
Gastroenterology billing is not simply a matter of submitting claims and waiting for payment. It is a specialized, detail-driven process that touches clinical documentation, payer policy, and federal regulation all at once.
According to the Medical Group Management Association, the average physician practice loses up to 30 percent of potential revenue due to billing errors, claim denials, and poor follow-up. For GI practices, where a single colonoscopy claim can carry reimbursement of $500 or more, those losses compound fast.
The American Society for Gastrointestinal Endoscopy estimates that over 19 million colonoscopies are performed annually in the United States, making this one of the most billed and most audited procedures in all of medicine.
This guide is for gastroenterology providers, practice managers, and billing staff who want a clear, practical understanding of how GI billing works, where it goes wrong, and what it takes to protect practice revenue.
What Gastroenterology Billing Includes?
Gastroenterology billing encompasses every financial and administrative function that occurs after a patient receives care. This includes charge capture, medical coding, claim submission, payment posting, denial management, and patient collections. In a well-run GI practice, these functions operate as a continuous cycle rather than isolated tasks.
Key Components of the Gastroenterology Revenue Cycle Management
| Revenue Cycle Component | Core Function |
|---|---|
| Patient Registration | Demographic and insurance data capture |
| Eligibility Verification | Confirming active coverage before service |
| Medical Coding | Translating clinical documentation into billable codes |
| Charge Entry | Entering procedure and diagnosis codes into the billing system |
| Claim Submission | Transmitting clean claims to payers electronically |
| Payment Posting | Reconciling payments against expected reimbursements |
| Denial Management | Identifying, appealing, and resolving rejected claims |
| Patient Collections | Billing and collecting patient-responsible balances |
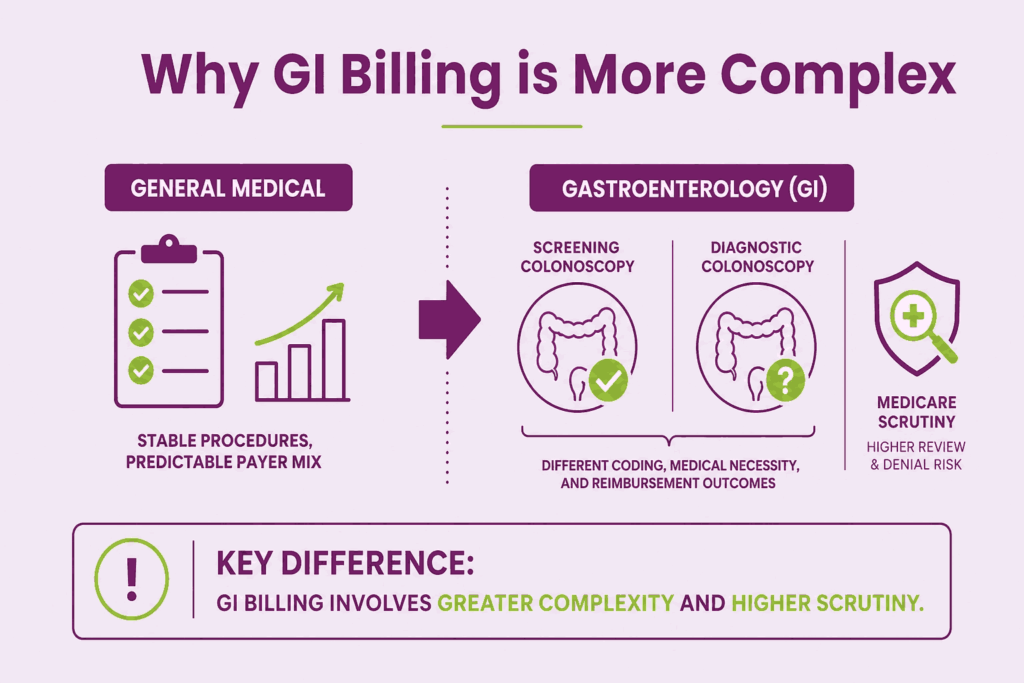
Why GI Billing is More Complex Than General Medical Billing
Most medical specialties deal with a relatively stable set of procedures and a predictable payer mix. Gastroenterology is different. GI practices perform a wide range of procedures, from routine preventive screenings to complex therapeutic interventions, each with its own coding requirements, modifier rules, and documentation standards.
