Neurology ICD-10 codes classify nervous system diseases and symptoms across two ICD-10-CM chapters: G00–G99 (diseases of the nervous system) and R00–R99 (symptoms and signs). The distinction between these two chapters governs reimbursement. Symptom codes such as R51.9 (headache) and R42 (dizziness) document a presenting complaint, while diagnosis codes such as G43 (migraine) and G62.9 (polyneuropathy) document a confirmed condition.
In 2025, a RAF score of 1.0 equaled about $10,402 per member per year, and each 0.1 RAF increase added roughly $1,040 annually. Under V28, each dementia HCC carries a RAF of 0.341, translating to about $3,500 per member per year in risk-adjusted revenue. Because HCC capture resets annually, this value must be re-documented each year.
With dementia underdiagnosed in more than half of cases, missing capture in just 100 Medicare Advantage patients can mean roughly $350,000 in lost annual capitation revenue. CMS has also resumed RADV audits for 2018 through 2024, making MEAT-supported documentation essential to retain risk-adjusted payments and avoid recovery risk. This is precisely where specialized billing companies for neurology concentrate their effort, treating MEAT-supported documentation as the core defense against recovery exposure.
Payers treat the two categories differently, and code specificity drives first-pass claim acceptance. This guide reflects the FY2026 ICD-10-CM code set, effective October 1, 2025, including the restructured dementia codes (F01–F03) and the expanded Parkinson’s disease codes (G20.A1–G20.C).
How Neurology ICD-10 Codes Are Structured
Neurology ICD-10 codes occupy two chapters of the ICD-10-CM system: Chapter 6 (G00–G99, Diseases of the nervous system) and Chapter 18 (R00–R99, Symptoms, signs, and abnormal findings not elsewhere classified). Three additional chapters supply high-frequency neurology codes: Chapter 4 (E08–E13) for diabetic neuropathy, Chapter 9 (I60–I69) for stroke, and Chapter 5 (F01–F09) for dementia.
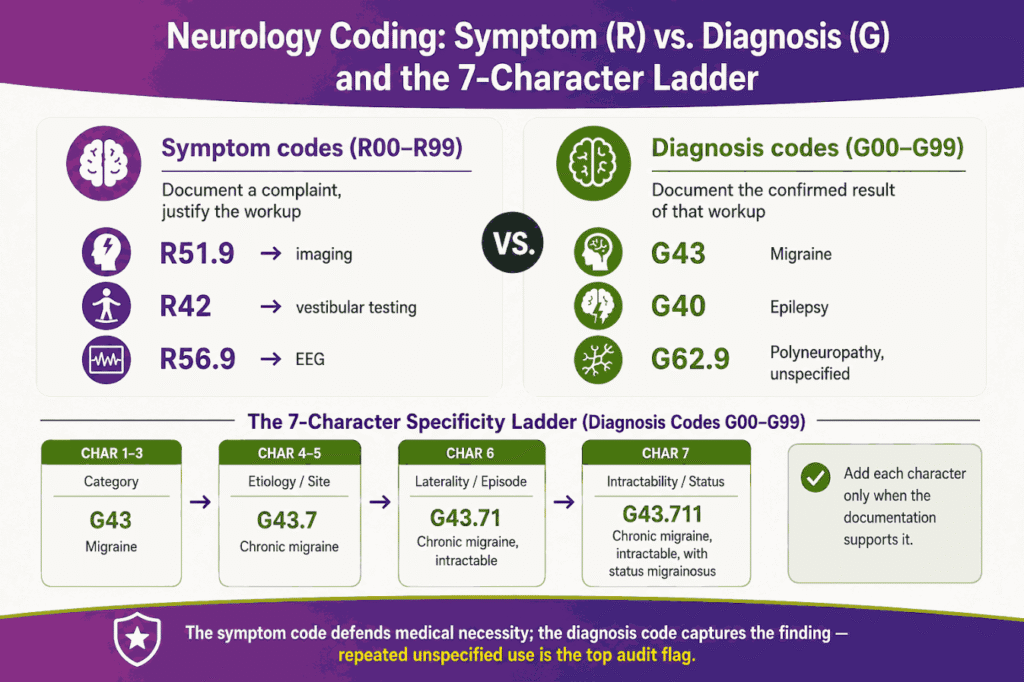
A neurology ICD-10 code carries up to 7 characters that encode increasing specificity:
- Category: the first 3 characters identify the condition family (G43 = migraine).
