")
Summary: “Epilepsy is reported under ICD-10-CM category G40, with every billable code requiring two specificity layers: intractability status and presence or absence of status epilepticus. The most-billed codes are G40.909 (unspecified epilepsy, not intractable, without status epilepticus), G40.919 (unspecified, intractable), G40.209/G40.219 (focal symptomatic epilepsy with complex partial seizures), and G40.309/G40.319 (generalized idiopathic epilepsy).”
Epilepsy affects more than 3.4 million Americans and generates recurring claims across neurology, primary care, emergency medicine, and hospital settings. It is also one of the most frequently miscoded neurological conditions. The wrong diagnosis code can turn a chronic neurological disorder into an unreimbursed symptom claim.
Documentation remains the biggest coding risk. CMS reported a 6.55% improper payment rate in Medicare fee-for-service for FY 2025, with insufficient documentation remaining one of the leading causes of payment errors. For epilepsy, reimbursement depends on accurately capturing seizure type, intractability status, and status epilepticus within the ICD-10 G40 code family.
Missing any of these elements can trigger denials, downcoding, or delayed payment. The risk works both ways. Undercoding leaves legitimate revenue uncollected, while overcoding increases audit exposure and payer scrutiny.
This guide explains the complete G40 code family, when to code epilepsy versus seizures, and how to apply intractability and status epilepticus classifications correctly. Every section connects code selection to documentation requirements, claim approval, and reimbursement outcomes.
What Is the ICD-10 Code for Epilepsy?
There is no single ICD-10 code for epilepsy. Epilepsy uses the G40 code family under Chapter 6, Diseases of the Nervous System. The exact code depends on seizure type, intractability, and whether status epilepticus is present.
The most common default is G40.909, epilepsy, unspecified, not intractable, without status epilepticus. Coders use it when epilepsy is confirmed, but the record lacks detail. Specific documentation should move the claim to a more precise code.
Here is the quick-reference table for epilepsy ICD-10 codes:
| Condition | ICD-10 Code | Meaning |
|---|---|---|
| Epilepsy, unspecified | G40.909 | Confirmed epilepsy, no further detail |
| Seizure disorder | G40.909 | Coded as epilepsy when documented as a disorder |
| Single seizure, no epilepsy | R56.9 | Unspecified convulsions, symptom only |
| Intractable epilepsy | G40.919 | Drug-resistant, without status epilepticus |
Epilepsy vs. Seizure vs. Convulsion: The Coding Distinction That Prevents Denials
The biggest coding error in this space is treating a seizure and epilepsy as the same thing. They are not. A seizure is a single event. Epilepsy is a chronic disorder of two or more unprovoked seizures.
This distinction decides which ICD-10 chapter you code from. It also decides whether the claim carries risk-adjustment value. Payers read these two code groups very differently.
The rule that trips up most providers comes straight from payer guidance:
- Document “seizure” alone, and the patient codes to R56.9, unspecified convulsions.
- Document “seizure disorder” or “recurrent seizures,” and the patient codes to G40.909, epilepsy.
- Document a provoked event such as fever or trauma, and you stay in the R56 symptom range.
Why the R56 vs. G40 Choice Affects Reimbursement
The financial gap between these codes is distinct. R56.9 is a symptom code and carries no HCC under CMS-HCC risk adjustment. G40 epilepsy codes map to an HCC and add RAF weight to the patient’s risk profile.
That means a patient with true epilepsy coded as R56.9 is under-represented to the payer. The practice loses risk-adjusted revenue and weakens medical necessity for ongoing care. For value-based contracts, this gap compounds across the panel. Partnering with the best neurology billing services ensures your team has the algorithmic rules and auditing tools in place to capture this missing risk-adjusted revenue automatically.
| Feature | Seizure Codes (R56.9) | Epilepsy Codes (G40) |
|---|---|---|
| Medical meaning | Single or isolated event | Chronic neurological disorder |
| ICD-10 chapter | Symptoms and signs (R) | Nervous system diseases (G) |
| Risk adjustment | No HCC value | Maps to an HCC, adds RAF |
| Billing message | Acute or one-time care | Long-term condition management |
| Use case | First seizure, diagnostic workup | Confirmed epilepsy follow-up |
Complete Epilepsy ICD-10 Code List (G40 Category, 2026)
The G40 category covers every confirmed form of epilepsy. The fourth character names the seizure type or syndrome. Additional characters define intractability and status epilepticus, which the next section explains in full.