The distinction between a screening colonoscopy and a diagnostic colonoscopy, for instance, affects which CPT code is used, what modifiers apply, how much the patient owes, and how the payer processes the claim. Get that distinction wrong, and the financial consequences follow quickly.
Gastroenterology medical billing also sits at a particularly sensitive intersection with Medicare policy, because colonoscopy is one of the most commonly billed preventive services among Medicare beneficiaries. That means CMS scrutiny is constant, and the margin for error is narrow.
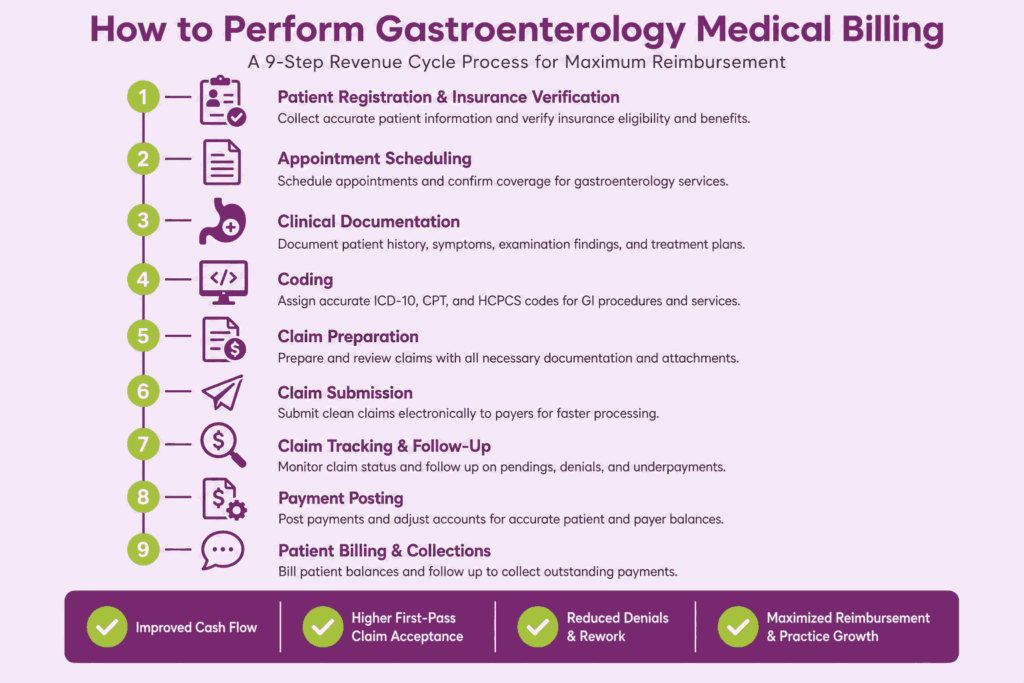
How to Perform Gastroenterology Medical Billing
Gastroenterology billing is not simple. Between procedure-specific coding rules, payer requirements, and documentation standards, there is a lot that can go wrong and a lot of money left on the table when it does. Here is the detailed breakdown of the complete Gastroenterology medical billing process.
Step 1: Patient Registration and Insurance Verification
This is where everything starts, and honestly, it is the most important foundation you can build. Before any procedure even happens, you need to collect complete patient information. That means full legal name, date of birth, address, contact details, and both primary and secondary insurance information if applicable. You also need to get the member ID, group number, and payer ID.