- Etiology and anatomic site: characters 4–5 add cause or location (G43.7 = chronic migraine without aura).
- Laterality and episode detail: character 6 adds side or episode type (G56.01 = carpal tunnel, right limb).
- Specificity extension: character 7 adds intractability, status, or encounter type (G43.711 = chronic migraine without aura, intractable, with status migrainosus).
The symptom-versus-diagnosis distinction determines medical necessity. A symptom code justifies the diagnostic workup. A diagnosis code documents the confirmed result of that workup. Coders assign the symptom code when documentation describes a complaint without a confirmed cause, and the diagnosis code when the provider records a definitive condition.
Unspecified codes carry the highest denial risk in neurology coding. An unspecified code ends in a placeholder digit such as .9 (G62.9 = polyneuropathy, unspecified) or .909 (G43.909 = migraine, unspecified, not intractable, without status migrainosus). Auditors flag repeated unspecified-code use as evidence of incomplete documentation review. The fix lies in documentation specificity, not code selection alone.
Headache ICD-10 Codes
The ICD-10 code for headache is R51.9 (Headache, unspecified), a billable symptom code that documents head pain without a confirmed cause. R51.9 functions as a symptom code, and payers frequently deny R51.9 as a primary diagnosis when documentation supports a more specific headache diagnosis. The companion code R51.0 (Headache with orthostatic component, not elsewhere classified) applies when head pain worsens on standing.
Headache coding escalates from symptom to diagnosis along a documented decision path. R51.9 applies at the initial presentation. Once the provider documents a headache type such as migraine, tension-type, cluster, or post-traumatic, coding moves to the corresponding G43 or G44 code. The symptom code defends the imaging or specialist referral that produces the definitive diagnosis.
The following table presents the most-reported ICD-10 codes for headache and their billing status:
| ICD-10 Code | Description | Type | Billing Note |
|---|---|---|---|
| R51.9 | Headache, unspecified | Symptom | Billable; denial risk as primary Dx |
| R51.0 | Headache with orthostatic component | Symptom | Billable; documents postural component |
| G44.209 | Tension-type headache, unspecified, not intractable | Diagnosis | Billable; most common chronic headache |
| G44.1 | Vascular headache, not elsewhere classified | Diagnosis | Billable |
| G44.009 | Cluster headache syndrome, unspecified, not intractable | Diagnosis | Billable |
