")
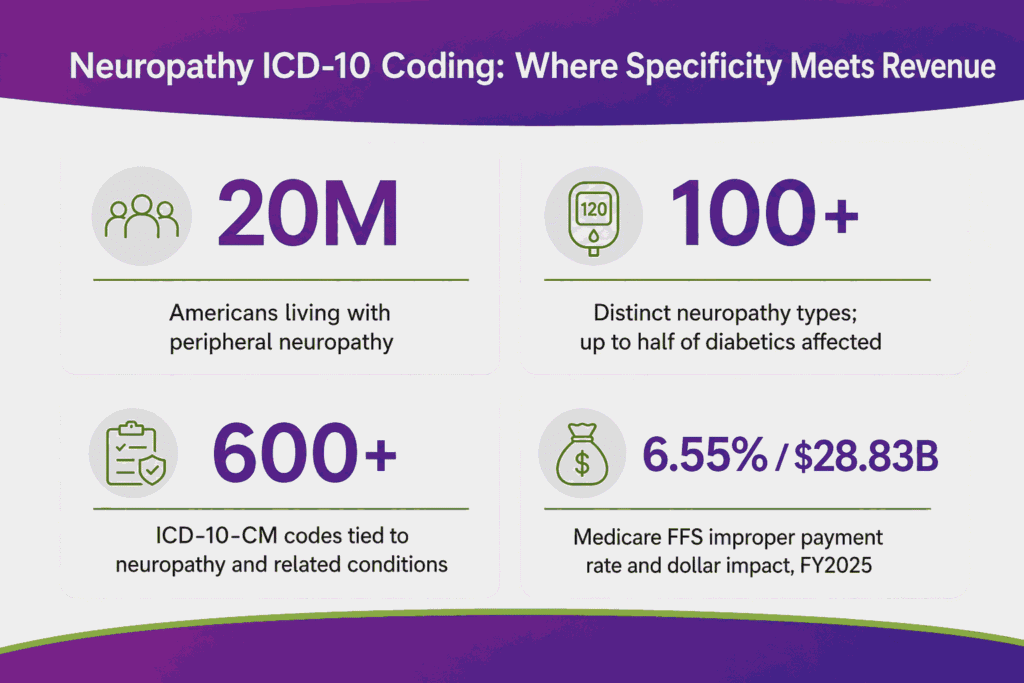
Neuropathy is damage or disease affecting the peripheral nerves. These nerves carry signals between the brain, the spinal cord, and the rest of the body. Nerve damage produces pain, numbness, tingling, and muscle weakness. An estimated 20 million people in the United States live with some form of peripheral neuropathy, and more than 100 distinct types exist. Up to one-half of people with diabetes develop peripheral neuropathy, which makes diabetes the most common cause.
That clinical volume creates billing exposure. ICD-10-CM contains more than 600 codes tied to neuropathy and related conditions. The correct code depends on the type, the cause, and the affected nerves. Coders also document laterality whenever a code requires it. The margin for error is thin: CMS reported a Medicare fee-for-service improper payment rate of 6.55% in FY 2025, accounting for $28.83 billion.
Most neuropathy codes fall within the G60 to G65 range of ICD-10-CM. Diabetic forms use combination codes drawn from E08 through E13. Pain-led presentations without a known cause often map to M79.2. This guide covers the full neuropathy code set, diabetic coding rules, documentation requirements, and denial prevention.
What Is the ICD-10 Code for Neuropathy?
The ICD-10 code for neuropathy is G62.9, Polyneuropathy, unspecified, when no type or cause is documented. The hereditary or idiopathic default is G60.9. The single correct code always depends on what the clinical note specifies.
Coders reach for an unspecified code only when documentation gives no further detail. A specific code carries a higher reimbursement rate and a lower denial risk. The table below shows the default code for each common scenario.
| Scenario | ICD-10 Code | Descriptor |
|---|---|---|
| General neuropathy, cause unknown | G62.9 | Polyneuropathy, unspecified |
| Peripheral neuropathy, no cause stated | G62.9 | Polyneuropathy, unspecified |
| Hereditary or idiopathic neuropathy | G60.9 | Hereditary and idiopathic neuropathy, unspecified |
| Diabetic neuropathy, type 2 | E11.40 | Type 2 diabetes mellitus with diabetic neuropathy, unspecified |
| Neuropathic pain, no cause | M79.2 | Neuralgia and neuritis, unspecified |
| Autonomic neuropathy, idiopathic | G90.09 | Other idiopathic peripheral autonomic neuropathy |
The most commonly used ICD-10 code for neuropathy unspecified is G62.9. Payers accept G62.9 as billable, yet they scrutinize repeated use. A documented type or cause moves the claim toward faster payment.
How ICD-10 Neuropathy Codes Are Structured
ICD-10 codes for neuropathy follow a chapter, block, and digit pattern. The letter signals the body system. The digits add the type, site, and cause. Reading G62.9 in pieces makes the logic clear.
- G marks Chapter 6, Diseases of the Nervous System.
- G60 to G65 is the block for polyneuropathies and peripheral nerve disorders.
- 62 identifies other and unspecified polyneuropathies.
- .9 signals “unspecified,” the lowest-detail option in the family.
Four code families hold the codes you assign most. Each family answers a different clinical question about the neuropathy. The table below maps the families to their purpose.
| Code Family | Range | What It Covers |
|---|---|---|
| Hereditary and idiopathic | G60.0 to G60.9 | Genetic and unknown-origin neuropathy |
| Inflammatory polyneuropathy | G61.0 to G61.9 | Guillain-Barré, CIDP, autoimmune forms |
| Other polyneuropathies | G62.0 to G62.9 | Drug, alcohol, toxin, and unspecified types |
| Diabetic neuropathy | E08 to E13 | Combination codes for diabetes with nerve damage |
Why Code Specificity Drives Reimbursement
Payers tie reimbursement to documented medical necessity. A specific code proves the provider identified the cause and the affected nerves. An unspecified code leaves the payer guessing and results in a denial.
