CPT code 95816 reports a routine electroencephalogram (EEG) that records brain electrical activity during awake and drowsy states. The American Medical Association (AMA) maintains CPT 95816 within the Routine Electroencephalography (EEG) Procedures family (95812, 95813, 95816, 95819, 95822, 95827).
This guide defines CPT 95816, its modifiers, 2026 cost and RVU values, clinical scenarios, and the documentation and reimbursement rules that govern clean claims.
What Is the Description of CPT Code 95816?
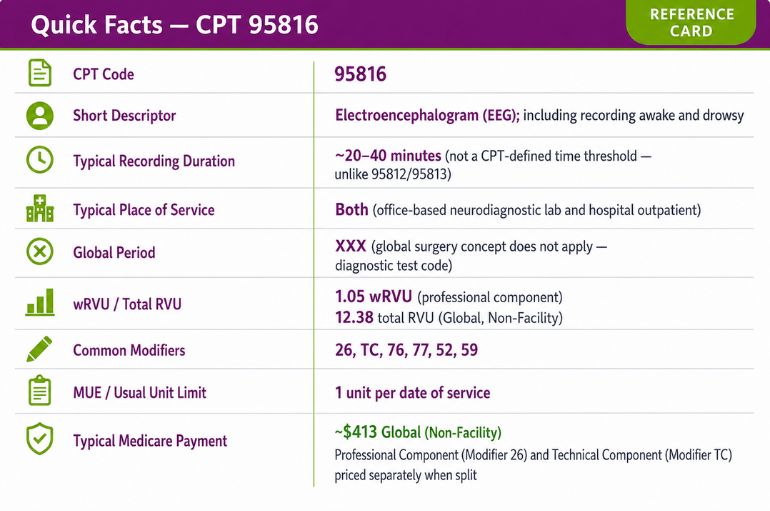
CPT code 95816 is defined by the AMA as “Electroencephalogram (EEG); including recording awake and drowsy.” CPT 95816 is a non-invasive neurodiagnostic test that uses scalp electrodes to record cortical electrical activity across two states: full wakefulness and spontaneous drowsiness.
CPT 95816 captures epileptiform discharges that surface during the wake-to-drowsy transition. Drowsiness lowers the seizure threshold and increases the diagnostic yield for abnormalities, particularly absence seizures and focal epileptiform discharges. A complete CPT 95816 study often incorporates activation procedures: hyperventilation and photic stimulation.
Two technical thresholds define a billable CPT 95816 study:
- Minimum 20 minutes of technically satisfactory recording
- Minimum 8 channels, per American Clinical Neurophysiology Society (ACNS) standards
What Does “Awake and Drowsy” Recording Require for CPT Code 95816?
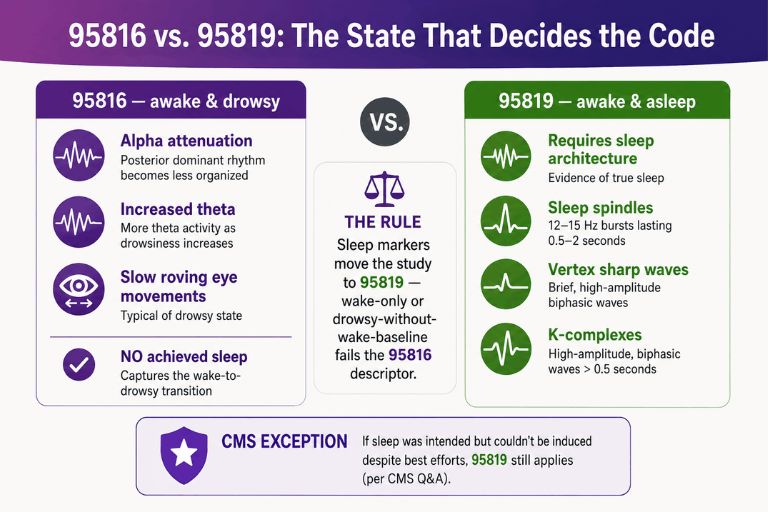
“Awake and drowsy” requires documented recording across the alert wake state and the spontaneous drowsy state, with no achieved sleep. Drowsiness presents as alpha rhythm attenuation, increased theta activity, and slow roving eye movements. CPT 95816 documents the transition into early drowsiness without progression to confirmed sleep.