Then you verify eligibility. Actually call the payer or use an eligibility portal to confirm the patient has active coverage and find out exactly what their plan covers. You want to know:
- What is the deductible, and how much has been met
- What is the co-pay or co-insurance for the specific procedure
- Whether a referral is required
- What the out-of-pocket maximum looks like
For instance, gastroenterology procedures like colonoscopies, EGDs, and ERCPs also require prior authorization before the procedure date. Submit that request early, document the authorization number, and attach it to the account. Skipping this step can lead to a claim being denied later.
Step 2: Thorough Clinical Documentation
In gastroenterology billing, accurate clinical documentation is the foundation of clean claims and proper reimbursement. Payers rely entirely on the physician’s notes to determine whether a procedure was medically necessary, correctly coded, and eligible for payment. If critical details are missing, the claim can be denied, downcoded, or flagged for audit.
For GI procedures such as colonoscopies, EGDs, sigmoidoscopies, or biopsy services, documentation must clearly capture the following details:
- Patient’s symptoms
- Medical history
- Indications for the procedure
- The physician’s findings
Moreover, the details such as polyps removed, biopsies performed, bleeding identified, inflammation severity, or lesion location should be documented precisely to support CPT and ICD-10 coding.
The distinction between a screening colonoscopy and a diagnostic colonoscopy is especially important because it directly affects coding, modifier usage, payer coverage, and patient responsibility. Physicians should also document the type of sedation administered, procedure completion status, pathology samples collected, complications encountered, and recommended follow-up care.
Step 3: Medical Coding
This is the technical core of the entire gastroenterology billing process and directly impacts reimbursement accuracy and claim acceptance. Gastroenterology billing depends on three essential medical coding systems working together correctly to support clean and compliant claim submissions. CPT codes identify the exact gastroenterology procedure performed during the patient encounter and determine the reimbursement amount from payers.
Commonly Used Gastroenterology CPT Codes
CPT Codes describe the procedure performed. Some common ones you will work with regularly:
| Procedure | CPT Code |
|---|---|
| Diagnostic colonoscopy | 45378 |
| Screening colonoscopy (Medicare) | G0105 / G0121 |
| Colonoscopy with biopsy | 45380 |
| Colonoscopy with polypectomy (snare) | 45385 |
| Diagnostic EGD | 43239 |
| EGD with biopsy | 43239 |
| Flexible sigmoidoscopy | 45330 |
| Capsule endoscopy | 91110 |
| ERCP with stent placement | 43274 |
ICD-10-CM Codes
Common GI ICD-10 categories include:
- K57 series: Diverticular disease of the intestine
- K92 series: Other diseases of the digestive system
- Z12.11: Encounter for screening for malignant neoplasm of the colon
- K21: Gastroesophageal reflux disease
- K80: Cholelithiasis
Modifiers Commonly Used in GI Billing
Modifiers are where a lot of people stumble, but they are genuinely important in GI billing.
- Modifier 59 shows the payer that two procedures are distinct and should each be reimbursed.
- Modifier PT is one you need to know specifically for gastroenterology because it tells Medicare that a screening colonoscopy became diagnostic during the procedure, which affects the patient’s cost-sharing.
- Modifier 53 is used when a procedure was started but had to be discontinued.
| Modifier | Purpose |
|---|---|
| 33 | Preventive service (waives patient cost-sharing) |
| PT | Colorectal cancer screening test that became diagnostic (Medicare) |
| 59 | Distinct procedural service |
| 52 | Reduced services |
| 53 | Discontinued procedure |
| 76 | Repeat the procedure by the same physician |
Step 4: Charge Capture and Fee Schedule
Once the codes are assigned, every charge needs to be captured accurately and mapped to your practice fee schedule. One thing that trips up a lot of people is forgetting that gastroenterology billing often involves multiple separate claims for the same encounter. The physician, facility, or ASC bills separately. If a biopsy was sent to pathology, that lab bills separately, too.
And here is where things get granular. Each of those claims needs its own attending provider information, its own diagnosis codes, and its own modifiers where applicable. For example, if a colonoscopy with biopsy was performed, the physician’s claim typically uses CPT 45380, while a snare polypectomy on the same patient during the same session would require modifier 51 to indicate multiple procedures. Missing that modifier does not just slow things down. It often triggers an outright denial.