| G44.301 | Post-traumatic headache, acute, not intractable | Diagnosis | Billable; links to injury code |
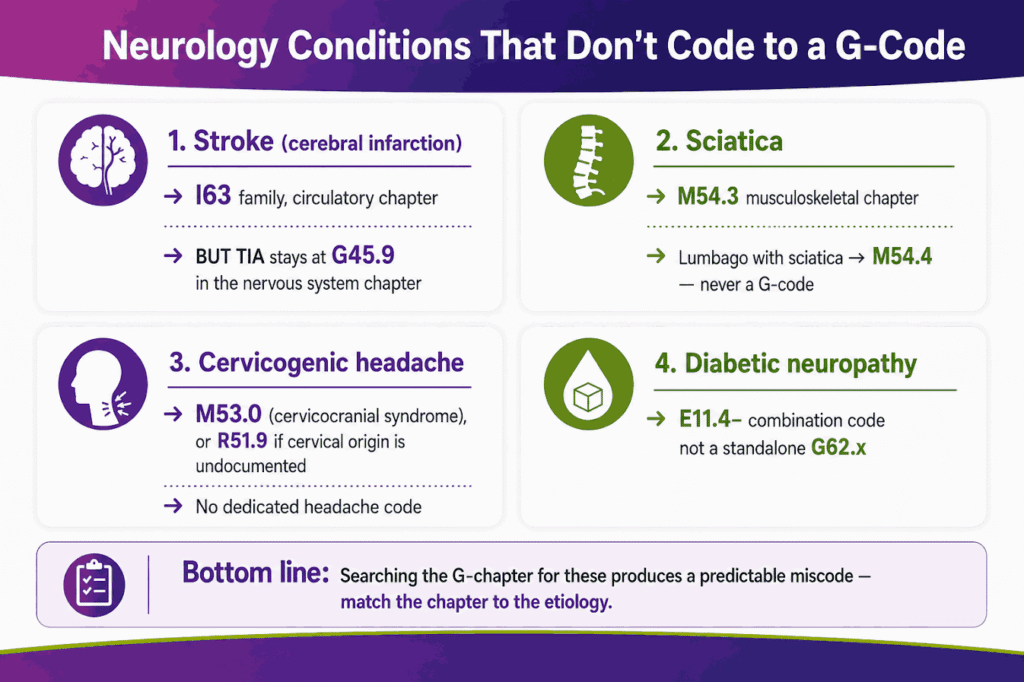
Cervicogenic headache lacks a dedicated ICD-10 code. Coders map cervicogenic headache to M53.0 (Cervicocranial syndrome) in the musculoskeletal chapter or to R51.9 when cervical origin is undocumented. This mapping gap produces frequent miscodes, since cervicogenic headache reads as a headache diagnosis but codes outside the headache families.
Documentation supports headache specificity through 4 recorded elements: headache type, chronicity (acute or chronic), intractability, and presence of status. Reviewing a comprehensive ICD 10 codes guide ensures that clinical staff structure these visit parameters correctly, since symptom coding with R51.9 also establishes medical necessity for a CT or MRI ordered to exclude secondary causes.
Migraine ICD-10 Codes
The ICD-10 code for migraine is G43.909 (Migraine, unspecified, not intractable, without status migrainosus), the default code when migraine type is undocumented. The G43 family subdivides along 2 axes: intractability (intractable versus not intractable) and status migrainosus (with status versus without status). Status migrainosus describes a migraine attack lasting longer than 72 hours.
The following table presents the most-reported migraine ICD-10 codes:
| ICD-10 Code | Description |
|---|---|
| G43.909 | Migraine, unspecified, not intractable, without status migrainosus |
| G43.009 | Migraine without aura, not intractable, without status migrainosus |
| G43.109 | Migraine with aura, not intractable, without status migrainosus |
| G43.709 | Chronic migraine without aura, not intractable, without status migrainosus |
| G43.E09 | Chronic migraine with aura, not intractable, without status migrainosus |
| G43.409 | Hemiplegic migraine, not intractable, without status migrainosus |
The G43.E family for chronic migraine with aura entered the code set in FY2024, effective October 1, 2023. Coding cheat sheets predating that date omit G43.E and misassign chronic migraine with aura to G43.709 (chronic migraine without aura), producing documentation mismatches.
Migraine coding errors usually fall into four categories: missing the required intractability or status specification, using unspecified migraine codes when the migraine type is documented, assigning the wrong aura category, and reporting status migrainosus without documentation supporting the duration requirement. In most cases, the root cause is incomplete documentation review rather than incorrect code lookup.
