
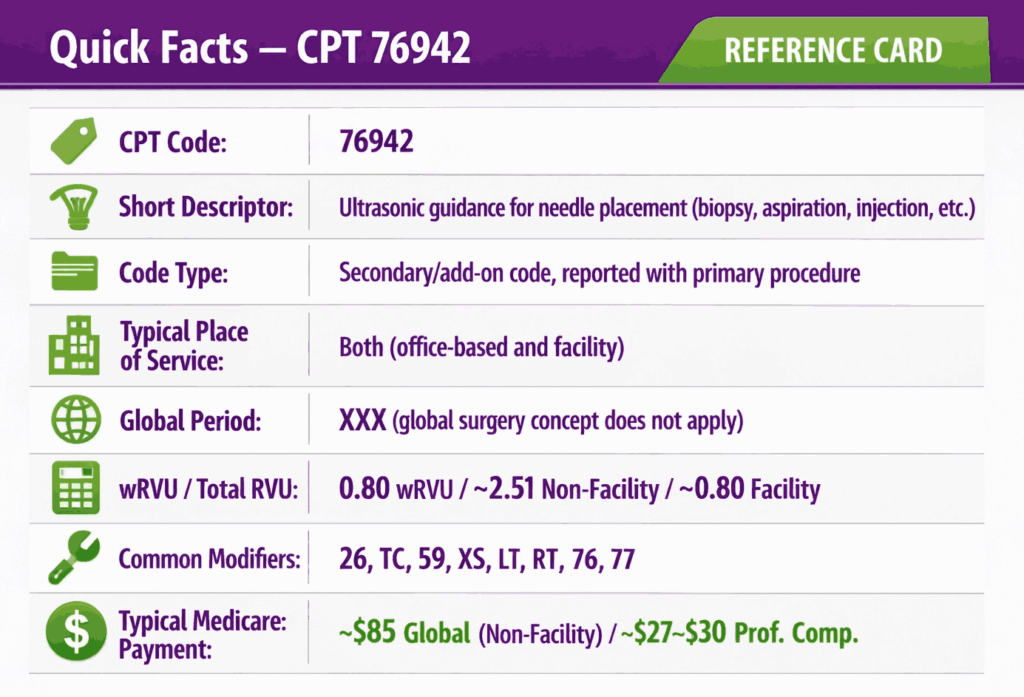
CPT code 76942 is a radiology add-on code used to report ultrasonic guidance for needle placement procedures. The procedure includes biopsies, aspirations, injections, and localization device placements, along with the associated imaging supervision and interpretation. Code 76942 is reported in addition to the primary procedural code and applies when real-time ultrasound is used to guide needle advancement and permanent image documentation is retained. This code is used across radiology, surgery, musculoskeletal medicine, endocrinology, and oncology in both facility and non-facility settings.
What Is the Description of CPT Code 76942?
76942 CPT code description is defined by the AMA as: “Ultrasonic guidance for needle placement (e.g., biopsy, aspiration, injection, localization device), imaging supervision and interpretation.”
This code captures the real-time ultrasound guidance service performed during a needle-based interventional procedure, separate from and in addition to the primary procedural code. It is not a standalone diagnostic ultrasound. 76942 CPT is a guidance service that accompanies a named procedure. CPT 76942 is always secondary to a primary procedure code, which must be present on the claim for the guidance to be billable.
