
CPT code 43239 reports an upper endoscopy with biopsy. The full name is esophagogastroduodenoscopy, flexible, transoral, with biopsy, single or multiple. Gastroenterologists use it across the upper digestive tract.
The code serves common GI conditions seen every day in the clinic. These include refractory GERD, Barrett’s esophagus, gastritis, peptic ulcers, celiac disease, and upper GI Crohn’s. Each one drives a biopsy decision documented in the note.
A defining rule sets 43239 apart from most codes. You report one unit per session, no matter how many biopsies you take. One forceps pass or twelve, the unit count stays the same.
43239 is also one of the most audit-sensitive codes in GI billing. Payers scrutinize the diagnosis link, the operative note, and the pathology order. This article covers the descriptor, 2026 reimbursement, clinical scenarios, billing rules, and the denial patterns that cost practices revenue.
What Is the 43239 CPT Code? (Description)
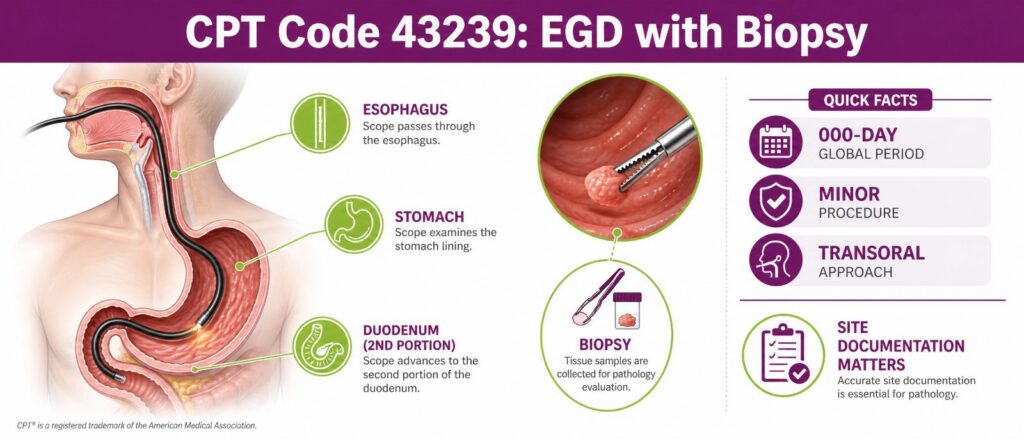
43239 describes a diagnostic upper endoscopy where the physician removes tissue for pathology. The scope passes through the mouth into the esophagus, stomach, and duodenum. The biopsy makes it 43239 rather than the base diagnostic code.
The code falls in the surgery section of the CPT manual. It carries a 000-day global period, which marks it as a minor procedure. That global period shapes how same-day evaluation services get paid.
Official 43239 Code Descriptor and Anatomy Covered
The American Medical Association (AMA) defines 43239 with precise anatomy. The flexible scope enters transorally and examines three regions in one pass.
- Esophagus, from the upper sphincter to the gastroesophageal junction.
- Stomach, including the cardia, body, antrum, and pylorus.
- Duodenum, through at least the second portion, in a complete exam.
The biopsy may come from any of these regions. Site documentation matters because payers tie the diagnosis to the biopsy location during review.
What 43239 Includes vs. Excludes
43239 covers the diagnostic exam plus tissue sampling with forceps. It does not cover therapeutic work performed through the same scope. Mixing those up is a frequent coding error.
| Included in 43239 | Excluded from 43239 |
|---|---|
| Full upper endoscopic exam | Polyp or lesion removal (use 43250 or 43251) |
| Forceps biopsy, single or multiple | Control of active bleeding (use 43255) |
| Diagnostic tissue sampling | Dilation, ablation, or stent placement |
| Pathology specimen collection | Foreign body removal |
When the physician removes a polyp by snare, the correct code is the polypectomy code, not 43239. Biopsy of a separate, distinct lesion may still qualify for a separate code with the right modifier.
