalone codes is a compliance error and an audit trigger. |
CKD with Diabetes: E-Code Combination Codes
ICD-10-CM also assumes a causal link between diabetes and CKD when both are documented. This assumed relationship applies unless documentation explicitly says otherwise.
The sequencing rule for diabetic CKD places the diabetes combination code first and the N18 stage code second.
| Diabetes Type | Combination Code | Additional Code Required |
|---|---|---|
| Type 1 | E10.22 — Type 1 diabetes with CKD | N18.1 through N18.6 or N18.9 to identify CKD stage |
| Type 2 | E11.22 — Type 2 diabetes with CKD | N18.1 through N18.6 or N18.9 to identify CKD stage |
| Drug-induced | E09.22 — Drug-induced diabetes with CKD | N18.x stage code; add T-code for causative drug |
| Other specified | E13.22 — Other specified diabetes with CKD | N18.x stage code added second |
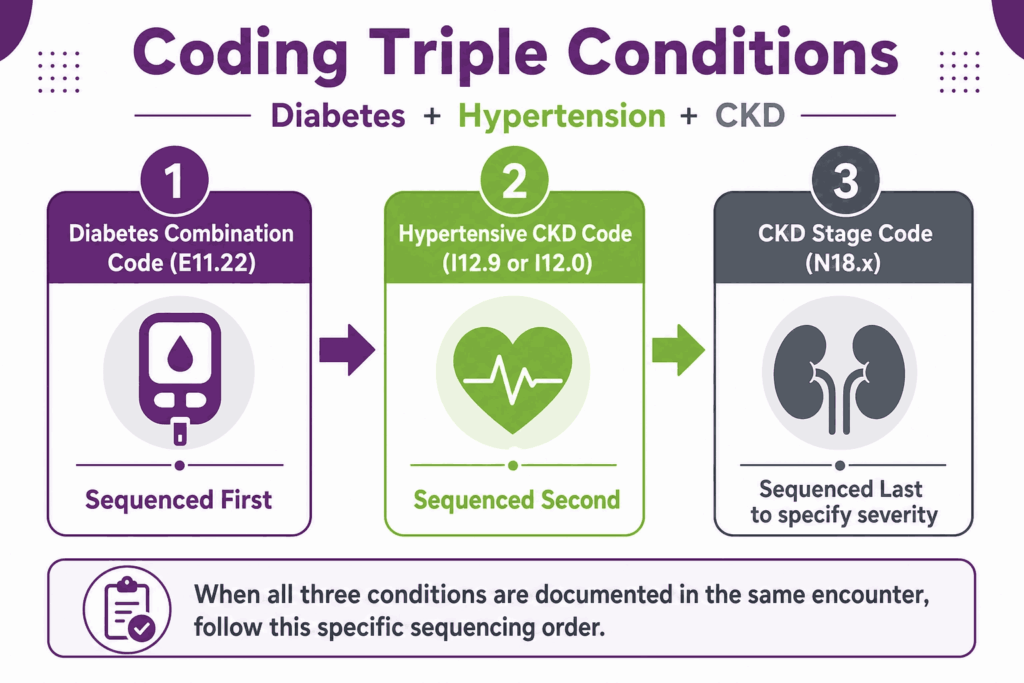
When All Three Conditions Are Present: Diabetes, Hypertension, and CKD
When a patient has type 2 diabetes, hypertension, and CKD documented in the same encounter, three codes are required: E11.22, I12.9 (or I12.0), and N18.x. The diabetes combination code is sequenced first. The hypertensive CKD code follows. The N18 stage code comes last to specify CKD severity.
| CODING EXAMPLE — Triple Comorbidity: Patient: type 2 diabetes, hypertension, CKD stage 3b. Correct code sequence: (1) E11.22 — type 2 diabetes with CKD; (2) I12.9 — hypertensive CKD stages 1 to 4; (3) N18.32 — CKD stage 3b. Do not separately code I10 for hypertension in this encounter. Do not code N18.32 without the upstream combination codes. |
Dialysis and Transplant Status Codes
Dialysis dependence and transplant status significantly affect CKD code selection, sequencing, and medical necessity reporting. ICD-10-CM requires additional status codes to accurately reflect whether a patient is actively receiving dialysis or living with a functioning kidney transplant alongside ongoing CKD.
