
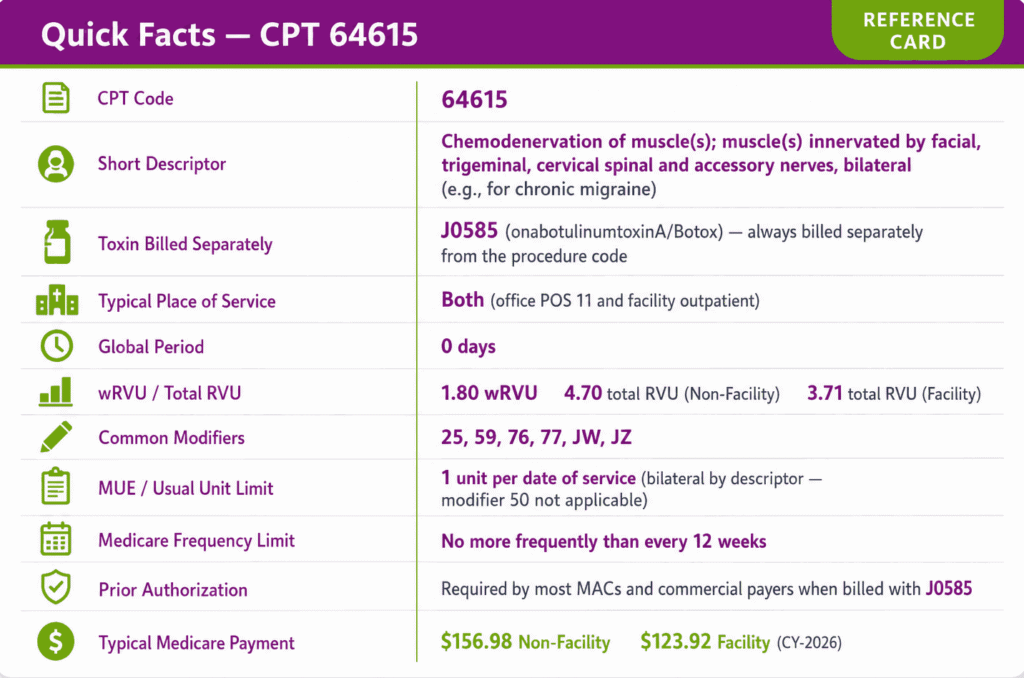
CPT code 64615 reports the bilateral chemodenervation of head and neck muscles for chronic migraine prevention, performed with onabotulinumtoxinA (Botox, HCPCS J0585) across the 31-site PREEMPT protocol. CPT code 64615 carries a 2025 work RVU of 1.85, requires the J0585 drug to be billed on a separate claim line, and reimburses once per session every 12 weeks under Medicare medical-necessity criteria.
This guide defines CPT code 64615, the covered muscle sites, the cost structure, three clinical scenarios, and the reimbursement rules that prevent denials.
What Is the Description of CPT Code 64615?
CPT code 64615 is defined by the AMA as “Chemodenervation of muscle(s); muscle(s) innervated by facial, trigeminal, cervical spinal and accessory nerves, bilateral (eg, for chronic migraine).”
The code reports the injection procedure only. It covers the placement of botulinum toxin type A into the targeted muscle groups during a single bilateral session for chronic migraine. The AMA added 64615 to the chemodenervation family in 2013, separating migraine chemodenervation from the limb, neck-dystonia, and facial chemodenervation codes and bundling the previously used 64612 and 64613 for this indication.
CPT 64615 represents one billable unit per treatment session, reported once regardless of the number of injection sites. The PREEMPT protocol commonly uses 31 injection sites across 7 muscle groups, but that figure is clinical-protocol guidance and not part of the official code definition.
Which Nerve Groups and Muscle Sites Are Covered Under CPT Code 64615?
