ICD-10 is the World Health Organization’s standardized system for classifying diseases and health-related problems. It is used to assign alphanumeric diagnosis codes and to record patient functioning.
ICD-10 diagnosis codes are structured alphanumeric identifiers such as E11.9 (type 2 diabetes without complications) or J45.901 (unspecified asthma) assigned to every documented condition. These codes drive medical billing, insurance reimbursement, epidemiological tracking, and clinical decision-making worldwide.
ICD-10’s functioning component links diagnostic information to categories that describe activity and participation, based on WHO functioning/WHODAS concepts. It allows recording of disability and functional status alongside diagnoses. This supports outcome measurement and health services planning.
Limitations of ICD-10 include variable coding accuracy between settings, limited clinical granularity for some conditions, and dependence on coder training and documentation quality. Validation studies and systematic reviews report mixed positive predictive values and variable sensitivity for specific diagnoses.
A recent narrative review published in JAMIA Open reported real-world accuracy data. In a qualitative AHIMA Foundation study of 156 coding professionals, 38% reported perceived changes in accuracy after ICD-10 implementation, with some reporting an average increase of 25% and others an average decrease of 13%.
What is ICD-10?
ICD-10 (International Classification of Diseases, 10th Revision) is a medical classification system developed and maintained by the World Health Organization (WHO) that assigns standardized alphanumeric codes to diseases, symptoms, abnormal findings, injuries, and external causes of health conditions.
Its purpose is to create a universal language for documenting health conditions across clinical, administrative, and statistical settings. ICD-10 codes allow healthcare providers to record diagnoses consistently, regardless of language, geography, or healthcare system.
The WHO governs ICD-10 at the international level, publishing and updating the core classification framework. In the United States, the Centers for Medicare and Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) maintain ICD-10-CM, the clinical modification adapted for domestic use.
ICD-10 is used across four primary functions:
Every patient encounter that results in a documented diagnosis requires at least one ICD-10 code. Without a valid ICD-10 diagnosis code, a medical claim cannot be processed by a payer.
What is ICD-10 Diagnosis Code List?
An ICD-10 diagnosis code list is a structured reference of alphanumeric codes assigned to every documented disease, condition, symptom, and injury under the ICD-10-CM classification system. Each code maps directly to a specific diagnosis, enabling consistent use across medical billing, clinical documentation, and insurance claim processing. The sections below organize ICD-10 diagnosis codes by clinical category.
Gastrointestinal (GI) Conditions
The following ICD-10 codes cover the most frequently documented gastrointestinal conditions in clinical practice, used across outpatient visits, inpatient admissions, and insurance claim submissions.
| ICD-10 Code | Description |
|---|---|
| K21.0 | GERD with esophagitis |
| K21.9 | GERD without esophagitis |
| R10.9 | Unspecified abdominal pain |
| R10.0 | Acute abdomen |
| R10.13 | Epigastric pain |
| K59.00 | Constipation, unspecified |
| K59.01 | Slow transit constipation |
| R19.7 | Diarrhea, unspecified |
| R11.0 | Nausea alone |
| R11.2 | Nausea with vomiting |
| R13.10 | Dysphagia, unspecified |
| K92.1 | Melena (GI bleed) |
| K92.2 | GI hemorrhage, unspecified |
| K62.5 | Rectal bleeding |
| K64.9 | Hemorrhoids, unspecified |
| K58.9 | IBS without diarrhea |
| K58.0 | IBS with diarrhea |
| K80.20 | Cholelithiasis without cholecystitis |
| I85.00 | Esophageal varices without bleeding |
| I85.01 | Esophageal varices with bleeding |
| K56.60 | Small bowel obstruction, unspecified |
| R10.2 | Pelvic pain |
| R63.4 | Abnormal weight loss |
| R63.0 | Anorexia |
Cardiovascular Diseases
The following ICD-10 codes cover the most frequently documented cardiovascular conditions used across emergency, inpatient, and outpatient clinical settings for billing, diagnosis documentation, and insurance claim filing.
