
Psychiatry CPT codes are the standardized billing codes that psychiatrists, psychiatric nurse practitioners, and behavioral health practices use to describe clinical services on insurance claims. The American Medical Association (AMA) maintains these five-digit codes through its CPT Editorial Panel.
For psychiatry, the code set is distinct from general mental health coding. Psychiatrists almost always pair an Evaluation and Management (E/M) code with a psychotherapy add-on. Therapists, social workers, and counselors typically bill psychotherapy codes alone. That difference drives reimbursement, audit risk, and documentation rules.
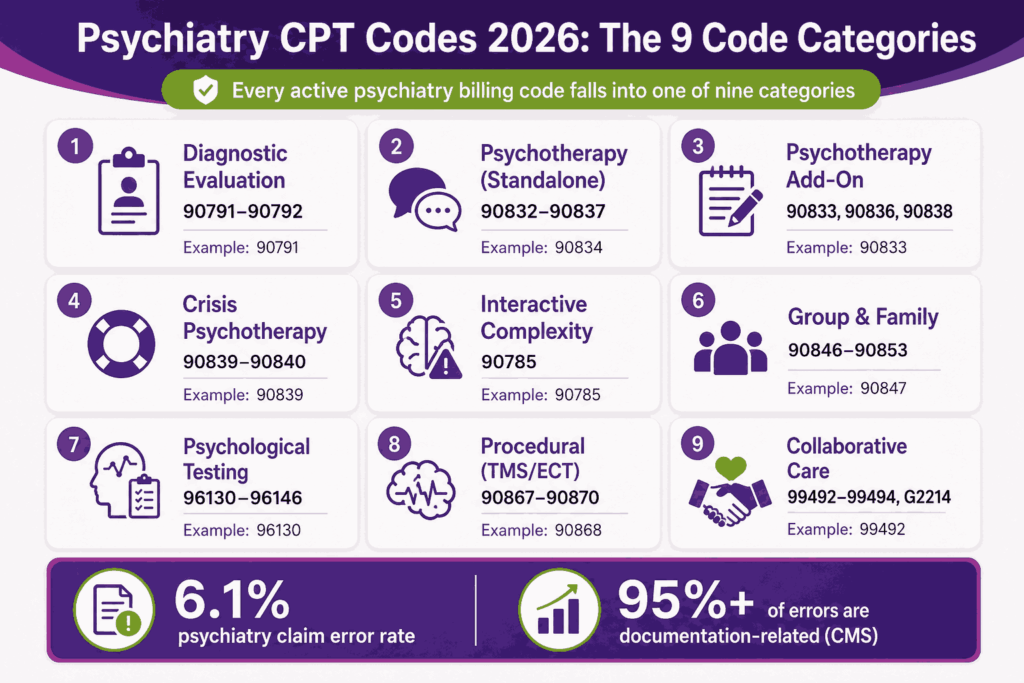
The HHS Office of Inspector General has repeatedly identified psychotherapy as a high-risk billing area in multiple audit cycles. CMS data further highlights the issue, as 6.1% psychiatry claim error rate, 78.3% of improper payments caused by insufficient documentation, 17% by missing documentation, and 2.6% by incorrect coding. In total, documentation-related failures account for more than 95% of psychiatry billing errors.
This guide covers every active psychiatry CPT code category in 2026. It maps each code to its time range, billing scenario, documentation requirement, and Medicare reimbursement rate. It also covers the 2025 and 2026 changes to G2211, telehealth modifiers, and collaborative care codes that most published guides have not updated.
If you bill psychiatric services, lead a billing operation, or work in an RCM function supporting behavioral health, this guide gives you the working reference you need for accurate claims, fewer denials, and clean audit defense.
What Psychiatry CPT Codes Cover
Current Procedural Terminology (CPT) is the AMA’s standardized code set for medical, surgical, and diagnostic services. Psychiatry CPT codes describe the specific behavioral health services delivered, including evaluations, psychotherapy, crisis intervention, testing, and procedural services like Transcranial Magnetic Stimulation (TMS).
Each code is five digits. Most psychiatry codes sit in the 90785 to 90899 range. E/M codes used by psychiatrists fall in the 99202 to 99215 range. Some procedural and HCPCS Level II codes (the G-codes) also apply.
CPT codes differ from ICD-10 codes. CPT describes what the provider did. ICD-10 describes why, by capturing the diagnosis. Both appear on a claim. Both must match for the claim to clear payer adjudication.
Who Uses Psychiatry CPT Codes
The code set applies across multiple provider types, but the codes each provider can bill are not the same.