CPT 95816 does not require sleep architecture. Sleep markers like sleep spindles, vertex sharp waves, and K-complexes define achieved sleep and trigger CPT 95819 instead. Recording that captures only wakefulness, or only drowsiness without a documented wake baseline, fails the descriptor. The technologist documents both states in the recording log to support the code.
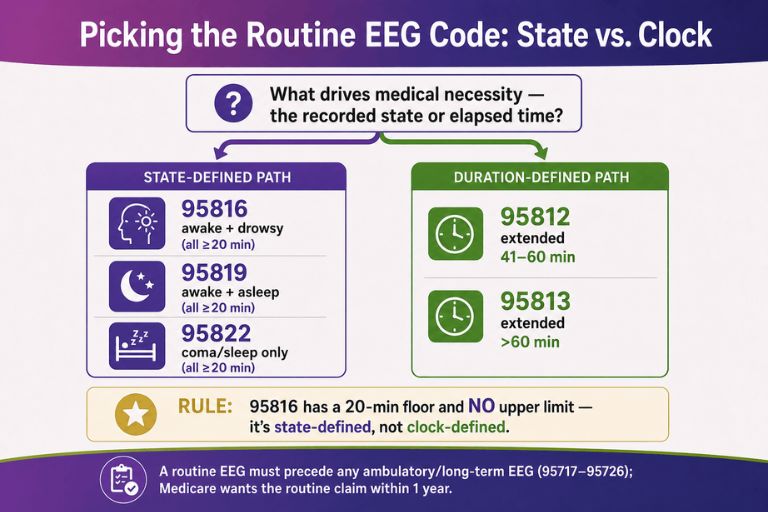
Why CPT Code 95816 Has No Defined Time Threshold Unlike CPT 95812 and 95813
CPT 95816 carries no upper time threshold because the code is state-defined, not duration-defined. CPT 95816 requires a 20-minute minimum and a documented awake-and-drowsy capture; the descriptor sets no maximum recording length.
CPT 95812 and CPT 95813 are the duration-defined members of the routine EEG family:
- CPT 95812: Electroencephalogram (EEG) extended monitoring; 41 to 60 minutes
- CPT 95813: Electroencephalogram (EEG) extended monitoring; greater than 1 hour
The following table contrasts the state-defined and duration-defined routine EEG codes:
| CPT Code | Definition Basis | Recording Parameter | Captured States |
|---|---|---|---|
| 95816 | State | ≥20 min, no upper limit | Awake + drowsy |
| 95812 | Duration | 41–60 min | Extended monitoring |
| 95813 | Duration | >60 min | Extended monitoring |
| 95819 | State | ≥20 min | Awake + asleep |
| 95822 | State | ≥20 min | Coma or sleep only |
CPT 95816 selection depends on the recorded states, whereas CPT 95812 and CPT 95813 selection depends on elapsed recording time. Coders assign 95812 or 95813 when extended duration drives the medical necessity, and 95816 when the awake-and-drowsy capture defines the study.
How Does CPT Code 95816 Differ From CPT 95819, 95822, and the Long-Term EEG Monitoring Codes (95717–95726)?
CPT 95816 differs from CPT 95819 and CPT 95822 by recorded state, and from CPT 95717–95726 by recording duration and code structure. CPT 95816 reports a single routine EEG of less than 24-hour continuous duration covering wake and drowsy states.
State-based distinctions within the routine EEG family:
- CPT 95816: Awake and drowsy. No achieved sleep.
- CPT 95819: Awake and asleep. Documented sleep architecture (spindles, vertex waves, K-complexes) is required.
- CPT 95822: Coma or sleep only. No awake baseline is captured.
The CMS guidance resolves the 95816-versus-95819 boundary directly. A coder assigns CPT 95819 when the patient achieves sleep, and CPT 95816 when sleep is not obtained. When a sleep study is intended but the technologist cannot induce sleep despite best efforts, CPT 95819 remains permissible per CMS Q&A guidance.
The long-term EEG monitoring codes (95717–95726) report continuous recordings of 24 hours or longer and use a split structure introduced in the 2020 code revision:
- Technical component codes: 95700, 95705–95716 (EEG technologist work, setup, and monitoring level)
- Professional component codes: 95717–95726 (physician interpretation, differentiated by recording days and video)
CPT 95816 reports a complete short-duration study under one code. The 95717–95726 code set reports physician work for prolonged monitoring under separate codes from the technical component. A routine EEG (95812, 95813, 95816, 95819, or 95822) must precede ambulatory or long-term EEG monitoring, and Medicare requires the routine EEG claim within 1 year of the long-term study date of service. For a complete breakdown of cross-cutting mapping rules, review our comprehensive Neurology CPT codes guide.
