
Summary: The ICD-10 code for knee pain is M25.561 (right), M25.562 (left), or M25.569 (unspecified). But knee pain is a symptom code, not a diagnosis. When a confirmed diagnosis exists in the chart, that code takes primary.
Knee pain is one of the most common musculoskeletal complaints in US ambulatory care. The Centers for Disease Control and Prevention (CDC) reports that arthritis affects 53.2 million US adults, with the knee being the most commonly affected weight-bearing joint. The American Academy of Orthopaedic Surgeons (AAOS) lists total knee arthroplasty among the highest-volume orthopedic procedures in the US.
The ICD-10-CM code family for pain in the knee is M25.56x. M25.561 covers the right knee, M25.562 covers the left knee, and M25.569 covers an unspecified knee. But knee pain coding is different from disease coding. Knee pain (M25.56x) is a symptom code, not a diagnosis code, in ICD-10-CM. When the chart documents a confirmed diagnosis, such as osteoarthritis or a meniscus tear, that diagnosis takes primary.
This guide covers the M25.56x codes in detail, the related ICD-10 categories that often replace them (M17, M22, M23, M70.5, M76.5, S80 through S89), the procedural pairings for E&M visits, imaging, injections, physical therapy, and DME, and the denial patterns specific to symptom-versus-diagnosis sequencing.
What Is the ICD-10 Code for Knee Pain?
The ICD-10 code for knee pain is M25.56, with the fifth digit specifying laterality. The M25.56x family sits inside ICD-10-CM Chapter 13, “Diseases of the Musculoskeletal System and Connective Tissue,” under M25 (other joint disorders, not elsewhere classified).
What Are the M25.56x Codes for Pain in the Knee?
The M25.56x family contains three billable codes that differ only by laterality. None of these codes specifies cause, character, or chronicity.
| Code | Description |
|---|---|
| M25.561 | Pain in right knee |
| M25.562 | Pain in left knee |
| M25.569 | Pain in unspecified knee |
M25.561: Pain in Right Knee
M25.561 is the ICD-10 code for pain in the right knee. It is the highest-volume knee pain code in US claims data. The chart must document the right side and confirm pain is the presenting reason without a confirmed underlying diagnosis.
M25.562: Pain in Left Knee
M25.562 is the ICD-10 code for pain in the left knee. The chart must document the left side. M25.562 applies under the same symptom-only rules as M25.561.
M25.569: Pain in Unspecified Knee (and Why It Triggers Denials)
M25.569 is the ICD-10 code for pain in an unspecified knee. The code applies only when the chart does not specify the affected knee. Payers routinely flag M25.569 on imaging, injection, and PT claims because laterality is almost always inferable.
How Does ICD-10-CM Classify the M25.56x Family?
The M25.56x family sits inside the M25 block, which captures joint symptom codes for observable findings without naming an underlying disease. M25 codes apply when a symptom is the presenting complaint and no definitive diagnosis has been established yet. Referencing a detailed ICD 10 codes guide helps clinical teams map these initial presentations to their parent categories before downstream testing modifies the claim.
Is Knee Pain a Symptom Code or a Diagnosis Code in ICD-10?
Knee pain (M25.56x) is a symptom code, not a diagnosis code, in ICD-10-CM. The distinction matters because ICD-10-CM Section IV.G prohibits reporting a symptom code alongside an established diagnosis that the symptom integrally represents.
What Is the Difference Between Knee Pain and Knee Joint Pain in ICD-10?
Knee pain and knee joint pain are coded the same way in ICD-10-CM. Both phrases route to M25.56x in the Alphabetic Index. The clinical wording in the note does not change the code assignment.
When Should You Code Knee Pain (M25.56x) vs. the Underlying Diagnosis?
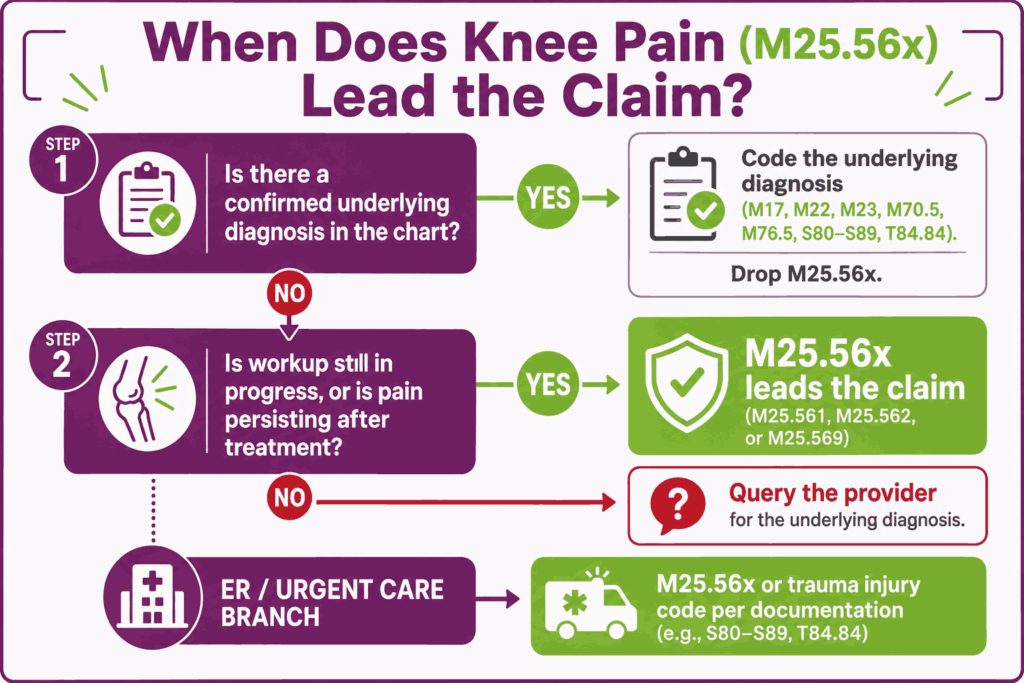
The decision to code knee pain (M25.56x) or the underlying diagnosis depends on the workup stage. ICD-10-CM Section IV.G is explicit: when an underlying diagnosis is established, that diagnosis takes primary, and the symptom does not also code unless it is clinically significant beyond what the diagnosis captures.