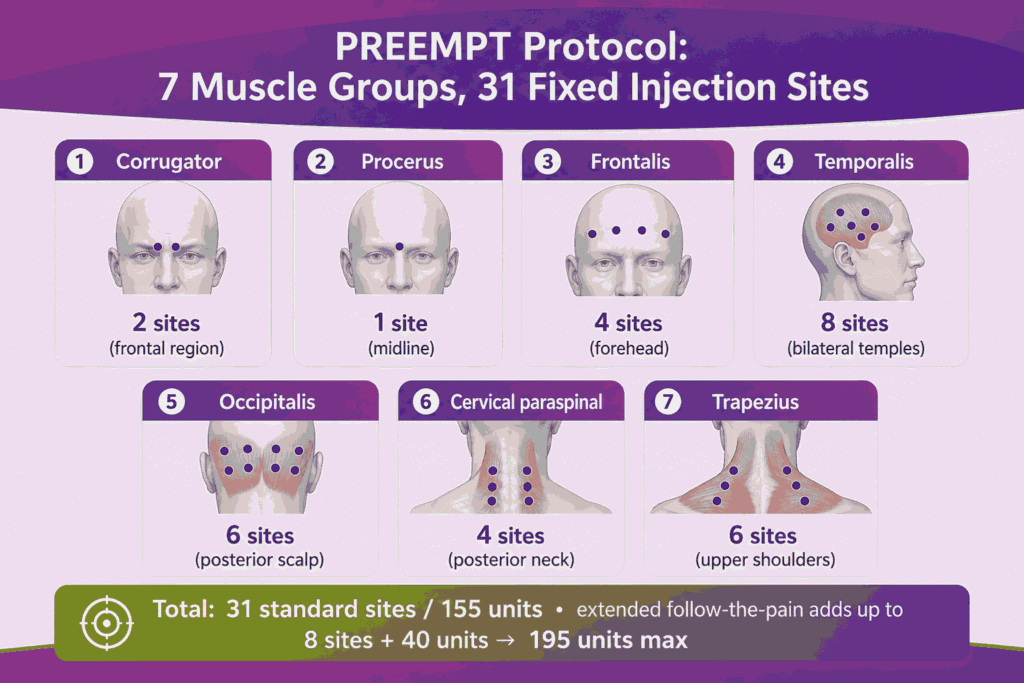
CPT code 64615 covers 4 nerve distributions and 7 muscle groups across the head and neck. The 4 nerve distributions are the facial nerve, the trigeminal nerve, the cervical spinal nerves, and the accessory nerve. The 7 muscle groups treated under the PREEMPT protocol are:
- Corrugator (2 sites, frontal region)
- Procerus (1 site, midline)
- Frontalis (4 sites, forehead)
- Temporalis (8 sites, bilateral temples)
- Occipitalis (6 sites, posterior scalp)
- Cervical paraspinal (4 sites, posterior neck)
- Trapezius (6 sites, upper shoulders)
These 7 muscle groups total 31 fixed injection sites in the standard PREEMPT paradigm.
What Is the PREEMPT Injection Protocol and Unit Range for CPT Code 64615?
The PREEMPT protocol is the FDA-approved chronic migraine paradigm of 155 units of onabotulinumtoxinA injected across 31 fixed sites every 12 weeks. PREEMPT stands for Phase III Research Evaluating Migraine Prophylaxis Therapy, the trial program that established the dosing standard. The standard dose is 155 units across 31 sites.
The extended “follow-the-pain” range adds up to 40 units across 8 optional sites, raising the maximum to 195 units across 39 sites for refractory cases. CPT code 64615 reports the procedure once per session, while J0585 reports the unit count (155 to 195 units) of onabotulinumtoxinA administered.
Why Is CPT Code 64615 Inherently Bilateral and Why Modifier 50 Does Not Apply?
CPT code 64615 is inherently bilateral because the code descriptor specifies bilateral injection, so modifier 50 does not apply. The PREEMPT protocol injects both the left and right corrugator, temporalis, occipitalis, cervical paraspinal, and trapezius muscles within a single procedure.
Appending modifier 50 to CPT code 64615 duplicates a service already defined as bilateral and triggers a denial for an inappropriate bilateral modifier. CPT code 64615 reports as 1 unit on 1 claim line with no laterality modifier (no 50, no LT, no RT) in standard physician-office and facility settings.
How Does CPT Code 64615 Differ From CPT 64612 and CPT 64616?
CPT code 64615 differs from CPT 64612 and CPT 64616 by anatomical target, laterality, and clinical indication. The following table compares the 3 chemodenervation codes most often confused in headache and movement-disorder billing:
| Code | Target | Laterality | Primary indication |
|---|---|---|---|
| 64615 | Facial, trigeminal, cervical spinal, accessory nerve muscles (head + neck) | Bilateral (built into code) | Chronic migraine |
| 64612 | Muscles innervated by the facial nerve | Unilateral (per side) | Blepharospasm, hemifacial spasm |
| 64616 | Neck muscles, excluding larynx | Unilateral (per side) | Cervical dystonia (spasmodic torticollis) |
CPT code 64615 is the only code in this set that is bilateral by definition and the only code indicated for chronic migraine. CPT 64612 and CPT 64616 each report per side and target narrower muscle groups. Reviewing a detailed CPT codes guide allows practice managers to differentiate these underlying chemodenervation boundaries clearly, preventing severe downcoding errors on mixed clinical claims.