What ICD-10 Codes and Medical Necessity Criteria Support CPT Code 95816?
ICD-10 codes that support CPT 95816 establish a neurological indication consistent with seizure evaluation, altered awareness, or unexplained transient events. Medical necessity for CPT 95816 requires a documented symptom or condition that an awake-and-drowsy EEG evaluates.
Supporting ICD-10 diagnosis codes include:
- G40.909: Epilepsy, unspecified, not intractable, without status epilepticus
- G40.A09: Absence epileptic syndrome, not intractable, without status epilepticus
- R56.9: Unspecified convulsions
- R56.00: Simple febrile convulsions
- R55: Syncope and collapse
- R40.4: Transient alteration of awareness
- R41.82: Altered mental status, unspecified
- G93.40: Encephalopathy, unspecified
- R51.9: Headache, unspecified
Clinicians can cross-reference our standalone neurology ICD 10 codes guide to verify acceptable diagnostic indicators. Medical necessity for CPT 95816 rests on 4 documentation elements. Medical necessity for CPT 95816 rests on 4 documentation elements: the referring clinical indication, the ordering physician’s order, the recorded awake-and-drowsy states, and the interpreting physician’s written report.
Payers deny CPT 95816 when the linked ICD-10 code falls outside the covering Local Coverage Determination (LCD). Coders verify the diagnosis-to-procedure linkage against the applicable Medicare Administrative Contractor (MAC) LCD before submission.
What are the Modifiers for CPT Code 95816?
CPT 95816 accepts 6 primary modifiers that split the service, identify repeats, or flag reduced or distinct services. Each modifier communicates a specific billing condition to the payer.
Modifier 26: Professional Component Only
Modifier 26 reports the physician interpretation and written report only. A neurologist who reads a CPT 95816 recording produced by a separate facility appends 95816-26. Modifier 26 reimburses the physician work portion of the global service. The hospital or diagnostic center that owns the equipment bills the technical component separately.
Modifier TC: Technical Component Only
Modifier TC reports the equipment, supplies, and technologist work only. A hospital that performs the CPT 95816 recording while an external neurologist interprets it bills 95816-TC. Modifier TC reimburses the practice expense for the EEG machine, electrodes, and technologist time. Modifier TC and modifier 26 together equal the global service.
Modifier 76: Repeat Procedure by Same Physician (Serial EEG Monitoring)
Modifier 76 reports a repeat CPT 95816 by the same physician on the same date of service. A neurologist who performs a second medically necessary awake-and-drowsy EEG on one patient the same day appends 95816-76 to the second line. Modifier 76 documents serial EEG monitoring and overrides the per-day Medically Unlikely Edit (MUE) limit when supported.
Modifier 77: Repeat Procedure by Another Physician
Modifier 77 reports a repeat CPT 95816 by a different physician on the same date of service. A second neurologist who repeats the awake-and-drowsy EEG on the same patient the same day appends 95816-77. Modifier 77 distinguishes the repeat from a duplicate-claim denial.
Modifier 52: Reduced Services (Incomplete or Aborted Recording)
Modifier 52 reports a CPT 95816 recording shortened below the 20-minute minimum due to patient intolerance or technical failure. A study aborted at 12 minutes because of patient agitation reports 95816-52. Modifier 52 signals reduced reimbursement and prevents a recoupment for billing a substandard recording at the full rate. The technologist documents the reason for the shortened recording.
Modifier 59: Distinct Procedural Service
Modifier 59 reports a CPT 95816 that is distinct and separate from another procedure performed the same day that would otherwise bundle. Modifier 59 applies only when no more specific modifier (76, 77, or an anatomic modifier) describes the service. CMS guidance restricts modifier 59 to the narrowest case and reviews its use closely.