What Does ICD-10-CM Section IV.G Say About Symptom Coding?
ICD-10-CM Section IV.G states that codes for symptoms, signs, and abnormal findings are acceptable as primary diagnoses when no related definitive diagnosis has been established. Once a definitive diagnosis is confirmed, that diagnosis replaces the symptom code as primary.
When Is M25.56x the Correct Primary Diagnosis?
M25.56x is the correct primary diagnosis in three scenarios: symptom-only encounters, workup-in-progress encounters, and persistence after the underlying condition is resolved.
Initial Visits and Workup-in-Progress
Initial visits and workup-in-progress encounters are the most common scenarios for M25.56x as primary. The patient presents with knee pain, the provider has not yet confirmed a diagnosis, and the encounter focuses on history, exam, and ordering tests.
ER and Urgent-Care Encounters
ER and urgent-care encounters frequently use M25.56x as primary when the patient presents with acute knee pain and the workup is limited. If trauma is documented and a specific injury code from S80 through S89 applies, the injury code takes primary instead.
Pain Persisting After the Underlying Condition Is Resolved
M25.56x applies as primary when knee pain persists after the underlying condition is resolved. An example is residual pain after meniscus repair when the original tear is healed. The chart must document the persistence and the resolved status of the original diagnosis.
When Should the Underlying Diagnosis Be Coded Primary Instead?
The underlying diagnosis takes primary whenever the chart confirms a specific knee condition that the presenting pain integrally represents. M25.56x is then either omitted or sequenced secondary if clinically meaningful beyond the primary code.
Confirmed Osteoarthritis (Use M17.x)
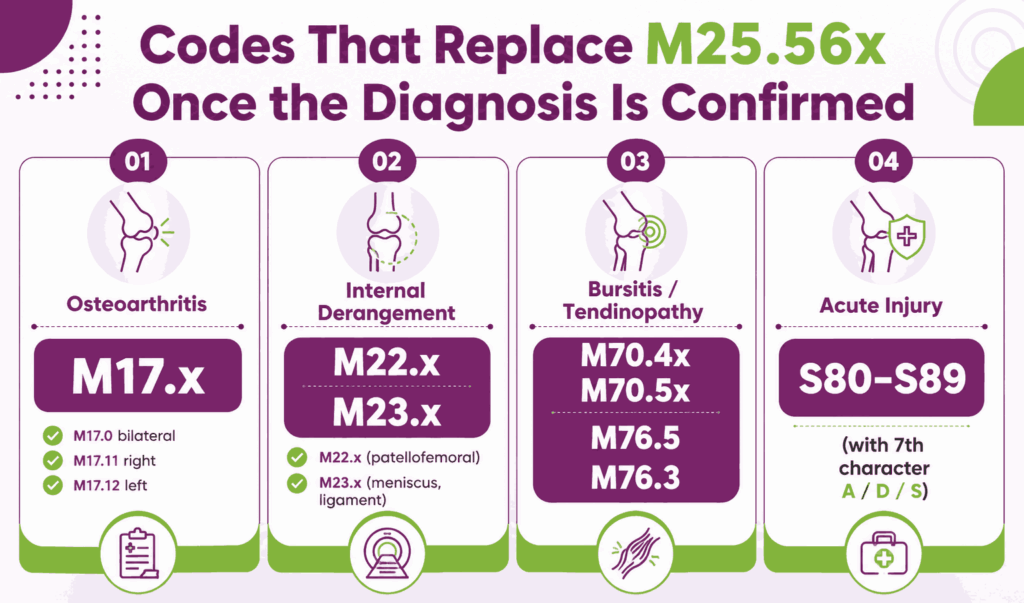
Confirmed osteoarthritis of the knee uses an M17 code as primary. M17.0 covers bilateral primary, M17.11 covers right primary, and M17.12 covers left primary. M25.56x does not appear on the claim because OA pain is integral to the OA diagnosis.
Confirmed Internal Derangement (Use M22.x or M23.x)
Confirmed patellofemoral disorders use M22 codes. Confirmed meniscus tears, ligament disruptions, or other internal derangements use M23 codes. The internal derangement code takes primary, and M25.56x is omitted.
Confirmed Bursitis or Tendinopathy (Use M70.5 or M76.5)
Confirmed prepatellar or other knee bursitis uses M70.4x or M70.5x. Confirmed patellar tendinitis uses M76.5. Iliotibial band syndrome uses M76.3. The specific soft-tissue diagnosis takes primary on the claim.
Acute Injury With a Confirmed Diagnosis (Use S80–S89)
Acute knee injury with a confirmed diagnosis uses an S80 through S89 code as primary. Sprains and strains code to S83.4x through S83.6x. Contusions code to S80.0x. Fractures code to S82.0x or S72.4x. The injury code takes primary, with M25.56x typically omitted.
How Do You Sequence Knee Pain With an Underlying Diagnosis?
Sequencing knee pain with an underlying diagnosis follows three rules. Sequence the definitive diagnosis first when established. Omit M25.56x unless the pain is clinically significant beyond what the primary diagnosis captures. Sequence G89 pain qualifier codes second when chronicity, trauma origin, or post-procedural status meaningfully affects management.
What Are the Other ICD-10 Codes Related to Knee Pain?
Knee pain coding extends beyond M25.56x because most knee pain in the US healthcare system has a documented underlying cause. The categories below cover the essential ICD 10 codes for Orthopedic billing that most often replace M25.56x as the primary diagnosis once the workup completes.