The “Single or Multiple” Rule: Why You Report Only One Unit
The descriptor ends in “single or multiple” for a reason. CMS and the AMA bundle every biopsy from the session into one unit of 43239. Quantity does not change the code or the units.
A common mistake here is billing 43239 with two or three units after multiple biopsies. That triggers a Medically Unlikely Edit denial almost every time. The Medically Unlikely Edit (MUE) for 43239 reflects the single-unit design.
You capture the extra work through documentation, not units. Note each biopsy site and the number of specimens in the operative report. The pathology requisition should match those sites line for line.
43239 vs. 43235, 43236, 43250, 43251, 43255
The upper endoscopy family shares one base exam with different add-on actions. Choosing the wrong sibling code is a top driver of bundling denials. The table below maps the distinctions.
| Code | Descriptor | Biopsy? | When to Use |
|---|---|---|---|
| 43235 | EGD, diagnostic, with or without collection of specimen by brushing or washing | No forceps biopsy | Visual exam only, no tissue removed by forceps |
| 43236 | EGD with directed submucosal injection | No | Injection therapy, such as for varices or marking |
| 43239 | EGD with biopsy, single or multiple | Yes, forceps | Tissue sampling for pathology |
| 43250 | EGD with removal of tumor or polyp by hot biopsy forceps | Removal, not sampling | Polyp removal by hot biopsy or cautery |
| 43251 | EGD with removal of tumor or polyp by snare | Removal, not sampling | Polyp or lesion removal by snare technique |
| 43255 | EGD with control of bleeding, any method | No | Active bleeding control during the exam |
Use 43239 only when the goal is tissue diagnosis. The moment the physician removes a lesion or controls bleeding, the code changes. Clinicians can review a comprehensive CPT codes guide for a deeper breakdown of the base exam, including the diagnostic EGD criteria for 43235. When polyps come out, the EGD polypectomy codes 43250 and 43251 apply instead.
43239 Reimbursement and Cost
43239 payment depends heavily on where the procedure happens. The physician fee, the facility fee, and the site of service all move the number. A single national dollar figure rarely tells the whole story.
Medicare sets the baseline through the Physician Fee Schedule. Commercial payers negotiate from there, often as a percentage of Medicare. Knowing the components lets you forecast the allowable with accuracy.
2026 Medicare Physician Fee Schedule Rate for 43239
CMS calculates payment by multiplying total RVUs by the conversion factor. For 2026, the non-QP conversion factor is $33.4009. Qualifying APM participants use $33.5675 instead.
The work RVU of 2.33 already reflects the 2026 efficiency adjustment of negative 2.5 percent on non-time-based codes. The table shows the values and the resulting national payment by setting.
| Component | Facility setting | Non-facility (office) |
|---|---|---|
| Work RVU | 2.33 | 2.33 |
| Practice Expense RVU (approx.) | ~1.10 | ~9.94 |
| Malpractice RVU (approx.) | ~0.27 | ~0.27 |
| Total RVU | 3.70 | 12.54 |
| National payment (CF $33.4009) | ~$124 | ~$419 |
The practice expense split drives the gap between the two settings. In an office, the practice owns the scope, the room, and the staff time. In a facility, those costs shift to the facility fee instead.
Note: Confirm the exact PE and MP RVU values in the current CMS RVU26 file before publishing client-facing rate sheets. The totals above are verified; the component split is derived.
Facility vs. Non-Facility and ASC/OPPS Differences
Most 43239 procedures run in a hospital outpatient department or an ambulatory surgery center. The physician collects the facility-rate professional fee. The facility bills its own separate payment.
| Site of service | 2026 national payment | Billed by |
|---|---|---|
| Physician, facility | ~$124 | Billing provider |
| Physician, office | ~$419 | Billing provider |
| Hospital outpatient (OPPS, APC 5301) | ~$927 | Facility |
| Ambulatory surgery center (ASC) | ~$498 | Facility |
A practice billing 43239 in a hospital should expect the lower professional fee. The larger OPPS or ASC payment goes to the facility on a separate claim. Confusing the two leads to revenue forecasting errors.