Dizziness and Vertigo ICD-10 Codes
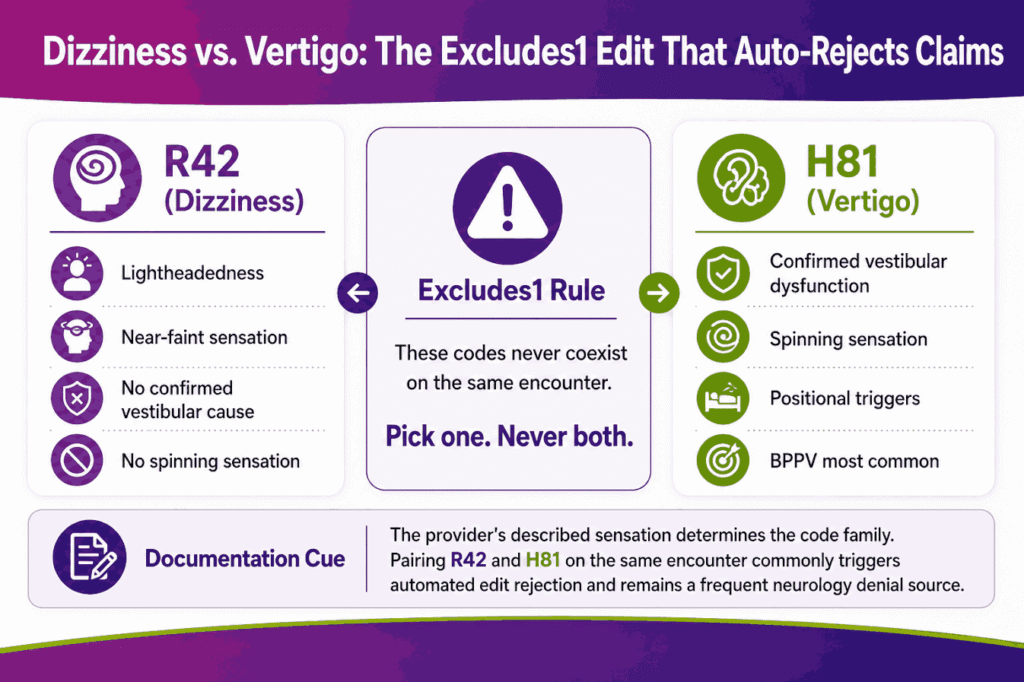
The ICD-10 code for dizziness is R42 (Dizziness and giddiness), a billable symptom code covering lightheadedness and unspecified vertigo. R42 applies when documentation describes a sensation of unsteadiness without a confirmed vestibular cause. Vertigo with a confirmed vestibular origin codes to the H81 family in the ear chapter rather than to R42.
Vertigo, the sensation that the external environment is moving, divides into peripheral and central origins. Peripheral vertigo originates in the inner ear or vestibular nerve. Central vertigo originates in the brainstem or cerebellum. Benign paroxysmal positional vertigo (BPPV) is the most common peripheral cause.
The following table presents the most-reported dizziness and vertigo ICD-10 codes:
| ICD-10 Code | Description | Origin |
|---|---|---|
| R42 | Dizziness and giddiness | Symptom |
| H81.10 | Benign paroxysmal vertigo, unspecified ear | Peripheral |
| H81.13 | Benign paroxysmal vertigo, bilateral | Peripheral |
| H81.4 | Vertigo of central origin | Central |
| H81.0- | Ménière’s disease | Peripheral |
| H81.8X9 | Other disorders of vestibular function, unspecified ear | Peripheral |
An Excludes1 note governs R42 and the H81 vertigo codes. R42 and H81 codes cannot be reported together for the same encounter, because an Excludes1 note designates conditions that never coexist on a single claim. The coder selects R42 for unexplained dizziness or H81 for confirmed vestibular dysfunction, never both. This Excludes1 conflict ranks among the top neurology coding denials, since automated edits reject claims pairing the two codes.
Documentation distinguishes dizziness from vertigo through the recorded sensation. Lightheadedness and near-faint support R42. A spinning sensation with positional triggers supports an H81 code. The provider’s description of the sensation determines the code family.
Syncope ICD-10 Codes
The ICD-10 code for syncope is R55 (Syncope and collapse), a billable symptom code documenting transient loss of consciousness with spontaneous recovery. R55 records the event regardless of cause, since the underlying etiology, vasovagal, cardiac, or neurologic, often remains under investigation at the time of the encounter. Syncope cross-codes with neurology workups because seizure, transient ischemic attack, and orthostatic intolerance enter the differential diagnosis.
Syncope differs from dizziness and vertigo in the loss of consciousness. R42 (dizziness) and H81 (vertigo) document sensations without loss of consciousness. R55 (syncope) documents a transient loss of consciousness. The presence or absence of consciousness loss in the chart determines whether coding moves to R55 or remains in the dizziness family.