| ICD-10 Code | Description |
|---|---|
| R07.9 | Chest pain, unspecified |
| R07.1 | Chest pain on breathing |
| R07.2 | Precordial pain |
| I25.10 | CAD without angina pectoris |
| I25.110 | CAD with unstable angina |
| I10 | Essential hypertension |
| I48.91 | Atrial fibrillation, unspecified |
| I48.0 | Paroxysmal atrial fibrillation |
| R00.0 | Tachycardia, unspecified |
| R00.1 | Bradycardia, unspecified |
| R00.2 | Palpitations |
| I95.9 | Hypotension, unspecified |
| I50.9 | CHF, unspecified |
| I50.20 | HFrEF, unspecified |
| I50.30 | HFpEF, unspecified |
| I25.5 | Ischemic cardiomyopathy |
| I42.9 | Cardiomyopathy, unspecified |
| R79.89 | Elevated troponin |
| I21.4 | NSTEMI |
| I63.9 | Stroke/CVA, unspecified |
| I82.401 | DVT, unspecified, right leg |
| I82.402 | DVT, unspecified, left leg |
| I26.99 | Pulmonary embolism, unspecified |
Respiratory Conditions
The following ICD-10 codes cover the most frequently documented respiratory conditions used across emergency, inpatient, and outpatient settings for clinical documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| J44.1 | COPD with acute exacerbation |
| J44.0 | COPD with acute lower respiratory infection |
| J44.9 | COPD, unspecified |
| J45.901 | Asthma, unspecified, uncomplicated |
| J45.51 | Severe persistent asthma with acute exacerbation |
| J18.9 | Pneumonia, unspecified organism |
| J69.0 | Aspiration pneumonia |
| R06.00 | Dyspnea/shortness of breath, unspecified |
| R05.9 | Cough, unspecified |
| R09.02 | Hypoxia |
| J10.01 | Influenza A with pneumonia |
| J10.1 | Influenza A with other respiratory manifestations |
| J32.9 | Sinusitis, unspecified |
Neurological Disorders
The following ICD-10 codes cover the most frequently documented neurological conditions used across inpatient, outpatient, and emergency settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| R51.9 | Headache, unspecified |
| G43.909 | Migraine, unspecified, without aura |
| G43.109 | Migraine with aura, unspecified |
| R42 | Dizziness and giddiness |
| M62.81 | Muscle weakness, generalized |
| G40.909 | Seizure disorder, unspecified |
| G93.41 | Acute metabolic encephalopathy |
| G93.40 | Encephalopathy, unspecified |
| F03.90 | Dementia, unspecified |
| R41.3 | Memory loss, unspecified |
| G60.9 | Neuropathy, unspecified |
| G57.00 | Peripheral neuropathy, unspecified |
Musculoskeletal Pain
The following ICD-10 codes cover the most frequently documented musculoskeletal pain conditions used across orthopedic, primary care, and inpatient settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| M54.50 | Low back pain, unspecified |
| M54.51 | Vertebrogenic low back pain |
| M54.59 | Other back pain |
| M54.2 | Cervicalgia/neck pain |
| M54.16 | Lumbar radiculopathy |
| M54.12 | Cervical radiculopathy |
| M47.816 | Lumbar spondylosis without myelopathy |
| M48.06 | Lumbar spinal stenosis |
| M25.611 | Right shoulder pain |
| M25.612 | Left shoulder pain |
| M25.561 | Knee pain, unspecified |
| M25.561 | Right knee pain |
| M25.562 | Left knee pain |
| M25.551 | Right hip pain |
| M25.552 | Left hip pain |
| M72.2 | Plantar fasciitis |
| M94.0 | Costochondritis |
| M54.3 | Sciatica |
Bone, Joint and Inflammatory Conditions
The following ICD-10 codes cover the most frequently documented bone, joint, and inflammatory conditions used across rheumatology, orthopedic, and primary care settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| M81.0 | Age-related osteoporosis without fracture |
| M80.00 | Age-related osteoporosis with fracture |
| M85.80 | Osteopenia, unspecified |
| M19.90 | Osteoarthritis, unspecified |
| M19.011 | Primary osteoarthritis, right shoulder |
| M05.9 | Rheumatoid arthritis, unspecified |
| M06.9 | Inflammatory arthritis, unspecified |
| M10.9 | Gout, unspecified |
| M10.011 | Idiopathic gout, right shoulder |
| M79.3 | Fibromyalgia |
| M86.9 | Osteomyelitis, unspecified |
Hematologic and Lab Abnormalities
The following ICD-10 codes cover the most frequently documented hematologic and laboratory abnormality conditions used across inpatient, outpatient, and laboratory settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| D64.9 | Anemia, unspecified |
| D50.9 | Iron deficiency anemia, unspecified |
| D50.0 | Iron deficiency anemia due to blood loss |
| D72.829 | Leukocytosis, unspecified |
| D69.6 | Thrombocytopenia, unspecified |
| D75.838 | Thrombocytosis, unspecified |
| D61.818 | Pancytopenia, unspecified |