Below is the category-level map you can reference before working on a billable code:
| Code | Category | When It Applies |
|---|---|---|
| G40.0 | Localization-related (focal) idiopathic epilepsy | Focal onset, no identified cause |
| G40.1 | Localization-related symptomatic, simple partial | Focal seizures, awareness preserved |
| G40.2 | Localization-related symptomatic, complex partial | Focal seizures with impaired awareness |
| G40.3 | Generalized idiopathic epilepsy | Both hemispheres, no identified cause |
| G40.4 | Other generalized epilepsy | Generalized, not otherwise classified |
| G40.5 | Epileptic seizures related to external causes | Alcohol, drugs, hormonal, sleep deprivation |
| G40.8 | Other epilepsy and recurrent seizures | Named syndromes and other types |
| G40.9 | Epilepsy, unspecified | Confirmed epilepsy, no further detail |
The G40.A and G40.B subcategories were added to capture specific syndromes. These are easy to miss because they break the numeric pattern.
- G40.A covers absence epileptic syndrome, including childhood and juvenile absence epilepsy.
- G40.B covers juvenile myoclonic epilepsy, also known as Janz syndrome.
- G40.81 covers Lennox-Gastaut syndrome, a severe childhood-onset epilepsy.
- G40.82 covers epileptic spasms, including infantile spasms.
Focal (Localization-Related) Epilepsy: G40.0 to G40.2
Focal epilepsy starts in one area of the brain. The code depends on whether the cause is idiopathic or symptomatic and whether awareness is preserved. Temporal lobe epilepsy most often codes here under the complex partial group.
These three subcategories each expand into four billable codes. The endings follow the standard 0/1 intractability and 1/9 status pattern.
| Billable Code | Description |
|---|---|
| G40.001 | Focal idiopathic, not intractable, with status epilepticus |
| G40.009 | Focal idiopathic, not intractable, without status epilepticus |
| G40.011 | Focal idiopathic, intractable, with status epilepticus |
| G40.019 | Focal idiopathic, intractable, without status epilepticus |
| G40.101 | Focal symptomatic, simple partial, not intractable, with status |
| G40.109 | Focal symptomatic, simple partial, not intractable, without status |
| G40.111 | Focal symptomatic, simple partial, intractable, with status |
| G40.119 | Focal symptomatic, simple partial, intractable, without status |
| G40.201 | Focal symptomatic, complex partial, not intractable, with status |
| G40.209 | Focal symptomatic, complex partial, not intractable, without status |
| G40.211 | Focal symptomatic, complex partial, intractable, with status |
| G40.219 | Focal symptomatic, complex partial, intractable, without status |
In practice, G40.209 is one of the most-used focal codes. It captures the typical temporal lobe presentation with impaired awareness and no status event. Move to G40.219 only when the record documents drug resistance.
Generalized Epilepsy: G40.3 and G40.4
Generalized epilepsy involves both hemispheres at onset. G40.3 covers idiopathic generalized epilepsy with no identified cause. G40.4 covers other generalized epilepsies that do not fit the standard classification.
Tonic-clonic, also called grand mal, presentations code within this generalized range. The four-code split repeats the same intractability and status logic.
| Billable Code | Description |
|---|---|
| G40.301 | Generalized idiopathic, not intractable, with status epilepticus |
| G40.309 | Generalized idiopathic, not intractable, without status epilepticus |
| G40.311 | Generalized idiopathic, intractable, with status epilepticus |
| G40.319 | Generalized idiopathic, intractable, without status epilepticus |
| G40.401 | Other generalized, not intractable, with status epilepticus |
| G40.409 | Other generalized, not intractable, without status epilepticus |
| G40.411 | Other generalized, intractable, with status epilepticus |
| G40.419 | Other generalized, intractable, without status epilepticus |
Named Syndromes: G40.8, G40.A, and G40.B
The syndrome codes need extra attention because their endings break the standard pattern. The G40.8 subcategories use a 1/2/3/4 sixth character instead of 01/09/11/19. Coders who apply the focal pattern here will pick the wrong code.