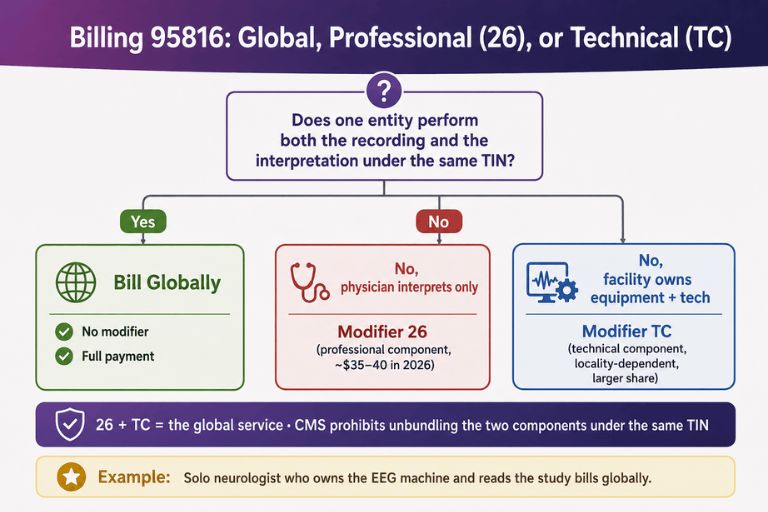
When Should CPT 95816 Be Billed Globally vs. With Modifier 26 or TC?
CPT 95816 is billed globally when one entity performs both the recording and the interpretation under the same Tax Identification Number (TIN). Global billing reports 95816 with no modifier and captures the full payment.
CPT 95816 is split when separate entities furnish the components:
- Modifier 26: The interpreting physician bills the professional component; a different entity owns the equipment.
- Modifier TC: The facility bills the technical component; an external physician interprets.
CMS prohibits unbundling these components under the same TIN. Our neurology billing guide details how to avoid this exact split-billing audit trap. A solo neurologist who owns the EEG equipment and reads the study bills CPT 95816 globally.
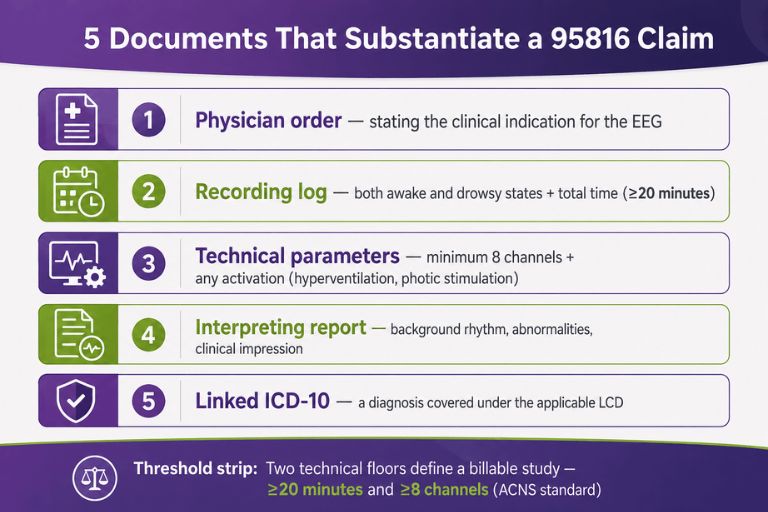
Which Documents Are Required For CPT Code 95816?
CPT 95816 requires 5 source documents that establish medical necessity and substantiate the recorded service. Complete documentation prevents the most frequent CPT 95816 denials.
Required documentation:
- Physician order stating the clinical indication for the EEG
- Recording log documenting both awake and drowsy states and total recording time (≥20 minutes)
- Technical parameters confirming minimum 8 channels and any activation procedures (hyperventilation, photic stimulation)
- Interpreting physician report describing background rhythm, abnormalities, and clinical impression
- Linked ICD-10 diagnosis supporting medical necessity under the applicable LCD
What is the Cost of CPT Code 95816?
The cost of CPT 95816 depends on which component is billed, the place of service, and geographic adjustment. The professional component reimburses the physician interpretation, the technical component reimburses the equipment and technologist work, and the global rate combines both.
RVUs & Medicare Payment
CPT 95816 carries a work RVU of 1.05 under the 2026 Medicare Physician Fee Schedule (RVU file RVU26A). Medicare converts RVUs to payment using the 2026 conversion factors: $33.4009 for non-qualifying APM clinicians and $33.5675 for qualifying APM participants (QPs).