How GPCI and Your MAC Change the Allowable
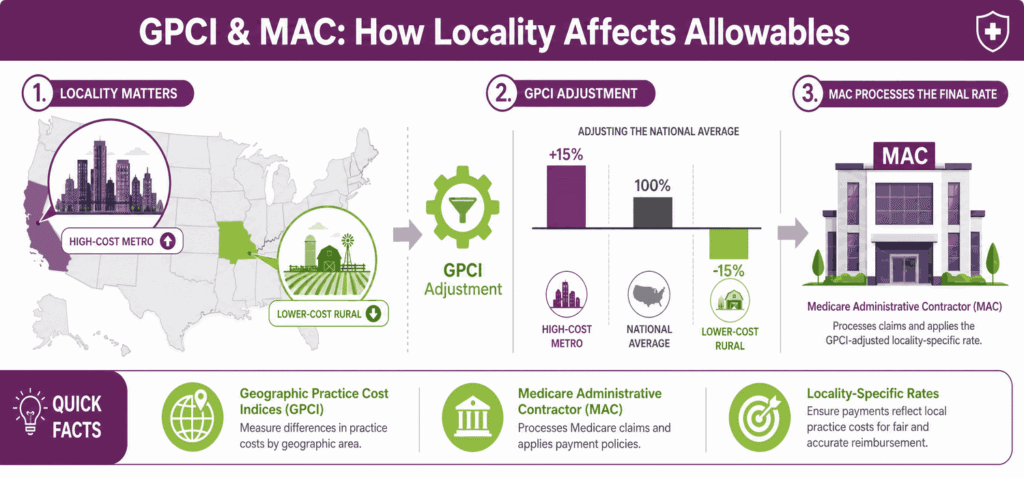
The national figures are starting points, not final allowances. CMS applies Geographic Practice Cost Indices (GPCI) to each RVU component by locality. Your Medicare Administrative Contractor (MAC) processes the adjusted rate.
- High-cost localities such as major metro areas push the allowance above the national average.
- Lower-cost regions can land below the national figure
- Each component carries its own GPCI, so the shift is not uniform
Always price 43239 against your specific MAC and locality. A San Francisco rate and a rural Nebraska rate can differ by a meaningful margin.
Professional vs. Facility Components (No Modifier 26 Split)
43239 does not carry a professional and technical component split. The code has no PC/TC indicator that would allow modifier 26 or modifier TC. Appending modifier 26 to 43239 is incorrect and gets rejected.
The professional and facility separation happens through different claims, not modifiers. The physician submits 43239 and receives the professional fee. The facility submits its own claim for the OPPS or ASC payment.
Commercial Payer Variance and Prior Authorization
Commercial payers rarely match Medicare exactly on 43239. Many anchor to a percentage of the fee schedule, often above 100 percent. Others negotiate flat case rates with facilities.
Prior authorization is the bigger variable for cash flow. Several plans require auth for elective upper endoscopy, especially surveillance exams. Aetna, BCBS, UnitedHealthcare, and Cigna each maintain their own medical policy criteria.
- Verify auth requirements before the procedure date, not after.
- Capture the medical necessity language that the plan policy requires.
- Track Medicare Advantage plans separately, since rules differ from traditional Medicare.
Common Clinical Scenarios for 43239
43239 supports a defined set of diagnostic indications. Each scenario carries an expected biopsy site and a supporting diagnosis. Matching the two is what survives payer review.
The scenarios below cover the bulk of upper endoscopy biopsy volume. Documentation should always state the clinical question the biopsy answers.
Refractory GERD and Suspected Esophagitis
When reflux symptoms persist despite therapy, the physician examines the distal esophagus. Biopsies confirm or rule out esophagitis and other mucosal changes. The note should record the failed medical management.
Refractory GERD is a strong medical necessity anchor when documented well. A simple symptom code without a treatment history invites a denial. Reflux esophagitis findings support codes such as K20.0 or K21.00.
Barrett’s Esophagus Surveillance and Dysplasia Biopsy
Barrett’s esophagus requires periodic surveillance biopsy on a defined schedule. The physician samples the columnar-lined segment using a systematic protocol. Pathology determines whether dysplasia is present.