Electrolyte and Metabolic Disorders
The following ICD-10 codes cover the most frequently documented electrolyte and metabolic conditions used across inpatient, outpatient, and laboratory settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| E87.6 | Hypokalemia |
| E83.42 | Hypomagnesemia |
| E78.5 | Hyperlipidemia, unspecified |
| E78.1 | Hypertriglyceridemia |
| R73.03 | Prediabetes |
| K76.0 | Fatty liver/Hepatic steatosis |
| R74.01 | Elevated liver enzymes/Transaminitis |
Mental Health Conditions
The following ICD-10 codes cover the most frequently documented mental health conditions used across psychiatric, primary care, and inpatient settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| F41.1 | Generalized anxiety disorder |
| F41.9 | Anxiety disorder, unspecified |
| F33.9 | Major depressive disorder, unspecified |
| F33.0 | MDD, single episode, mild |
| F31.9 | Bipolar disorder, unspecified |
| F20.9 | Schizophrenia, unspecified |
| F43.10 | PTSD, unspecified |
| F90.9 | ADHD, unspecified |
| G47.00 | Insomnia, unspecified |
| R45.851 | Suicidal ideation |
| F10.20 | Alcohol dependence, uncomplicated |
Genitourinary and Reproductive Conditions
The following ICD-10 codes cover the most frequently documented genitourinary and reproductive conditions used across urology, gynecology, and primary care settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| N39.0 | Urinary tract infection, unspecified |
| R30.0 | Dysuria |
| R31.9 | Hematuria, unspecified |
| R33.9 | Urinary retention, unspecified |
| R32 | Urinary incontinence, unspecified |
| N31.9 | Neurogenic bladder, unspecified |
| N40.1 | BPH with lower urinary tract symptoms |
| N40.0 | BPH without lower urinary tract symptoms |
| N52.9 | Erectile dysfunction, unspecified |
| N76.0 | Bacterial vaginosis |
Infections and Sepsis
The following ICD-10 codes cover the most frequently documented infection and sepsis conditions used across emergency, inpatient, and critical care settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| L03.90 | Cellulitis, unspecified |
| L03.011 | Cellulitis of right finger |
| L03.012 | Cellulitis of left finger |
| R78.81 | Bacteremia |
| A41.9 | Sepsis, unspecified |
| R65.21 | Septic shock |
| N10 | Acute pyelonephritis |
| N11.9 | Chronic pyelonephritis |
Renal Disorders
The following ICD-10 codes cover the most frequently documented renal conditions used across nephrology, inpatient, and emergency settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| N17.9 | Acute kidney injury, unspecified |
| N18.1 | Chronic kidney disease, stage 1 |
| N18.2 | Chronic kidney disease, stage 2 |
| N18.3 | Chronic kidney disease, stage 3 |
| N18.4 | Chronic kidney disease, stage 4 |
| N18.5 | Chronic kidney disease, stage 5 |
| N18.6 | End stage renal disease (ESRD) |
| N13.30 | Hydronephrosis, unspecified |
Cancer and Neoplasms
The following ICD-10 codes cover the most frequently documented cancer and neoplasm conditions used across oncology, inpatient, and surgical settings for diagnosis documentation, billing, and insurance claim processing.
| ICD-10 Code | Description |
|---|---|
| C34.90 | Lung cancer, unspecified |
| C34.10 | Lung cancer, upper lobe |
| C18.9 | Colon cancer, unspecified |
| C61 | Prostate cancer |
| E04.1 | Thyroid nodule, single |
| E04.2 | Thyroid nodule, multiple |
How Does ICD-10 Function?
The functions of ICD-10 extend beyond simple disease labeling. The system operates as the structural backbone of modern healthcare, connecting clinical documentation, financial processing, and population health reporting through a single standardized code set. Each function below represents a distinct operational role ICD-10 plays across healthcare settings.
1. Standardizes Disease Identification
ICD-10 functions as a uniform coding system that assigns a single, globally recognized alphanumeric code to every documented disease, condition, symptom, and injury. This eliminates reliance on varied clinical terminology across providers, facilities, and countries.
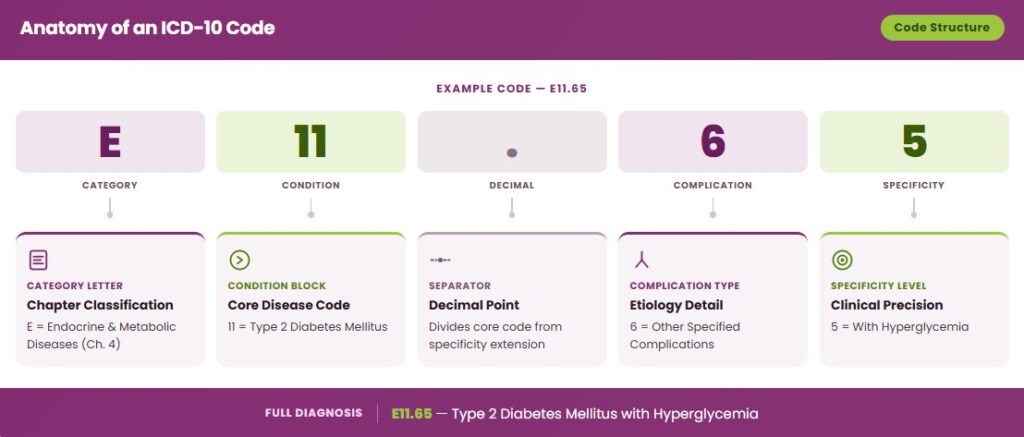
Each ICD-10 code follows a structured alphanumeric format, a letter followed by up to six characters, where every additional character increases diagnostic specificity. For example, M54.50 identifies unspecified low back pain, while M54.51 specifically identifies vertebrogenic low back pain. This structure ensures that two clinicians documenting the same condition will always arrive at the same code.