G62.9 groups into MS-DRG 073 and 074 for cranial and peripheral nerve disorders. The more specific the code, the cleaner the link between diagnosis and treatment. Specificity also supports prior authorization for nerve studies and high-cost drugs.
Complete List of Neuropathy ICD-10 Codes by Type
Neuropathy codes break into clear clinical categories. Each category answers what kind of neuropathy the patient has. The sections below list every code a coder assigns in daily practice.
Hereditary and Idiopathic Neuropathy (G60)
The G60 group covers neuropathy with a genetic or unknown origin. Coders use these codes when no diabetes or toxin link exists. The ICD-10 code for idiopathic peripheral neuropathy falls under this category.
| Code | Descriptor | Example Condition |
|---|---|---|
| G60.0 | Hereditary motor and sensory neuropathy | Charcot-Marie-Tooth disease |
| G60.1 | Refsum’s disease | Lipid metabolism disorder |
| G60.2 | Neuropathy with hereditary ataxia | Friedreich’s ataxia |
| G60.3 | Idiopathic progressive neuropathy | Progressive nerve damage, unknown cause |
| G60.8 | Other hereditary and idiopathic neuropathies | Small fiber, sensory variants |
| G60.9 | Hereditary and idiopathic neuropathy, unspecified | Genetic or unknown origin, no detail |
G60.8 absorbs several searched terms. Small fiber neuropathy, sensory neuropathy, and some sensorimotor forms map here when hereditary or idiopathic. The next section covers the small fiber nuance in detail.
Inflammatory Polyneuropathy (G61)
The G61 group covers autoimmune and inflammatory nerve disease. These codes signal an active immune process attacking the nerves. Documentation should name the specific syndrome.
| Code | Descriptor |
|---|---|
| G61.0 | Guillain-Barré syndrome |
| G61.1 | Serum neuropathy |
| G61.81 | Chronic inflammatory demyelinating polyneuritis (CIDP) |
| G61.82 | Multifocal motor neuropathy (MMN) |
| G61.89 | Other inflammatory polyneuropathies |
| G61.9 | Inflammatory polyneuropathy, unspecified |
Other and Toxic Polyneuropathies (G62)
The G62 group holds drug, alcohol, toxin, and unspecified types. This family carries the highest daily volume for most coders. It also contains the unspecified default, G62.9.
| Code | Descriptor | Common Trigger |
|---|---|---|
| G62.0 | Drug-induced polyneuropathy | Chemotherapy, isoniazid, other drugs |
| G62.1 | Alcoholic polyneuropathy | Chronic alcohol use |
| G62.2 | Polyneuropathy due to other toxic agents | Lead, solvents, heavy metals |
| G62.81 | Critical illness polyneuropathy | ICU and sepsis-related |
| G62.82 | Radiation-induced polyneuropathy | Radiation therapy exposure |
| G62.89 | Other specified polyneuropathies | Documented type without a unique code |
| G62.9 | Polyneuropathy, unspecified | No type or cause documented |
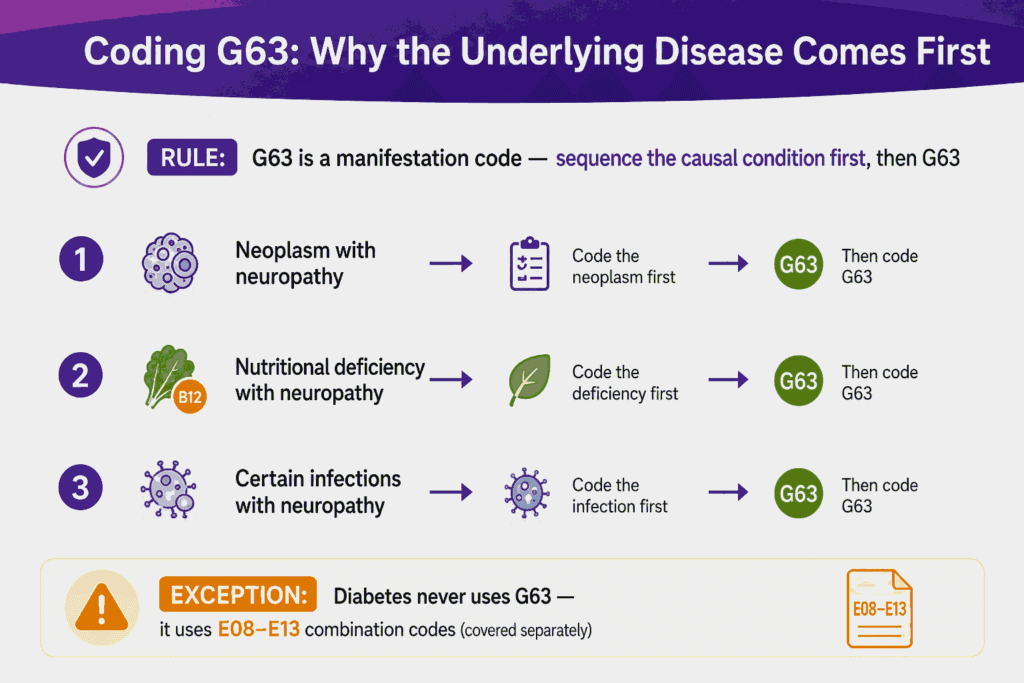
Polyneuropathy in Diseases Classified Elsewhere (G63)
G63 is a manifestation code. It reports neuropathy caused by a separate, named disease. The underlying disease gets coded first, then G63.