- K22.70 supports surveillance of Barrett’s without dysplasia
- K22.710 and K22.711 apply when low-grade or high-grade dysplasia is found
- Surveillance frequency should match published guideline intervals
Frequency limits are a real denial risk for surveillance exams. A biopsy performed earlier than guidelines requires documented justification. Note the prior pathology and the interval rationale.
Gastric and Duodenal Ulcers / H. pylori Confirmation
Ulcers found on exam often warrant a biopsy to confirm the cause and rule out malignancy. Gastric ulcers in particular carry a biopsy expectation. Tissue can also confirm Helicobacter pylori infection.
| Finding | Common ICD-10 | Biopsy purpose |
|---|---|---|
| Gastric ulcer | K25.9 | Rule out malignancy, confirm healing |
| Duodenal ulcer | K26.9 | Confirm diagnosis, assess cause |
| Gastritis with H. pylori suspicion | K29.00 | Confirm infection by tissue test |
Document why the biopsy was clinically necessary, not routine. A gastric ulcer biopsy is well supported. A duodenal ulcer biopsy needs a clearly stated reason.
Suspected Celiac Disease (Duodenal Biopsy)
Suspected celiac disease drives duodenal biopsy during upper endoscopy. The physician samples the second portion of the duodenum, often with multiple specimens. Serology results usually precede the procedure.
The note should reference the positive serology or strong clinical suspicion. Celiac disease maps to K90.0 once confirmed. Until then, document the symptoms and serologic findings that justify the exam.
Upper GI Crohn’s Involvement
Crohn’s disease can involve the upper digestive tract, not only the colon. Biopsy confirms inflammation and helps stage disease extent. This indication is less common but well recognized.
Upper GI Crohn’s maps to the K50 family based on site and complications. Document the established Crohn’s history and the reason for upper tract sampling. Tie the biopsy site to the suspected involvement.
ICD-10 Linkage Map by Scenario
The diagnosis code carries the medical necessity for 43239. Local Coverage Determinations list the supported diagnoses for upper endoscopy. The map below pairs each scenario with a common supporting code.
| Scenario | ICD-10 | Biopsy site rationale |
|---|---|---|
| Refractory GERD, suspected esophagitis | K21.9, K20.0 | Distal esophagus, confirm mucosal injury |
| Barrett’s surveillance | K22.70 | Columnar segment, detect dysplasia |
| Barrett’s with dysplasia found | K22.710, K22.711 | Targeted segment, grade dysplasia |
| Gastric ulcer | K25.9 | Ulcer margin, rule out malignancy |
| Gastritis, H. pylori suspicion | K29.00 | Antrum and body, confirm infection |
| Suspected celiac disease | K90.0 | Second duodenum, confirm villous change |
| Upper GI Crohn’s | K50.- | Involved site, confirm inflammation |
Always confirm the active LCD for your MAC before relying on a code. Coverage lists change, and a supported code in one region may differ in another.
Billing Rules and Modifiers for 43239
Clean 43239 claims depend on documentation, edits, and correct modifiers. The code is simple to report but easy to deny. Most denials trace back to one of three control points.
This section covers what the note must contain, which edits apply, and which modifiers are valid. It also explains why two common modifiers do not belong on 43239.
Documentation Requirements
The operative note and pathology order together prove the service. Payers want evidence that the biopsy was intentional and indicated. Vague notes lose appeal.
- Intent: The note states the biopsy was planned or clinically driven.
- Site: each biopsy location is named specifically.
- Indication: the clinical reason ties to the diagnosis code.
- Pathology order: the requisition matches the biopsy sites.
- Operative report: signed, dated, and consistent with the claim.
A pathology report alone does not carry the claim. The operative note must show the physician’s decision and the sites sampled. The two documents should agree.
NCCI Edits, MUE, and Bundling Risk with Other EGD Codes
The National Correct Coding Initiative (NCCI) bundles 43239 into more extensive EGD codes. When a polypectomy or bleeding control happens at the same site, 43239 bundles in. Reporting both without justification triggers an edit.