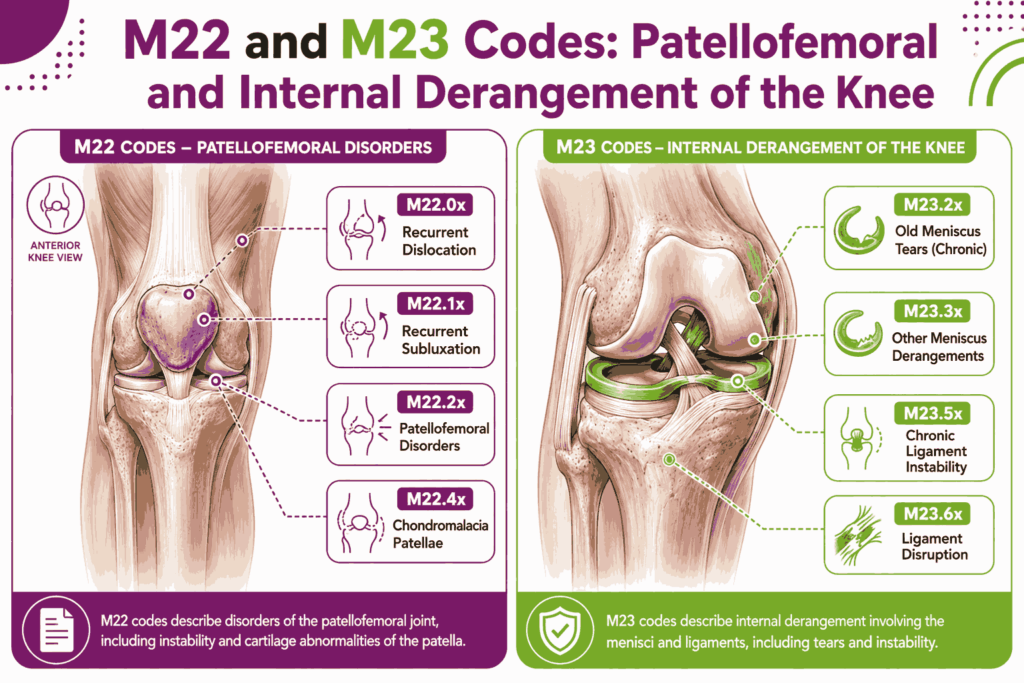
What Are the Codes for Patellofemoral and Internal Derangement Causes? (M22 and M23)
M22 captures disorders of the patella. M23 captures internal derangement of the knee, including meniscus tears, ligament disruptions, and cruciate ligament disorders.
Patellofemoral Disorders (M22.0–M22.9)
Patellofemoral disorders code under M22. M22.0x covers recurrent patellar dislocation. M22.1x covers recurrent patellar subluxation. M22.2x covers patellofemoral disorders such as malalignment. M22.4x covers chondromalacia patellae. Anterior knee pain often maps to M22 codes once the patellofemoral source is confirmed.
Meniscus Tears and Derangements (M23.20x–M23.30x)
Meniscus tears and derangements code under M23.20 through M23.30. Characters specify the meniscus involved (medial or lateral, anterior or posterior horn) and laterality. Old chronic meniscus tears code under M23.2x. Other meniscus derangements code under M23.3x.
Cruciate and Collateral Ligament Disorders (M23.5x, M23.6x)
Chronic ligament instability of the knee codes under M23.5x. Other spontaneous disruption of ligament of the knee codes under M23.6x. The codes specify cruciate (anterior or posterior), collateral (medial or lateral), or unspecified ligament.
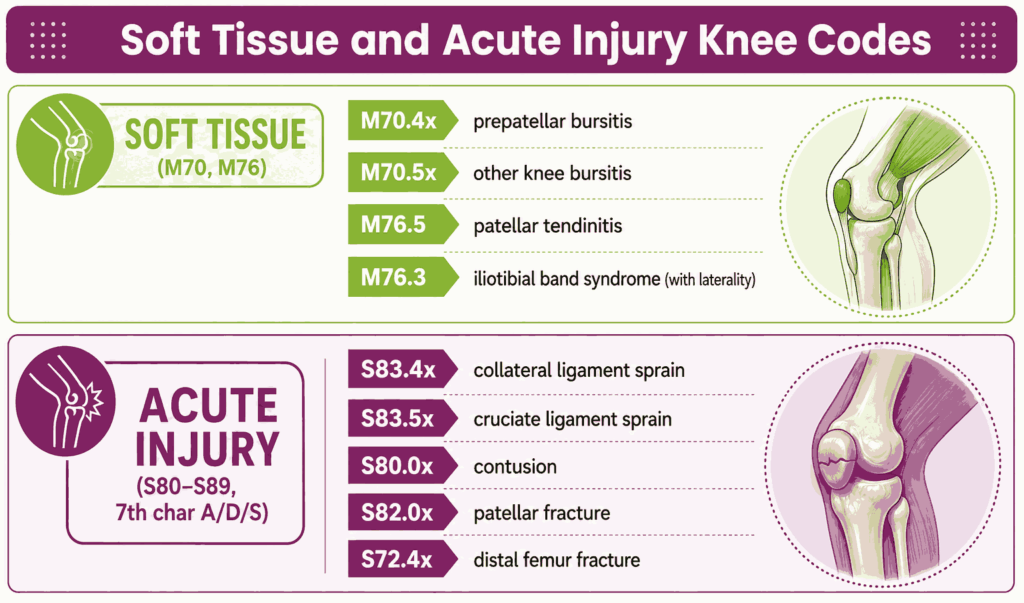
What Are the Codes for Bursitis and Tendinopathy of the Knee?
Bursitis and tendinopathy of the knee code under M70 and M76. These codes apply when soft-tissue inflammation is the documented cause of pain.
Prepatellar and Other Knee Bursitis (M70.4x, M70.5x)
Prepatellar bursitis codes under M70.4x. Other bursitis of the knee, including infrapatellar and other knee bursae, codes under M70.5x. Each carries laterality digits: 1 right, 2 left, 0 unspecified.
Patellar Tendinitis (M76.5)
Patellar tendinitis codes to M76.5. The code does not split by laterality at the parent level. The chart documents the affected side in the body of the note.
Iliotibial Band Syndrome (M76.3)
Iliotibial band syndrome codes to M76.3 with laterality. M76.31 covers the right side, M76.32 covers the left, and M76.30 covers unspecified.
What Are the Codes for Acute Knee Injuries? (S80–S89)
Acute knee injuries code under the S80 through S89 block, which covers injuries of the knee and lower leg. The codes require a 7th character for encounter type: A (initial), D (subsequent), or S (sequela).
Sprains and Strains (S83.4x–S83.6x)
Knee sprains and strains code under S83. S83.4x covers sprain of the collateral ligament. S83.5x covers sprain of the cruciate ligament. S83.6x covers sprain of the superior tibiofibular joint and ligament. The 6th character specifies structure; the 7th specifies encounter.