The “code first” note matters here. Coders sequence the causal condition ahead of G63. Common causes include neoplasm, nutritional deficiency, and certain infections. Diabetes is the major exception, covered in its own section below.
Small Fiber, Sensory, Axonal, and Sensorimotor Neuropathy Codes
ICD-10-CM has no unique code for small fiber neuropathy. Coders map it based on the documented cause. The same rule applies to sensory, axonal, and sensorimotor patterns.
These descriptors describe a nerve damage pattern, not a distinct diagnosis. The code follows the cause first, then the pattern. The table shows how to assign each searched term.
| Documented Type | Most Common Code | Coding Note |
|---|---|---|
| Small fiber neuropathy | G60.8 or G90.09 | G62.9 if idiopathic and unspecified |
| Sensory peripheral neuropathy | G60.8 or G62.9 | Use cause-specific code when known |
| Axonal sensorimotor neuropathy | G62.9 or G60.8 | Pattern only, code the cause first |
| Severe peripheral neuropathy | G62.9 or cause code | Severity does not change the ICD-10 code |
| Chronic peripheral neuropathy | G62.9 | “Chronic” alone adds no code specificity |
A common error assigns a small fiber code as if it were unique. No such code exists in ICD-10-CM. The note must state the cause to support a specific code.
Severity terms follow the same rule. The ICD-10 code for severe neuropathy still resolves through type and cause. Words like severe, chronic, or progressive describe the condition without changing the code.
Diabetic Neuropathy ICD-10 Codes (E08 to E13)
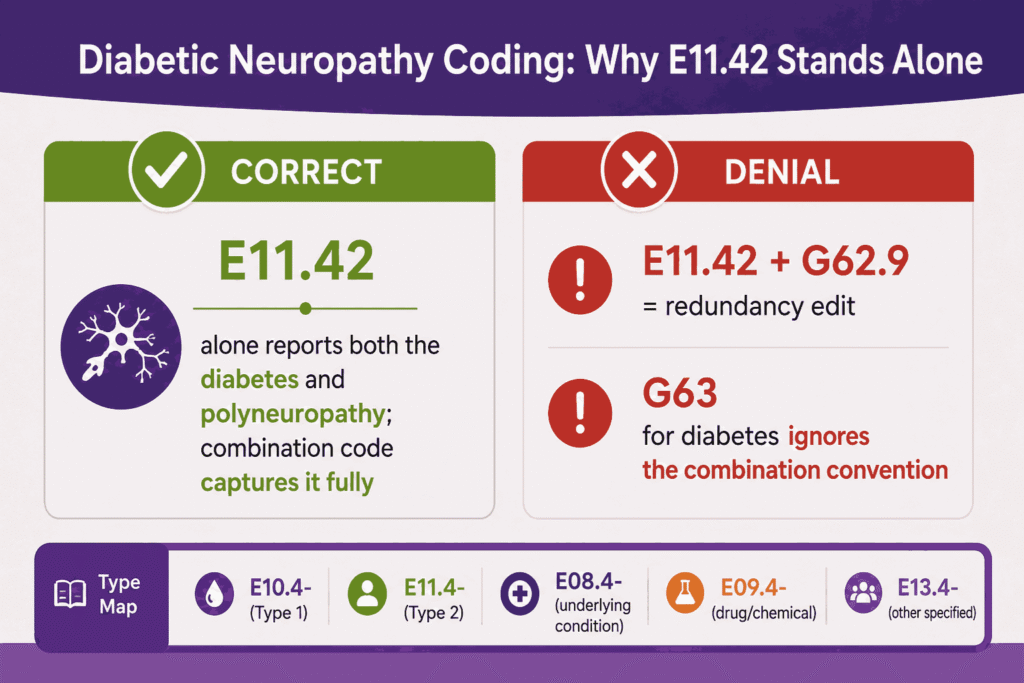
The ICD-10 code for diabetic neuropathy uses a combination code, not a G-code. A single E-series code reports both the diabetes and the nerve damage. The ICD-10 code for diabetic neuropathy most often resolves to E11.40 or E11.42.
This combination rule is the most missed point in neuropathy coding. Coders should not add G62.9 alongside a diabetic neuropathy code. The combination code already captures the polyneuropathy. The table lists the type 2 set.
| Code | Descriptor |
|---|---|
| E11.40 | Type 2 diabetes with diabetic neuropathy, unspecified |
| E11.41 | Type 2 diabetes with diabetic mononeuropathy |
| E11.42 | Type 2 diabetes with diabetic polyneuropathy |
| E11.43 | Type 2 diabetes with diabetic autonomic (poly)neuropathy |
| E11.44 | Type 2 diabetes with diabetic amyotrophy |
Type 1, Drug-Induced, and Other Diabetes Forms
The diabetes type changes the first three characters of the code. Type 1 uses the E10 family. Drug-induced and secondary diabetes use E08, E09, and E13.
| Diabetes Type | Code Family | Example |
|---|---|---|
| Type 1 diabetes | E10.4- | E10.42 with diabetic polyneuropathy |
| Type 2 diabetes | E11.4- | E11.42 with diabetic polyneuropathy |
| Due to underlying condition | E08.4- | E08.42 with polyneuropathy |
| Drug or chemical induced | E09.4- | E09.42 with polyneuropathy |
| Other specified diabetes | E13.4- | E13.42 with polyneuropathy |
The ICD-10 code for type 2 diabetes with peripheral neuropathy maps to E11.42 in most charts. The ICD-10 code for diabetic autonomic neuropathy maps to E11.43. Each variant searched, including dm with neuropathy and t2dm with neuropathy, resolves inside the E11.4- set.