You also need to apply the correct Place of Service code because it affects reimbursement rates. Office visits get POS 11. Outpatient hospital procedures get POS 22. Ambulatory Surgery Centers get POS 24. The reimbursement difference between POS 22 and POS 24 can be significant, depending on your payer contracts, so this is not a field to guess on or copy from a previous claim without verifying. Using the wrong one can result in underpayment or denial, so double-check it every time.
Step 5: Claim Submission
The claim goes out on a CMS-1500 form for professional billing or a UB-04 for facility billing. Most practices submit electronically through a clearinghouse like Availity or Change Healthcare, which is significantly faster than paper and allows you to catch errors before the claim even reaches the payer.
A good clearinghouse will flag things like mismatched NPI numbers or missing authorization codes right at the front door, which saves you from a denial that could have been avoided entirely.
Before submission, run through a checklist every single time. Confirm the correct NPI for both the billing and rendering provider, because using a group NPI when the payer expects an individual NPI is one of the common gastroenterology billing mistakes that causes unnecessary delays. Make sure the taxonomy code accurately reflects the provider’s specialty.
Verify that the date of service matches the documentation exactly, that diagnosis codes are properly linked to the correct procedure codes, and that any required authorization number is included on the claim.
For gastroenterology specifically, procedures like colonoscopies and upper endoscopies performed in an ASC setting frequently require prior authorization from commercial payers like UnitedHealthcare and Cigna, and forgetting to include that number is one of the fastest ways to generate a denial.
Timely filing limits are non-negotiable. Medicare allows one year from the date of service. Most commercial payers allow 90 to 180 days, though some are stricter. Aetna, for example, requires submission within 90 days for many plans.
Missing those windows means you lose the money entirely, so track your submission dates carefully and build internal alerts into your practice management system before claims age past the safe zone.
Step 6: Payment Posting and EOB Review
When the payer sends back an Explanation of Benefits or an Electronic Remittance Advice, you post the payment to the patient account and review what the payer actually paid versus what was billed. This step sounds straightforward, but it is where a lot of money quietly disappears.
Look carefully at any adjustments or reductions and make sure contractual write-offs are applied correctly based on your payer contracts. If your contract with BlueCross says the allowed amount for CPT 45378 is $320 and they paid $288, you need to know whether that $32 difference is a legitimate contractual adjustment or a processing error before you write it off.
If the payer paid less than expected, figure out why before you move on. Sometimes it is a standard contractual adjustment that reflects your negotiated rate. Other times it signals something worth investigating, like a procedure being downgraded, a modifier being ignored, or a bundling edit that should not have been applied.
For instance, if you billed a colonoscopy with polyp removal and the payer only reimbursed for the colonoscopy alone, that is a bundling issue worth appealing with the correct modifier and supporting documentation.
Step 7: Denial Management and Appeals
Denials happen. Even in the most organized billing departments, claims get denied. The key is working them quickly and systematically, because most payers give you a limited window to appeal, often 60 to 180 days from the denial date, depending on the payer and your contract terms.
Common denial reasons in gastroenterology include missing or invalid prior authorization, medical necessity not established, incorrect modifier usage, duplicate claim submission, and coding errors or mismatched diagnosis and procedure codes.
Each one of those requires a different response. A duplicate claim denial, for example, just needs you to verify whether the original claim was processed and paid correctly. A medical necessity denial for a diagnostic colonoscopy ordered for rectal bleeding requires the physician to provide clinical notes, relevant history, and supporting documentation showing why the procedure was warranted.
When a denial comes in, read the remark codes carefully. CARC code 4 means the procedure requires prior authorization. CARC code 197 means the authorization number is missing or invalid. CARC code 50 means the service is not covered under the patient’s plan. Each of those tells you a completely different story and requires a completely different fix.