Why Must J0585 Always Be Billed Separately From CPT Code 64615?
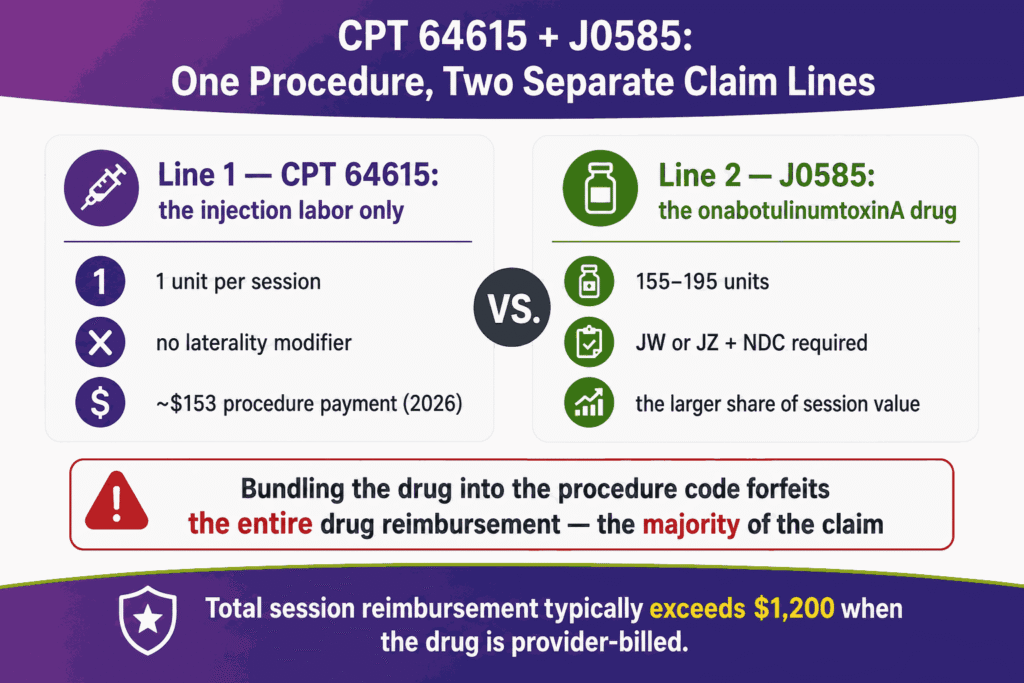
J0585 must be billed separately from CPT code 64615 because CPT code 64615 reimburses the injection labor only and excludes the drug acquisition cost. CPT code 64615 covers the physician’s work of placing the injections. J0585 covers the onabotulinumtoxinA itself, priced per unit.
Bundling the drug into the procedure code forfeits the entire drug reimbursement, which represents the majority of the total claim value per session. The claim reports CPT code 64615 on 1 line and J0585 with the administered unit count (typically 155) on a second line.
Why 64615 Requires onabotulinumtoxinA (J0585) and Not Dysport, Xeomin, or Myobloc
CPT code 64615 paired with J0585 requires onabotulinumtoxinA because onabotulinumtoxinA is the only botulinum toxin FDA-approved for chronic migraine. The 4 commercial botulinum toxins carry distinct HCPCS codes and distinct FDA indications:
- J0585 onabotulinumtoxinA (Botox): FDA-approved for chronic migraine
- J0586 abobotulinumtoxinA (Dysport): not FDA-approved for chronic migraine
- J0588 incobotulinumtoxinA (Xeomin): not FDA-approved for chronic migraine
- J0587 rimabotulinumtoxinB (Myobloc): not FDA-approved for chronic migraine
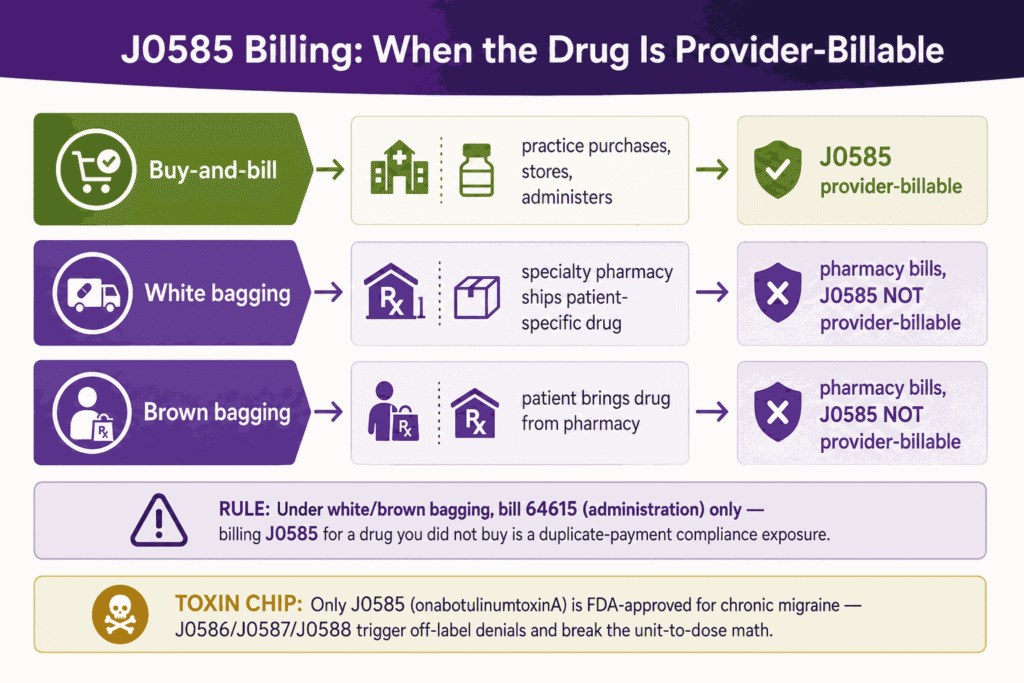
Billing CPT code 64615 with J0586, J0587, or J0588 produces an off-label denial because chronic migraine coverage extends only to onabotulinumtoxinA. The 4 toxins are not interchangeable in units, so substitution also breaks the unit-to-dose calculation.
Buy-and-Bill vs. White/Brown Bagging: When J0585 Is and Is Not Provider-Billable
J0585 is provider-billable under buy-and-bill and not provider-billable under white or brown bagging. The 3 acquisition models determine who bills the drug:
- Buy-and-bill: The practice purchases onabotulinumtoxinA, stores it, administers it, and bills J0585 to the payer. J0585 is provider-billable.
- White bagging: A specialty pharmacy ships patient-specific onabotulinumtoxinA to the practice. The specialty pharmacy bills the drug. J0585 is not provider-billable by the practice.
- Brown bagging: The patient receives onabotulinumtoxinA from a pharmacy and brings the drug to the appointment. The pharmacy bills the drug. J0585 is not provider-billable by the practice.