Sequencing Diabetes and Neuropathy Codes
The combination code removes the need for separate sequencing in most diabetic cases. The E11.4 code stands alone for the neuropathy. Coders add other codes only for unrelated conditions.
ICD-10-CM guidelines treat diabetes complications as a linked relationship. A note that says “diabetic neuropathy” supports the combination code directly. A note that says “diabetes” and “neuropathy” separately still allows the link under current guidance.
Diabetic Neuropathy vs G63: A Key Distinction
Diabetes neuropathy never uses G63 in ICD-10-CM. The E11.4 combination codes replace the manifestation pairing. This separates diabetes from every other systemic cause.
- Diabetes with neuropathy: Use the combination E08 to E13 code only.
- Neoplasm with neuropathy: Code the neoplasm first, then G63.
- Nutritional cause with neuropathy: Code the deficiency first, then G63.
Mixing these rules creates denials. A claim that pairs E11.42 with G62.9 risks rejection for redundant coding. A claim that uses G63 for diabetes ignores the combination convention.
Mononeuropathy Codes: Ulnar, Peroneal, and Nerve-Specific Sites
Mononeuropathy affects a single named nerve. These codes live in the G56 and G57 families, not G60 to G62. The ICD-10 code for ulnar neuropathy and ICD-10 code for peroneal neuropathy sit here.
Single-nerve codes require laterality. The final digit identifies the right side, the left side, or bilateral involvement. The table shows the structure for the two most searched nerves.
| Nerve | Base Code | Laterality Options |
|---|---|---|
| Ulnar nerve (upper limb) | G56.2- | .21 right, .22 left, .23 bilateral, .20 unspecified |
| Peroneal nerve (lower limb) | G57.3- | .31 right, .32 left, .33 bilateral, .30 unspecified |
A missing laterality digit triggers a coding edit. The ICD-10 code for right ulnar neuropathy is G56.21. The ICD-10 code for left peroneal neuropathy is G57.32. Each side-specific search maps to one exact code.
Upper Extremity, Cervical, and Hand Neuropathy Codes
Upper-limb neuropathy follows the same single-nerve logic as the leg. The G56 family covers named nerves in the arm and hand. The “ICD-10 code for upper extremity neuropathy” depends on the affected nerve.
Cervical neuropathy describes nerve involvement at the neck. Most cervical cases reflect radiculopathy, not peripheral polyneuropathy. The “ICD-10 code for cervical neuropathy” usually maps to M54.12, radiculopathy of the cervical region.
| Searched Term | Assigned Code | Reason |
|---|---|---|
| Upper extremity neuropathy | G56.9- | Mononeuropathy of upper limb, unspecified nerve |
| Right hand neuropathy | G56.91 | Single nerve, right upper limb |
| Left arm neuropathy | G56.92 | Single nerve, left upper limb |
| Cervical neuropathy | M54.12 | Cervical radiculopathy, not peripheral type |
A “neuropathy in hands” note with no named nerve maps to G62.9 when diffuse. A single named nerve, such as the median or ulnar, uses the G56 family with laterality. The cause and the nerve together set the final code.
What Causes Neuropathy and How Cause Affects Coding
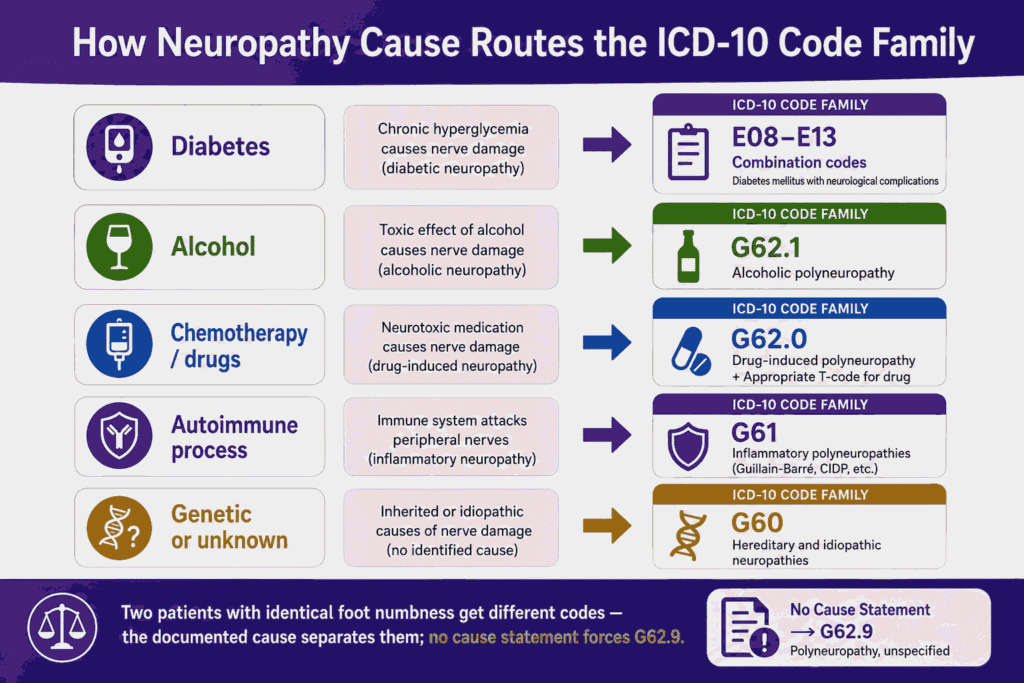
The cause of neuropathy drives the ICD-10 code more than the symptom does. Two patients with identical foot numbness receive different codes. The documented cause separates one code from the other.