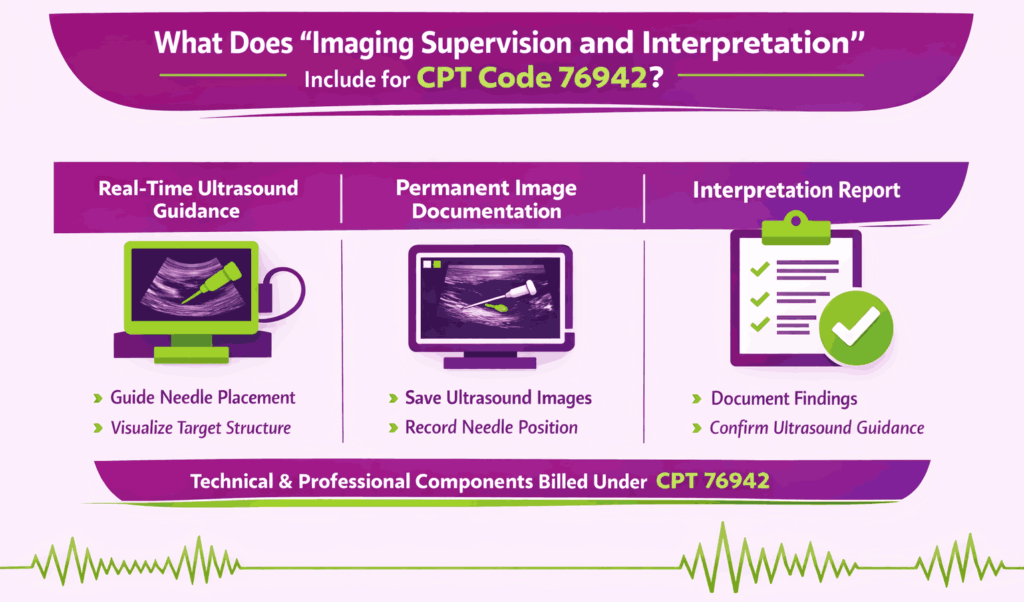
What Does “Imaging Supervision and Interpretation” Include for CPT Code 76942?
The imaging supervision and interpretation component of code CPT 76942 encompasses several distinct elements that must all be documented to support billing. The provider must perform real-time ultrasound imaging during the procedure to visualize the target structure and guide needle advancement. Permanent image documentation must be retained as part of the medical record, typically a saved static image or video clip that demonstrates the needle trajectory, target structure, and final needle position.
The provider must also generate a written or dictated interpretation documenting the anatomical site, use of ultrasound guidance during needle placement, the findings observed, and confirmation that guidance was used. Both the technical performance of the guidance and the professional interpretation are captured within this single code when billed globally.
How Does CPT Code 76942 Differ From CPT 76937 and CPT 76998?
CPT 76942, 76937, and 76998 all involve ultrasound guidance, but they serve distinct procedural contexts.
CPT 76937: Used for ultrasound guidance for vascular access, it is specific to vascular access procedures. These include central venous catheter placement, angioplasty, AV fistula procedures, and similar vascular interventions. It requires documentation of potential access site evaluation, vessel patency, and real-time needle visualization with permanent recording.
CPT 76942: This CPT code is the appropriate code for non-vascular needle placement guidance, biopsies, aspirations, injections, and localization device placements in non-vascular structures.
CPT 76998: An add-on code for ultrasound guidance, 76998 is used during certain specific surgical procedures as a supplemental service. Per NCCI Chapter 9, CPT 76998 should not be reported separately alongside 76942 when both involve ultrasound guidance for the same needle placement procedure.
When Is CPT Code 76942 Not Separately Billable Due to Bundling With the Primary Procedure?
Per CMS NCCI Policy Manual Chapter 9 and CPT guidelines, the 76942 code CPT is bundled into, and cannot be separately billed with, primary procedure codes that already include ultrasound guidance within their own descriptor. Notable examples confirmed from official sources include:
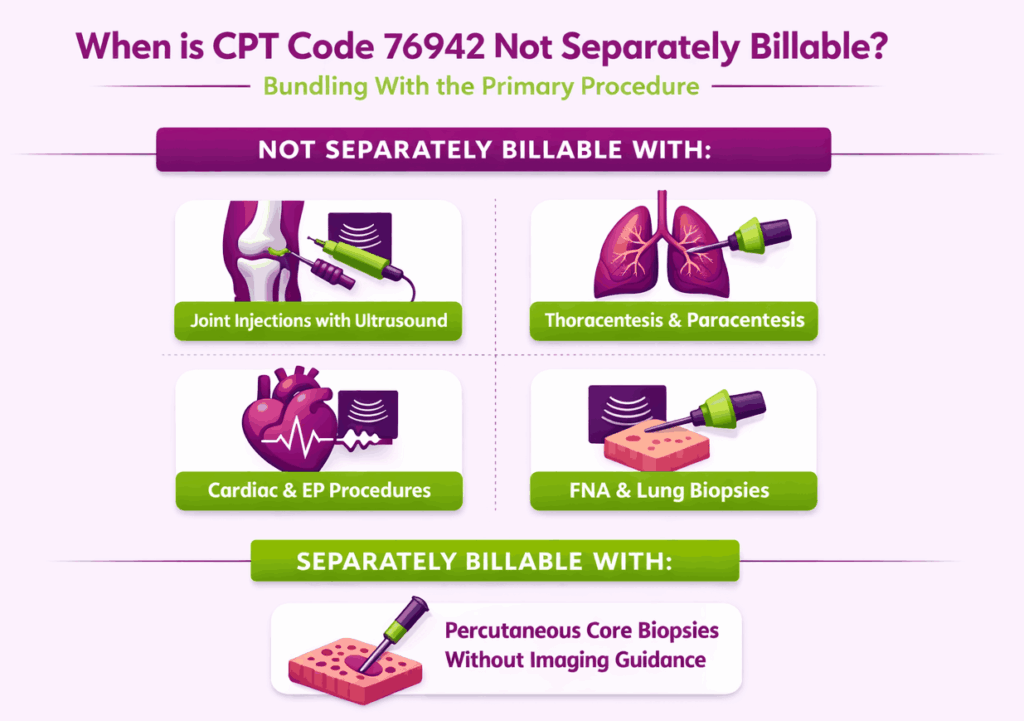
- Joint aspiration/injection codes with ultrasound guidance included: CPT codes 20604, 20606, and 20611 (arthrocentesis with ultrasound guidance) already include ultrasound guidance with permanent recording and reporting. CPT 76942 cannot be reported separately with these codes.
- Thoracentesis and paracentesis with imaging guidance included: CPT codes 32555 and 49083 include imaging guidance in their descriptors. CPT 76942 is not separately reportable with these codes.