Under white and brown bagging, the practice bills CPT code 64615 (the administration) but omits J0585. Billing J0585 for a drug the practice did not purchase creates a duplicate-payment compliance exposure.
Can EMG Guidance or Ultrasound Guidance Be Billed Alongside CPT Code 64615?
EMG guidance and ultrasound guidance are not separately billable alongside CPT code 64615 for standard chronic migraine injections. The PREEMPT protocol uses fixed anatomical landmarks, not image or electrical guidance, so guidance codes lack medical necessity for the 31-site paradigm.
CPT 95874 (needle EMG for guidance) and CPT 76942 (ultrasound guidance for needle placement) are designed for deep or variable muscle targets, not the superficial fixed sites of chronic migraine chemodenervation. Reporting CPT 95874 or CPT 76942 with CPT code 64615 produces a medical-necessity denial absent documentation of an atypical clinical reason.
Which ICD-10 Codes Support Medical Necessity for CPT Code 64615?
CPT code 64615 requires a chronic migraine ICD-10 code in the G43.7 family to support medical necessity. The G43.7 subcategory describes chronic migraine without aura, and payers require the intractable variants for Botox coverage. The 4 supporting ICD-10 codes are:
- G43.711: Chronic migraine without aura, intractable, with status migrainosus
- G43.719: Chronic migraine without aura, intractable, without status migrainosus
- G43.701: Chronic migraine without aura, not intractable, with status migrainosus
- G43.709: Chronic migraine without aura, not intractable, without status migrainosus
Most payers require an intractable code (G43.711 or G43.719) plus a documented headache diary. Unspecified migraine (G43.909) and episodic migraine codes fail medical necessity for CPT code 64615 and trigger diagnosis-based denials. This cross-referencing loop represents one of the most heavily audited areas in therapeutic injection billing, as payers demand absolute alignment between diagnostic criteria and specialized neurology CPT codes before releasing payments.
What Are the Modifiers for CPT Code 64615?
CPT code 64615 uses 6 primary modifiers across the procedure line and the J0585 drug line. The 6 modifiers are 25, 59, 76, 77, JW, and JZ. Each modifier signals a distinct billing condition.