Diabetes is the leading cause of peripheral neuropathy in the United States. Other causes include alcohol use, chemotherapy, autoimmune disease, and toxin exposure. Each cause routes to a different code family.
- Diabetes: E08 to E13 combination codes.
- Alcohol: G62.1, alcoholic polyneuropathy.
- Chemotherapy or drugs: G62.0 with a T-code.
- Autoimmune process: G61 inflammatory codes.
- Genetic or unknown: G60 hereditary and idiopathic codes.
A chart that names the cause supports a specific, billable code. A chart that omits the cause forces the unspecified G62.9. Coders read the full note for any cause statement before defaulting to unspecified.
The diagnostic workup also supports code selection. Nerve conduction studies, lab panels, and biopsy results confirm the type and cause. These results justify the specificity that payers expect on a clean claim.
Drug-Induced and Chemotherapy-Induced Neuropathy
Drug-induced neuropathy uses G62.0 as the base diagnosis. Chemotherapy-induced peripheral neuropathy (CIPN) also reports under G62.0. An external cause code names the responsible drug.
The “ICD-10 code for chemotherapy-induced neuropathy” pairs two codes. G62.0 reports the nerve damage. The T-code reports the drug as the cause. The table shows the pairing.
| Element | Code | Purpose |
|---|---|---|
| Nerve damage | G62.0 | Drug-induced polyneuropathy |
| Adverse effect of antineoplastic drug | T45.1X5- | Names chemotherapy as the cause |
| Encounter detail | 7th character A, D, or S | Initial, subsequent, or sequela |
The “ICD-10 code for chemotherapy-induced peripheral neuropathy” follows the same two-code logic. Oncology coders add the T45.1X5- code to document the drug link. The 7th character reflects the encounter type.
Alcoholic Neuropathy ICD-10 Code
The ICD-10 code for alcoholic neuropathy is G62.1, Alcoholic polyneuropathy. This code reports nerve damage from chronic alcohol use. Many payers expect a paired alcohol-use disorder code.
Documentation should state the alcohol link directly. The “ICD-10 code for alcohol induced neuropathy” maps to G62.1 as well. A paired F10.- code for alcohol use disorder supports medical necessity.
Autonomic and Optic Neuropathy Codes
Autonomic neuropathy affects involuntary functions such as heart rate and digestion. The idiopathic form uses G90.09. The diabetic form uses E11.43, as shown earlier.
Optic neuropathy affects the optic nerve and falls outside the G60 to G65 block. These codes sit in Chapter 7 for the eye. The table separates the two patterns.
| Type | Code | Descriptor |
|---|---|---|
| Idiopathic autonomic neuropathy | G90.09 | Other idiopathic peripheral autonomic neuropathy |
| Autonomic disorder, unspecified | G90.9 | Disorder of the autonomic nervous system, unspecified |
| Ischemic optic neuropathy | H47.01- | Reports laterality with final digit |
| Optic neuritis | H46.- | Inflammatory optic nerve involvement |
Neuropathy by Anatomical Site and Laterality
ICD-10-CM has no direct code for neuropathy of the feet or neuropathy of the lower extremities. Polyneuropathy codes do not carry a site digit. Coders assign G62.9 for these site-based searches when the cause is unknown.
Site language describes where the patient feels symptoms. The polyneuropathy code reflects the diffuse nature of the disease. The table maps the common site searches to their codes.
| Searched Term | Assigned Code | Reason |
|---|---|---|
| Neuropathy in feet | G62.9 | Polyneuropathy, no specific foot code |
| Neuropathy of lower extremities | G62.9 | Diffuse polyneuropathy pattern |
| Bilateral lower extremity neuropathy | G62.9 | No laterality digit on polyneuropathy |
| Right leg neuropathy | G57.91 or G62.9 | G57.91 for one nerve, G62.9 when diffuse |
| Left leg neuropathy | G57.92 or G62.9 | Single-nerve code carries the side digit |
| Right foot neuropathy | G57.91 or G62.9 | Mononeuropathy of right lower limb |
| Left foot neuropathy | G57.92 or G62.9 | Mononeuropathy of left lower limb |
| Single-nerve site (foot drop, peroneal) | G57.3- | Mononeuropathy carries laterality |
Laterality applies only to single-nerve mononeuropathy codes. Polyneuropathy is bilateral and symmetric by definition. A bilateral feet neuropathy note still maps to G62.9, not a paired laterality code.
The icd 10 code for diabetic neuropathy in feet follows the diabetic rule, not the site rule. The foot location does not change the combination code. E11.42 or E11.40 reports the condition regardless of where symptoms appear.