ICD-10 operates within the WHO’s global classification framework, making it the standard diagnostic language across 130+ countries. This enables health data to be compared, analyzed, and reported consistently across international health systems and research institutions.
By replacing free-text diagnosis descriptions with standardized codes, ICD-10 removes ambiguity from diagnosis terminology. A condition documented as “sugar disease,” “high blood sugar,” or “diabetes” is mapped to a single verified code, eliminating interpretation errors in billing, research, and clinical handoffs.
2. Supports Medical Documentation
ICD-10 ensures accurate recording of diagnoses by requiring clinicians to assign a specific, verified code to every documented condition at each patient encounter. Vague or incomplete diagnosis entries are replaced by structured codes that capture disease type, etiology, severity, and laterality where applicable.
ICD-10 codes enhance clarity in patient health records by converting narrative clinical descriptions into a standardized format readable across all provider systems and electronic health record (EHR) platforms. A patient’s complete diagnostic history becomes consistently interpretable regardless of which facility or provider accesses the record.
The standardized code structure improves communication between providers by creating a shared diagnostic language across specialties, care settings, and geographic locations. A referring physician, specialist, and inpatient team can all interpret the same ICD-10 code without ambiguity or the need for additional clarification.
ICD-10 documentation also supports legal and compliance standards by creating an auditable record of every diagnosis tied to a clinical encounter. Payers, accreditation bodies, and regulatory agencies use ICD-10-coded records to verify medical necessity, assess care quality, and enforce documentation compliance under CMS and HIPAA guidelines.
3. Enables Medical Billing and Insurance Claims
ICD-10 codes directly link every documented diagnosis to the reimbursement process by establishing the clinical justification for each billed procedure or service. Without a valid ICD-10 code attached to a claim, a payer cannot determine whether a service was medically warranted or eligible for reimbursement.
ICD-10 code submission is a mandatory requirement for all insurance claim filings across Medicare, Medicaid, and private payers in the United States. Every CMS-1500 and UB-04 claim form requires at least one ICD-10-CM diagnosis code before a claim can be accepted for adjudication.
Payers use ICD-10 codes to validate medical necessity, confirming that the procedure or service billed is clinically appropriate for the documented diagnosis. A mismatch between the diagnosis code and the billed procedure is one of the most common triggers for automatic claim rejection.
Accurate ICD-10 coding directly reduces claim denials by ensuring the diagnosis code submitted matches payer coverage policies, LCD (Local Coverage Determination) guidelines, and NCD (National Coverage Determination) criteria. Specificity in code selection, choosing M54.51 over the unspecified M54.50, for example, can be the difference between a paid and a denied claim.
4. Helps in Data Collection and Reporting
ICD-10 codes aggregate healthcare data across hospitals, clinics, laboratories, and insurance systems into a single structured dataset. This aggregation allows health institutions to analyze patient populations, measure outcomes, and identify care gaps at a scale that unstructured clinical notes cannot support.
Epidemiological research depends on ICD-10 coded data to identify disease prevalence, incidence rates, and risk factors across defined populations. Researchers use ICD-10 data extracted from claims databases, EHR systems, and national registries to conduct population-level studies without requiring direct patient contact.
ICD-10 enables real-time tracking of disease trends and outbreak patterns by flagging abnormal increases in specific diagnosis codes across geographic regions. During the COVID-19 pandemic, ICD-10 codes such as U07.1 (COVID-19) and U09.9 (post-COVID condition) were rapidly deployed to monitor infection rates, hospitalization patterns, and long-term health impacts at a national level.
Government agencies and institutional bodies rely on ICD-10-coded data for mandatory public health reporting. The CDC, CMS, WHO, and state health departments all use ICD-10 data to fulfill reporting obligations, allocate healthcare resources, set reimbursement policy, and publish national health statistics, including the National Hospital Discharge Survey and the Global Burden of Disease report.
5. Improves Clinical Decision-Making
ICD-10 provides detailed diagnostic specificity that gives clinicians a precise, structured picture of a patient’s condition at every encounter. A code such as M80.011A, age-related osteoporosis of the right shoulder with current pathological fracture, initial encounter, communicates far more clinical detail than a general fracture notation, enabling faster and more accurate clinical decisions.
Diagnostic specificity directly supports treatment planning accuracy by ensuring the documented condition aligns with evidence-based treatment protocols. Clinical decision support systems (CDSS) integrated into EHR platforms use ICD-10 codes to trigger condition-specific treatment pathways, medication alerts, and preventive care recommendations at the point of care.