R55 establishes medical necessity for the syncope evaluation. The code justifies a tilt-table test, electrocardiogram, or neurologic workup ordered to identify the cause. Documentation of the witnessed event, recovery time, and absence of postictal confusion supports R55 over a seizure code.
Peripheral Neuropathy ICD-10 Codes
The ICD-10 code for peripheral neuropathy is G62.9 (Polyneuropathy, unspecified), the default code when neuropathy type and cause are undocumented. Peripheral neuropathy describes damage to peripheral nerves, producing numbness, weakness, or pain, most often in the hands and feet. The term “neuropathy” alone underperforms in audits, since unspecified neuropathy codes invite documentation requests and downcoding.
The following table presents the most-reported ICD-10 codes for Neuropathy:
| ICD-10 Code | Description | Coding Note |
|---|---|---|
| G62.9 | Polyneuropathy, unspecified | Default; high audit scrutiny |
| G60.9 | Hereditary and idiopathic neuropathy, unspecified | Idiopathic and inherited forms |
| G60.0 | Hereditary motor and sensory neuropathy | Charcot-Marie-Tooth disease |
| G62.0 | Drug-induced polyneuropathy | Add code for the causative drug |
| G62.81 | Critical illness polyneuropathy | ICU-associated |
| G63 | Polyneuropathy in diseases classified elsewhere | Manifestation; code underlying condition first |
| G90.09 | Idiopathic peripheral autonomic neuropathy | Autonomic involvement |
Diabetic neuropathy follows a combination-coding rule that captures both the diabetes and the neuropathy in a single code. Type 2 diabetes mellitus with diabetic polyneuropathy codes to E11.42, the most common diabetic peripheral neuropathy code. The E11.4 subcategory subdivides by neuropathy type:
- E11.40: Type 2 diabetes mellitus with diabetic neuropathy, unspecified
- E11.41: Type 2 diabetes mellitus with diabetic mononeuropathy
- E11.42: Type 2 diabetes mellitus with diabetic polyneuropathy
- E11.43: Type 2 diabetes mellitus with diabetic autonomic (poly)neuropathy
- E11.44: Type 2 diabetes mellitus with diabetic amyotrophy
Parallel families exist for Type 1 diabetes (E10.40–E10.44) and other specified diabetes (E13.40–E13.44). The combination code E11.42 captures both the diabetes and the polyneuropathy, so coders do not assign a separate G62.x code for the same neuropathy. Assigning both E11.42 and a standalone polyneuropathy code duplicates the diagnosis and triggers a denial.
The manifestation rule governs neuropathy in diseases classified elsewhere. G63 (Polyneuropathy in diseases classified elsewhere) carries a “code first” instruction. The underlying condition codes first, followed by G63. Sequencing G63 before the underlying condition reverses the required order and produces a sequencing-error denial. The combination code E11.42 differs from this manifestation pairing, since E11.42 already integrates the etiology and the neuropathy into one code.
Other Common Peripheral Nerve Codes
Peripheral nerve compression and cranial nerve disorders generate 4 high-frequency neurology codes outside the polyneuropathy families. Each code requires anatomic specificity that drives both reimbursement and audit defense.
The following table presents 4 common peripheral and cranial nerve codes:
| ICD-10 Code | Description | Specificity Requirement |
|---|---|---|
| G56.00 | Carpal tunnel syndrome, unspecified upper limb | Laterality (right G56.01, left G56.02) |
| G51.0 | Bell’s palsy | None at category level |
| G50.0 | Trigeminal neuralgia | None at category level |
| M54.30 | Sciatica, unspecified side | Laterality (right M54.31, left M54.32) |
Sciatica codes outside the nervous system chapter. Sciatica maps to M54.3 in the musculoskeletal chapter (Chapter 13), not to a G-code, and lumbago with sciatica codes to M54.4. Coders searching the nervous system chapter for sciatica miss the correct code family, producing a common miscode.
Laterality omission ranks among the most frequent peripheral nerve denials. Carpal tunnel syndrome and sciatica require a 6th or 5th character identifying the affected side. Reporting the unspecified-side code (G56.00 or M54.30) when the chart documents a specific side invites a documentation request and delays payment.