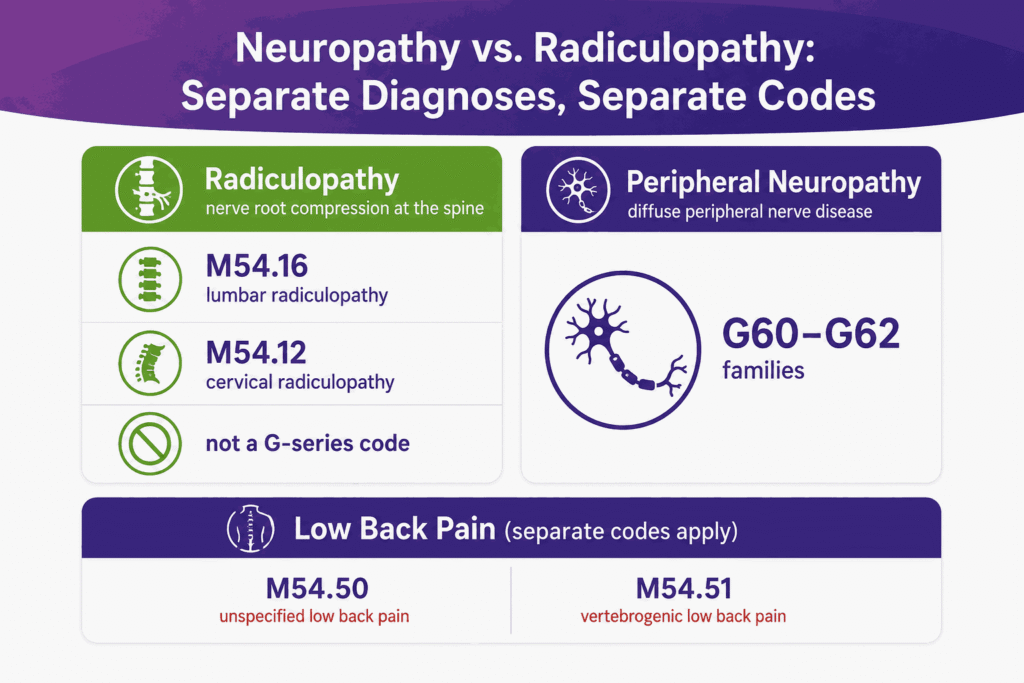
Neuropathy vs Radiculopathy: Low Back Pain Coding
Neuropathy and radiculopathy are separate diagnoses with separate codes. The ICD-10 code for low back pain with neuropathy often requires two codes. One reports the pain, the other the nerve root involvement.
Radiculopathy reflects nerve root compression at the spine. The “ICD-10 code for lumbar neuropathy usually maps to M54.16, lumbar radiculopathy. Low back pain alone uses the M54.5- series.
- M54.16: Radiculopathy, lumbar region.
- M54.50: Low back pain, unspecified.
- M54.51: Vertebrogenic low back pain.
A documented radiculopathy uses M54.16, not a G-series neuropathy code. Coders separate spinal nerve root pain from peripheral polyneuropathy. The distinction protects against incorrect code assignment.
History of Neuropathy Coding
A resolved neuropathy uses a personal history code. The “ICD-10 code for history of neuropathy maps to Z86.69. This code reports a past condition that no longer requires active treatment.
Active neuropathy never uses a history code. Z86.69 applies only when the condition has resolved. Coders assign an active G-series or E-series code while treatment continues.
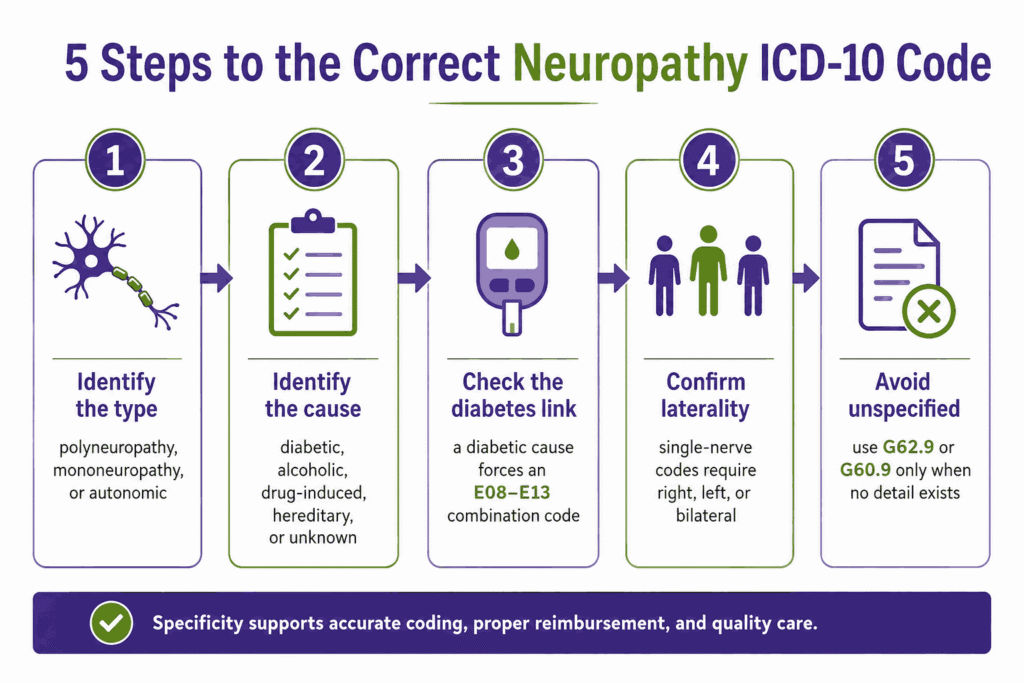
How to Choose the Right Neuropathy Code
Correct code selection follows a repeatable sequence. Each step narrows the choice from general to specific. This sequence prevents the unspecified-code overuse that drives denials.
- Identify the type. Polyneuropathy, mononeuropathy, or autonomic.
- Identify the cause. Diabetic, alcoholic, drug-induced, hereditary, or unknown.
- Check the diabetes link. A diabetic cause forces an E08 to E13 combination code.
- Confirm laterality. Single-nerve codes require right, left, or bilateral.
- Avoid unspecified codes. Use G62.9 or G60.9 only when no detail exists.