- MUE: 43239 is built for a single unit per session
- Column 1 / Column 2 edits: therapeutic EGD codes often include the biopsy
- Same-site rule: biopsy of the treated lesion is not separately billable
A separate biopsy at a distinct site can sometimes bypass the edit. That requires the right modifier and clear site documentation. Without both, the edit holds.
Modifiers That Apply to 43239
A small set of modifiers is valid on 43239. Each one answers a specific billing situation. Using the wrong modifier is itself a denial trigger.
| Modifier | Meaning | When valid on 43239 |
|---|---|---|
| 22 | Increased procedural services | Substantially greater work, documented; rare for biopsy |
| 51 | Multiple procedures | Multiple endoscopies in the same session, per payer rules |
| 53 | Discontinued procedure | The exam stopped after scope insertion for patient reasons |
| 59 | Distinct procedural service | Separate procedure at a separate site or session |
| XE | Separate encounter | Service in a distinct encounter, subset of 59 |
| XP | Separate practitioner | Performed by a different practitioner, subset of 59 |
| XS | Separate structure | Separate organ or anatomic site, subset of 59 |
The X modifiers refine modifier 59 with more precision. XS is the most common on GI claims, marking a separate anatomic site. Payers increasingly prefer the X set over a blanket 59.
Why Modifier 25 Generally Does Not Apply
Modifier 25 marks a significant, separately identifiable evaluation on the day of a procedure. 43239 carries a 000-day global period, so the routine pre-procedure assessment is bundled. A standard same-day visit does not justify modifier 25.
Payers, led by Medicare and NCCI, target improper modifier 25 use on minor procedures. The E/M must address a separate problem beyond the decision to scope. Without that, the visit is part of the procedure package.
Medical Necessity, LCD/NCD Compliance, and Frequency Limits
Medical necessity is the foundation of every paid 43239 claim. The diagnosis must appear on the applicable Local Coverage Determination. Surveillance exams also face frequency limits.
- LCD and NCD: confirm the diagnosis is covered for your MAC
- Frequency: surveillance intervals must match the guideline timing
- Documentation: the note must justify any early or repeat exam
A medically supported indication with a covered diagnosis clears most reviews. Frequency edits catch surveillance done ahead of schedule. Document the interval rationale every time.
Why 43239 Claims Get Denied (and How to Fix Them)
43239 denials are predictable, which means they are preventable. Most fall into a handful of root causes. Fixing the upstream control point stops the pattern.
This section names the top denial reasons, gives a resolution checklist, and sets out pre-submission controls. These are the differences between a 95 percent clean rate and a backlog of appeals.
Top Denial Reasons
Four causes account for the majority of 43239 denials. Each one maps to a documentation or coding gap. Knowing them lets billers catch issues before submission.
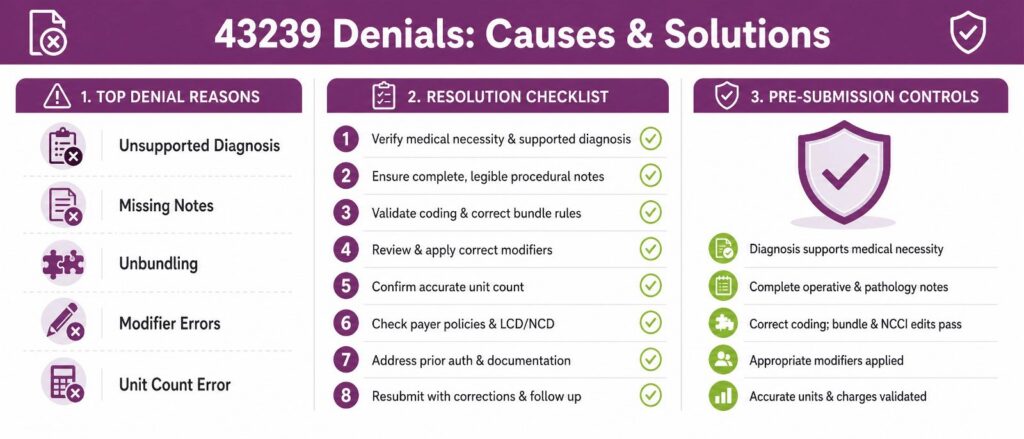
- Unsupported diagnosis: the linked ICD-10 is not on the LCD
- Missing operative or pathology note: the record does not prove intent or site
- Unbundling: 43239 reported with a code that already includes biopsy
- Modifier inconsistency: a 59 or X modifier without supporting documentation
A unit-count error is the fifth common cause. Billing more than one unit of 43239 hits the MUE wall. The single-unit rule is not optional.