Dementia ICD-10 Codes
The ICD-10 code for dementia is F03.90 (Unspecified dementia, unspecified severity, without behavioral disturbance, psychotic disturbance, mood disturbance, and anxiety), the default code restructured in FY2024. The dementia codes F01 (vascular dementia), F02 (dementia in diseases classified elsewhere), and F03 (unspecified dementia) underwent a major restructure effective October 1, 2023, adding mandatory severity and behavioral-disturbance characters.
The restructured dementia codes encode severity through the 4th character:
- Unspecified severity: .8 or .9 (F03.90, F03.91)
- Mild: .A (F03.A0, F03.A11)
- Moderate: .B (F03.B0, F03.B11)
- Severe: .C (F03.C0, F03.C11)
The behavioral-disturbance subdivisions follow the severity character. A dementia code documents the presence or absence of agitation, psychotic disturbance, mood disturbance, or anxiety. F03.90 documents unspecified dementia without any disturbance. F03.911 documents unspecified dementia, unspecified severity, with agitation.
The following table presents the primary ICD-10 codes for Dementia by family:
| ICD-10 Code | Description | Coding Note |
|---|---|---|
| F03.90 | Unspecified dementia, unspecified severity, without disturbance | Default dementia code |
| F03.A0–F03.C4 | Unspecified dementia by severity and disturbance | FY2024 severity matrix |
| F01.50 | Vascular dementia, unspecified severity, without disturbance | Vascular etiology |
| F01.A0–F01.C4 | Vascular dementia by severity and disturbance | FY2024 severity matrix |
| F02.80 | Dementia in diseases classified elsewhere, without disturbance | Manifestation; code etiology first |
| G30.9 | Alzheimer’s disease, unspecified | Etiology; codes before F02.8- |
| G31.83 | Dementia with Lewy bodies | Lewy body dementia |
Alzheimer’s dementia follows a mandatory etiology-first pairing. Alzheimer’s disease codes to G30.9 (etiology), followed by F02.8- (the dementia manifestation). The G30.9 code sequences first, and the F02.8- code documents the dementia with its severity and disturbance characteristics. Coding F02.8- alone, without the G30.9 etiology code, omits the required underlying diagnosis and triggers a denial.
The dementia restructure represents the single largest neurology coding change of the past 3 years. Cheat sheets and templates built before October 1, 2023, reference deleted codes such as F03.90 used without severity granularity, or F02.81 as a billable code. F02.81 converted to a parent code and now requires a severity-specific child code. Outdated dementia codes now produce denials on claims that passed cleanly before the restructure.
Seizure and Epilepsy ICD-10 Codes
The ICD-10 code for seizure is R56.9 (Unspecified convulsions), a billable symptom code documenting a seizure event without a confirmed epilepsy diagnosis. The ICD-10 code for epilepsy is the G40 family, which documents a confirmed seizure disorder. R56.9 and G40 separate the symptom from the diagnosis, mirroring the headache and dizziness families.
The G40 family subdivides along epilepsy type, intractability, and status epilepticus. Status epilepticus describes a prolonged seizure or repeated seizures without recovery between events. The 7th character documents intractability and status.
The following table presents the most-reported ICD-10 codes for Epilepsy and seizures:
| ICD-10 Code | Description | Type |
|---|---|---|
| R56.9 | Unspecified convulsions | Symptom |
| G40.909 | Epilepsy, unspecified, not intractable, without status epilepticus | Diagnosis |
| G40.409 | Other generalized epilepsy, not intractable, without status epilepticus | Diagnosis |
| G40.209 | Localization-related symptomatic epilepsy with complex partial seizures, not intractable | Diagnosis |
| G40.311 | Generalized idiopathic epilepsy, intractable, with status epilepticus | Diagnosis |
Seizure coding transitions from R56.9 to G40 as documentation matures. A first unexplained seizure codes to R56.9. A confirmed epilepsy diagnosis after workup codes to the corresponding G40 code with its intractability and status characters. The symptom code R56.9 establishes medical necessity for the EEG and neuroimaging that confirm the epilepsy diagnosis.