| Billable Code | Description |
|---|---|
| G40.811 | Lennox-Gastaut, not intractable, with status epilepticus |
| G40.812 | Lennox-Gastaut, not intractable, without status epilepticus |
| G40.813 | Lennox-Gastaut, intractable, with status epilepticus |
| G40.814 | Lennox-Gastaut, intractable, without status epilepticus |
| G40.821 | Epileptic spasms, not intractable, with status epilepticus |
| G40.822 | Epileptic spasms, not intractable, without status epilepticus |
| G40.823 | Epileptic spasms, intractable, with status epilepticus |
| G40.824 | Epileptic spasms, intractable, without status epilepticus |
| G40.A09 | Absence epileptic syndrome, not intractable, without status |
| G40.A19 | Absence epileptic syndrome, intractable, without status |
| G40.B09 | Juvenile myoclonic epilepsy, not intractable, without status |
| G40.B19 | Juvenile myoclonic epilepsy, intractable, without status |
Unspecified Epilepsy: G40.9
G40.9 is the fallback when epilepsy is confirmed, but the type is not documented. It carries the standard four-code split shown earlier in the character-logic table. Use it as a starting point, not a permanent label.
The goal is always to replace G40.909 with a typed code as documentation improves. Repeated unspecified coding across visits is a known audit trigger, covered later in this guide.
How to Read a G40 Code: The 5th and 6th Character Logic
A G40 code is a decision tree, not a single label. Once you pick the seizure type, two more decisions complete the code. These are intractability and status epilepticus. Most coders lose accuracy here because they default to the unspecified ending. The fifth and sixth characters carry clinical and financial weight. Utilizing top epilepsy billing services can safeguard your revenue cycle, as specialized teams deploy continuous clinical documentation improvement (CDI) audits to capture these precise final digits before claims are ever generated.
Most coders lose accuracy here because they default to the unspecified ending. The fifth and sixth characters carry clinical and financial weight. Reading them correctly is what separates a clean claim from a denial.
The two final decisions follow a fixed pattern across most G40 subcategories:
- Fifth character (intractability): 0 means not intractable, 1 means intractable.
- Sixth character (status epilepticus): 1 means with status epilepticus, 9 means without status epilepticus.
Here is how that logic plays out using the unspecified G40.9 family:
| Code | Intractable? | Status Epilepticus? |
|---|---|---|
| G40.909 | No | No |
| G40.901 | No | Yes |
| G40.919 | Yes | No |
| G40.911 | Yes | Yes |
The same 0/1 and 1/9 pattern repeats for focal and generalized codes. For example, G40.009 is focal idiopathic, not intractable, without status. G40.019 is the intractable version of the same seizure type.
Intractable (Drug-Resistant) Epilepsy Coding
Intractable epilepsy is a high-value code that requires clear documentation. The International League Against Epilepsy (ILAE) defines it as failure of two appropriate antiepileptic drug trials. The drugs must be adequately dosed and tolerated.
This matters for risk adjustment. Intractable epilepsy codes carry greater clinical severity and support continued advanced care. Payers expect the record to prove the medication failures, not just state the label.
Several documented terms are treated as equivalent to intractable in ICD-10-CM:
- Refractory
- Drug-resistant
- Medically resistant
- Poorly controlled
- Treatment-resistant
When a provider uses any of these terms, the coder should select the intractable fifth character. A common mistake here is coding a patient on three antiepileptic drugs as not intractable simply because the word “intractable” never appears. The equivalent terms count.
Status Epilepticus: The High-Severity Coding Axis
Status epilepticus is the most severe presentation captured in the G40 family. It is a prolonged seizure or a cluster of seizures without recovery between them. The sixth character flags it, and that flag carries weight in both clinical and billing review.
Coders should treat status epilepticus as a separate decision from intractability. A patient can be intractable without status, or have a status event without being labeled intractable. The two axes combine into the four-code split shown earlier.
The documentation must support the status finding directly. Look for these signals in the record:
- A seizure lasting five minutes or longer
- Repeated seizures without return to baseline between events
- Emergency intervention to stop ongoing seizure activity
- Provider use of the term “status epilepticus” or “status.”
A status epilepticus code often accompanies emergency or inpatient care. That setting affects DRG assignment and expected reimbursement. When the record supports status, coding it captures the true severity and the resources used. Leaving it off understates the encounter and the claim.