ICD-10 enables better outcome tracking by creating a longitudinal record of a patient’s diagnoses across encounters, providers, and care settings. Clinicians can analyze coded diagnosis histories to measure treatment response, monitor disease progression, and adjust care plans based on documented outcomes rather than recall or incomplete records.
Across multidisciplinary teams, including physicians, nurses, pharmacists, and care coordinators, ICD-10 codes serve as a shared clinical reference that eliminates the need to re-interpret diagnosis terminology at each handoff. Every team member accessing the same ICD-10 coded record works from an identical diagnostic baseline, reducing miscommunication and supporting coordinated, consistent patient care.
What are the Limitations of ICD-10?
ICD-10 operates as a comprehensive classification system, but its complexity introduces operational challenges across clinical, administrative, and billing functions. The limitations below represent the most documented barriers to accurate and efficient ICD-10 implementation.
Complexity & Code Volume: ICD-10-CM contains over 70,000 diagnosis codes, making navigation and accurate code selection a significant operational challenge. Coders must distinguish between highly specific codes, such as differentiating M80.011A from M80.012A based solely on laterality and encounter type, where a single character error produces an entirely different diagnosis entry.
Steep Learning Curve: Accurate ICD-10 coding requires formal training for both medical coders and clinical documentation specialists. The transition from ICD-9 to ICD-10 introduced a 400% increase in code volume, and clinicians face an increased documentation burden to support the specificity requirements that ICD-10 demands at every encounter.
Risk of Coding Errors: The specificity requirements of ICD-10 increase the risk of misclassification when documentation is incomplete or ambiguous. A coding error, such as assigning an unspecified code where a specific code is required, directly impacts claim reimbursement, medical necessity validation, and the accuracy of population health data derived from coded records.
Documentation Dependency: ICD-10 coding accuracy is entirely dependent on the quality and completeness of provider documentation. If a clinician documents “diabetes” without specifying type, complications, or insulin use, the coder cannot assign the correct code from the E11.x series, resulting in unspecified coding that weakens both billing accuracy and clinical data integrity.
What is the Difference Between ICD-10 and ICD-11?
The main difference between ICD-10 and ICD-11 is that ICD-11 is a fully digital, modernized classification system built to support contemporary healthcare needs, while ICD-10 was designed for paper-based and early electronic health record environments.
Version Evolution Context: ICD-10 was introduced by the WHO in 1992 and adopted by the United States in 2015. ICD-11 was officially released by the WHO in 2019 and came into effect globally on January 1, 2022. The United States has not yet mandated a transition date to ICD-11, meaning ICD-10-CM remains the active standard for clinical coding in the US.
Structural Differences: ICD-10 uses an alphanumeric structure with codes up to seven characters, organized across 21 chapters based on body system and disease etiology. ICD-11 introduces a fully digital framework with a stem code and extension code system, allowing multiple codes to be clustered together to represent a single complex condition, a capability ICD-10 does not support. ICD-11 also incorporates a content model that links each code to standardized clinical definitions, synonyms, and diagnostic criteria directly within the classification system.
Code Volume & Specificity: ICD-10-CM contains over 70,000 diagnosis codes. ICD-11 expands this to over 55,000 unique entities at the international level, but its extension code and clustering system allow for significantly greater diagnostic specificity than raw code volume suggests. ICD-11 also introduces new classification chapters not present in ICD-10, including traditional medicine conditions, sleep-wake disorders as a standalone chapter, and conditions related to sexual health.
Is VSD a Diagnosis or a Coding Term in ICD-10?
VSD (Ventricular Septal Defect) is a diagnosis. In ICD-10, it is classified under code Q21.0, a congenital cardiac malformation in which an abnormal opening exists between the right and left ventricles of the heart. “VSD” is the clinical abbreviation used by providers to document the condition; Q21.0 is the corresponding ICD-10 code assigned to that diagnosis for billing, documentation, and reporting purposes.
How Do ICD-10 and DSM-5 Work Together in Behavioral Health?
ICD-10 and DSM-5 work together in behavioral health by operating as complementary systems. DSM-5 provides the clinical framework for diagnosing mental health conditions, while ICD-10 provides the standardized codes required for documentation, billing, and reporting those diagnoses.