- Psychiatrists (MD/DO) can bill the full range, including E/M codes
- Psychiatric Mental Health Nurse Practitioners (PMHNPs) can bill most psychiatry codes, including E/M
- Physician Assistants (PAs) working in psychiatry can bill E/M and add-on codes
- Psychologists (PhD/PsyD) can bill psychotherapy and testing codes, not E/M
- Licensed Clinical Social Workers (LCSWs), LPCs, LMFTs can bill psychotherapy and 90791, not E/M or 90792
Psychiatry CPT Code Categories at a Glance
The codes fall into nine working categories. Each category has its own documentation and timing rules.
| Category | Code Range | Common Codes | Used For |
|---|---|---|---|
| Diagnostic Evaluation | 90791-90792 | 90791, 90792 | Initial assessments |
| Psychotherapy (standalone) | 90832-90838 | 90832, 90834, 90837 | Therapy by time |
| Psychotherapy Add-On | 90833, 90836, 90838 | 90833, 90836, 90838 | Therapy with E/M |
| Crisis Psychotherapy | 90839-90840 | 90839, 90840 | Acute crisis sessions |
| Interactive Complexity | 90785 | 90785 | Communication barriers |
| Group and Family | 90846-90853 | 90846, 90847, 90853 | Group, family, multi-patient |
| Psychological Testing | 96130-96146 | 96130, 96136, 96146 | Testing and assessment |
| Procedural Psychiatry | 90867-90870 | 90867, 90868, 90870 | TMS, ECT |
| Collaborative Care | 99492-99494, G2214 | 99492, 99493, G2214 | CoCM behavioral health |
Psychiatric Diagnostic Evaluation Codes
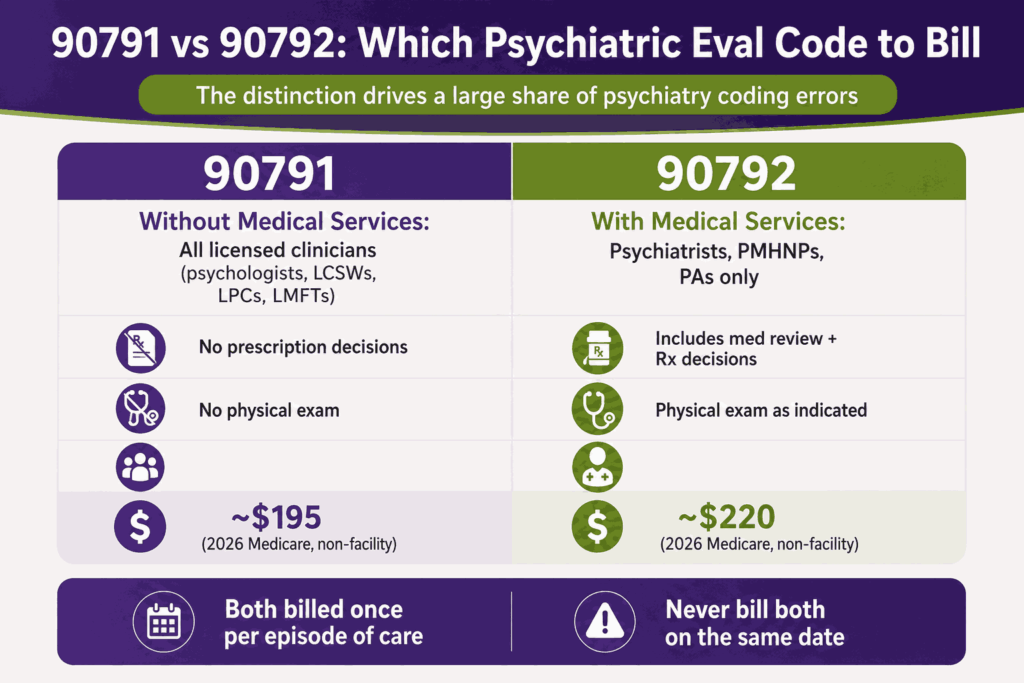
Diagnostic evaluation codes cover the intake assessment that opens a new course of care. There are two codes, and the distinction between them drives a large share of psychiatry coding errors.
CPT Code 90791 (Without Medical Services)
CPT code 90791 is a psychiatric diagnostic evaluation without medical services. It covers an integrated biopsychosocial assessment, including history, mental status exam, and treatment recommendations.
Non-prescribing clinicians use 90791. This includes psychologists, LCSWs, LPCs, and LMFTs. The code does not include prescription decisions or physical exam elements. Documentation must show that the assessment took place face-to-face or via approved telehealth.
CPT Code 90792 (With Medical Services)
CPT code 90792 is a psychiatric diagnostic evaluation with medical services. It covers the same biopsychosocial assessment plus medical elements: history of present illness, physical exam as indicated, medication review, lab orders, and prescription decisions.
Only providers qualified to deliver medical services can bill 90792. That means psychiatrists, PMHNPs, and PAs. The code carries a higher reimbursement rate than 90791 because of the added medical complexity.