A code chosen through these steps matches the documentation. The match supports medical necessity and clean claim submission. Skipping a step usually produces an unspecified code and a slower payment.
Documentation Requirements for Neuropathy Coding
Every neuropathy code needs supporting documentation in the chart. The note must justify the type, the cause, and the laterality. Missing elements force a less specific code or a denial.
The documentation rules differ by code tier. Specific codes demand more detail than unspecified codes. The table connects each code element to its required note content.
| Code Element | Required Documentation | Common Denial Reason |
|---|---|---|
| Type of neuropathy | Polyneuropathy, mononeuropathy, autonomic | Type not stated, defaults to G62.9 |
| Cause or etiology | Diabetes, alcohol, drug, hereditary | No cause link, lower specificity |
| Laterality | Right, left, or bilateral nerve | Missing side on mononeuropathy code |
| Diabetes relationship | Stated diabetic neuropathy link | Separate codes risk redundancy edit |
Strong documentation names the cause and the affected nerves. It also records test results such as nerve conduction studies. These details move a claim from an unspecified code to a billable, specific one.
CPT Codes for Neuropathy Testing and Treatment
ICD-10 codes report the diagnosis. CPT codes report the services performed to diagnose and treat the neuropathy. A clean claim pairs the right diagnosis code with the right procedure code.
Neuropathy claims center on a small set of diagnostic CPT codes. Electrodiagnostic testing, autonomic testing, and skin biopsy confirm the type and cause. The table below maps the core procedure families.
| Service | CPT Range | Purpose |
|---|---|---|
| Office visits (E/M) | 99202 to 99215 | Evaluation, history, and exam |
| Nerve conduction studies | 95907 to 95913 | Large fiber nerve function |
| Needle EMG | 95860 to 95887 | Muscle and motor unit activity |
| Autonomic function testing | 95921 to 95924 | Parasympathetic and sympathetic function |
| Skin punch biopsy | 11104, 88356 | Small fiber nerve density |
| Peripheral nerve injection | 64450, 64640 | Pain block or nerve destruction |
Nerve Conduction Study CPT Codes (95907 to 95913)
Nerve conduction study codes are selected by the total number of studies performed. A single study is one sensory test, one motor test with or without F wave, or one H-reflex. Each named nerve counts once per study type, regardless of the sites stimulated.
| CPT Code | Number of Studies |
|---|---|
| 95907 | 1 to 2 |
| 95908 | 3 to 4 |
| 95909 | 5 to 6 |
| 95910 | 7 to 8 |
| 95911 | 9 to 10 |
| 95912 | 11 to 12 |
| 95913 | 13 or more |
Coders report one unit of the single code that matches the total count. Billing two NCS codes on the same encounter triggers an edit. The note must list every nerve and study type tested.
EMG CPT Codes (95860 to 95887)
The EMG code set splits on one question: were nerve conduction studies done the same day? Standalone EMG uses 95860 to 95864, selected by the number of extremities. Same-day EMG with NCS uses the add-on codes 95885 to 95887.
- 95860 to 95864: Needle EMG of 1, 2, 3, or 4 extremities, no same-day NCS.
- 95885: Limited EMG of one extremity, billed with same-day NCS.
- 95886: Complete EMG of one extremity, five or more muscles, with same-day NCS.
- 95887: Add-on for non-extremity muscles, never billed alone.
The 95885 and 95886 codes report per extremity, not per muscle. A complete bilateral lower-limb study with NCS bills 95886 twice. Medicare contractors audit this pairing through local coverage determinations (LCDs).
Autonomic Function Testing CPT Codes (95921 to 95924)
Autonomic testing supports diagnoses such as E11.43 and G90.09. Each code reports a distinct branch of autonomic function. CMS articles set strict component requirements for each one.
| CPT Code | Test | Requirement |
|---|---|---|
| 95921 | Cardiovagal innervation | Two or more parasympathetic measures |
| 95922 | Vasomotor adrenergic | Valsalva plus at least 5 minutes of tilt |
| 95923 | Sudomotor function | QSART or equivalent sweat testing |
| 95924 | Combined testing | Parasympathetic and sympathetic with tilt |
Automated point-of-care devices do not meet the 95923 description under several Medicare LCDs. Novitas directs Sudoscan-type testing to the unlisted code 95999 with a claim narrative. Billing 95923 for device-based screening invites recoupment.
Skin Biopsy for Small Fiber Neuropathy
Skin punch biopsy is the confirmatory test for small fiber neuropathy. The procedure bills 11104 for a single punch biopsy. The pathology analysis of nerve fiber density bills 88356, morphometric analysis of nerve.
Coverage for intraepidermal nerve fiber density (IENFD) testing varies by payer. Many plans require failed or normal electrodiagnostic results first. Pair the claim with G60.8 or the documented cause code, not a screening diagnosis.
Treatment and Injection CPT Codes
Treatment claims for painful neuropathy run through pain management codes. Peripheral nerve blocks bill 64450, injection of an anesthetic agent into another peripheral nerve or branch. Neurolytic destruction of a peripheral nerve bills 64640.
Both codes require a site, a laterality, and a linked diagnosis. M79.2, G57.3-, and the E11.4- set are the common pairings. The diagnosis must show why the injected nerve matches the symptom pattern.