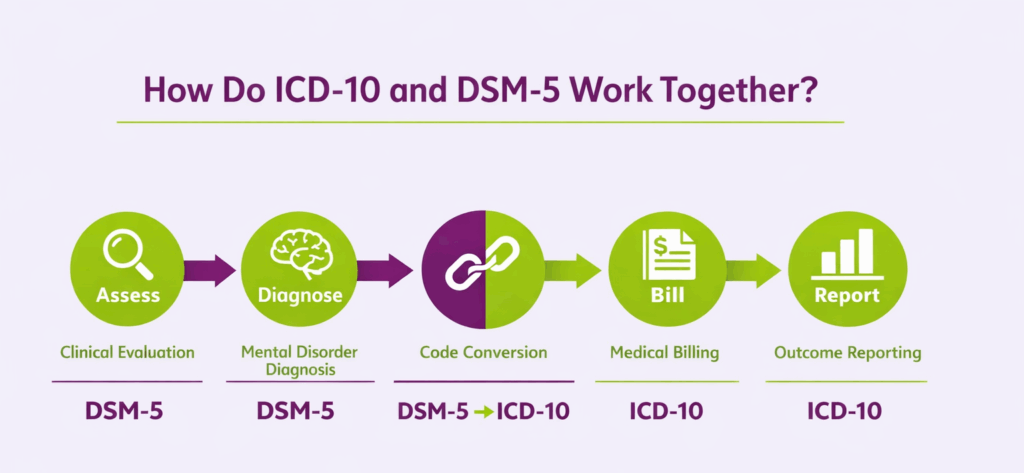
- Clinical Assessment: The clinician conducts a behavioral health evaluation using DSM-5 diagnostic criteria, which define the specific symptom thresholds, duration requirements, and functional impairment standards that must be met before a mental health diagnosis is assigned.
- Diagnosis: Once DSM-5 criteria are met, the clinician establishes a formal diagnosis using DSM-5 terminology. For example, a patient meeting the criteria for Major Depressive Disorder, single episode, mild, receives that DSM-5 diagnosis label.
- Code Selection: The DSM-5 diagnosis is then mapped to its corresponding ICD-10-CM code. DSM-5 includes ICD-10-CM codes directly within its diagnostic entries, Major Depressive Disorder, single episode, mild maps to F32.0, eliminating the need for a separate code lookup in most cases.
- Billing: The ICD-10-CM code derived from the DSM-5 diagnosis is submitted on the insurance claim. Payers recognize ICD-10 codes, not DSM-5 terminology, meaning the ICD-10 code is the operative billing identifier for every behavioral health service rendered.
- Reporting: ICD-10 coded behavioral health data is aggregated for institutional, state, and federal reporting. DSM-5 diagnoses converted to ICD-10 codes feed into national mental health databases, Medicaid and Medicare reporting systems, and epidemiological research on psychiatric condition prevalence and treatment outcomes.
Why Was ICD-9 Replaced by ICD-10?
ICD-9 was replaced by ICD-10 because its structure, code capacity, and specificity level were no longer sufficient to support modern clinical documentation, billing accuracy, or population health reporting requirements.
Limitations of ICD-9: ICD-9 contained approximately 14,000 diagnosis codes organized under a numeric-only structure that had reached its maximum capacity for expansion. The system lacked the ability to capture laterality, episode of care, disease severity, and combination diagnoses within a single code, forcing coders to use multiple imprecise codes to document conditions that ICD-10 captures in one specific entry. Its outdated structure also produced frequent code collisions, where unrelated conditions shared the same code due to space constraints.
Need for Greater Specificity: ICD-10 introduced an alphanumeric structure extending up to seven characters, enabling documentation of laterality (right vs. left), disease severity (mild, moderate, severe), episode of care (initial, subsequent, sequela), and condition etiology within a single code. This level of specificity was architecturally impossible within ICD-9’s numeric framework and became a clinical and administrative necessity as payer policies increasingly required precise diagnosis documentation to validate medical necessity.
Advancements in Medical Science: Diseases, procedures, and technologies that emerged or evolved after ICD-9’s development, including HIV/AIDS classifications, new cancer subtypes, genomic conditions, and advanced surgical procedures, could not be accurately represented within ICD-9’s limited code set. ICD-10 introduced dedicated code categories for these advancements, ensuring the classification system reflected the current state of medical science.
Data Accuracy & Reporting Improvements: ICD-10 significantly improved data accuracy by eliminating the vague, catch-all codes that ICD-9 relied on for undifferentiated conditions. The increased specificity of ICD-10 coded data produces more reliable epidemiological datasets, more precise reimbursement outcomes, and more actionable population health reports, directly addressing the data quality deficiencies that made ICD-9 inadequate for modern healthcare reporting standards.
Are ICD-10 and SNOMED Used Together in Healthcare?
Yes. ICD-10 and SNOMED CT (Systematized Nomenclature of Medicine Clinical Terms) are used together in healthcare. This is done through a formally maintained mapping system developed by the WHO and SNOMED International. SNOMED CT serves as the clinical reference terminology used at the point of care, capturing granular clinical concepts, findings, and procedures within EHR systems, while ICD-10 serves as the administrative classification system used for billing, reporting, and statistical analysis. When a clinician documents a condition using SNOMED CT terminology within an EHR, the system uses the SNOMED-to-ICD-10 map to automatically generate the corresponding ICD-10 code for claim submission and reporting purposes.
When Should Providers Use ICD-10 Instead of CPT?