Seizure Codes Without Epilepsy (R56 Category)
Not every seizure is epilepsy. The R56 category handles single, provoked, or unconfirmed seizure events. Using R56 correctly keeps you compliant when epilepsy has not been established.
These codes belong to the symptoms chapter, so they signal acute rather than chronic care. Do not assign R56 codes once the provider confirms epilepsy. The patient should move to a G40 code at that point.
The R56 codes you will use most often are below:
| Code | Meaning | When It Applies |
|---|---|---|
| R56.00 | Simple febrile convulsions | Fever-related seizure, uncomplicated |
| R56.01 | Complex febrile convulsions | Fever-related, prolonged or focal |
| R56.1 | Post-traumatic seizures | Acute seizure after head trauma |
| R56.9 | Unspecified convulsions | Single or unconfirmed seizure event |
Two related codes sit outside the R56 range but belong in this discussion. F44.5 captures psychogenic non-epileptic seizures, also called conversion disorder with seizures. These are confirmed when the EEG is normal during a clinical event.
Provoked seizures from alcohol withdrawal or metabolic causes also stay out of the G40 range. An alcohol withdrawal seizure is coded to the withdrawal condition with a seizure descriptor, not to epilepsy. The trigger defines the code.
Specialty-Specific Coding Notes
Epilepsy coding shifts by specialty because patient populations differ. The same G40 family applies, but the common codes and pitfalls change. Aligning code selection with the specialty reduces denials.
These notes reflect the buyer specialties most affected by seizure coding:
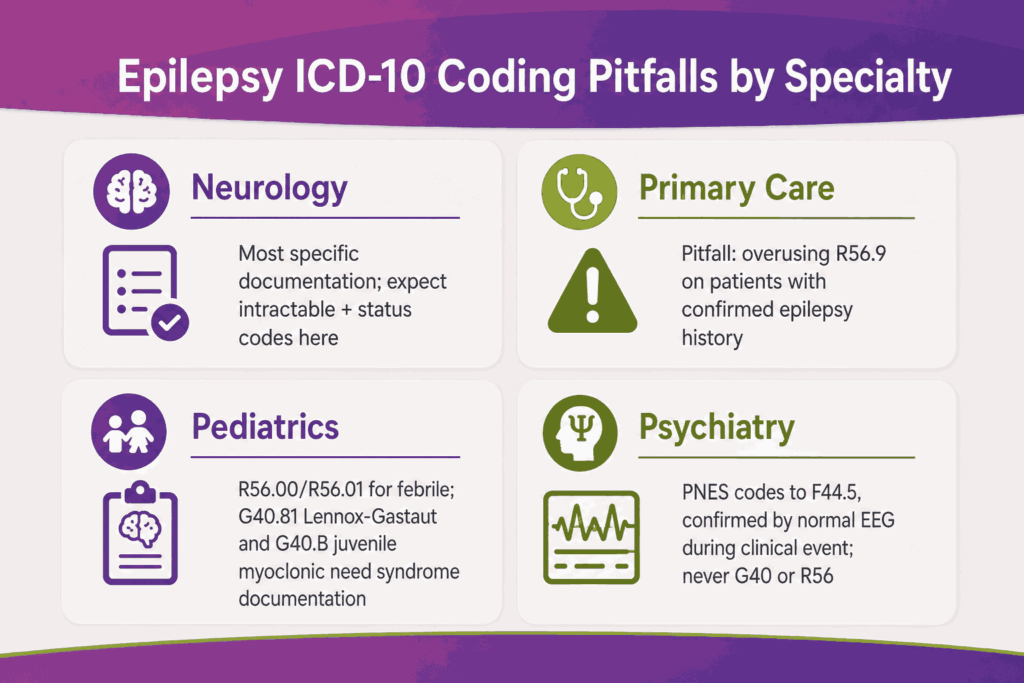
Neurology
Neurology carries the most specific epilepsy documentation. Coders should expect seizure type, frequency, EEG findings, and medication response. This is where intractable and status epilepticus codes appear most often, and navigating these fields seamlessly requires using the top EMRs for neurology billing to ensure high-severity indicators auto-populate without manual data gaps.
Primary Care
Primary care often sees the first seizure or ongoing maintenance visits. The risk here is overusing R56.9 for patients with a confirmed epilepsy history. When the record references an established diagnosis, code the G40 condition.