Modifier 25: Significant, Separately Identifiable E/M on Same Day as Procedure
Modifier 25 attaches to an E/M code, not to CPT code 64615, when a significant and separately identifiable evaluation occurs on the same day as the injection. Modifier 25 applies to the office-visit code (such as 99213 or 99214) when the physician addresses a problem distinct from the scheduled chemodenervation. A routine pre-injection check does not qualify for modifier 25. Many payers deny same-day E/M with CPT code 64615 absent clear, separate-service documentation.
Modifier 59: Distinct Procedural Service
Modifier 59 identifies a procedure that is distinct or independent from another service performed on the same day, used to override an NCCI procedure-to-procedure edit. Modifier 59 applies only when documentation supports a separate anatomical site, session, or lesion.
Modifier 59 does not apply between CPT code 64615 and CPT code 64612, which are not separately reportable for the same session. Payers increasingly require the more specific X{EPSU} modifiers in place of modifier 59.
Modifier 76: Repeat Procedure by Same Physician
Modifier 76 reports a repeat of CPT code 64615 by the same physician on the same day. Modifier 76 rarely applies to chronic migraine chemodenervation because the protocol is a single session per date of service. Modifier 76 documents intent when a clinical circumstance requires a same-day repeat by the original physician.
Modifier 77: Repeat Procedure by Another Physician
Modifier 77 reports a repeat of CPT code 64615 by a different physician on the same day. Modifier 77 distinguishes a second provider’s repeat service from a duplicate-claim error. Modifier 77, like modifier 76, applies infrequently to the once-per-session migraine protocol.
Modifier JW: Drug Amount Discarded/Not Administered to Patient
Modifier JW reports the units of J0585 discarded from a single-dose vial and not administered to the patient. Modifier JW attaches to a separate J0585 line listing the wasted units. A 200-unit vial used for a 155-unit dose yields 45 discarded units reported with modifier JW. Modifier JW captures payment for documented waste under the discarded-drug policy.
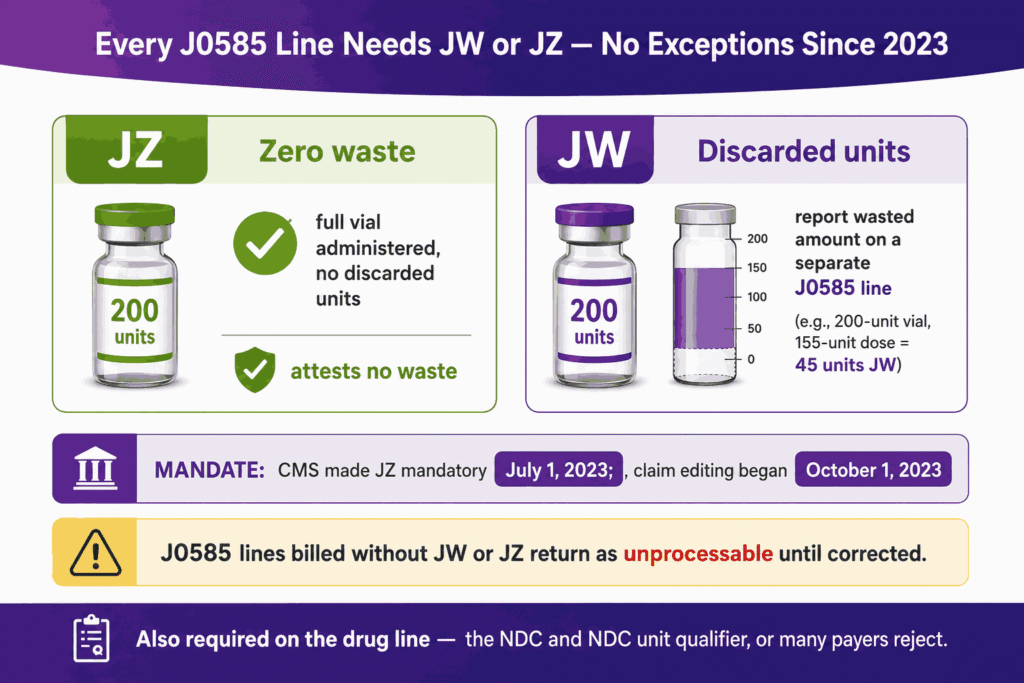
Modifier JZ: Zero Waste – Full Vial Administered With No Discarded Amount
Modifier JZ attests that zero units of J0585 were discarded, required on all single-dose drug claims since July 1, 2023. CMS made modifier JZ mandatory effective July 1, 2023, with claim editing beginning October 1, 2023. Modifier JZ applies when the administered dose consumes the full vial content with no waste. J0585 claims billed without the modifier JW or the modifier JZ on or after October 1, 2023, will return as unprocessable until corrected.