90791 vs 90792 at a Glance
| Element | 90791 | 90792 |
|---|---|---|
| Includes medical services | No | Yes |
| Eligible providers | All licensed clinicians | Psychiatrists, PMHNPs, PAs |
| Prescription decisions | Excluded | Included |
| Physical exam elements | Excluded | Included as indicated |
| 2026 Medicare rate (non-facility) | ~$195 | ~$220 |
| Typical frequency | Once per episode of care | Once per episode of care |
Both codes are usually billed once per patient per episode of care. Some payers allow a second 90791 or 90792 if the patient returns after a long gap or presents with a new clinical concern.
Psychotherapy CPT Codes
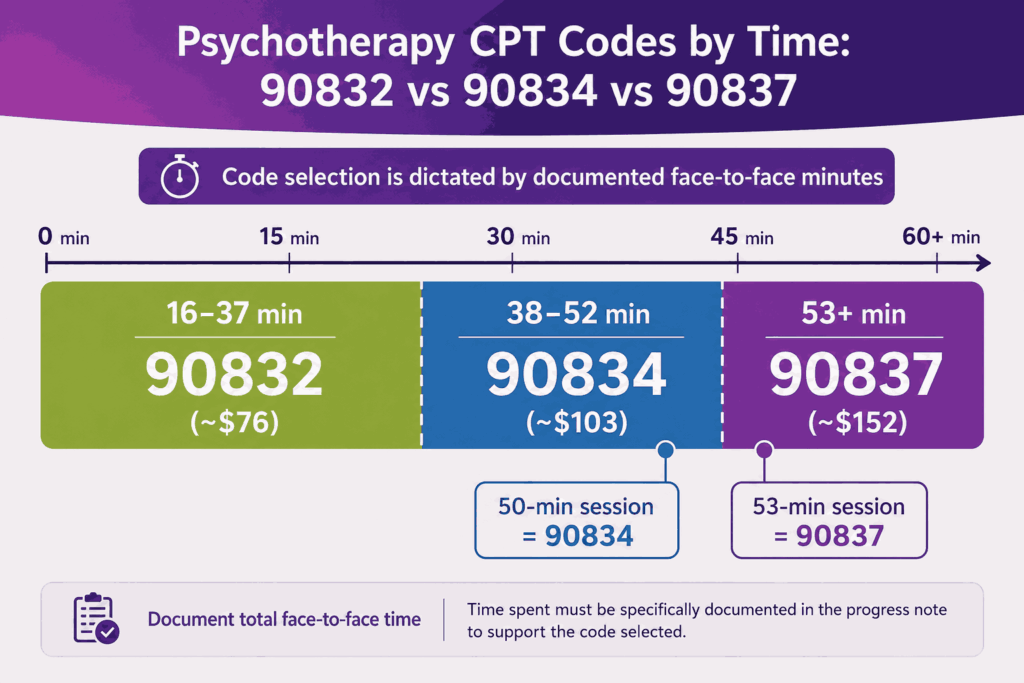
Psychotherapy codes are time-based. The minutes of face-to-face therapy delivered dictate the code selection. These are the three most common standalone psychotherapy codes in psychiatry billing.
Time-Based Psychotherapy Codes (90832, 90834, 90837)
| Code | Time Range | Description | 2026 Medicare Rate (Non-Facility) |
|---|---|---|---|
| 90832 | 16-37 minutes | Psychotherapy with patient | ~$76 |
| 90834 | 38-52 minutes | Psychotherapy with patient | ~$103 |
| 90837 | 53+ minutes | Psychotherapy with patient | ~$152 |
The midpoint rule applies. A 50-minute session bills as 90834. A 53-minute session billed as 90837. Document the exact start and stop time of psychotherapy in every note.
Why 90837 Carries the Highest Audit Risk
Payer scrutiny is highest on 90837. Some commercial insurers and Medicare Administrative Contractors (MACs) audit providers who bill 90837 on a high percentage of total claims. The Centers for Medicare and Medicaid Services (CMS) has flagged 90832, 90834, and 90837 as priority audit targets in past years.
Audit triggers that auditors look for:
- Bills 90837 on more than 60-70% of claims without supporting documentation
- Note that does not document actual start and stop time
- Generic copy-pasted progress notes across multiple sessions
- No clear treatment plan linking the session to a defined goal
- Missing modality (CBT, DBT, EMDR, psychodynamic) in the note
When Psychiatrists Use Standalone Psychotherapy Codes
In most psychiatry workflows, the psychiatrist bills an E/M code paired with a psychotherapy add-on code. Standalone 90832, 90834, or 90837 is rarely the right code for a psychiatrist because medication management almost always factors into the visit. The standalone codes are more common for psychologists and licensed therapists. Dedicated psychiatry billing services routinely flag standalone code submissions for prescribing providers to protect the clinical revenue cycle from unnecessary downgrading.