The following table summarizes 2026 CPT 95816 reimbursement components at the non-QP conversion factor:
| Component | Modifier | What It Reimburses | Approximate 2026 Medicare Payment |
|---|---|---|---|
| Professional | 26 | Physician interpretation (work RVU 1.05) | ~$35–$40 |
| Technical | TC | Equipment + technologist (practice expense) | Higher; locality-dependent |
| Global | None | Both components combined | Substantially higher than 26 alone |
The professional component tracks the 1.05 work RVU and reimburses in the $35–$40 range in 2026. The global non-facility rate runs materially higher because the technical component carries a large practice-expense load for the EEG equipment and technologist time. CMS applies a −2.5% efficiency adjustment to work RVUs for non-time-based services in 2026, which reduces the interpretation reimbursement incrementally. Practices verify the exact locality figure in the 2026 MPFS Relative Value File before projecting revenue.
Commercial Payers
Commercial payers reimburse CPT 95816 at negotiated rates that exceed the Medicare allowable, typically expressed as a percentage of the MPFS or as a fee-schedule multiple. Commercial rates for CPT 95816 vary by contract, region, and place of service. Many commercial plans adopt the CMS RVU structure and the same professional/technical split logic, then apply a contracted conversion factor above the Medicare rate. Commercial MUE limits sometimes exceed CMS limits, though such exceptions concentrate in a narrow set of code categories.
Place-of-Service & Geographic Adjustments
Place-of-service and Geographic Practice Cost Index (GPCI) adjustments change the CPT 95816 payment by setting and locality. Medicare applies a facility rate and a non-facility rate to CPT 95816.
Two adjustments drive the variance:
- Place of service: The non-facility (office) global rate includes the technical component; the facility rate excludes the technical component because the facility bills it separately.
- GPCI: CMS multiplies the work, practice-expense, and malpractice RVUs by locality-specific indices, raising payment in high-cost regions and lowering it in low-cost regions.
The non-facility global payment for CPT 95816 exceeds the facility professional-only payment because the office setting bundles the equipment and technologist practice expense. A practice confirms the correct setting and locality before estimating the CPT 95816 allowable.
What Are Example Clinical Scenarios or Use Cases for CPT Code 95816?
CPT 95816 applies across 3 representative neurological scenarios where awake-and-drowsy recording drives the diagnostic decision. Each scenario links a clinical presentation to the awake-and-drowsy capture that CPT 95816 reports.
Scenario 1: New-Onset Staring Spells With Suspected Absence Seizures
A 47-year-old patient presents with brief staring spells and episodic confusion. The physician orders CPT 95816 to record baseline activity during wakefulness and to capture epileptiform discharges during drowsiness. The drowsy state raises the yield for the 3-Hz spike-and-wave discharges associated with absence seizures. The interpreting physician documents the background rhythm and any discharges in the written report. Supporting ICD-10 codes include R41.82 (altered mental status) and G40.A09 (absence epileptic syndrome).
Scenario 2: Pediatric Developmental Regression With Suspected Subclinical Seizure Activity
A 6-year-old who previously met developmental milestones loses bladder control and multi-word speech. The physician orders CPT 95816 to screen for subclinical or non-convulsive seizure activity across awake and drowsy states. The awake-and-drowsy capture identifies subtle epileptiform abnormalities that an awake-only recording obscures. The study informs whether the regression links to an epileptic syndrome. Supporting ICD-10 codes include R56.9 (unspecified convulsions) and G40.909 (epilepsy, unspecified).
Scenario 3: Recurrent Syncope With Differentiation Between Cardiac and Seizure Etiology
A 19-year-old presents with recurrent fainting spells accompanied by brief uncontrolled jerking movements. The physician orders CPT 95816 to record brain activity during wakefulness and drowsiness and to differentiate seizure activity from cardiac syncope. The awake-and-drowsy EEG identifies or excludes an epileptiform basis for the events. The result directs the workup toward cardiology or neurology. Supporting ICD-10 codes include R55 (syncope and collapse) and R56.9 (unspecified convulsions).
What Are the CPT Code 95816 Rules To Ensure Successful Reimbursement?
CPT 95816 reimbursement depends on 4 rule categories: bundling and NCCI edits, units and MUE limits, prior authorization and frequency limits, and denial prevention. Adherence to each category reduces the CPT 95816 denial rate.
Bundling / NCCI / Same-Day Procedure Rules
National Correct Coding Initiative (NCCI) edits prohibit billing CPT 95816 with another routine EEG state code for the same recording. CPT 95816, CPT 95819, and CPT 95822 describe mutually exclusive recorded states for a single study.
NCCI same-day rules for CPT 95816:
- Report one routine EEG code (95816, 95819, or 95822) per recording, not multiple state codes for the same session.
- Append modifier 59 only when a genuinely distinct EEG service occurs the same day and no more specific modifier applies.