Contusions (S80.0x)
Knee contusions code under S80.0. S80.01xA covers right knee contusion, initial encounter. S80.02xA covers the left knee. S80.00xA covers an unspecified knee.
Fractures (S82.0x, S72.4x)
Patellar fractures code under S82.0. Distal femur fractures involving the knee region code under S72.4. Each carries laterality and 7th-character encounter detail.
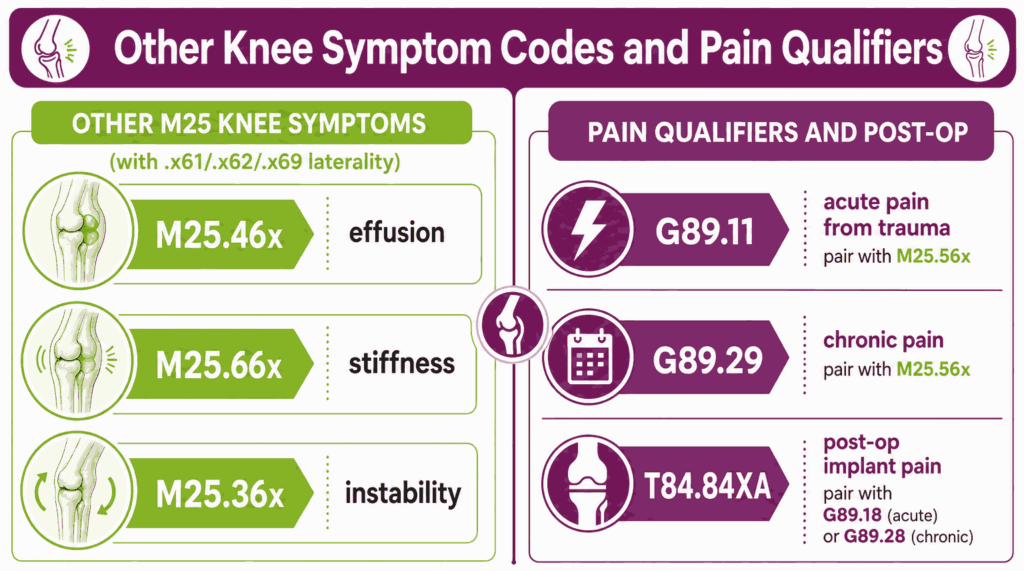
What Are the Codes for Other Knee Joint Symptoms?
Other knee joint symptoms outside of pain have their own M25 family codes. These symptoms appear alongside or instead of M25.56x, depending on what the patient reports and what the provider documents.
Knee Effusion (M25.46x)
Knee effusion codes to M25.46. M25.461 covers the right knee, M25.462 the left, and M25.469 an unspecified knee.
Knee Stiffness (M25.66x)
Knee stiffness not elsewhere classified codes to M25.66. M25.661 covers the right knee, M25.662 the left, and M25.669 an unspecified knee.
Knee Instability (M25.36x)
Other instability of the knee codes to M25.36. M25.361 covers the right knee, M25.362 the left, and M25.369 an unspecified knee. Ligament-related chronic instability codes to M23.5x instead.
What Are the Codes for Chronic and Post-Procedural Knee Pain?
Chronic and post-procedural knee pain require G89 pain qualifier codes paired with M25.56x or T84.84XA. Sequencing follows the ICD-10-CM Official Guidelines on pain coding.
Chronic Knee Pain (G89.29 Paired With M25.56x)
Chronic knee pain codes as G89.29 (other chronic pain) paired with M25.561, M25.562, or M25.569. G89.29 captures the chronicity; M25.56x captures the site and laterality. Sequence G89.29 first when the encounter focuses on chronic pain management.
Acute Pain From Trauma (G89.11 Paired With M25.56x)
Acute pain due to trauma codes as G89.11 paired with M25.56x and the relevant S80 through S89 injury code. G89.11 applies when the encounter focuses on trauma-related pain management.
Postprocedural Knee Pain (T84.84XA and G89.18)
Postprocedural pain after knee arthroplasty or other knee implant codes to T84.84XA, initial encounter, pain due to internal orthopedic prosthetic device. G89.18 (other acute postprocedural pain) pairs with T84.84XA when post-op pain is acute. G89.28 pairs when chronic. M25.56x does not apply to implant-related pain.
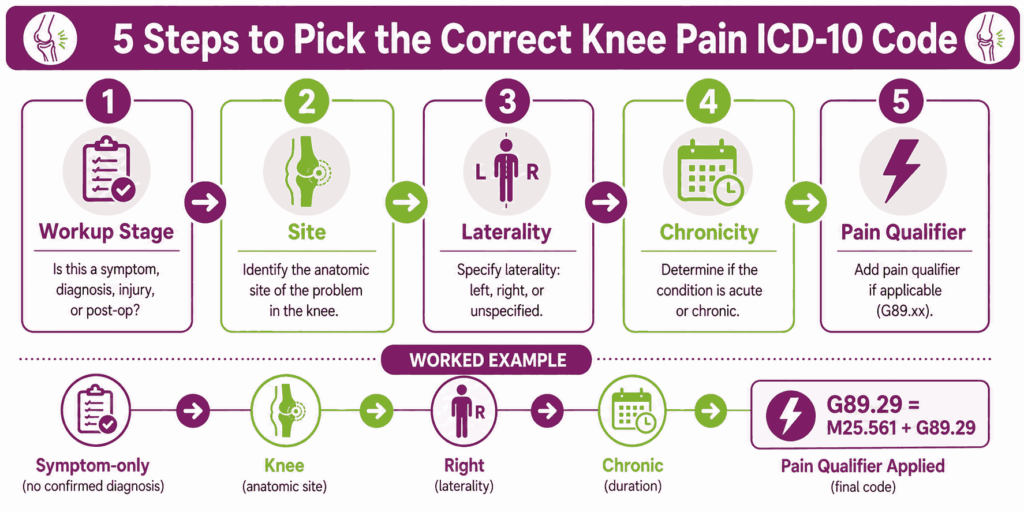
How Do You Choose the Correct Knee Pain ICD-10 Code?
Knee pain ICD-10 code selection follows a five-step decision logic. Each step narrows the code by one attribute: workup stage, site, laterality, chronicity, and pain qualifier.