Movement Disorder ICD-10 Codes
The ICD-10 codes for movement disorders document Parkinson’s disease, tremor, and restless legs syndrome. Parkinson’s disease coding changed in FY2024, when the single G20 code expanded into 5 specific codes. G20 converted to a non-billable parent code, and coders now assign a child code identifying dyskinesia and motor fluctuations.
The expanded Parkinson’s disease codes encode 2 clinical features:
- G20.A1: Parkinson’s disease without dyskinesia, without mention of fluctuations
- G20.A2: Parkinson’s disease without dyskinesia, with fluctuations
- G20.B1: Parkinson’s disease with dyskinesia, without mention of fluctuations
- G20.B2: Parkinson’s disease with dyskinesia, with fluctuations
- G20.C: Parkinsonism, unspecified
The following table presents the primary movement disorder ICD-10 codes:
| ICD-10 Code | Description | Coding Note |
|---|---|---|
| G20.A1 | Parkinson’s disease without dyskinesia, without fluctuations | Default Parkinson’s code |
| G20.C | Parkinsonism, unspecified | Use when type undocumented |
| G21.- | Secondary parkinsonism | Drug-induced or external cause |
| R25.1 | Tremor, unspecified | Symptom code |
| G25.0 | Essential tremor | Diagnosis code |
| G25.81 | Restless legs syndrome | Diagnosis code |
Parkinson’s disease with dementia follows the same etiology-first pairing as Alzheimer’s dementia. Parkinson’s disease codes first (G20.A1–G20.C), followed by the dementia manifestation code F02.8- with its severity and disturbance characters. The Parkinson’s code documents the etiology, and the F02.8- code documents the associated dementia. Documentation that fails to specify dyskinesia and motor fluctuations defaults to G20.A1, the least-specific billable Parkinson’s code.
Other High-Frequency Neurology Codes
Four additional neurology conditions generate high search and claim volume across multiple ICD-10-CM chapters. Multiple sclerosis, stroke, transient ischemic attack, and Bell’s palsy each carry distinct coding rules.
The following table presents 4 high-frequency neurology codes:
| ICD-10 Code | Description | Chapter |
|---|---|---|
| G35 | Multiple sclerosis | Nervous system (G00–G99) |
| I63.9 | Cerebral infarction, unspecified | Circulatory (I60–I69) |
| G45.9 | Transient cerebral ischemic attack, unspecified | Nervous system (G00–G99) |
| G51.0 | Bell’s palsy | Nervous system (G00–G99) |
Stroke codes outside the nervous system chapter. Cerebral infarction (stroke) codes to the I63 family in the circulatory chapter (Chapter 9), not to a G-code. Transient ischemic attack, by contrast, codes to G45.9 in the nervous system chapter. This split places two closely related cerebrovascular conditions in separate chapters, producing a common coder navigation error.
Multiple sclerosis codes to a single category, G35, without severity or laterality subdivisions. The simplicity of G35 contrasts with the multi-character precision required for migraine, dementia, and Parkinson’s disease.
Symptom Codes vs Diagnosis Codes: The Coder’s Decision Framework
Neurology coding follows a decision framework that selects between a symptom code (R-chapter) and a diagnosis code (G-chapter) based on documentation maturity. The symptom code applies when documentation describes a complaint without a confirmed cause. The diagnosis code applies when the provider records a definitive condition. The framework determines both code selection and medical-necessity defense.
Symptom codes establish medical necessity for the diagnostic workup. R51.9 (headache) justifies neuroimaging. R42 (dizziness) justifies vestibular testing. R56.9 (convulsions) justifies an EEG. The symptom code documents why the workup occurred, and the resulting diagnosis code documents what the workup found.