N18.6 and Z99.2: ESRD with Active Dialysis
ESRD requiring chronic dialysis requires two codes: N18.6 (end-stage renal disease) and Z99.2 (dependence on renal dialysis). Neither code alone is complete for a dialysis encounter.
| Code | Description | When to Add |
|---|---|---|
| N18.6 | End-stage renal disease | Provider has documented ESRD; patient is on or being initiated on chronic dialysis. |
| Z99.2 | Dependence on renal dialysis | Always added when N18.6 is coded and dialysis is active. |
| N18.5 | CKD stage 5 (no dialysis) | GFR below 15 but dialysis has not started. Never use with Z99.2. |
Kidney Transplant Status: Z94.0 with Ongoing CKD
A kidney transplant does not eliminate CKD. Transplant patients may still meet criteria for CKD stages if the graft provides partial but not complete restoration of renal function. When CKD persists after transplant, code the N18 stage plus Z94.0 (kidney transplant status). Z94.0 signals transplant status without implying a transplant complication.
| CODING RULE — Transplant vs. Complication: Having CKD after a kidney transplant does not mean there is a transplant complication. Code the CKD stage (N18.x) plus Z94.0 for transplant status. Only use T86.1x codes (kidney transplant complications) when the provider explicitly documents a complication such as rejection or failure. |
CKD Manifestation and Comorbidity Codes
CKD frequently generates secondary diagnoses that carry their own billing weight. These manifestation codes are never first-listed. They always follow the underlying N18 stage code.
| Code | Description | Sequencing Rule | Common Stage |
|---|---|---|---|
| D63.1 | Anemia in CKD | Always after N18.x. Never first-listed. | Stages 3 through 5 and ESRD |
| N25.81 | Secondary hyperparathyroidism, renal origin | After N18.x. Separate from primary hyperparathyroidism. | Stages 4, 5, and ESRD |
| E87.5 | Hyperkalemia | Code when documented and managed separately from CKD. | Stages 4, 5, and ESRD |
| N17.9 | Acute kidney failure, unspecified (AKI) | Code both N17.9 and N18.x when AKI occurs on top of CKD. | Any CKD stage |
| R94.4 | Abnormal results of kidney function studies | Pair with N18.x when abnormal GFR is the only documented finding. | Any stage |
| CRITICAL RULE — D63.1 Sequencing: Submitting D63.1 (anemia in CKD) as a standalone code or as first-listed will trigger an automatic denial. The underlying CKD code (N18.x) must precede D63.1 on every claim. This is an ICD-10-CM mandatory coding convention, not a payer-specific rule. |
Code Sequencing Rules
Correct code sequencing is essential in CKD billing because ICD-10-CM guidelines determine which diagnosis must be reported first based on the reason for the encounter and the care setting. Sequencing rules also change when CKD is documented with related conditions such as hypertension, diabetes, ESRD, or acute kidney injury (AKI).
Outpatient Sequencing Rules
In outpatient settings, the first-listed diagnosis is the condition chiefly responsible for services rendered in that encounter. Section IV of the ICD-10-CM guidelines governs outpatient coding.
- If the encounter is for established CKD management, the N18 stage code or appropriate I12 combination code is first-listed.
- If both hypertension and CKD are documented, the I12 combination code is first-listed, not I10.
- If both diabetes and CKD are documented, the E-code combination (e.g., E11.22) is first-listed.
- Symptoms integral to the CKD diagnosis (e.g., fatigue, edema) are not separately coded per Section IV.J.
- AKI on CKD requires both N17.9 and the appropriate N18.x code; sequence N17.9 first when AKI is the primary reason for the encounter.
Inpatient Sequencing Rules
In inpatient settings, the principal diagnosis is the condition established after study to be chiefly responsible for the admission. The UHDDS definition governs.
- If admitted for CKD management or a CKD complication, the N18 stage code (or I12 combination code) is the principal diagnosis.
- If admitted for AKI occurring on a background of CKD, N17.9 is the principal diagnosis; N18.x is added as a secondary code.
- ESRD patients admitted for dialysis complications: N18.6 is principal; Z99.2, CPT access codes, and complication codes follow.
- Anemia managed during admission is coded with D63.1 as additional; N18.x remains the principal unless anemia is the sole reason for admission.
Documentation Requirements for Each CKD Code
Documentation drives code selection in CKD billing. Each N18 code has specific requirements that must be present at the time of claim submission.