- Lung/mediastinum biopsy (32408): This code includes imaging guidance. CPT 76942 cannot be separately reported.
- Fine needle aspiration with ultrasound guidance (10005, 10006): These codes already include ultrasound guidance. CPT 76942 cannot be reported with 10005 or 10006.
- Cardiac and electrophysiology procedures (33202–33275, 93600–93662): Per NCCI Chapter 5, CPT 76942 shall not be reported with pacemaker/ICD procedures or intracardiac EP procedure codes. The guidance is integral to those procedures.
By contrast, most anatomy-specific percutaneous needle core biopsy codes (19083, 20220, 47000, 49180) do not include imaging guidance, making 76942 separately reportable when used.
What Are the Modifiers for CPT Code 76942?
CPT code 76942 is a global code encompassing both technical and professional components, and can be split or further defined using the following modifiers.
Modifier 26: Professional Component Only
Modifier 26 is appended when the interpreting provider bills only for the professional interpretation and supervision, real-time image supervision during needle placement, and the written interpretation/report. This applies when a radiologist or other qualified provider supervises and interprets the guidance while a separate entity owns and operates the equipment.
Modifier TC: Technical Component Only
Modifier TC is appended when the facility or practice bills only for the technical component, the ultrasound equipment, supplies, and trained staff performing the real-time imaging. This is used when the professional interpretation is billed separately by another provider. Do not bill both TC and 26 from the same entity for the same encounter.
Modifier 59: Distinct Procedural Service
Modifier 59 is used when the CPT 76942 code is performed as a distinct service from a diagnostic ultrasound of the same anatomical region on the same date. It is applicable only when the two procedures were performed in different anatomic regions. Per NCCI Chapter 9 and the NCCI Policy Manual, a diagnostic ultrasound and 76942 of the same anatomic region on the same date are not separately reportable. Modifier 59 applies only when they address different anatomic regions.
Modifier XS: Separate Structure
Modifier XS is the more specific X-modifier subset indicating the service was performed on a separate anatomic structure. Where payers accept XS modifiers, it is preferred over modifier 59 to indicate that the diagnostic ultrasound and guidance service was performed on distinct anatomic sites on the same date. The clinical documentation must clearly identify each separate structure.
Modifier LT: Left Side Procedure
Modifier LT is used to identify that CPT 76942 was performed on the left side of the body, particularly relevant for bilateral structures such as breasts, kidneys, or extremity joints. Apply when payer policy or claim submission requires laterality identification.