What Is the Five-Step Decision Logic for Knee Pain Coding?
The five-step logic for knee pain coding works as follows.
- Identify the workup stage. Symptom-only, diagnosis-confirmed, or post-procedural. This determines whether M25.56x or the underlying diagnosis takes primary.
- Identify the site. Pain in the knee uses M25.56x. Pain elsewhere in the knee region (patellofemoral, meniscus, ligament, bursa, tendon) uses M22, M23, M70, or M76 codes.
- Identify laterality. Right (1), left (2), or unspecified (9). Laterality selects the final digit of M25.56x.
- Identify chronicity. Acute, chronic, or unspecified. Chronicity determines G89 pairing.
- Apply pain qualifiers. G89.11 for acute trauma pain, G89.29 for chronic non-trauma pain, G89.18 or G89.28 for post-procedural pain.
How Do You Determine Acute vs. Chronic Knee Pain for Coding?
The distinction between acute and chronic depends on duration and provider documentation. Acute knee pain is typically less than three months and often follows trauma or a recent procedure. Chronic knee pain persists three months or longer and may have no identifiable acute trigger.
How Is Pain Location Within the Knee Documented for Code Selection?
Pain location within the knee (anterior, medial, lateral, posterior) does not change the M25.56x code. M25.56x captures laterality but not intra-joint location. Anterior knee pain often supports a patellofemoral diagnosis (M22.2x or M22.4x) once worked up. Medial or lateral pain often supports meniscus or collateral ligament diagnoses (M23.x).
How Is Bilateral Knee Pain Coded in ICD-10?
Bilateral knee pain in ICD-10 is reported with both M25.561 (right) and M25.562 (left) on the same claim. ICD-10-CM does not provide a single bilateral code for knee pain. Coders sequence the two codes based on which side drove the encounter.
How Do Excludes1 and Excludes2 Notes Apply to M25.56x?
The Excludes1 note at M25 prohibits reporting an M25 code for joint pain that is integral to a more specific diagnosis already on the claim. The Excludes2 note allows reporting M25 codes alongside conditions that are not the same as M25 but may coexist clinically.
What Documentation Supports Knee Pain ICD-10 Claims?
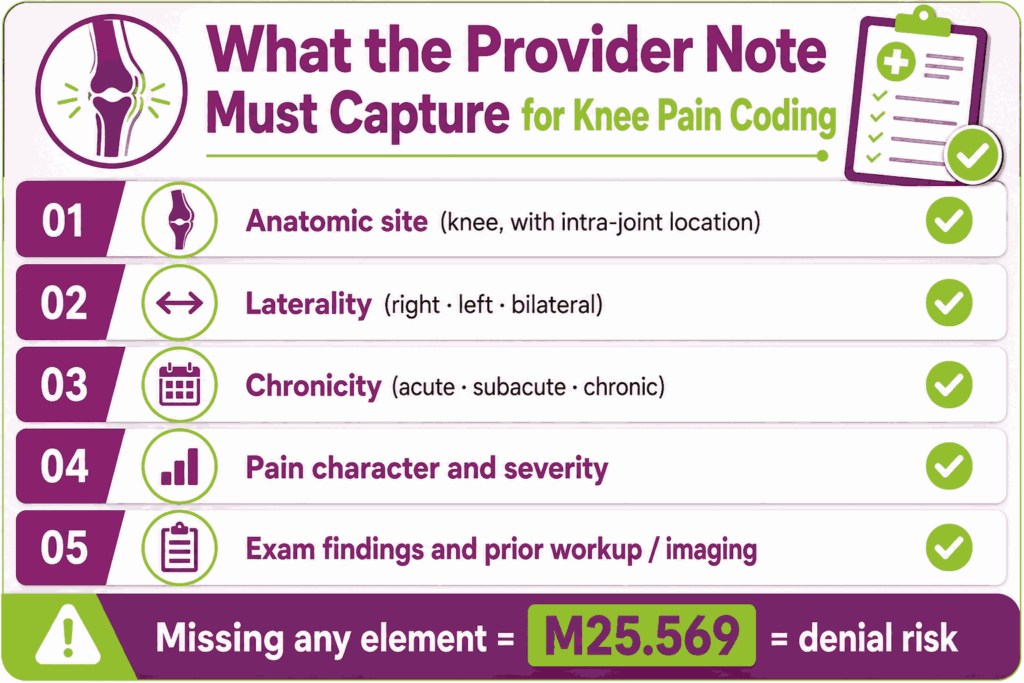
Documentation supports knee pain ICD-10 claims when the provider’s note captures workup stage, laterality, chronicity, pain character, and exam findings. ICD-10-CM Official Guidelines require complete documentation for accurate code assignment.
What Clinical Elements Must the Provider’s Note Contain?
The provider’s note for a knee pain encounter must capture five clinical elements that drive code selection.
- Anatomic site (knee, with location within the knee when documented)
- Laterality (right, left, or bilateral)
- Chronicity (acute, subacute, or chronic)
- Pain character and severity
- Exam findings and any prior imaging or workup
Why Is Laterality the Most-Cited Documentation Gap for Knee Pain?
Laterality is the most-cited gap because providers often write “knee pain” without specifying the side. Coders cannot infer laterality from context. Missing laterality forces the use of M25.569, which carries denial risk on imaging, injection, and PT claims.
How Should the Pain Site Within the Knee Be Documented?
Pain site within the knee (anterior, medial, lateral, posterior) is documented in the body of the note, even though M25.56x does not split by site. Site documentation drives downstream decisions about which underlying diagnosis (M22.x, M23.x, M70.5x, M76.5) becomes primary once the workup completes.
How Should Chronicity Be Documented?
Chronicity is documented with onset date, duration, and progression. Acute pain is documented as less than three months and often linked to trauma or a recent procedure. Chronic pain is documented as three months or longer with persistence despite treatment.
How Should Pain Character and Functional Impact Be Captured?
Pain character includes sharp, dull, aching, throbbing, and burning descriptors. Functional impact captures activities limited by the pain, such as walking, stair climbing, and weight bearing. These details support medical necessity for imaging, injections, and PT.
What Imaging and Exam Findings Should Be Captured?