Pediatrics
Pediatric coding centers on febrile seizures and childhood syndromes. R56.00 and R56.01 handle febrile events. Lennox-Gastaut (G40.81) and juvenile myoclonic epilepsy (G40.B) require specific syndrome documentation.
Psychiatry and Behavioral Health
Psychiatry encounters psychogenic non-epileptic seizures coded to F44.5. The diagnosis depends on EEG confirmation that no epileptic activity occurred. Coding these as G40 or R56 misrepresents the clinical picture and invites denials.
History of Epilepsy and Resolved Seizures (Z-Codes)
Z-codes capture conditions that no longer require active treatment but still affect care. They matter for anesthesia planning, medication reviews, and surveillance visits. Using them correctly avoids coding a resolved condition as active.
Two Z-codes apply to seizure and epilepsy history:
- Z86.69 covers personal history of other diseases of the nervous system, used for a resolved personal seizure history.
- Z82.0 covers family history of epilepsy and other nervous system diseases.
Do not assign a history Z-code while the patient remains on antiepileptic therapy for active control. A personal history code is appropriate only when the record shows the condition is resolved. The provider should attest to remission or discontinued treatment.
Documentation Requirements for Clean Epilepsy Claims
Code specificity depends entirely on what the provider writes. Official ICD-10 guidelines state that accurate coding is impossible without complete documentation. The note must carry the details the code demands.
For epilepsy, the record needs five elements to support a specific G40 code:
- Seizure type (focal, generalized, or named syndrome)
- Intractability status, using a recognized term
- Presence or absence of status epilepticus
- Treatment plan and medication response
- Underlying etiology, when known
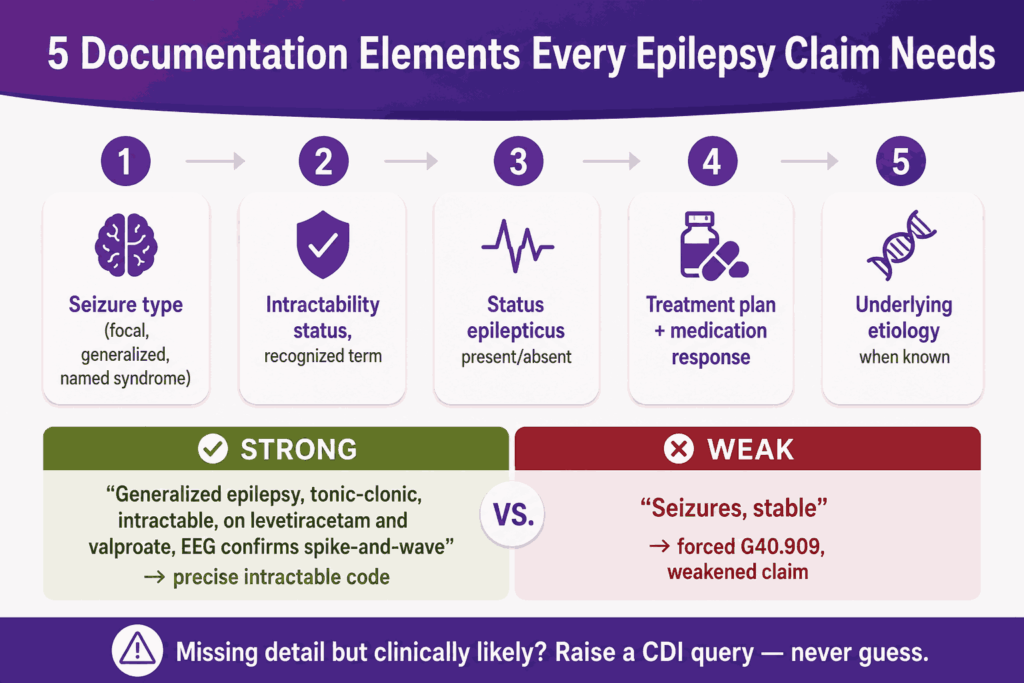
A strong note reads like a billable code. Consider this example: “Generalized epilepsy with tonic-clonic seizures, intractable, on levetiracetam and valproate, with EEG confirming generalized spike-and-wave.” That single sentence supports a precise intractable code.
A weak note simply states “seizures, stable.” That phrasing forces an unspecified code and weakens the claim. When detail is missing but clinically likely, the coder should raise a clinical documentation improvement (CDI) query rather than guess.