E/M Plus Psychotherapy Add-On Codes
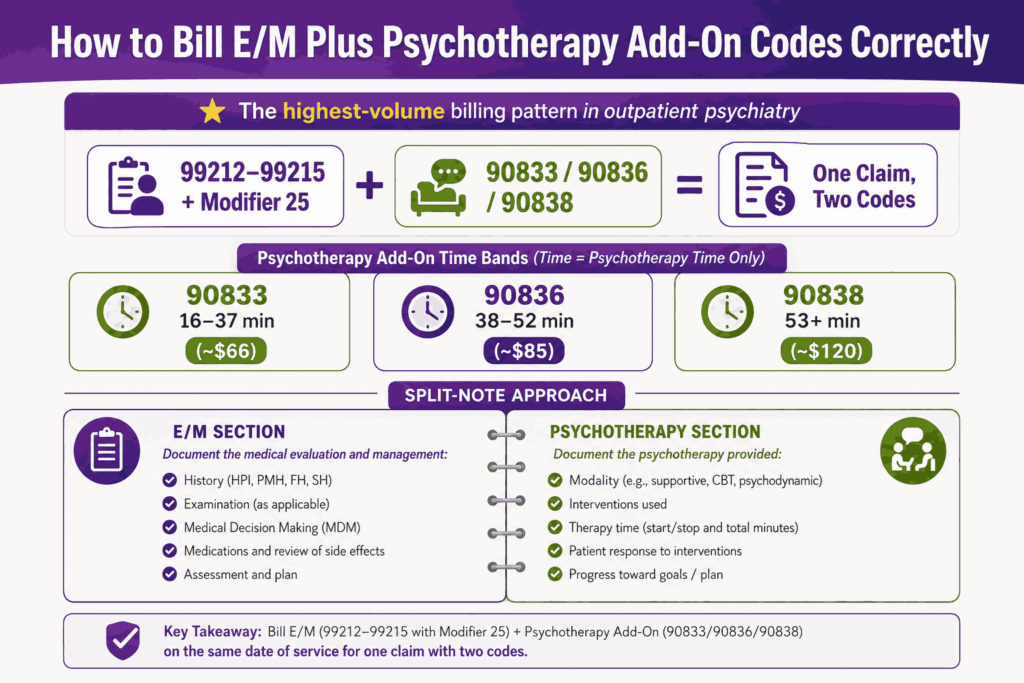
This is the highest-volume billing pattern in outpatient psychiatry. The psychiatrist bills an E/M code for the medical visit, then adds a psychotherapy add-on code for the therapy portion. Two codes appear on the claim.
The Three Psychotherapy Add-On Codes
| Code | Therapy Time | Pairs With | 2026 Medicare Rate (Non-Facility) |
|---|---|---|---|
| 90833 | 16-37 minutes | 99212-99215 or 99202-99205 | ~$66 |
| 90836 | 38-52 minutes | 99212-99215 or 99202-99205 | ~$85 |
| 90838 | 53+ minutes | 99212-99215 or 99202-99205 | ~$120 |
Add-on codes cannot stand alone. They must accompany a primary E/M code on the same date of service. The time billed for the add-on is therapy time only. E/M activities like medication review, MDM, and history-taking are tracked separately under the E/M code.
E/M Codes Used in Psychiatry
| Code | Visit Type | Time (2021+ Guidelines) | 2026 Medicare Rate |
|---|---|---|---|
| 99202 | New patient | 15-29 min | ~$72 |
| 99203 | New patient | 30-44 min | ~$111 |
| 99204 | New patient | 45-59 min | ~$169 |
| 99205 | New patient | 60-74 min | ~$224 |
| 99212 | Established patient | 10-19 min | ~$56 |
| 99213 | Established patient | 20-29 min | ~$91 |
| 99214 | Established patient | 30-39 min | ~$129 |
| 99215 | Established patient | 40-54 min | ~$183 |
Since 2021, E/M code level selection is based on either medical decision-making (MDM) or total time on the date of service. Total time can include both face-to-face and non-face-to-face work, like chart review and care coordination.
Modifier 25 Documentation Rule
When billing an E/M code with a psychotherapy add-on, append modifier 25 to the E/M code. This signals to the payer that the E/M service is significant, separately identifiable, and distinct from the psychotherapy component.
The note must clearly separate the E/M elements (medication review, MDM, history, ROS) from the psychotherapy elements (modality, interventions, patient response, therapy minutes). A blended single-paragraph note invites denial.
Crisis and Interactive Complexity Codes
Some sessions fall outside standard psychotherapy time bands. The crisis and interactive complexity codes cover these scenarios.