Modifier RT: Right Side Procedure
Modifier RT is used to identify that CPT 76942 was performed on the right side of the body. As with modifier LT, apply when laterality is required by the payer for paired bilateral structures.
Modifier 76: Repeat Procedure by Same Physician
Modifier 76 is used when the same provider repeats CPT 76942 on the same patient on the same date due to a distinct clinical necessity, for example, guiding a second procedure at a different anatomic site on the same date. Documentation must establish a separate clinical indication for the repeat service.
Modifier 77: Repeat Procedure by Another Physician
Modifier 77 is used when a different provider performs a repeat ultrasound guidance service on the same date. Documentation must confirm the distinct clinical purpose and identify the separate provider.
Why Modifier 50 (Bilateral) Does Not Apply to CPT Code 76942
Modifier 50 (bilateral procedure) does not apply to code CPT 76942. Per CMS payment policy and the NCCI, the unit of service for CPT 76942 is the patient encounter, not the number of lesions, aspirations, biopsies, injections, or localizations performed during that encounter.
Only one unit of 76942 is reportable per encounter, even when multiple needle placements or bilateral structures are addressed in the same session. Bilateral modifier 50 is inappropriate because 76942 already captures all guidance performed at a single encounter in one unit.
Which Documents Are Required For CPT Code 76942?
Documentation for CPT code 76942 must support the medical necessity of ultrasound guidance, confirm real-time imaging was performed during needle placement, and include permanent image retention.
Required documents checklist:
- Primary procedure code and documentation confirming the needle-based procedure was performed
- Identification of the anatomical target and clinical indication, establishing why ultrasound guidance was necessary (e.g., deep location, proximity to vascular structures, small or non-palpable target)
- Documentation that real-time ultrasound imaging was used during needle advancement, not pre- or post-procedurally only
- Permanent saved image(s) or video clip retained in the medical record demonstrating needle trajectory and target structure
- Written or dictated interpretation documenting: anatomical site, the guidance was performed in real-time, findings observed, and confirmation of accurate needle placement
- Identification of who performed the imaging supervision and who provided the interpretation (when component billing applies)
- Provider signature with date and time of service
- Accurate place-of-service designation
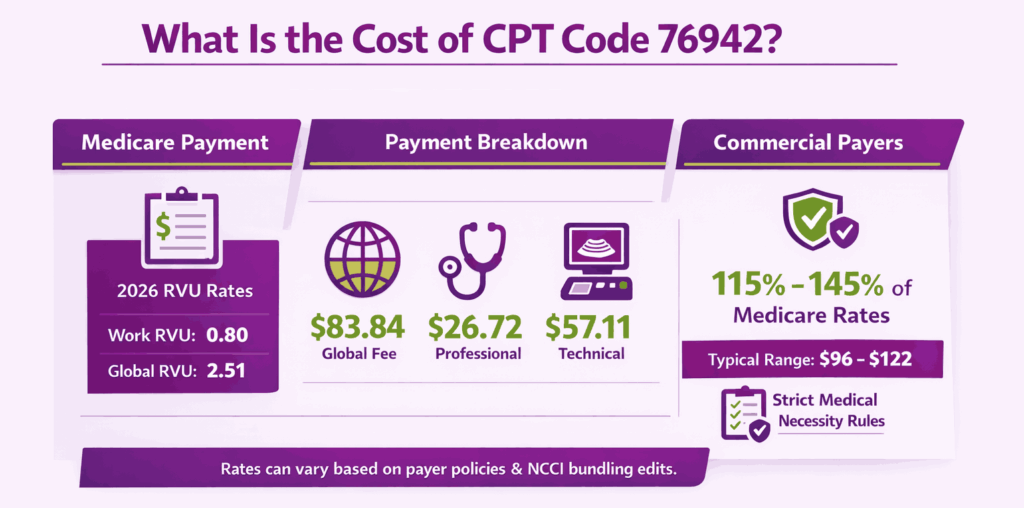
What Is the Cost of CPT Code 76942?
The cost of CPT code 76942 varies by component billed (global, professional, or technical), payer, geographic location, and place of service.