A Worked CDI Query Example
The CDI query is the tool that turns a vague note into a billable code. It asks the provider to clarify, without leading them to a specific answer. Here is how one plays out in a real epilepsy encounter.
The starting note: “Patient followed for seizures. Continue levetiracetam and lamotrigine. Recent breakthrough seizure last month. Plan: add third agent.”
| Query Element | Content |
|---|---|
| What is unclear | Seizure type and intractability status are not stated |
| Clinical clue | Two failed agents plus a breakthrough event suggests drug resistance |
| Query wording | “Please clarify the seizure type and whether the epilepsy is intractable, based on response to current therapy.” |
| Likely outcome | Provider confirms intractable focal epilepsy |
| Resulting code | G40.219 instead of G40.909 |
That single query moves the claim from an unspecified code to an intractable focal code. The coding shift adds risk-adjustment weight and strengthens medical necessity for the third agent. The query is documented in the record as audit support.
Common Epilepsy Coding Mistakes and Denials
Most epilepsy denials trace back to a small set of repeat errors. They are predictable, which means they are preventable. Catching them before submission protects both revenue and audit standing. To achieve this, dedicated neurology billing companies design customized front-end scrubbing edits that freeze claims containing conflicting clinical data, allowing practices to fix errors proactively.
The errors that generate the most denials and audit flags are below:
- Lingering R56.9 after diagnosis. Keeping a symptom code on record after epilepsy is confirmed signals diagnostic uncertainty to auditors.
- Chronic unspecified overuse. Repeated G40.909 use across visits, when detail exists, flags the record for lack of specificity.
- Missing intractability. Failing to code intractable when equivalent terms appear understates severity and loses RAF value.
- Symptom-coding established epilepsy. Coding R56.9 for a known epilepsy patient’s breakthrough seizure misrepresents the encounter.
A breakthrough seizure deserves special attention. When a patient with known epilepsy has a breakthrough event, you code the underlying epilepsy, not R56.9. The chronic condition drives the visit, so the G40 code carries the claim.
The table below maps each error to its denial reason and the corrective action:
| Coding Error | Why Claims Get Denied | Corrective Action |
|---|---|---|
| R56.9 after epilepsy confirmed | Symptom code fails medical necessity for chronic care | Recode to the established G40 type |
| Repeated G40.909 use | Lack of specificity flags the record for audit | Query for type, then assign a typed code |
| Intractable not coded | Severity understated, RAF value lost | Apply intractable character when terms appear |
| Wrong G40.8 ending | Pattern mismatch creates an invalid code | Use the 1/2/3/4 syndrome ending |
CPT Codes for Epilepsy Diagnosis and Management
A G40 diagnosis rarely bills alone. It supports the procedures and visits that make up an epilepsy encounter. Matching the diagnosis to the right CPT codes is what completes the claim.
Epilepsy services fall into four CPT groups. These are routine EEG, long-term EEG monitoring, neurostimulator services, and evaluation and management visits. Each group has its own coding logic and payer rules.
Routine EEG Codes
Routine EEG is the standard diagnostic study, recorded for under 24 continuous hours. Code selection depends on recording length and patient state. The G40 or R56 diagnosis establishes medical necessity for the study.
| CPT Code | Description |
|---|---|
| 95812 | EEG extended monitoring, 41 to 60 minutes |
| 95813 | EEG extended monitoring, 61 to 119 minutes |
| 95816 | EEG including recording awake and drowsy |
| 95819 | EEG including recording awake and asleep |
| 95822 | EEG recording in coma or sleep only |
One payer rule matters here. Medicare requires a routine EEG before an ambulatory continuous EEG, billed within one year of the ambulatory study. Skipping that sequence is a built-in denial.
Long-Term and Video EEG Monitoring (95700 Series)
Long-term monitoring replaced the old 95950 series codes in 2020. The structure splits the technical and professional work into separate codes. Three dimensions define each code: video use, recording duration, and the level of technologist monitoring.
| Code Range | Component | What It Covers |
|---|---|---|
| 95700 | Technical setup | Electrode application and patient education, once per recording |
| 95705 to 95716 | Technical, daily | Technologist review, by duration and monitoring level |
| 95717 to 95726 | Professional | Physician review and interpretation, with or without video |
| 95957 | Professional | Digital EEG analysis, often for surgical workups |
In practice, a 72-hour unmonitored ambulatory video EEG bills 95700 for setup. The technical work bills one daily unit per recording day, plus the matching professional code. Billing the professional code without the daily technical units is a common revenue leak.