Denial-to-Resolution Checklist
When a 43239 denial lands, work it in order. A structured pass resolves most claims without a formal appeal. Follow the steps below.
- Read the remark code and identify the exact denial reason
- Pull the operative note and confirm biopsy intent and sites
- Match the pathology order to the documented sites
- Verify the diagnosis sits on the current LCD for your MAC
- Check units: confirm only one unit of 43239 was billed
- Review any modifier for documentation support
- Correct and resubmit with the supporting record attached
- Escalate to appeal only if the corrected claim is denied again
Most denials are clear at step seven with the right attachment. Reserve formal appeals for genuine payer error. Track the root cause so the pattern does not repeat.
Pre-Submission Audit Controls
The cheapest denial is the one you prevent. A short pre-bill audit on 43239 claims catches the common errors. Build these checks into the charge-entry workflow.
- Diagnosis check: the ICD-10 is on the LCD before submission
- Unit check: exactly one unit of 43239 per session
- Bundling check: no conflicting EGD code on the same site
- Documentation check: operative note and pathology order present
- Modifier check: every modifier has a documented reason
Practices that run these controls see fewer reworks and faster payment. The same checks reduce audit exposure on a high-scrutiny code. Outsourced gastroenterology revenue cycle services can run them at scale across high volumes.
How Do You Bill CPT 43239 Correctly?
Billing 43239 correctly comes down to one principle. Report one unit, link a supported diagnosis, and document every biopsy site. The questions below cover the points coders ask most.
When should I use 43239 instead of 43235?
Use 43239 when the physician removes tissue by forceps for pathology. Use 43235 when the exam is visual only, with no forceps biopsy. The presence of a forceps biopsy is the deciding factor.
A washing or brushing alone still falls under 43235. The moment forceps take a tissue sample, the code becomes 43239. Read the operative note for the actual technique used.
Can I bill 43239 more than once per session?
No, you report only one unit per session. The descriptor “single or multiple” bundles every biopsy into that single unit. Billing two or more units triggers an MUE denial.
The number of biopsies does not change the unit count. Capture the extra work through site documentation in the note. The pathology order should list each site separately.
Does 43239 cover polyp removal?
No, 43239 covers biopsy only, not removal. Polyp removal uses 43250 for hot biopsy forceps or 43251 for snare. Reporting 43239 for a removal is a coding error.
Biopsy samples tissue, while polypectomy removes a lesion. If the physician removes a polyp, code the removal. A separate biopsy at a different site may still apply with the right modifier.
What ICD-10 codes support medical necessity?
Common supporting codes include K21.9, K22.70, K29.00, K25.9, and K90.0. The right code depends on the documented finding and indication. The diagnosis must appear on the LCD for your MAC.
- K21.9: GERD without esophagitis
- K22.70: Barrett’s esophagus without dysplasia
- K29.00: acute gastritis without bleeding
- K90.0: celiac disease
Always confirm the active coverage list before billing. A code covered in one region may not be covered in another.
Can 43239 be billed with anesthesia (00731/00732)?
Yes, the anesthesia provider bills the anesthesia code separately. For a standard upper endoscopy with biopsy, the anesthesia code is 00731. Code 00732 applies to procedures involving ERCP.
The gastroenterologist bills 43239 for the procedure itself. The anesthesiologist or CRNA submits 00731 on a separate claim. The two services do not bundle because they are different providers.