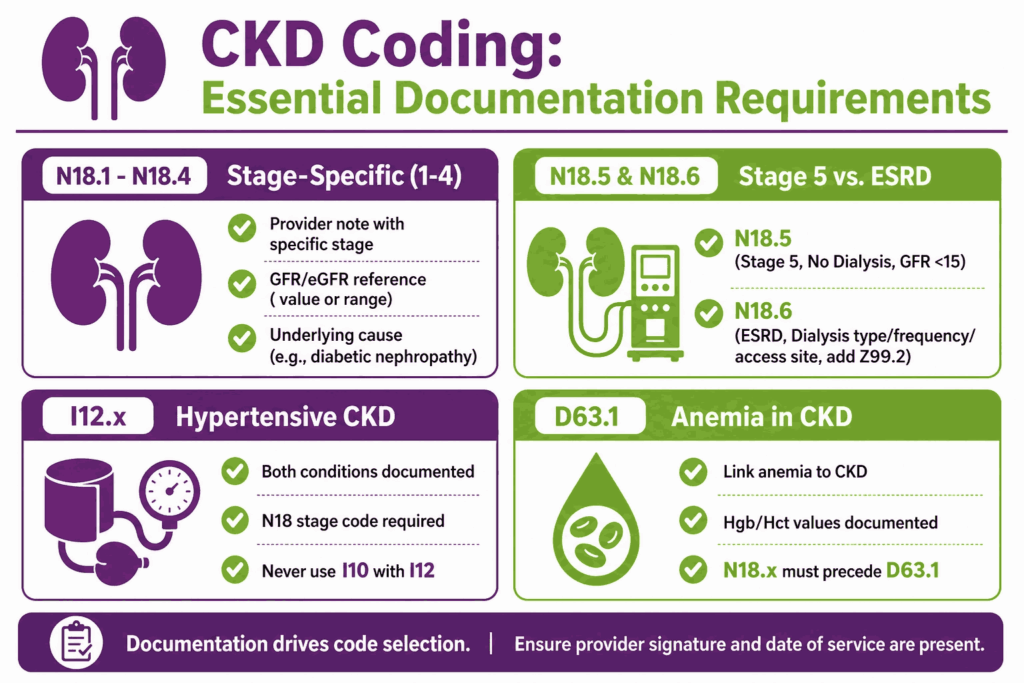
N18.1 through N18.4: Stage-Specific Documentation
- Provider note or problem list documenting the specific CKD stage (e.g., CKD stage 3b).
- Recent GFR or eGFR value referenced in the clinical note, linking the lab value to the stage.
- Documentation of the underlying cause (e.g., diabetic nephropathy, hypertensive nephropathy, glomerulonephritis) when known.
- Provider signature with date of service.
N18.5: Stage 5 CKD without Dialysis
- Provider explicitly documents CKD stage 5 or GFR below 15.
- Dialysis has not started or has been declined and documentation supports pre-dialysis status.
- ESRD should not appear in the documentation if N18.5 is used; query provider if conflicting language exists.
N18.6: ESRD
- Provider explicitly documents ESRD or end-stage renal disease.
- Dialysis type and frequency documented (hemodialysis or peritoneal dialysis).
- Access site documented (fistula, graft, or catheter) for dialysis claims.
- Z99.2 added to every claim where active dialysis is taking place.
I12.x: Hypertensive CKD Combination Codes
- Both hypertension and CKD documented in the same encounter.
- Provider has not stated the conditions are unrelated.
- N18 stage code always required alongside I12.x.
- I10 must not appear on the same claim when I12 is used.
D63.1: Anemia in CKD
- Provider documents anemia and links it to CKD (e.g., anemia of chronic kidney disease).
- Hemoglobin or hematocrit value referenced in the note.
- N18.x stage code must precede D63.1 on the claim.
- If iron deficiency anemia is also present, add D50.x as an additional code.