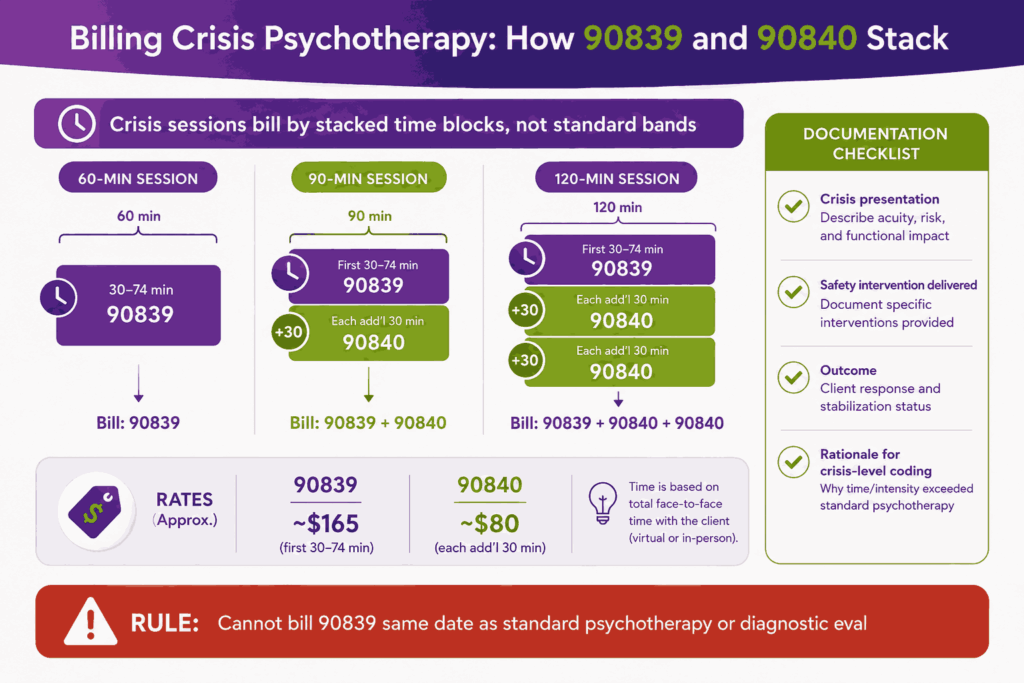
CPT Codes 90839 and 90840 (Crisis Psychotherapy)
CPT code 90839 covers the first 30 to 74 minutes of psychotherapy for a patient in acute crisis. Use it for sessions where the patient presents with active suicidality, acute psychosis, or another condition requiring immediate stabilization.
CPT code 90840 is the add-on for each additional 30 minutes beyond 74 minutes. A 90-minute crisis session bills as 90839 + 90840. A 120-minute crisis session bills as 90839 + 90840 + 90840.
Documentation must include:
- Description of the crisis presentation
- Specific safety planning or intervention delivered
- Outcome of the intervention
- Rationale for crisis-level coding over standard psychotherapy
90839 cannot be billed on the same date as a standard psychotherapy code or a diagnostic evaluation code for the same patient.
CPT Code 90785 (Interactive Complexity)
CPT code 90785 is an add-on code for sessions with communication factors that complicate care delivery. It is not a standalone code.
Common scenarios for 90785:
- Sessions requiring an interpreter for language or hearing
- Sessions where a parent or guardian must be involved alongside the patient
- Sessions where caretakers or third parties create communication challenges
- Sessions involving mandated reporting decisions
90785 pairs with 90791, 90792, 90832, 90834, 90837, 90833, 90836, 90838, or 90853. Reimbursement is modest (around $7 on the 2026 Medicare fee schedule), but the code captures real clinical complexity.
Group, Family, and Multi-Patient Codes
Outpatient psychiatry includes group and family sessions. The CPT codes for these scenarios differ from individual psychotherapy codes.
| Code | Description | Typical Setting |
|---|---|---|
| 90846 | Family psychotherapy without patient present | Family-led care planning |
| 90847 | Family psychotherapy with patient present | Joint family sessions |
| 90849 | Multiple-family group psychotherapy | Group of families together |
| 90853 | Group psychotherapy (not family) | Group therapy with unrelated patients |
90846 and 90847 each cover approximately 50 minutes of family work. 90853 covers a single group session for one patient, regardless of how many group members are present. Bill 90853 per patient, not per group.
Family codes are not time-flexible the way 90832, 90834, and 90837 are. If a family session runs longer, you cannot upcode by minutes. Some payers allow prolonged service codes (99354, 99355) for extended family sessions, but coverage varies.