What Are the Medicare Prior Authorization and Medical Necessity Criteria for CPT Code 64615?
CPT code 64615 requires documented chronic migraine, a minimum headache-day threshold, and a failed oral preventive trial under Medicare and commercial medical-necessity criteria. Coverage attaches to chronic migraine confirmed by diagnosis code, a headache diary, and a record of inadequate response to oral preventives.
Prior authorization is standard across Medicare Advantage and commercial payers, with traditional Medicare applying the same medical-necessity documentation through LCD and NCD review.
Documented ≥15 Headache Days Per Month and Failed Trial of ≥2 Oral Preventive Classes
CPT code 64615 requires documentation of 15 or more headache days per month for at least 3 consecutive months and a failed trial of at least 2 oral preventive classes. The 15-day threshold defines chronic migraine and separates the condition from episodic migraine, which does not qualify.
The failed-preventive requirement spans drug classes such as beta-blockers, anticonvulsants (topiramate, valproate), and tricyclic antidepressants. Some payers require failure of 3 oral preventive classes rather than 2, so payer-specific policy verification precedes the first claim.
Which Documents Are Required For CPT Code 64615?
CPT code 64615 requires 6 documentation elements to support a clean claim. The 6 required documents are:
- Headache diary showing 15+ headache days per month across 3 months
- Oral preventive trial history listing the failed drug classes and outcomes
- Chronic migraine diagnosis recorded with the G43.7 ICD-10 code
- Procedure note listing all 31 injection sites and units per site
- Drug record stating total units administered and units discarded
- Prior authorization approval number from the payer
These 6 elements form the audit-defensible record that supports CPT code 64615 and the paired J0585 drug line.
What is the Cost of CPT Code 64615?
CPT code 64615 reimburses an estimated $150 to $160 nationally for the injection procedure under 2026 Medicare rates, separate from the J0585 drug, which represents the larger share of total session cost. CPT code 64615 cost is divided into 2 components: the procedure payment (CPT code 64615) and the drug payment (J0585).
The drug component for 155 units of onabotulinumtoxinA exceeds the procedure payment by a wide margin, so total session reimbursement typically ranges above $1,200 when the drug is provider-billed.
RVUs & Medicare Payment
CPT code 64615 carries a 2026 work RVU of 1.80, reduced from 1.85 under the CY2026 efficiency adjustment that cut work RVUs by 2.5% for non-time-based procedures. The following table presents the 2026 RVU components and Medicare conversion factors:
| Component | Value |
|---|---|
| Work RVU (2026) | 1.80 |
| Total RVU (non-facility, 2026) | ~4.6 |
| 2026 conversion factor (non-QP) | $33.4009 |
| 2026 conversion factor (QP) | $33.5675 |
| Estimated 2026 national payment (non-facility, procedure only) | ~$153–154 |
The 2026 Medicare Physician Fee Schedule applies a 2.5% efficiency adjustment that reduces work RVUs for non-time-based codes, including CPT code 64615, slightly lowering the procedure payment versus 2025. The procedure payment excludes the J0585 drug, which Medicare reimburses separately at ASP plus the applicable add-on percentage per unit.
Commercial Payers
Commercial payers reimburse CPT code 64615 at 120% to 200% of the Medicare rate, structured as a percentage of the Medicare Physician Fee Schedule. Commercial contracts are anchored to the Medicare RVU benchmark, so the conversion-factor change flows into commercial rates at the contracted multiplier.
Commercial drug reimbursement for J0585 follows AWP-based, ASP-based, or contracted-rate methodologies that vary by plan. Prior authorization remains mandatory across commercial payers for both CPT code 64615 and J0585.
Place-of-Service & Geographic Adjustments
CPT code 64615 payment varies by place of service and geographic practice cost index (GPCI). The non-facility setting (POS 11, physician office) pays a higher practice-expense RVU than the facility setting (POS 22 outpatient hospital, POS 24 ASC), because the office absorbs the supply and overhead cost.
The GPCI adjusts each of the 3 RVU components (work, practice expense, malpractice) by Medicare locality, so identical CPT code 64615 claims pay different amounts in different regions. High-cost localities pay above the national estimate, and rural localities pay below it.
What Are Example Clinical Scenarios or Use Cases for CPT Code 64615?
CPT code 64615 applies across 3 representative chronic migraine scenarios: an initial qualifying patient, a refractory repeat-cycle patient, and an extended-protocol patient with cervical involvement. The 3 scenarios illustrate how documentation, units, and reauthorization drive correct billing.