Providers use ICD-10 codes and CPT codes for entirely different purposes. They are not interchangeable and are always used together, never in place of one another.
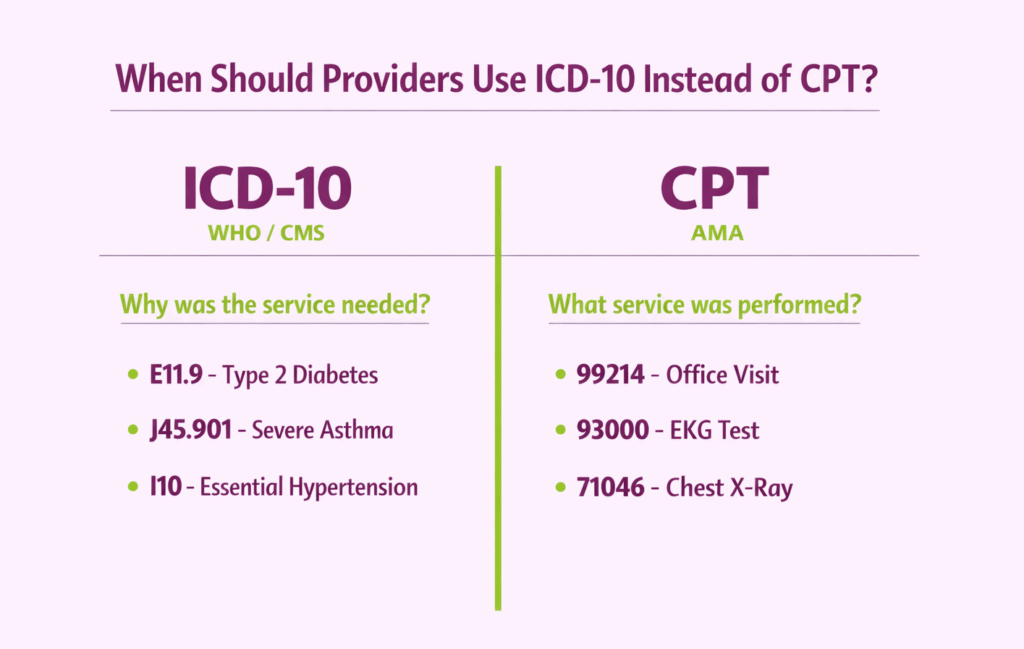
Purpose Distinction: ICD-10 codes classify diagnoses, every documented disease, condition, symptom, and injury a patient presents with. CPT (Current Procedural Terminology) codes classify procedures and services, including evaluations, treatments, tests, and interventions performed by the provider.
Diagnosis vs. Procedure Context: ICD-10 codes are assigned based on the documented diagnosis driving the clinical encounter. CPT codes in medical billing are assigned based on the specific service or procedure performed during that encounter. A patient presenting with type 2 diabetes (E11.9) who receives an office consultation receives both an ICD-10 code for the diagnosis and a CPT code, such as 99214, for the level of evaluation and management service provided.
Billing & Claims Submission Requirements: Every insurance claim requires both ICD-10 and CPT codes to be submitted together. The ICD-10 diagnosis code establishes medical necessity for the CPT procedure code. Without a valid ICD-10 code linked to each CPT service, the payer cannot verify that the procedure performed was clinically justified, resulting in automatic claim denial.
Clinical Documentation Requirements: Providers must document the diagnosis with sufficient specificity to support both the ICD-10 code selected and the CPT service billed. A documented diagnosis of unspecified chest pain (R07.9) linked to a high-complexity E&M service (CPT 99215) may trigger a medical necessity audit if the documentation does not support the complexity level billed. This makes accurate ICD-10 coding and thorough clinical documentation inseparable requirements in every patient encounter.
How Do SNOMED CT and ICD-10 Integrate in EHR Systems?
SNOMED CT and ICD-10 integrate within EHR systems through a structured mapping architecture that allows clinical documentation and administrative coding to operate simultaneously from a single point of data entry.