Psychological and Neuropsychological Testing Codes
Testing codes are a distinct subset within psychiatry CPT. They cover formal psychological assessment, neuropsychological testing, and brief screening instruments. The 2019 restructure replaced older testing codes with the current 96130 to 96146 range.
| Code | Description | Time Component |
|---|---|---|
| 96130 | Psychological testing evaluation services (first hour) | First 60 minutes |
| 96131 | Each additional hour of 96130 | Per additional hour |
| 96132 | Neuropsychological testing evaluation services (first hour) | First 60 minutes |
| 96133 | Each additional hour of 96132 | Per additional hour |
| 96136 | Test administration by professional (first 30 min) | First 30 minutes |
| 96137 | Test administration by professional (each additional 30) | Per additional 30 min |
| 96138 | Test administration by technician (first 30 min) | First 30 minutes |
| 96139 | Test administration by technician (each additional 30) | Per additional 30 min |
| 96146 | Single automated test, electronic platform | Per test |
96130 and 96132 cover the professional time spent integrating test results, writing reports, and interpreting findings. 96136 and 96138 cover the actual test administration time, separated by whether a professional or a technician administered the test.
Brief Screening Code (96127)
CPT code 96127 covers brief emotional or behavioral assessment instruments like the PHQ-9, GAD-7, or AUDIT. Each completed instrument bills as one unit of 96127. Up to four instruments per visit are typically reimbursable.
Procedural Psychiatry Codes
Psychiatry includes procedural services that most generalist mental health coding guides skip. These codes carry higher reimbursement and stricter documentation rules.
Transcranial Magnetic Stimulation (TMS) Codes
| Code | Description |
|---|---|
| 90867 | TMS therapy, initial treatment, motor threshold determination, delivery, and management |
| 90868 | TMS therapy, subsequent treatment, delivery, and management |
| 90869 | TMS therapy, subsequent motor threshold redetermination with delivery and management |
TMS is FDA-cleared for treatment-resistant major depressive disorder, OCD, and select other indications. Most commercial payers require prior authorization. Medicare coverage varies by MAC and Local Coverage Determination (LCD). Document failed prior trials of at least two antidepressants for typical coverage.
Electroconvulsive Therapy (ECT) Codes
CPT code 90870 covers electroconvulsive therapy, including necessary monitoring during the procedure. Anesthesia services bill separately under appropriate anesthesia codes. ECT remains the most rapidly effective intervention for severe depression with suicidality, catatonia, and severe psychotic depression.
Collaborative Care and Behavioral Health Integration Codes
The Psychiatric Collaborative Care Model (CoCM) is one of the fastest-growing behavioral health billing pathways for primary care and integrated care settings. The codes apply when a primary care provider, a behavioral health care manager, and a psychiatric consultant work together to deliver behavioral health treatment.
Core CoCM Codes
| Code | Description | Time Component |
|---|---|---|
| 99492 | Initial CoCM services | First 70 min/month |
| 99493 | Subsequent CoCM services | Each subsequent month, 60 min |
| 99494 | CoCM add-on | Each additional 30 min/month |
| G2214 | Brief CoCM services | First 30 min/month or subsequent 30 min |
99492 is billed for the first calendar month of CoCM services. 99493 is billed for each subsequent month. 99494 is an add-on for time beyond the base.
General Behavioral Health Integration (BHI)
CPT code 99484 covers care management services for behavioral health conditions. It requires at least 20 minutes per calendar month of clinical staff time directed by a billing provider. Unlike CoCM, BHI does not require a psychiatric consultant.
Digital Mental Health Treatment Codes (G0552-G0554)
CMS added HCPCS codes G0552 through G0554 for FDA-cleared digital mental health treatment devices furnished under a behavioral health treatment plan. These codes apply when a prescription includes digital therapeutic supplements, traditional psychotherapy, or medication management. Coverage and rates are still settling across payers as of 2026.
Telehealth Coding for Psychiatry in 2026
Telehealth is a permanent feature of psychiatric care delivery. The 2025 and 2026 rules continue Medicare’s expanded coverage of mental and behavioral health telehealth services.