Scenario 1: Chronic Migraine With 15+ Headache Days Per Month Failing Oral Preventive Therapy
Scenario 1 bills CPT code 64615 plus J0585 x 155 units for a first Botox cycle after a documented failed oral preventive trial. A patient with 18 headache days per month for 4 months, after failing topiramate and propranolol, qualifies for chronic migraine chemodenervation.
The claim reports CPT code 64615 (1 unit), J0585 (155 units) with modifier JZ, and ICD-10 G43.719. The headache diary, the 2-class preventive failure, and the prior authorization complete the medical-necessity record.
Scenario 2: Refractory Chronic Migraine Requiring Repeat Botox Cycle After Documented Prior Response
Scenario 2 bills a repeat CPT code 64615 cycle at 12 weeks after documenting a 50% or greater reduction in headache days from the prior cycle. A patient who dropped from 20 to 9 headache days per month after cycle 1 demonstrates the response that supports reauthorization.
The claim reports CPT code 64615 (1 unit) and J0585 (155 units) with modifier JZ, dated at least 84 days after the prior session. The documented headache-day reduction satisfies the payer’s reauthorization criterion for the next cycle.
Scenario 3: Chronic Migraine With Concurrent Cervical Muscle Involvement Requiring Extended Injection Protocol
Scenario 3 bills CPT code 64615 plus J0585 at the extended 195-unit dose for a patient with cervical muscle involvement under the follow-the-pain paradigm. A patient with chronic migraine and pronounced cervical paraspinal and trapezius tenderness receives the standard 155 units plus 40 follow-the-pain units.
The claim reports CPT code 64615 (still 1 unit) and J0585 (195 units) with the procedure note documenting the additional sites and clinical rationale. CPT code 64615 remains a single procedure unit regardless of the 195-unit drug total.
What Are the CPT Code 64615 Rules To Ensure Successful Reimbursement?
CPT code 64615 reimburses successfully when the claim respects 5 rule sets: NCCI bundling edits, unit and frequency limits, the 64615/64612 mutual exclusion, prior authorization with drug-waste documentation, and denial-prevention practices. The 5 rule sets govern the procedure line, the J0585 drug line, and the supporting documentation.
Bundling / NCCI / Same-Day Procedure Rules
CPT code 64615 follows NCCI procedure-to-procedure edits that bundle other chemodenervation and guidance codes into the migraine procedure. NCCI edits prevent reporting CPT code 64615 with overlapping chemodenervation codes for the same session.
Same-day services such as EMG guidance (95874) and ultrasound guidance (76942) bundle into CPT code 64615 absent a distinct documented service. An NCCI modifier (59 or X{EPSU}) overrides an edit only when documentation supports a genuinely separate service.
Units, MUEs & 12-Week Medicare Frequency Restrictions
CPT code 64615 carries a Medically Unlikely Edit (MUE) of 1 unit per date of service and a Medicare frequency limit of one session every 12 weeks. CPT code 64615 reports as exactly 1 unit because the bilateral 31-site session is a single procedure.
J0585 reports the unit count (155 to 195) and carries its own higher MUE for the drug. The 12-week frequency restriction sets a minimum 84-day interval between cycles, and claims dated earlier than 84 days from the prior session deny for frequency.
Why CPT 64615 and CPT 64612 Are Mutually Exclusive and Must Never Be Billed Together
CPT code 64615 and CPT 64612 are mutually exclusive under NCCI procedure-to-procedure edits and report separately only with documented distinct services. CPT code 64615 already includes the facial-nerve muscle territory that CPT 64612 reports, so billing both for the same migraine session double-counts the facial muscles.
The NCCI edit pairs CPT code 64615 and CPT 64612 to block this overlap. Reporting CPT code 64615 with CPT 64612 for the same session, without a documented separate indication and the correct override modifier, produces a bundling denial.
Prior Authorization Requirements and Payer-Specific Drug Waste Documentation (JW and JZ)
CPT code 64615 requires prior authorization plus a JW or JZ modifier on every J0585 line to document drug-waste status. Prior authorization confirms chronic migraine, the headache-day threshold, and the failed preventive trial before the session. Every J0585 claim line carries modifier JZ (zero waste) or modifier JW (discarded units) since the July 1, 2023, mandate. Omitting both modifiers returns the J0585 line as unprocessable.
Documented ≥50% Headache-Day Reduction Required for 12-Week Reauthorization
CPT code 64615 reauthorization at 12 weeks requires a documented 50% or greater reduction in headache days from the pre-treatment baseline. The headache-day reduction proves clinical response and justifies the next cycle. A patient who fails to reach the 50% reduction faces a reauthorization denial under most payer policies. The headache diary across each cycle supplies the comparison data the payer reviews.