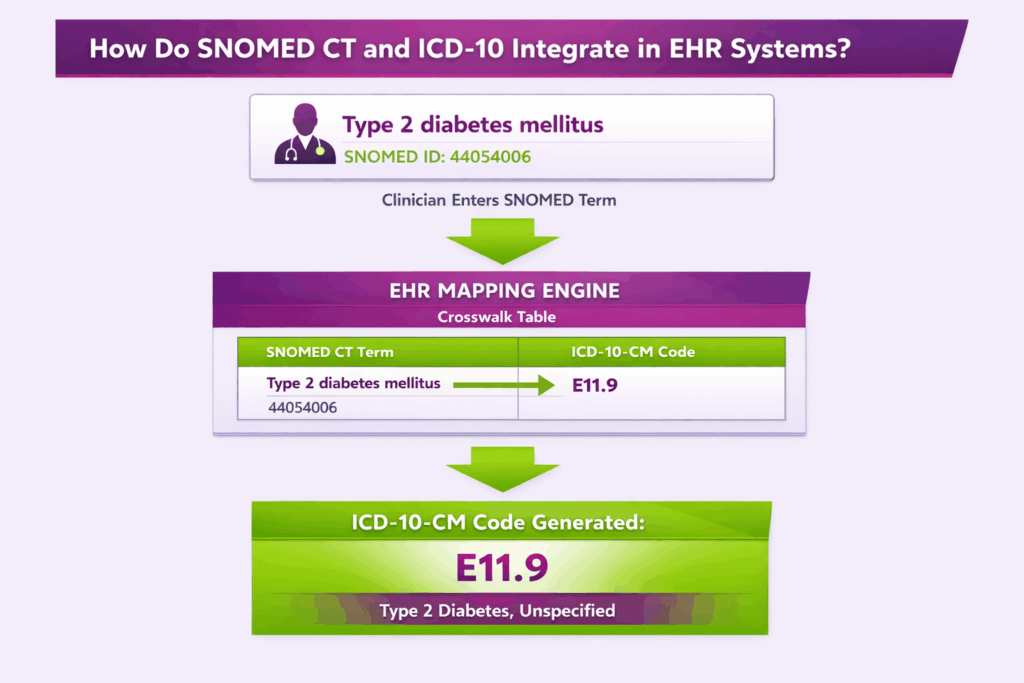
Terminology vs Classification Layer: SNOMED CT serves as the clinical terminology layer in an EHR, capturing granular, clinically precise concepts. These include findings, observations, procedures, and anatomical locations at the point of care. ICD-10 serves as the classification layer, converting clinical concepts into standardized codes required for billing, insurance reporting, and population health analysis. SNOMED CT prioritizes clinical detail; ICD-10 prioritizes administrative standardization.
Workflow Integration: During a clinical encounter, the provider documents diagnoses and findings using SNOMED CT terminology directly within the EHR interface. The EHR system then automatically maps the documented SNOMED CT concept to its corresponding ICD-10 code in the background, generating the administrative code required for claim submission without requiring the clinician to perform a separate coding step. This dual-layer workflow reduces documentation burden while maintaining both clinical precision and billing compliance.
Mapping Mechanisms: EHR systems use three primary tools to execute SNOMED CT to ICD-10 mapping. First, crosswalk tables maintained by SNOMED International and the WHO provide pre-built concept-to-code relationships between the two systems. Second, mapping tables within the EHR translate specific SNOMED CT concept IDs to their closest ICD-10-CM equivalents. Third, automated encoding tools embedded in the EHR apply mapping rules in real time, flagging cases where a one-to-one map does not exist and prompting the coder to manually select the most appropriate ICD-10 code.
How Do Medical Coders Assign ICD-10 Codes?
Medical coders assign ICD-10 codes by following a structured, step-by-step process that converts documented clinical information into verified, billable diagnosis codes for every patient encounter.
- Reviewing the Medical Documentation: The coder begins by reviewing the complete medical record for the encounter, including the physician’s notes, discharge summary, operative reports, lab results, and any additional clinical documentation that supports the diagnoses recorded during the visit.
- Identifying Key Diagnosis Information: The coder identifies the principal diagnosis, secondary diagnoses, comorbidities, complications, and any symptoms or conditions documented as clinically significant during the encounter. Each identified condition requires its own ICD-10 code assignment.
- Using the ICD-10-CM Codebook: The coder references the ICD-10-CM codebook, starting with the Alphabetic Index to locate the condition by its main term, then verifying the code in the Tabular List to confirm the full code, its description, and any instructional notes attached to that code entry.
- Following Official Coding Guidelines: The coder applies the Official ICD-10-CM Coding Guidelines published annually by CMS and NCHS, which govern sequencing rules, principal diagnosis selection, and condition-specific coding instructions that override general coding logic where applicable.
- Applying Coding Conventions: The coder applies ICD-10-CM conventions, including includes and excludes notes, code-first and use-additional-code instructions, and default code rules, to ensure every assigned code reflects the highest level of specificity supported by the documentation.
- Querying the Provider (If Needed): If the documentation is ambiguous, incomplete, or does not support the specificity required for accurate code assignment, the coder submits a formal clinical documentation improvement (CDI) query to the treating provider requesting clarification before finalizing the code.
- Entering Codes into the Billing System: Once all codes are verified and sequenced correctly, the coder enters the final ICD-10-CM codes into the practice management or hospital billing system, where they are attached to the corresponding CPT procedure codes and submitted as part of the insurance claim.
How does diagnosis coding impact the reimbursement process?
Accurate coding in medical billing establishes the medical necessity required for payers to approve and pay for billed procedures. This diagnostic data must align perfectly with reported services to ensure a seamless revenue cycle and prevent claim denials.