Neurostimulator and Surgical Codes
Drug-resistant epilepsy often moves to device therapy. Vagus nerve stimulation (VNS) carries its own implant and programming codes. The intractable G40 diagnosis is what supports medical necessity for these services.
| CPT Code | Description |
|---|---|
| 64568 | VNS electrode and pulse generator implantation |
| 64569 | VNS electrode revision or replacement |
| 64570 | VNS electrode and generator removal |
| 95976 | Simple cranial nerve neurostimulator programming |
| 95977 | Complex cranial nerve neurostimulator programming |
E/M Codes for Epilepsy Visits
Office visits bill 99202 to 99215 based on medical decision making or time. Chronic epilepsy management typically supports moderate complexity. Inpatient epilepsy monitoring unit stays add initial and subsequent hospital care codes alongside the daily EEG codes.
Billing Modifiers for Epilepsy Claims
Modifiers tell the payer how a service relates to other services on the claim. Epilepsy billing relies on them heavily because EEG studies are split into components and often paired with visits. A missing or wrong modifier is one of the quietest denial sources in neurology billing.
The modifiers that appear most often on epilepsy claims are below:
| Modifier | Meaning | Epilepsy Use Case |
|---|---|---|
| 26 | Professional component | Physician interprets an EEG on hospital-owned equipment |
| TC | Technical component | Facility bills the recording when interpretation is billed elsewhere |
| 25 | Separate E/M, same day | Office visit plus a same-day EEG study |
| 95 | Synchronous telehealth | Virtual epilepsy medication follow-up visits |
| 59 | Distinct procedural service | Separate studies bundled by NCCI edits |
| 76 | Repeat procedure, same provider | Repeat EEG on the same date after an event |
| 24 | Unrelated E/M in global period | Epilepsy visit during the VNS implant global period |
| 52 | Reduced services | EEG study terminated before the full protocol |
The 26/TC Split in Practice
The professional and technical split deserves its own note. When the practice owns the EEG equipment and reads the study, it bills the global code with no modifier. When a hospital owns the equipment, the practice bills with modifier 26 and the facility bills TC.
Billing globally when only the interpretation was performed is an overpayment risk. Auditors recover those payments and flag the pattern. The ownership of the equipment decides the modifier each time.
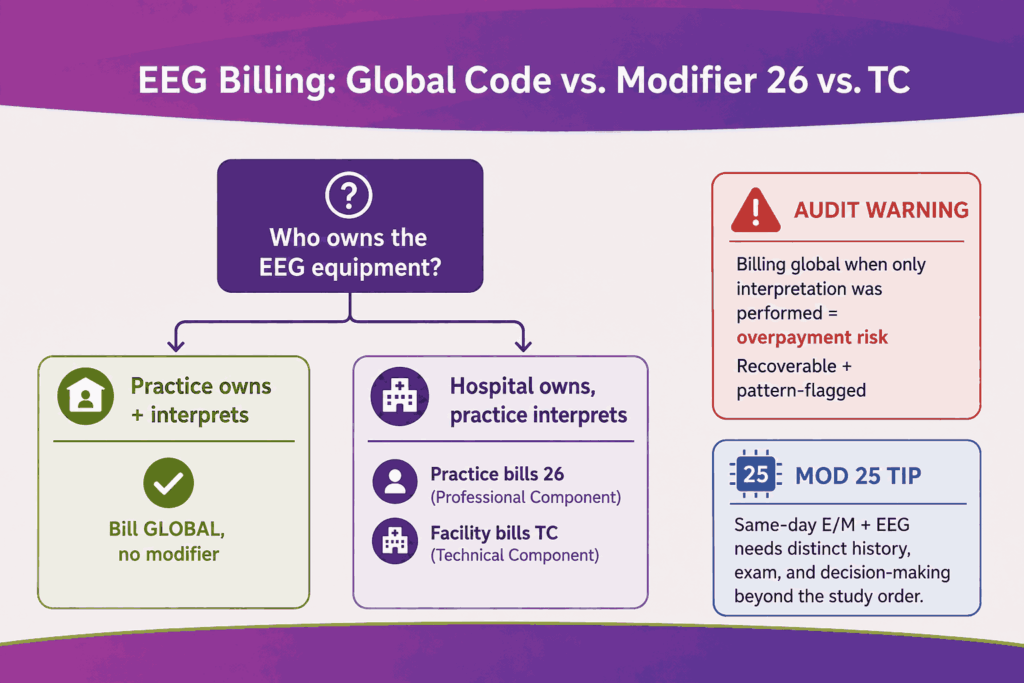
Modifier 25 Documentation Standard
Modifier 25 pairs an E/M visit with a same-day procedure. The visit must be significant and separately identifiable from the EEG itself. The note needs distinct history, exam, and decision-making content beyond the study order.