Imaging findings include X-ray, MRI, ultrasound, or CT results. Key findings cover joint space, alignment, soft-tissue thickness, effusion, and bony pathology. Exam findings include range of motion, tenderness location, ligament stability tests, and effusion presence.
When Is a Provider Query Necessary for Knee Pain Coding?
A provider query is necessary when the chart documents knee pain without laterality, without chronicity, or with conflicting information about whether a diagnosis has been confirmed. Queries also apply when post-procedural pain is documented, but the relationship to the prior surgery is unclear.
Which CPT and HCPCS Codes Pair With Knee Pain ICD-10 Codes?
Knee pain ICD-10 codes pair with E&M, imaging, injection, physical therapy, and DME codes. Correct CPT-to-ICD-10 pairing supports medical necessity, especially for imaging claims where symptom-to-indication linkage is the most-audited element.
Which E&M Codes Are Billed With Knee Pain?
E&M codes 99202 through 99205 (new patient office) and 99211 through 99215 (established patient office) are most commonly billed with M25.56x. Emergency department codes 99281 through 99285 apply when knee pain presents to the ER. Chronic knee pain encounters often pair E&M with G89.29 as a secondary code.
Which Imaging Codes Pair With M25.56x?
Imaging codes pair with M25.56x when the encounter focuses on diagnostic workup. Payers require a documented symptom-to-indication link for each imaging order.
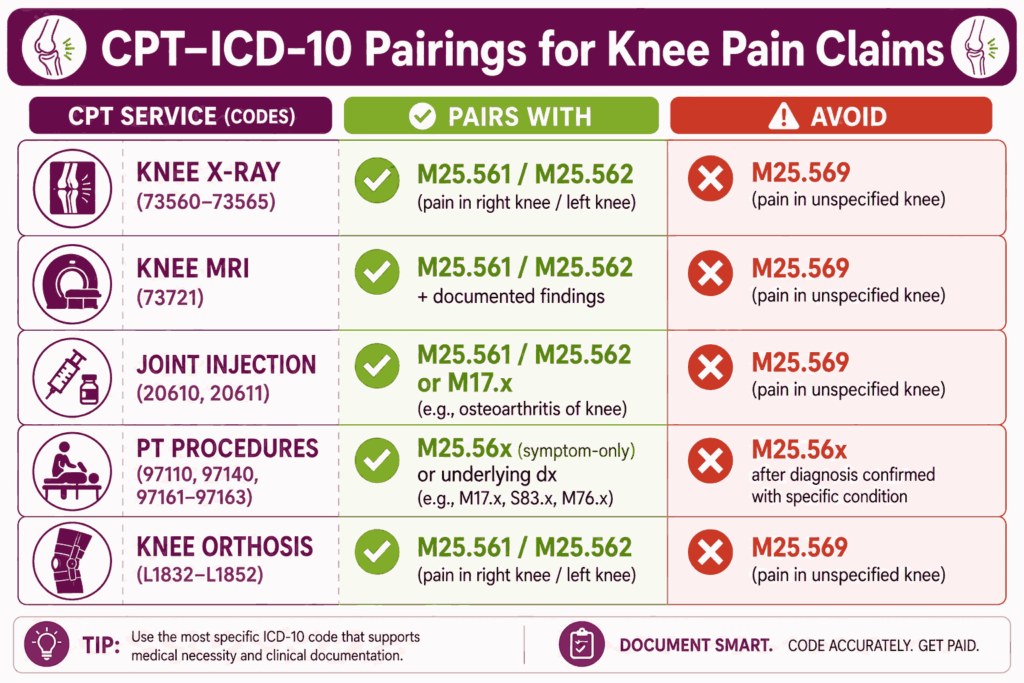
Knee X-Ray (CPT 73560, 73562, 73564, 73565)
Knee X-ray codes are 73560 (1 or 2 views), 73562 (3 views), 73564 (4 or more views), and 73565 (both knees, standing AP). Each pairs cleanly with laterality-specific M25.561 or M25.562.
Knee MRI Without Contrast (CPT 73721)
CPT 73721 covers MRI of any lower extremity joint without contrast. Knee MRI without contrast is the most common imaging code for knee pain workup when soft-tissue evaluation is needed. The order requires documented exam findings supporting MRI medical necessity.
Knee MRI With and Without Contrast (CPT 73722, 73723)
CPT 73722 covers MRI with contrast. CPT 73723 covers MRI without and with contrast. These codes apply when contrast is medically necessary, such as suspected tumor or postoperative evaluation. Most commercial payers require prior authorization for both codes.
Diagnostic Musculoskeletal Ultrasound (CPT 76881, 76882)
CPT 76881 covers complete musculoskeletal ultrasound of one joint. CPT 76882 covers limited ultrasound. Ultrasound is useful for effusion and soft-tissue evaluation in pain management and sports medicine workflows.
Which Procedural Codes Pair With Knee Pain?
Procedural codes for knee pain include joint aspiration, injection, and diagnostic arthroscopy. These pair with M25.56x when the procedure addresses the symptom, and a confirmed diagnosis has not yet replaced the symptom code.
Joint Injection (CPT 20610, 20611)
CPT 20610 covers major joint or bursa injection without imaging guidance. CPT 20611 adds ultrasound guidance. Both pair with M25.561 or M25.562 for diagnostic injection, or with an M17.x code when osteoarthritis is the confirmed underlying diagnosis.
Diagnostic Arthroscopy (CPT 29870)
CPT 29870 covers diagnostic knee arthroscopy. The procedure pairs with M25.56x when the indication is unexplained knee pain. Once arthroscopy confirms a diagnosis (meniscus tear, articular cartilage damage), the post-procedure documentation should code the confirmed diagnosis.
Which Physical Therapy Codes Pair With Knee Pain?
Physical therapy codes for knee pain include evaluation and therapeutic procedure codes. PT claims require a referring diagnosis that supports medical necessity for the therapy plan.
PT Evaluation Codes (97161, 97162, 97163)
CPT 97161 covers low-complexity PT evaluation. 97162 covers moderate complexity. 97163 covers high complexity. Re-evaluation uses 97164. The evaluation must document functional impact and a measurable treatment plan.
Therapeutic Procedures (97110, 97112, 97140, 97530)
CPT 97110 covers therapeutic exercises. 97112 covers neuromuscular reeducation. 97140 covers manual therapy. 97530 covers therapeutic activities. Each pairs with M25.56x or the relevant underlying knee diagnosis on the PT claim.