NDC Reporting Requirement for J0585 on Drug Claims
J0585 claims require the National Drug Code (NDC) of the administered onabotulinumtoxinA vial alongside the HCPCS units. The NDC identifies the specific vial product, lot, and packaging the payer reimburses. Many payers reject J0585 lines that report HCPCS units without the corresponding NDC and NDC unit qualifier. The NDC requirement applies across Medicare Advantage and commercial drug claims for J0585.
Top Reasons For Denials Specific To 64615 & Quick Remedies
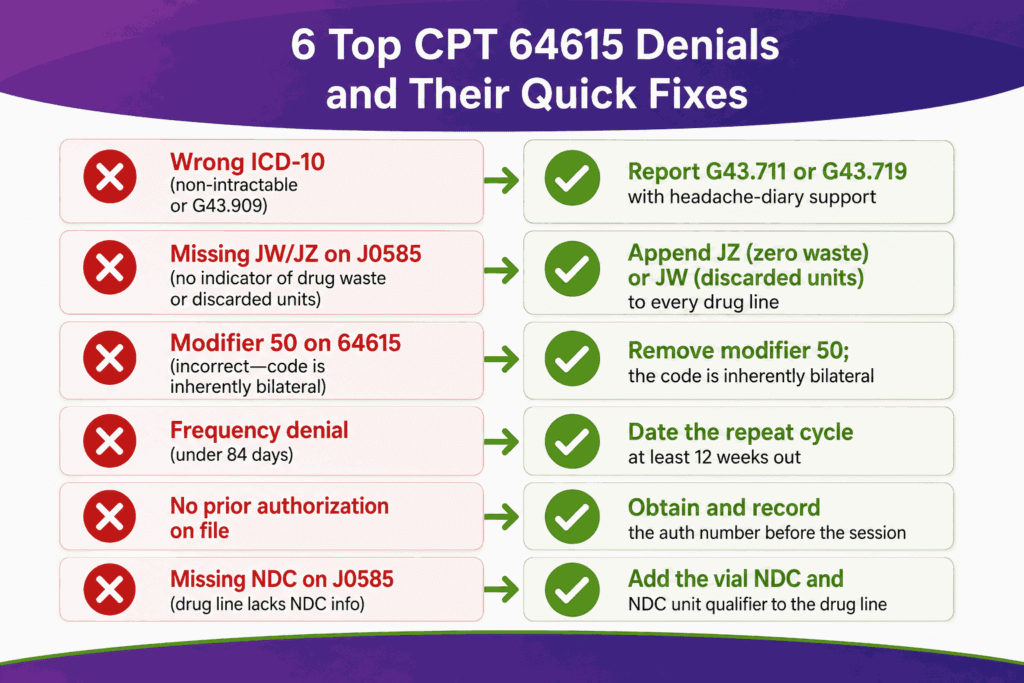
CPT code 64615 denials concentrate in 6 recurring root causes, each with a direct remedy. The following table maps the 6 top denial reasons to their quick remedies:
| Denial reason | Quick Fix |
|---|---|
| Missing or wrong ICD-10 (non-intractable or G43.909) | Report intractable code G43.711 or G43.719 with diary support |
| Missing JW or JZ modifier on J0585 | Append JZ (zero waste) or JW (discarded units) to every J0585 line |
| Modifier 50 appended to 64615 | Remove modifier 50 as the code is inherently bilateral |
| Frequency denial (under 84 days) | Date the repeat cycle at least 12 weeks after the prior session |
| No prior authorization on file | Obtain and record the authorization number before the session |
| Missing NDC on J0585 | Add the vial NDC and NDC unit qualifier to the drug line |
These 6 remedies resolve the majority of CPT code 64615 and J0585 denials at the front end, before claim submission. Specialized neurology billing services execute these pre-submission tracking loops automatically to keep high-dollar medication and administration claims moving without automated clearinghouse rejections.
CPT code 64615 reimburses cleanly when the claim pairs the bilateral migraine procedure with a separately billed J0585 drug line, an intractable G43.7 diagnosis, a JW or JZ waste modifier, prior authorization, and the 12-week frequency interval.
CPT code 64615 carries a 2025 work RVU of 1.85 and reimburses once per session, while the 155-unit onabotulinumtoxinA drug drives the larger share of total session value. Correct CPT code 64615 billing depends on the documentation, the modifier discipline, and the medical-necessity criteria detailed across this guide.
Elite neurology billing companies protect this entire specialized stream by running continuous documentation audits that ensure your provider notes remain fully defensible under external review.