The following table maps neurology symptom codes to their likely definitive diagnosis codes:
| Symptom Code | Symptom | Likely Diagnosis Code | Diagnosis |
|---|---|---|---|
| R51.9 | Headache | G43.909 | Migraine |
| R42 | Dizziness | H81.10 | Benign paroxysmal positional vertigo |
| R55 | Syncope | G90.09 | Autonomic dysfunction |
| R56.9 | Convulsions | G40.909 | Epilepsy |
| R25.1 | Tremor | G20.A1 | Parkinson’s disease |
| R20.2 | Numbness and tingling | G62.9 | Polyneuropathy |
The symptom-to-diagnosis transition occurs once documentation confirms the cause. Coders retain the symptom code at the initial encounter and move to the diagnosis code at the encounter where the provider records the confirmed condition. Reporting a definitive diagnosis code before documentation confirms the diagnosis overstates the clinical certainty and exposes the claim to an audit.
Top Neurology Coding Errors That Trigger Denials
Neurology coding produces 5 recurring errors that drive claim denials. Each error reduces first-pass acceptance and increases the cost to collect.
The 5 most frequent neurology coding errors are:
- Overusing unspecified codes: Defaulting to G62.9, F03.90, or G43.909 when documentation supports a specific code invites downcoding and audit scrutiny.
- Omitting laterality: Reporting unspecified-side codes for carpal tunnel (G56.00) or sciatica (M54.30) when the chart documents a side delays payment.
- Violating Excludes1 notes: Pairing R42 (dizziness) with an H81 (vertigo) code on one claim triggers an automated edit rejection.
- Reversing etiology-manifestation sequencing: Coding F02.8- before G30.9 (Alzheimer’s) or G63 before the underlying condition produces a sequencing-error denial.
- Using outdated codes: Reporting deleted codes, such as single-character G20 or pre-restructuring dementia codes, causes edits on claims that previously passed.
Each error connects directly to clean-claim rate. A neurology practice that reduces these 5 errors raises first-pass acceptance and lowers denial-related rework. Many practices route this work to dedicated neurology billing services that enforce documentation review and code-set currency at the point of coding. The errors originate in documentation review and code-set currency rather than in code lookup.
Frequently Asked Questions
What Is The ICD-10 Code For Headache?
The ICD-10 code for headache is R51.9 (Headache, unspecified), a billable symptom code that documents head pain without a confirmed cause.
Is R51.9 Billable?
R51.9 is a billable ICD-10 code, though payers frequently deny R51.9 as a primary diagnosis when documentation supports a more specific headache code, such as a G43 migraine code.
What Is The Difference Between G62.9 And The Diabetic Neuropathy Codes?
G62.9 codes polyneuropathy of unspecified cause, while E11.42 codes Type 2 diabetes mellitus with diabetic polyneuropathy as a combination code that captures both the diabetes and the neuropathy in one code.
Did The Dementia ICD-10 Codes Change In 2024?
The dementia codes F01, F02, and F03 restructured effective October 1, 2023, adding mandatory severity characters (A for mild, B for moderate, C for severe) and behavioral-disturbance subdivisions.
Can You Code Dizziness And Vertigo Together?
R42 (dizziness) and H81 (vertigo) codes cannot be reported together on one claim, because an Excludes1 note designates the two conditions as mutually exclusive for a single encounter.
What Is The ICD-10 Code For Parkinson’s Disease?
The ICD-10 code for Parkinson’s disease is G20.A1 (Parkinson’s disease without dyskinesia, without mention of fluctuations) as the default, after G20 expanded into 5 specific codes effective October 1, 2023.
What Is The ICD-10 Code For Peripheral Neuropathy?
The ICD-10 code for peripheral neuropathy is G62.9 (Polyneuropathy, unspecified), with diabetic peripheral neuropathy coded to E11.42 for Type 2 diabetes.
How Do You Code Alzheimer’s Dementia?
Alzheimer’s dementia codes G30.9 (Alzheimer’s disease) first as the etiology, followed by F02.8- as the dementia manifestation with its severity and disturbance characters.
What Is The ICD-10 Code For Dizziness?
The ICD-10 code for dizziness is R42 (Dizziness and giddiness), a billable symptom code covering lightheadedness and unspecified vertigo.
Does Stroke Code To A G-Code?
Stroke codes to the I63 family in the circulatory chapter (I60–I69), not to a nervous system G-code, while transient ischemic attack codes to G45.9 in the nervous system chapter.