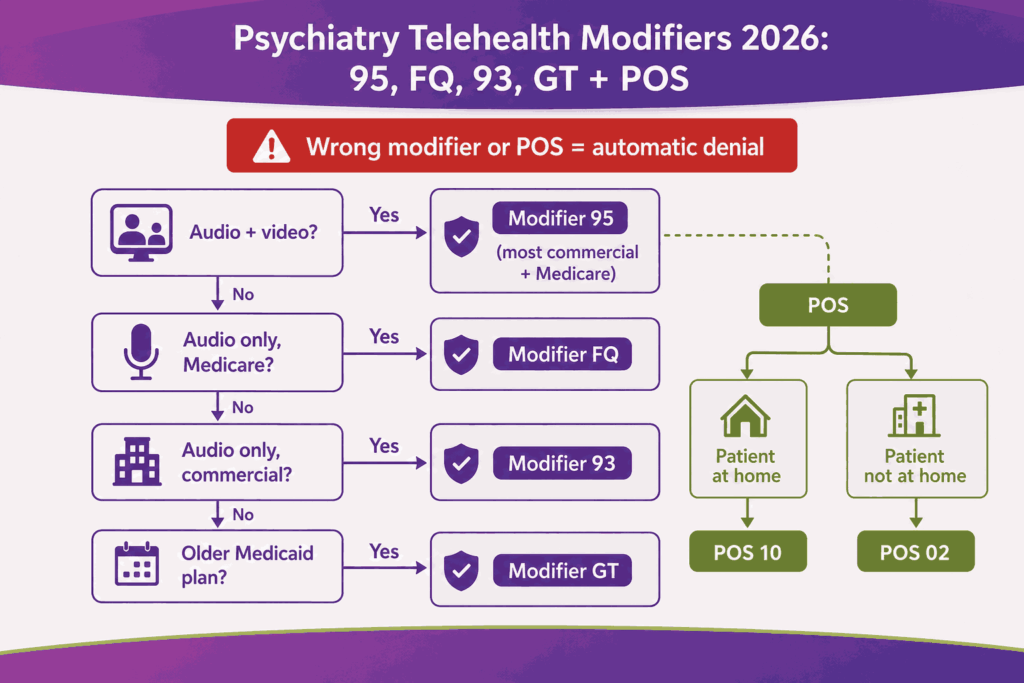
Telehealth Modifiers
| Modifier | Meaning |
|---|---|
| 95 | Synchronous telemedicine via real-time audio and video |
| 93 | Synchronous telemedicine via audio only |
| FQ | Audio-only telehealth service for mental health |
| GT | Telehealth via interactive audio and video (some Medicaid plans) |
Most commercial payers accept modifier 95. Some Medicaid plans still require GT. Medicare uses 95 for audio-video and FQ for audio-only mental health services.
Place of Service Codes for Telehealth
POS 02 indicates the patient was not at home during the telehealth visit. POS 10 indicates the patient was at home. The selection matters. Some payers reimburse differently for POS 02 vs POS 10. Medicare requires POS 10 when the patient receives telehealth services in their home.
CPT Code 98016 (Virtual Check-In)
CMS added code 98016 in 2025 for brief virtual check-ins between an established patient and provider. The check-in must not lead to a related E/M service within seven days or originate from a related E/M service in the prior seven days.
Final Reference: Codes Every Psychiatry Biller Should Know
| Code | Type | What It Covers |
|---|---|---|
| 90791 | Diagnostic eval | Intake assessment, no medical services |
| 90792 | Diagnostic eval | Intake assessment with medical services |
| 90832 | Psychotherapy | 30 minutes |
| 90834 | Psychotherapy | 45 minutes |
| 90837 | Psychotherapy | 60 minutes |
| 90833 | Add-on | 30 min therapy with E/M |
| 90836 | Add-on | 45 min therapy with E/M |
| 90838 | Add-on | 60 min therapy with E/M |
| 90839 | Crisis | First 60 minutes of crisis therapy |
| 90840 | Crisis add-on | Each additional 30 minutes |
| 90785 | Add-on | Interactive complexity |
| 90846 | Family | Family therapy without patient |
| 90847 | Family | Family therapy with patient |
| 90853 | Group | Group psychotherapy |
| 96130 | Testing | Psychological testing evaluation |
| 96132 | Testing | Neuropsychological testing evaluation |
| 96127 | Screening | Brief emotional or behavioral assessment |
| 90867 | TMS | Initial TMS treatment |
| 90868 | TMS | Subsequent TMS treatment |
| 90870 | ECT | Electroconvulsive therapy |
| 99492 | CoCM | Initial collaborative care |
| 99493 | CoCM | Subsequent collaborative care |
| 99494 | CoCM | Collaborative care add-on |
| 99484 | BHI | Behavioral health integration |
| G2211 | Complexity | E/M complexity add-on |
| G2214 | CoCM | Brief collaborative care |
| 99213 | E/M | Established patient, low complexity |
| 99214 | E/M | Established patient, moderate complexity |
| 99215 | E/M | Established patient, high complexity |
Accurate psychiatry CPT coding is one of the highest-leverage points in the behavioral health revenue cycle. The code set is small, the rules are precise, and the financial impact of getting it right compounds across every claim a practice submits.
Key Modifiers for Psychiatry CPT Coding
Modifiers carry as much weight as the base CPT code. The wrong modifier sends a claim for denial. The right modifier defends a clean payment.
| Modifier | Purpose | Common Use |
|---|---|---|
| 25 | Significant, separately identifiable E/M | E/M + psychotherapy add-on same day |
| 59 | Distinct procedural service | When NCCI edits flag bundling |
| 95 | Synchronous telehealth | Most commercial telehealth claims |
| FQ | Audio-only mental health telehealth | Medicare audio-only sessions |
| 93 | Synchronous audio-only | Some commercial audio-only claims |
| GT | Interactive audio-video telehealth | Older Medicaid telehealth |
| 26 | Professional component | Testing or imaging interpretation |
| 52 | Reduced services | Service partially completed |
Apply only the modifiers required by the specific payer for the specific service. Layering unnecessary modifiers can trigger an audit as quickly as missing required ones.