For clinical denials where the payer is questioning medical necessity, work with the physician to prepare a well-documented appeal letter that references the specific clinical documentation, the diagnosis that prompted the procedure, and any relevant clinical guidelines from organizations like the American College of Gastroenterology. Many of those denials are reversible when the appeal is thorough and timely.
Step 8: Patient Billing and Collections
After insurance pays, post any remaining patient responsibility to the account and send a clear, easy-to-read statement. Patients should be able to understand what the insurance paid, what was written off contractually, and what they owe without needing to call your office for an explanation. A confusing bill is one of the biggest reasons patient balances go uncollected, not because the patient is unwilling to pay, but because they do not understand what they are being asked to pay or why.
Offer payment plan options where the balance warrants it. A patient who owes $800 after a colonoscopy is much more likely to pay it in four installments of $200 than to write a single check. Most practice management platforms allow you to set up automated payment plans, which removes the friction on both sides.
If accounts go unpaid after multiple follow-up attempts, which typically means two to three statements and at least one phone call, you may escalate to a collections process. Before doing that, make sure every internal follow-up effort is documented in the patient account so the full picture is clear if there is ever a dispute later.
Step 9: Compliance and Ongoing Auditing
Gastroenterology billing is heavily scrutinized, particularly colonoscopy billing, because it is such a high-volume service. Regular internal audits of your coding and documentation practices protect the practice from overpayments, underpayments, and potential compliance issues. Stay current on payer policy changes, CMS updates, and coding guideline revisions because they change more often than most people realize.
The whole process works best when the clinical team, the coders, and the billing staff are communicating regularly. A great biller who never talks to the physician is going to miss things. A physician who documents well but has no idea what the billing team needs is also going to create problems. It really does take the whole team working together.
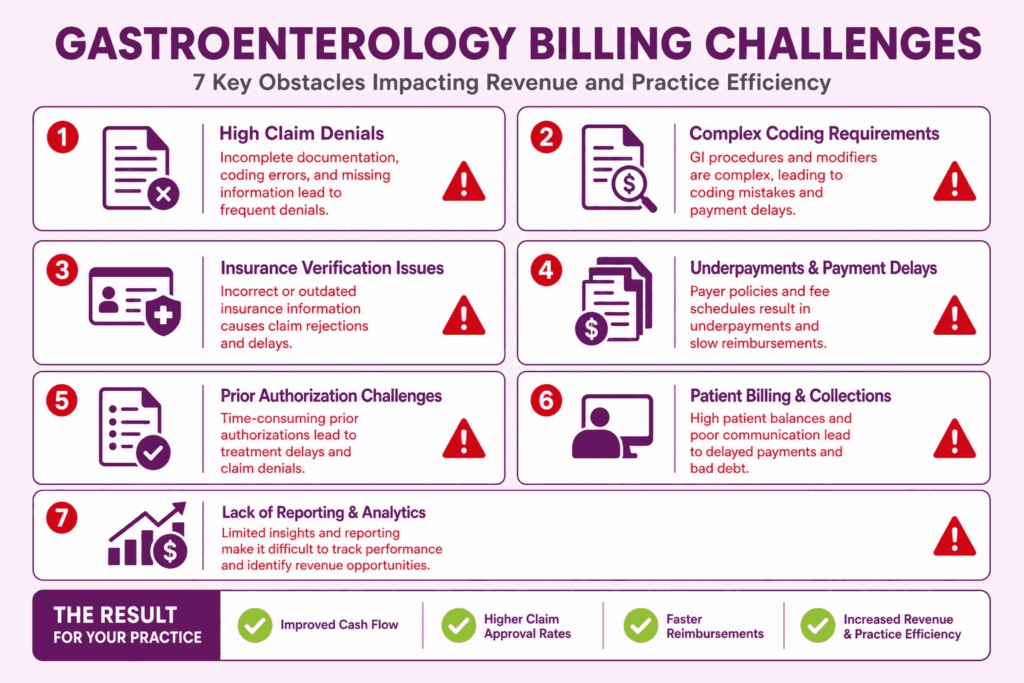
Gastroenterology Billing Challenges
Identifying and addressing common gastroenterology billing obstacles is essential for maintaining healthy cash flow and long-term practice growth. Here are the most common Gastroenterology billing challenges that practices face.