RVUs & Medicare Payment
For 2026, the Work RVU (wRVU) for 76942 has been finalized at 0.80. Despite this, the Total Global RVU for the office setting (Non-Facility) remains at 2.51, reflecting the technical costs of the ultrasound equipment and sonography support.
Applying the 2026 standard conversion factor of $33.4009, the national unadjusted CPT 76942 Medicare payment for the global service is $83.84. For practitioners billing only the Professional Component (-26), the payment is $26.72, while the Technical Component (-TC) for the equipment usage is valued at $57.11. These figures assume a standard non-APM participant; those in Advanced APMs would see a slightly higher conversion factor of $33.5675.
Commercial Payers
Commercial payers typically reimburse the procedure 76942 code at a rate of 115% to 145% of the Medicare Physician Fee Schedule, generally placing the global allowable between $96 and $122. Because this code is frequently bundled by NCCI edits, particularly with fluoroscopic guidance (77002), commercial insurers in 2026 are increasingly rigorous regarding “medical necessity” documentation.
Place-of-Service & Geographic Adjustments
The final payment is scaled by the Geographic Practice Cost Index (GPCI), ensuring that practices in higher-cost urban centers receive an adjustment to account for elevated rent and labor. Furthermore, the Place of Service (POS) determines the split of the fee: in a private oncology office (POS 11), the practice captures the full $83.84 global payment. In a hospital outpatient department (POS 22), the physician bills only the $26.72 professional interpretation, while the facility bills its own technical costs separately through the hospital payment system.
What Are Example Clinical Scenarios or Use Cases for CPT Code 76942?
76942 CPT code is used whenever real-time ultrasound guidance is employed to direct needle placement during a non-vascular interventional procedure, and the primary procedure code does not itself include imaging guidance.
Scenario 1: Ultrasound-Guided Fine Needle Aspiration of a Thyroid Nodule
ICD-10: E04.1 (Nontoxic single thyroid nodule)
A patient presents for evaluation of a 1.2 cm hypoechoic thyroid nodule identified on prior imaging, meeting biopsy criteria per clinical guidelines. The endocrinologist performs fine needle aspiration (FNA) under real-time ultrasound guidance, advancing the needle into the nodule under continuous visualization. A permanent image is saved, confirming needle position within the nodule. The procedure and guidance are documented separately. CPT 60100 (thyroid biopsy, needle) is reported as the primary code, and CPT 76942 is reported for the ultrasound guidance with imaging supervision and interpretation.
Scenario 2: Ultrasound-Guided Breast Mass Core Needle Biopsy
ICD-10: N63.10 (Unspecified lump in the right breast, unspecified quadrant)
A patient is referred for core needle biopsy of a 9 mm solid right breast mass identified on mammography. The radiologist performs image-guided core needle biopsy (CPT 19083) under real-time ultrasound visualization, targeting the mass with multiple passes. A saved image documents needle placement within the mass. The written interpretation confirms that real-time guidance was used and the target was successfully sampled. CPT 19083 is the primary code; CPT 76942 is not separately reported because CPT 19083 (breast biopsy with ultrasound guidance) already includes imaging guidance.
Note: This scenario illustrates a case where 76942 is NOT separately billable because the primary code 19083 already includes ultrasound guidance.
Scenario 3: Ultrasound-Guided Soft Tissue or Joint Injection for Musculoskeletal Conditions
ICD-10: M75.100 (Unspecified rotator cuff syndrome of unspecified shoulder)
A patient with shoulder pain and ultrasound-confirmed rotator cuff tendinopathy presents for a corticosteroid injection into the subacromial bursa. The provider performs the injection under real-time ultrasound guidance, visualizing the needle entry into the bursa and confirming injectate spread. A permanently saved image documents the needle and bursa position. CPT 20610 (arthrocentesis/injection, major joint) is the primary code. Because CPT 20611, the code that includes ultrasound guidance for major joint injection, was not used, CPT 76942 may be separately reported when documentation confirms real-time guidance was used and medical necessity is established.
What Are the CPT Code 76942 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for documentation, coding, bundling, and the one-unit-per-encounter policy. Meeting these CPT 76942 code rules reduces denials and ensures correct payment.