Modifiers for Neuropathy Claims
Modifiers tell the payer about circumstances the CPT code alone cannot show. Neuropathy claims rely on a short list of high-frequency modifiers. Wrong or missing modifiers cause a large share of electrodiagnostic denials.
| Modifier | Use Case | Neuropathy Example |
|---|---|---|
| 25 | Separate E/M, same day as procedure | Office visit plus same-day NCS |
| 59 or XS | Distinct procedural service | EMG and NCS on separate nerves or limbs |
| 26 | Professional component only | Physician interpretation of NCS |
| TC | Technical component only | Facility owns the EMG equipment |
| RT / LT | Right or left side | 64450 on the left peroneal nerve |
| 50 | Bilateral procedure | Bilateral nerve blocks, payer permitting |
| 52 | Reduced services | 95921 with only one cardiovagal test |
| 95 | Telehealth service | Virtual E/M for neuropathy follow-up |
| GA | ABN on file | Non-covered autonomic screening |
Common Neuropathy Coding Errors and Denials
Neuropathy claims fail for predictable reasons. Most errors trace back to specificity or sequencing. Fixing these patterns recovers revenue and lowers the denial rate.
- Overusing G62.9: Repeated unspecified codes flag medical-necessity reviews.
- Pairing E11.42 with G62.9: The combination code already includes the polyneuropathy.
- Using G63 for diabetes. Diabetes uses combination codes, never G63.
- Missing laterality: Mononeuropathy codes reject without a side digit.
- Skipping the drug cause code: Chemo neuropathy needs G62.0 plus T45.1X5-.
- Coding resolved cases as active: Resolved neuropathy uses Z86.69, not a G-code.
Each error carries a financial cost. A denied claim delays payment and adds rework hours. A clean first-pass claim depends on correct type, cause, laterality, and sequencing.
Neuropathy ICD-10 Codes by Specialty
Different specialties assign different neuropathy codes most often. The code set reflects the patient population each specialty treats. This map helps coders anticipate the high-frequency codes by practice type.
| Specialty | Common Codes | Clinical Focus |
|---|---|---|
| Pain Management | M79.2, G62.9, G57.3- | Neuropathic pain and nerve entrapment |
| Endocrinology | E11.4-, E10.4- | Diabetic neuropathy variants |
| Oncology | G62.0, T45.1X5- | Chemotherapy-induced neuropathy |
| Podiatry | G62.9, E11.42 | Lower-limb and diabetic foot neuropathy |
| Neurology | G60.-, G61.-, G62.- | Hereditary, inflammatory, and toxic types |
Specialty context shapes the documentation review. An endocrinology chart should link neuropathy to diabetes. An oncology chart should link it to the chemotherapy agent. Matching the code to the specialty pattern reduces avoidable denials.
2026 ICD-10 Updates for Neuropathy Coding
ICD-10-CM codes update each year on October 1. The 2026 code set took effect October 1, 2025. Coders confirm the active code set for each date of service.
2026 ICD-10 codes for neuropathy are still the same core codes from last year. G62.9, G60.9, and the E11.4- set carried into the 2026 update without change. The code year matters for billing dates, not for the code values themselves.
Reimbursement claims require the ICD-10-CM code active on the service date. A claim filed under a retired code triggers a rejection. Billing teams verify the 2026 descriptors against the current code book before submission.
- Confirm billable status for each code annually.
- Match the code year to the date of service.
- Replace any deleted or revised codes before filing.
Conclusion
Accurate neuropathy coding starts with documented type, cause, and laterality. The right code lowers denials and shortens the payment cycle. The wrong code, or an overused unspecified code, slows revenue and adds rework.
Revenue cycle teams that audit neuropathy claims recover measurable revenue. A coding review catches missing laterality, redundant pairings, and outdated codes before submission. For deeper coding support, see related guides on diabetic coding, denial management, and neurology billing.
Frequently Asked Questions
What is the ICD-10 code for peripheral neuropathy?
The ICD-10 code for peripheral neuropathy is G62.9, Polyneuropathy, unspecified. Coders use G60.9 when the cause is hereditary or idiopathic. A documented cause moves the claim to a more specific code.
Is G62.9 a billable code?
Yes, G62.9 is a billable and specific ICD-10-CM code. Providers report it for polyneuropathy when no cause is documented. Payers accept it, though repeated use invites medical-necessity review.
What is the difference between G62.9 and E11.42?
G62.9 reports polyneuropathy with no stated cause. E11.42 reports polyneuropathy caused by type 2 diabetes. The diabetic case uses E11.42 alone, without adding G62.9.
What is the CPT code for a nerve conduction study for neuropathy?
Nerve conduction studies bill CPT codes 95907 through 95913. The code depends on the total number of nerve studies performed. One unit of a single code reports the full encounter.
What modifier is used when billing EMG with nerve conduction studies?
Same-day EMG with NCS uses the add-on codes 95885 to 95887, which need no unbundling modifier. Modifier 59 or XS applies only when documentation shows distinct nerves, limbs, or sessions.
What is the ICD-10 code for diabetic neuropathy?
The ICD-10 code for diabetic neuropathy is E11.40 for an unspecified type in type 2 diabetes. Polyneuropathy uses E11.42. Type 1 diabetes uses the matching E10.4- codes.
Can you bill neuropathy and diabetes together?
Diabetic neuropathy uses one combination code, not two separate codes. The E11.4- code reports both the diabetes and the nerve damage. Adding a separate G62.9 risks a redundancy denial.
What is the ICD-10 code for neuropathic pain?
The ICD-10 code for neuropathic pain is M79.2, Neuralgia and neuritis, unspecified. Coders use it when the cause and location are unknown. A documented cause supports a more specific code.
Is there an ICD-10 code for obstructive neuropathy?
ICD-10-CM has no peripheral nerve code for “obstructive neuropathy.” This term usually refers to obstructive uropathy, a kidney condition under N13.-. Coders confirm the intended diagnosis before assigning a code.