Payers audit modifier 25 aggressively across all specialties. For epilepsy claims, a medication change or new symptom documented at the visit supports the modifier. A note that only references the EEG does not.
What Changed for FY2026 Epilepsy Coding
Epilepsy coding stays current through annual ICD-10-CM updates and CMS risk-adjustment model changes. Two areas deserve a fresh review each year. These are the syndrome subcategories and the HCC mapping.
The points below reflect what RCM teams should verify for the current cycle:
- Syndrome codes remain split out. Absence syndrome (G40.A) and juvenile myoclonic epilepsy (G40.B) stay separate from the older numeric groups.
- Risk-adjustment weight sits with G40. The CMS-HCC v28 model continues to value epilepsy, while R56.9 carries no HCC.
- Intractable specificity drives RAF. Documented drug resistance keeps shifting claims to the higher-weighted intractable codes.
- Status epilepticus stays on a separate axis. The sixth character continues to flag this high-severity presentation.
Confirm the exact HCC number and any code additions against the current-year code set before publishing internal guidance. Risk models shift between versions, and the mapping should be checked rather than assumed. Your coding lead should validate the active assignment for your payer mix.
Conclusion
Epilepsy coding is a revenue decision as much as a clinical one. The seizure versus epilepsy choice, the intractability character, and the status epilepticus digit each affect reimbursement and risk adjustment. Specificity is what keeps claims clean.
The practices that win on epilepsy claims pair accurate documentation with disciplined coding and active CDI queries. If your seizure and epilepsy claims face repeat denials or under-coded risk, a coding accuracy review is the fastest path to recovering lost revenue.
FAQs
What is the ICD-10 code for seizure disorder?
A documented seizure disorder codes to G40.909, epilepsy, unspecified, not intractable, without status epilepticus. The phrase “seizure disorder” maps to epilepsy, not to the R56 symptom range.
Is G40.909 a billable code?
Yes. G40.909 is a billable six-character code. It applies when epilepsy is confirmed, but the record lacks type, intractability, or status detail.
What is the difference between G40.909 and G40.919?
Both are unspecified epilepsy codes without status epilepticus. G40.909 is not intractable, while G40.919 is intractable. The intractable code requires documented failure of appropriate drug trials.
What is the ICD-10 code for a breakthrough seizure?
A breakthrough seizure in a known epilepsy patient codes to the underlying G40 epilepsy code. Do not assign R56.9 when epilepsy is already established.
What is the code for tonic-clonic seizures?
Tonic-clonic, or grand mal, seizures code within the generalized epilepsy range based on the documented syndrome. The exact code depends on intractability and status epilepticus.
When should R56.9 be used instead of G40?
Use R56.9 for a single, isolated, or unconfirmed seizure event. Once the provider confirms epilepsy, move the patient to the appropriate G40 code.
What is the ICD-10 code for a febrile seizure?
A simple febrile seizure codes to R56.00 and a complex febrile seizure codes to R56.01. These are fever-related events and do not code as epilepsy.
What is the code for intractable epilepsy?
Intractable epilepsy uses the fifth character 1 within the relevant G40 type. For example, G40.219 is intractable focal epilepsy without status epilepticus.
How is status epilepticus coded?
Status epilepticus is captured by the sixth character within the G40 code. A “1” ending, such as G40.911, signals that status epilepticus is present.
What is the ICD-10 code for psychogenic non-epileptic seizures?
Psychogenic non-epileptic seizures code to F44.5, conversion disorder with seizures. The diagnosis requires EEG confirmation that no epileptic activity occurred.