Bundling / NCCI / Same-Day Procedure Rules
The most critical bundling rule for CPT 76942 is sourced directly from the CMS NCCI Policy Manual Chapter 9. A diagnostic ultrasound CPT code and CPT code 76942 for the same anatomic region on the same date of service are not separately reportable. Only one may be reported, not both. This is an absolute NCCI rule, not a soft guideline.
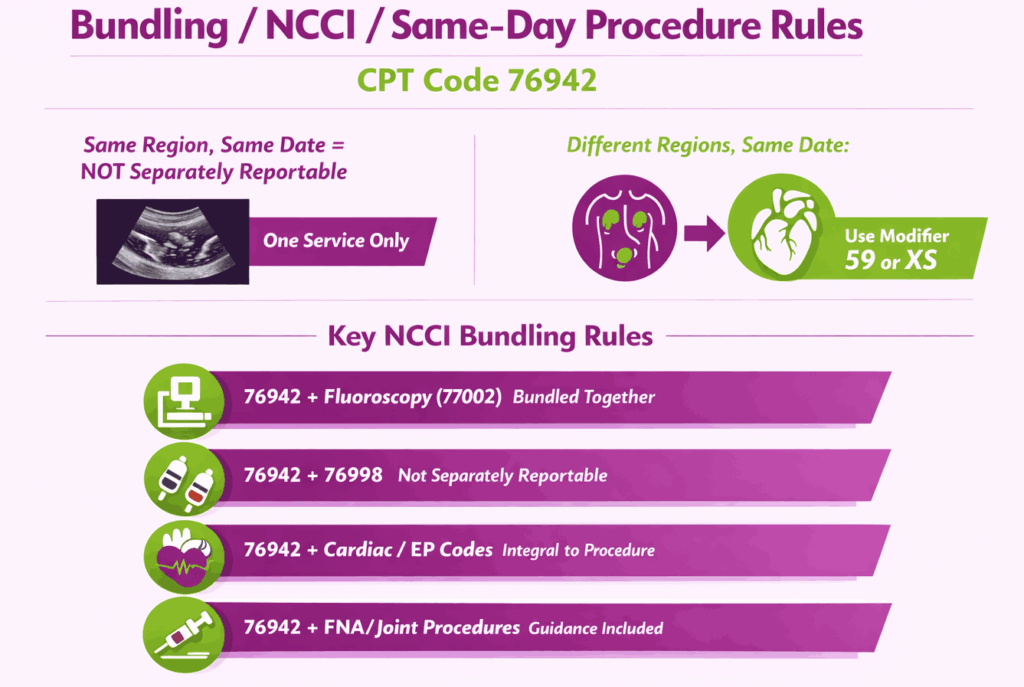
The exception is when each service is performed on a different anatomic region on the same date. In that case, both may be reported, and modifier 59 or XS is required to bypass the edit. Additional confirmed NCCI bundling rules include:
- CPT 76942 and fluoroscopic guidance (77002): bundled when both applied to the same region in the same session
- CPT 76942 with 76998: not separately reportable when both describe ultrasound guidance for the same needle placement
- CPT 76942 with cardiac/EP procedure codes (33202–33275, 93600–93662): guidance is integral, not separately reportable per NCCI Chapter 5
- CPT 76942 with 10005/10006 (FNA with ultrasound guidance): not separately reportable, the guidance is already included
- CPT 76942 with 32555/49083 (thoracentesis/paracentesis with imaging guidance): not separately reportable
- CPT 76942 with 20604/20606/20611 (joint procedures including ultrasound guidance): not separately reportable
Units, MUEs & One-Unit-Per-Encounter Policy
Per CMS NCCI Policy Manual and confirmed across multiple official sources, the unit of service for CPT 76942 is the patient encounter, not the number of lesions, aspirations, biopsies, injections, or localizations performed. Only 1 unit of 76942 is reportable per encounter, even when multiple needle placements are made at multiple target sites during the same session.
This is a firm CMS policy applicable to all of the CPT codes regarding radiologic guidance (76942, 77002, 77003, 77012, 77021). Billing multiple units of 76942 on the same date will be denied by the MAC.
Modifier 76 or 77 may support reporting a second unit when a repeat procedure at a different anatomic site on the same date involves distinct guidance, but this requires robust clinical documentation and payer pre-verification.