Which DME and HCPCS Codes Apply?
HCPCS L1832, L1843, L1845, L1851, and L1852 cover knee orthoses billed under DME. Coverage rules require documentation of conservative-care failure and a laterality-specific diagnosis. M25.569, paired with an L-code, triggers denial in most policies.
How Do You Avoid CPT–ICD-10 Mismatches for Knee Pain Claims?
Coders avoid CPT-ICD-10 mismatches by checking three points before submission. The diagnosis laterality matches the procedure or imaging laterality. The diagnosis chronicity matches the procedure indication. The workup stage matches the code chosen, with M25.56x for symptom-only encounters and the underlying diagnosis for confirmed conditions.
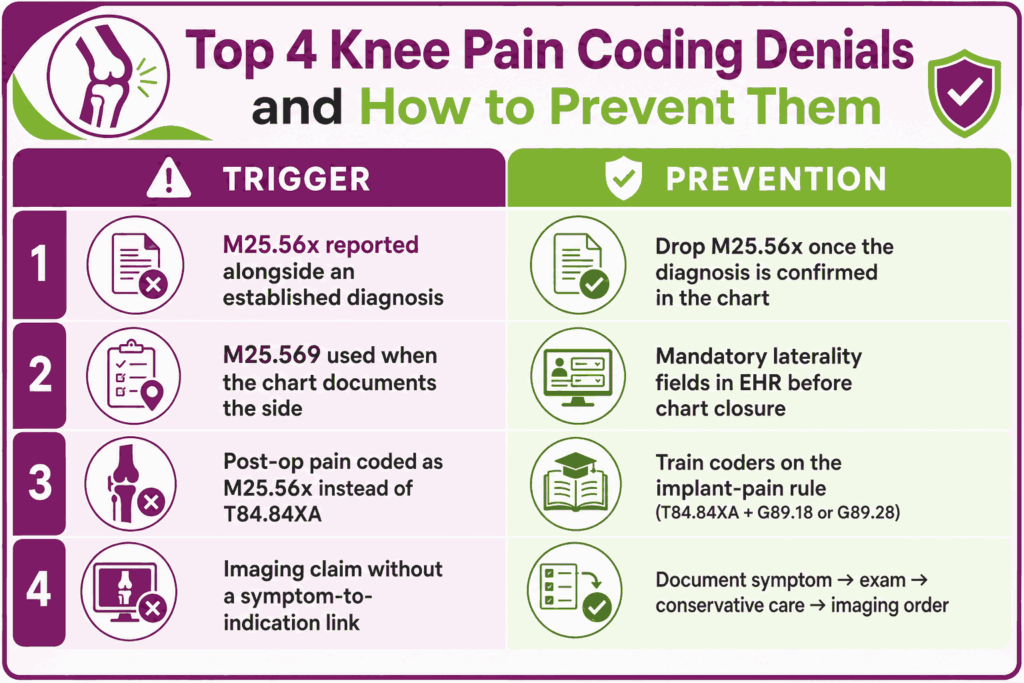
What Are the Most Common Knee Pain Coding Denials, and How Do You Prevent Them?
Knee pain coding denials come from symptom-versus-diagnosis errors, missing laterality, post-op miscoding, and CPT-ICD-10 mismatches. Each pattern has a known prevention path.
Why Are Knee Pain Claims Denied When a Diagnosis Is Already Established?
Knee pain claims are denied when M25.56x is reported alongside or in place of an established diagnosis. Payer edits flag M25.56x submitted with the same patient’s confirmed M17.x, M22.x, M23.x, or other underlying code from a prior or current encounter. Specialized orthopedic medical billing services prevent this oversight by deploying pre-submission tracking rules that systematically drop symptom codes the moment a definitive diagnosis enters the patient’s longitudinal record.
Why Does M25.569 (Unspecified Knee) Drive Denials?
M25.569 drives denials because nearly every clinical encounter that documents knee pain also documents the side. Payer edits flag M25.569 on claims for laterality-specific procedures such as knee X-ray RT, knee MRI LT, or 20610 RT. The fix is mandatory laterality fields in the EHR before chart closure.
How Does Missing Laterality Result in Rejection?
Missing laterality forces M25.569 use, which then triggers automated rejection on most laterality-aware procedure claims. A right knee X-ray (73560 RT) paired with M25.569 is rejected by most commercial payers and downcoded by Medicare contractors.
Why Are Post-Op Knee Pain Claims Denied When Coded as M25.56x?
Post-op knee pain coded as M25.56x is denied because the correct code is T84.84XA (pain due to internal orthopedic prosthetic device, initial encounter) when a knee implant is in place. G89.18 pairs with T84.84XA for acute post-procedural pain. G89.28 pairs for chronic post-procedural pain. M25.56x does not capture the device-related etiology.
How Does Missing the Acute/Chronic Distinction Cause Underpayment?
Missing the acute/chronic distinction causes underpayment because G89 pain qualifier codes affect E&M complexity and PT plan-of-care coverage. Chronic knee pain (G89.29 paired with M25.56x) supports higher-complexity E&M and longer PT durations. Acute pain without a G89 qualifier may be downcoded on E&M.
Why Are MRI and Imaging Claims Denied Without a Symptom-to-Indication Link?
MRI and imaging claims for knee pain are denied when the chart lacks a documented symptom-to-indication link. Payers require that the chart connect the symptom (M25.56x), the exam findings, the failed conservative care, and the imaging order in a clinical sequence. A missing element breaks the medical-necessity chain.
To resolve this, top billing companies for orthopedic practices provide documentation blueprints and clinical intake checklists that force the validation of these required medical links prior to advanced imaging orders.
What Are the Payer-Specific Rules for Knee Pain Coding?