1. Frequent Coding Errors
The most common coding errors in GI billing include using the wrong colonoscopy code family, failing to apply the correct modifier when a screening procedure becomes diagnostic, and missing add-on codes for services performed during the same session. These errors either result in denials or, worse, underpayments that go unnoticed for months.
2. Insurance Claim Denials
Denial rates in gastroenterology tend to be higher than in many other specialties, primarily because of the complexity of colonoscopy billing and the frequent use of prior authorization-dependent procedures. A denied claim is not a closed claim. It requires investigation, correction, and resubmission, all of which consume staff time and delay cash flow.
3. Prior Authorization Issues
Commercial payers commonly require prior authorization for capsule endoscopy, ERCP, and certain therapeutic colonoscopy procedures. When authorization is not obtained before the service, or when the authorization does not match the service actually performed, the claim will be denied. The financial burden then often falls on the patient or the practice.
4. Bundling and Unbundling Mistakes
The National Correct Coding Initiative (NCCI) establishes rules about which codes can and cannot be billed together. Billing two codes that are bundled under NCCI rules without the appropriate modifier is an unbundling error and constitutes a compliance violation. Conversely, failing to bill appropriate add-on codes when they are warranted results in revenue loss.
5. Gastroenterology Practice Documentation Issues
When clinical notes lack the specificity needed to support the billed codes, the practice is exposed to both denial and audit risks. This is particularly common in high-volume endoscopy centers, where procedure notes are templated, and providers may not sufficiently customize them to reflect what actually occurred.
A colonoscopy note that simply reads “polyp removed” without specifying the location, size, or removal technique gives the coder nothing reliable to work with. That gap between what happened in the procedure room and what was written down is where clean claims fall apart. Payers do not reimburse based on what the physician intended to document. They reimburse based on what is actually there.
6. Compliance and Audit Risks
The Office of Inspector General (OIG) regularly targets gastroenterology in its work plan, particularly around colonoscopy coding and modifier use. Practices that bill aggressively without adequate documentation review face the risk of recoupment, civil monetary penalties, and, in serious cases, exclusion from federal programs.
7. Underpayments from Insurance Companies
Not every payment error comes in the form of a denial. Payers sometimes pay less than the contracted rate, and if the practice does not have a system to catch these discrepancies, the underpayment becomes permanent. Regular payment variance analysis is an essential but often overlooked component of GI revenue cycle management.
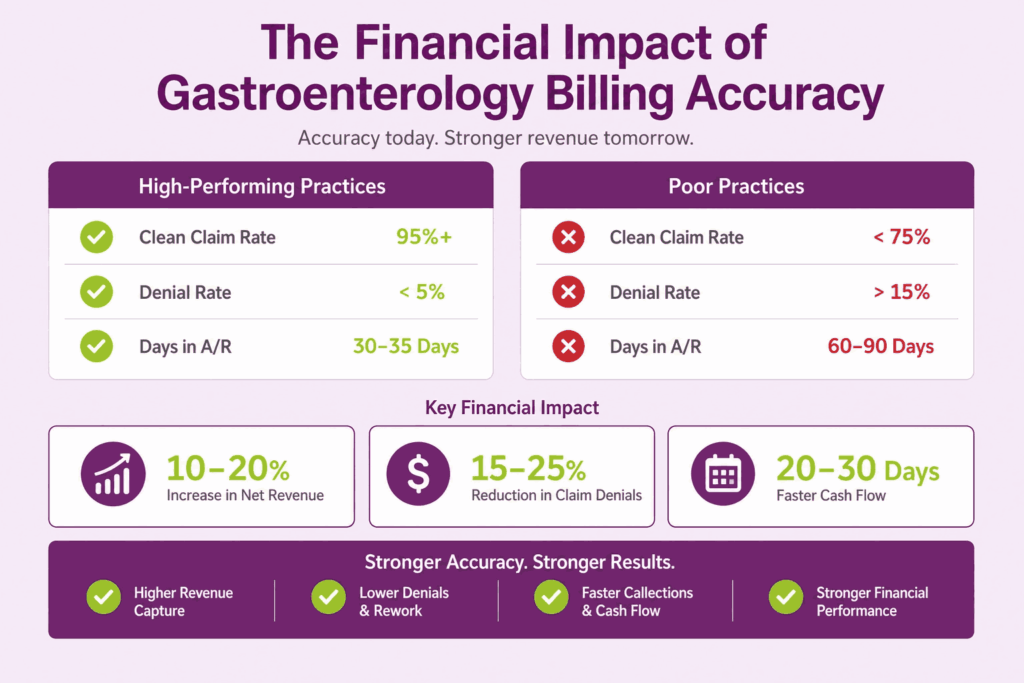
The Financial Impact of Gastroenterology Billing Accuracy