CPT Codes Commonly Paired with CKD ICD-10 Codes
ICD-10 codes establish medical necessity for every CPT code submitted in the same encounter. Mismatched or incomplete diagnosis codes fail medical necessity review at the claim scrubber level. Because navigating these dual code-mapping layers requires specialized expertise, many practices utilize professional nephrology billing services to ensure automated claim scrubbing rules align perfectly with actual clinical outputs.
| CPT Code | Description | ICD-10 Pairing Notes |
|---|---|---|
| 90935 | Hemodialysis, single eval | N18.6 plus Z99.2. Requires ESRD documentation; N18.5 will not support hemodialysis CPT codes. |
| 90945 | Peritoneal dialysis, single eval | N18.6 plus Z99.2. Same rule applies as hemodialysis. |
| 90951 to 90962 | Monthly ESRD-related services by physician | N18.6 and Z99.2 required. CPT selection is also age-driven (under 2, 2 to 11, 12 to 19, 20 and above). |
| 36800 to 36821 | Dialysis access creation (AV fistula, graft) | N18.6 primary; Z99.2 if dialysis is already active. |
| 99213 to 99215 | Office visit, established patient | N18.x or I12.x as first-listed; add comorbidity codes. Complexity level drives E/M selection. |
| 99354 to 99355 | Prolonged service, office visit | CKD-related encounters with documented time exceeding standard thresholds. N18.x primary. |
| 93990 | Duplex scan, hemodialysis access | N18.6 plus Z99.2. Pairs with access surveillance in ESRD patients. |
| 86235 | Antinuclear antibody testing | Pairs with N18.x when CKD workup includes autoimmune etiology evaluation. |
Common Denial Patterns in CKD Billing
Most CKD-related claim denials fall into one of five categories. Identifying the root cause prevents recurring revenue loss.
| Denial Type | Root Cause | Fix |
|---|---|---|
| Non-specific code | N18.9 used when stage is documented in the chart | Query provider for stage documentation; use stage-specific N18.x code. |
| I10 alongside N18.x | Hypertension coded as I10 instead of I12 combination code | When hypertension and CKD coexist and are not documented as unrelated, use I12.x, not I10. |
| D63.1 first-listed | Anemia in CKD submitted as primary or standalone diagnosis | Always sequence N18.x before D63.1. Never use D63.1 alone. |
| N18.5 for dialysis patient | CKD stage 5 coded when patient is actively on dialysis | When chronic dialysis is active and ESRD is documented, use N18.6 plus Z99.2. |
| Missing Z99.2 | N18.6 submitted without Z99.2 for active dialysis encounter | Add Z99.2 to every dialysis-related claim where N18.6 is used. |
| Lab-only stage assignment | Coder assigns CKD stage from GFR value without provider documentation | Code only what the provider has documented. Query before assigning a stage from labs. |
| DENIAL SCENARIO — I10 Error: A primary care provider documents hypertension and CKD stage 3a in the SOAP note. The coder assigns I10 for hypertension and N18.31 for CKD as separate codes. The claim clears the scrubber but fails an audit. The correct code sequence is I12.9 (hypertensive CKD stages 1 to 4), then N18.31. I10 must not appear when the assumed causal link between hypertension and CKD is present. |
CKD Coding in Risk Adjustment and Value-Based Models
CKD stage codes carry significant weight in risk-adjusted payment models, including Medicare Advantage, ACO programs, and CMS-HCC scoring. Unspecified CKD (N18.9) contributes a lower risk-adjustment factor than stage-specific codes. Stage 4 and stage 5 codes generate substantially higher HCC values than stages 1 and 2.
In value-based care contracts, chronic condition recapture requires CKD to be coded at every eligible encounter. A patient with stage 3b CKD must receive N18.32 (not N18.9) on every annual wellness visit and qualifying chronic care management encounter.
Because missing these specific tracking thresholds can result in thousands of dollars in lost risk-adjusted revenue, partnering with experienced nephrology billing companies is often the most reliable way for independent practices to safeguard their collections and maintain compliance under modern HCC models.
| Code | HCC Category | Risk Adjustment Impact |
|---|---|---|
| N18.1 to N18.2 | CKD stages 1 to 2 | Lower HCC weight. Specificity still required over N18.9. |
| N18.30 to N18.32 | CKD stage 3 | Moderate HCC weight. Subcodes (3a, 3b) preferred over unspecified 3. |
| N18.4 | CKD stage 4 (severe) | High HCC weight. Frequently undercoded due to provider documentation gaps. |
| N18.5 to N18.6 | CKD stage 5 and ESRD | Highest HCC weight. ESRD carries the maximum risk-adjustment factor in this category. |
| N18.9 | CKD, unspecified | Lowest HCC weight. Avoid in any risk-adjusted model. Query provider for stage. |