Payer rules for knee pain coding vary by program and procedure. The table below summarizes the most common requirements.
| Payer | Common Rule |
|---|---|
| Medicare | LCDs require laterality-specific diagnosis for knee X-ray, MRI, and injection claims |
| BCBS plans | MRI prior authorization required in most states; pain duration and conservative-care trial documented |
| UnitedHealthcare | Prior authorization for MRI and advanced imaging; tier-1 imaging required before MRI in most cases |
| Aetna | Step therapy before MRI for non-traumatic knee pain in many policies |
| Medicare Advantage | HCC capture weakened when M25.569 is used in chronic-care risk panels |
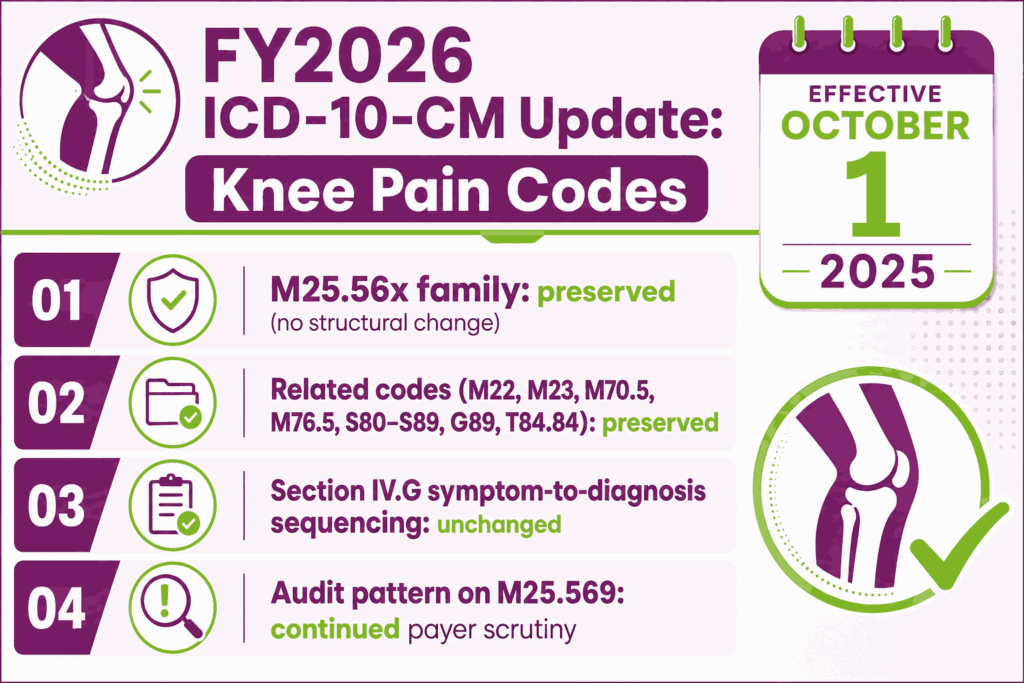
What Changed in the FY2026 ICD-10-CM Update for Knee Pain Codes?
The FY2026 ICD-10-CM update took effect October 1, 2025. The M25.56x family and related knee pain codes carried no structural changes. NCHS and CMS publish the addenda each summer before the October 1 effective date.
Were Any M25.56x or Related Codes Added, Revised, or Deleted Effective October 1, 2025?
The FY2026 update preserved the M25.56x, M22, M23, M70.5, M76.5, S80 through S89, G89, and T84.84 codes used for knee pain coding. Practices verify against the CMS-published FY2026 code set and the ICD-10-CM Official Guidelines for Coding and Reporting.
How Do FY2026 Changes Affect Symptom-to-Diagnosis Sequencing?
Symptom-to-diagnosis sequencing rules under ICD-10-CM Section IV.G are unchanged in FY2026. Coders continue to drop M25.56x once a definitive diagnosis is established and continue to pair G89 pain qualifiers when chronicity or trauma origin is documented.
What Audit Exposures Does FY2026 Create for M25.569 Use?
Audit exposure on M25.569 continues at the same pattern. Payers analyze provider claims data and flag practices that exceed peer benchmarks for unspecified-side knee pain coding.
Frequently Asked Questions About Knee Pain ICD-10 Coding
What Is the ICD-10 Code for Knee Pain?
The ICD-10 code for knee pain is M25.56, with M25.561 for the right knee, M25.562 for the left knee, and M25.569 for an unspecified knee. M25.56x applies when knee pain is the presenting symptom, and no confirmed underlying diagnosis exists, or when pain persists after the underlying condition is resolved.
What Is the ICD-10 Code for Right Knee Pain?
M25.561 is the ICD-10 code for pain in the right knee. The chart must document the right side. M25.561 applies when no underlying knee diagnosis has been confirmed for the right knee.
What Is the ICD-10 Code for Left Knee Pain?
M25.562 is the ICD-10 code for pain in the left knee. The chart must document the left side. M25.562 applies under the same symptom-only rules as M25.561.
What Is the ICD-10 Code for Bilateral Knee Pain?
Bilateral knee pain is coded with both M25.561 and M25.562 on the same claim. ICD-10-CM does not provide a single bilateral knee pain code. Coders sequence the two codes based on which side drove the encounter.
What Is the ICD-10 Code for Chronic Knee Pain?
Chronic knee pain is coded as G89.29 (other chronic pain) paired with M25.561, M25.562, or M25.569 for site and laterality. Sequence G89.29 first when the encounter focuses on chronic pain management.
What Is the ICD-10 Code for Post-Operative Knee Pain?
Post-operative knee pain is coded as T84.84XA (pain due to internal orthopedic prosthetic device, initial encounter) when a knee implant is in place. G89.18 pairs for acute post-procedural pain. G89.28 pairs for chronic post-procedural pain. M25.56x does not apply.
Is M25.569 the Same as M25.561 and M25.562?
M25.569 is not interchangeable with M25.561 or M25.562. M25.569 applies only when the chart does not document which knee is affected. Coders query the provider before defaulting to M25.569.
What Is the ICD-10 Code for Anterior Knee Pain?
Anterior knee pain has no dedicated ICD-10 code at the symptom level. M25.561 or M25.562 applies for the pain itself. When the patellofemoral source is confirmed, M22.2x (patellofemoral disorders) or M22.4x (chondromalacia patellae) takes primary.
Can M25.56x Be the Primary Diagnosis on an MRI Order?
M25.56x can be the primary diagnosis on a knee MRI order when no underlying diagnosis has been confirmed and the chart documents exam findings supporting MRI medical necessity. Most payers require documented conservative care (PT, NSAIDs, prior X-ray) before approving MRI for symptom-only knee pain.