Revenue cycle performance in gastroenterology is directly tied to documentation quality and coding precision. Practices that invest in accurate billing and in the right gastroenterology billing services to support it consistently see higher first-pass claim acceptance rates, faster reimbursement cycles, and fewer write-offs. Those that do not often discover the damage only when their accounts receivable start aging beyond 90 days.
According to industry benchmarks, clean claim rates for high-performing GI practices typically exceed 95 percent. For practices without dedicated billing oversight, rates below 80 percent are not uncommon, and each rejected claim represents both lost time and delayed revenue.
Best Practices to Maximize Gastroenterology Revenue
None of these practices is complicated. They’re just the ones that separate practices running a tight revenue cycle from ones constantly chasing their own tail.
1. Regular Coding Audits
Quarterly audits work best when you’re pulling claims across procedure categories, not just your highest volume ones. Audit colonoscopies and also audit your ERCP claims, because that’s where coding complexity and reimbursement value collide. Look specifically for modifier misuse, unbundling errors, and cases where a diagnostic procedure was coded as screening or vice versa. Those are the patterns that quietly drain revenue and, left unchecked, the ones that show up in payer audits later.
2. Staff Training and Education
Annual CMS updates, NCCI edit changes, and payer-specific policy shifts aren’t optional reading for your billing team. They’re the job. Build continuing education units into your staff expectations and support your coders in maintaining their CPC or CGSC credentials. A coder who last updated their knowledge in 2021 is coding like it’s 2021, and payers definitely aren’t paying like it’s 2021.
3. Accurate Documentation Habits
This one lives with the physician, not the biller. When a provider documents “colonoscopy with biopsy” without specifying the location, size, or method of removal, the coder is left guessing. Regular one-on-one feedback sessions between coders and providers, using actual claim examples, fix this faster than any policy memo ever will.
4. Monitoring Payer Trends
Pull your denial data by payer every month. If UnitedHealthcare suddenly starts denying capsule endoscopy claims that were sailing through six months ago, that’s not a coincidence. That’s a policy shift, and you need to catch it before it costs you thousands in unrecovered revenue.
5. Improving Patient Collections
High-deductible plans have made patients a significant payer category, and most practices still treat collections like an afterthought. Giving patients a real cost estimate before their procedure, offering a simple payment plan, and collecting what’s owed at check-in rather than chasing it afterward makes a measurable difference in what actually gets collected.
6. Tracking KPIs and Financial Performance
Key performance indicators to monitor in GI billing include:
| KPI | Target Benchmark |
|---|---|
| Clean claim rate | Above 95% |
| Days in AR | Below 35 days |
| Denial rate | Below 5% |
| First-pass resolution rate | Above 90% |
| Collection rate | Above 98% of the allowed amounts |