When CPT 76942 Cannot Be Billed With a Diagnostic Ultrasound of the Same Anatomical Region
Per NCCI Chapter 9, the following rule applies without exception. Evaluation of an anatomic region by diagnostic ultrasound and ultrasound guidance for needle placement in that same anatomic region on the same date of service are not separately reportable. Physicians should not split these into different dates to circumvent the edit. The NCCI Policy Manual explicitly prohibits this practice, stating that procedures historically performed on the same date should not be artificially separated across dates to avoid bundling edits.
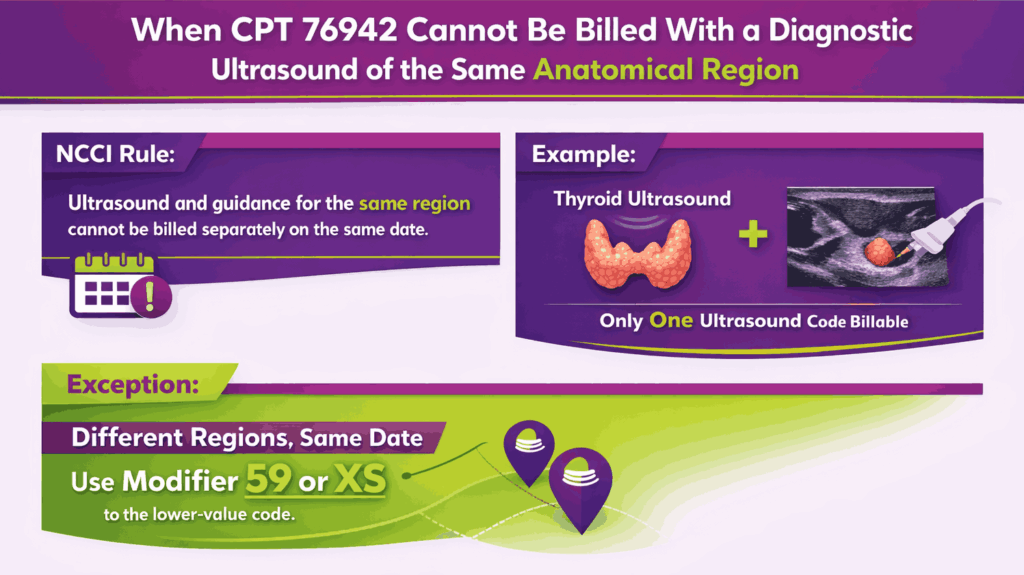
If a provider performs a diagnostic ultrasound of the thyroid and then performs FNA of a thyroid nodule under ultrasound guidance on the same date, only one ultrasound-related service is billable for the thyroid. Select whichever code is most appropriate based on what was documented, typically 76942 when a guidance procedure was performed, as it reflects the higher-complexity interventional service.
The exception applies only when the diagnostic ultrasound and 76942 address different anatomic regions on the same date. In that case, modifier 59 or XS must be appended to the lower-value code.
Top Reasons For Denials Specific To 76942 & Quick Remedies
- Billed Without a Primary Procedure Code: Prevent by confirming that a primary procedural code is always present on the claim. CPT 76942 is never a standalone code. It will be denied without a paired primary procedure.
- Billed With a Primary Code That Already Includes Guidance: Prevent by verifying the primary procedure code’s descriptor and bundling status. Codes such as 20604, 20606, 20611, 10005, 10006, 32555, 49083, and 32408 already include imaging guidance. 76942 is not separately billable.
- Multiple Units Billed Per Encounter: Prevent by billing only 1 unit of 76942 per patient encounter, regardless of the number of needle placements, lesions, or injections performed. CMS policy is explicit that the unit is the encounter, not the number of procedures.
- Missing Permanent Image Documentation or Written Interpretation: Prevent by confirming that a saved image and a written interpretation are retained in the record before submitting the claim. Absence of either documentation element is a top denial and audit trigger.
How are Specialized Guidance Services Identified?
Healthcare providers use standardized CPT codes in medical billing to communicate exactly when imaging was used to assist an interventional procedure. These codes, like 76942, ensure that the physician is reimbursed for the extra time, equipment, and expertise required to perform a safe and precise needle placement under real-time visualization.