- Confirm the routine EEG precedes any ambulatory or long-term EEG, with the routine EEG claim filed within 1 year of the long-term study for Medicare.
Units, MUEs & Same-Day Repeat EEG Billing Rules
The Medically Unlikely Edit (MUE) sets the maximum units of CPT 95816 reportable per patient per date of service by one provider. Routine EEG codes carry a low per-day MUE, consistent with one recording per session.
Same-day repeat billing for CPT 95816 follows a defined path:
- Report each medically necessary repeat on a separate claim line with modifier 76 (same physician) or modifier 77 (different physician).
- Attach documentation supporting the clinical necessity of units in excess of the MUE value.
- File a written appeal with medical records when a payer denies units above the MUE limit.
CMS adjudicates MUEs at the claim-line level for codes with a claim-line MUE Adjudication Indicator (MAI), which allows correctly modified separate lines to exceed the single-line limit. Confirm the current published MUE value on the quarterly CMS NCCI MUE table before billing repeats.
Prior Authorization and Payer-Specific Frequency Limitations
Prior authorization and frequency limits for CPT 95816 vary by payer and expand each year for neurodiagnostic services. Several commercial plans require prior authorization for EEG studies in select regions, and most apply frequency limits tied to medical necessity.
Frequency and authorization controls:
- Prior authorization: Required by select commercial plans and Medicare Advantage organizations before the study; obtained before the date of service.
- Frequency limits: Capped repeat EEG studies within a defined period absent a documented change in clinical status.
- LCD alignment: Coverage governed by the MAC’s EEG Local Coverage Determination, which defines covered diagnoses and limits.
A practice verifies authorization status and frequency allowance against the specific payer policy before scheduling CPT 95816.
Top Reasons For Denials Specific To 95816 & Quick Remedies
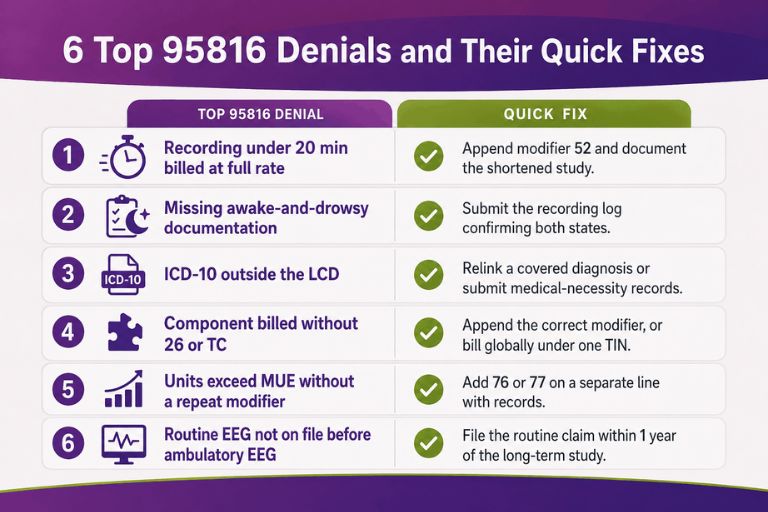
CPT 95816 denials concentrate in 6 recurring causes, each with a direct remedy. The following table maps each denial reason to its corrective action:
| Denial Reason | Quick Fix |
|---|---|
| Recording under 20 minutes billed at full rate | Append modifier 52 and document the reason for the shortened study |
| Missing awake-and-drowsy state documentation | Submit the recording log confirming both states |
| ICD-10 diagnosis outside the LCD | Relink a covered diagnosis or submit medical necessity documentation |
| Component billed without correct modifier (26 or TC) | Append the correct component modifier; bill globally under one TIN |
| Units exceed the MUE without a repeat modifier | Add modifier 76 or 77 on a separate line with supporting records |
| Routine EEG not on file before ambulatory EEG | File the routine EEG claim within 1 year of the long-term study |
Each remedy addresses the specific gap that triggered the denial. Utilizing dedicated neurology billing services provides pre-submission scrubbing to eliminate these local coverage errors completely. Practices that verify the 20-minute minimum reduce risk.
By applying CPT 95816 rules, including accurate state documentation, the 20-minute and 8-channel thresholds, correct modifier selection, MUE-compliant repeat billing, and LCD-aligned diagnosis linkage, billing teams secure clean reimbursement for the awake-and-drowsy routine EEG that CPT code 95816 reports.