Top Audit Risks and Denial Patterns in Psychiatry Billing
Psychiatry billing carries some of the highest payer scrutiny in outpatient medicine. Auditors look for specific patterns. The following list reflects the most common audit and denial triggers reported across MACs and commercial payers in 2025 and 2026.
Highest-Risk Audit Patterns
- 90837 over-billing without clear time documentation across a high percentage of total claims
- Modifier 25 misuse when the E/M and psychotherapy elements are not separately documented
- Identical progress notes copied across sessions, also called note cloning
- Time documentation gaps where start and stop times are missing from the note
- Diagnosis-code mismatch where the ICD-10 does not support the CPT billed
- Unbundling by billing 90791 and 90832 on the same day for the same patient
- Telehealth modifier errors where the wrong modifier is applied to the platform used
- G2211 documentation gaps that do not establish longitudinal care
- Crisis code billing without documentation of an acute crisis presentation
- Add-on codes without primary codes that auto-deny on submission
Most audit denials are preventable with structured documentation templates and pre-claim coding validation.
2026 Medicare Reimbursement Rates for Top Psychiatry CPT Codes
The 2026 Medicare conversion factor is $33.59, up 3.7% from the 2025 conversion factor of $32.35. Actual rates vary by geographic locality through the GPCI adjustment, by setting (facility vs non-facility), and by provider type.
| Code | Description | 2026 Medicare Rate (Non-Facility, National Avg) |
|---|---|---|
| 90791 | Diagnostic evaluation, no medical services | ~$195 |
| 90792 | Diagnostic evaluation with medical services | ~$220 |
| 90832 | Psychotherapy, 30 min | ~$76 |
| 90834 | Psychotherapy, 45 min | ~$103 |
| 90837 | Psychotherapy, 60 min | ~$152 |
| 90833 | Psychotherapy add-on, 30 min | ~$66 |
| 90836 | Psychotherapy add-on, 45 min | ~$85 |
| 90838 | Psychotherapy add-on, 60 min | ~$120 |
| 90839 | Crisis psychotherapy, first 60 min | ~$165 |
| 90840 | Crisis psychotherapy, each additional 30 min | ~$80 |
| 99213 | E/M established, low complexity | ~$91 |
| 99214 | E/M established, moderate complexity | ~$129 |
| 99215 | E/M established, high complexity | ~$183 |
| G2211 | Complexity add-on | ~$16 |
Commercial payers typically reimburse 120% to 250% of Medicare for behavioral health. State Medicaid rates vary widely. If a commercial payer is offering below 120% of the current Medicare for a high-volume code, that is documented grounds for contract renegotiation.
Documentation Requirements That Hold Up Under Audit
Every payer’s audit defense playbook starts and ends with documentation. The note must justify the code billed. Generic templates and AI-generated text without clinician review are flagged faster than ever.
What Every Psychiatry Note Should Contain
- Patient identifier and date of service
- Start and stop time of the encounter and of the psychotherapy portion
- Mode of service: in-person, audio-video telehealth, or audio-only
- Chief concern and current symptoms
- Mental status examination findings
- Medication review and any prescription changes
- Risk assessment with safety planning when relevant
- Therapy modality used and specific interventions delivered
- Patient response to interventions
- Updated treatment plan with measurable goals
The Split-Note Structure for E/M Plus Psychotherapy
When billing an E/M code with a psychotherapy add-on, the note should clearly be split into two sections: one for the E/M component, one for the psychotherapy component. The auditor needs to see the boundary.
The E/M section covers the medical visit elements: history, exam, medication management, and MDM. The psychotherapy section covers the modality, interventions, time, and clinical progress. A note that blends these into a single paragraph invites a modifier 25 denial.
Common Coding Errors That Trigger Denials
Most denials in psychiatry billing trace back to a small set of repeated errors. The list below captures the patterns that account for the majority of preventable rework.
- Billing 90837 without documenting at least 53 minutes of face-to-face psychotherapy
- Billing 90791 and 90792 on the same date for the same patient
- Missing modifier 25 on an E/M code billed with a psychotherapy add-on
- Using POS 11 (office) for a telehealth session
- Billing a psychotherapy add-on without a primary E/M code on the claim
- Applying modifier 95 to an audio-only session that requires FQ instead
- Selecting an E/M level by MDM when time would support a higher level
- Forgetting the brief screening code 96127 when validated instruments were used
- Billing 90785 without a documented communication complexity factor
- Using a generic ICD-10 like F32.9, when a more specific code is supported
Each of these errors is preventable with pre-claim coding validation, clinician training, and structured note templates aligned to the codes most commonly billed.
How Technology Reduces Coding Errors in Psychiatry
Most psychiatric practices and behavioral health networks now run pre-claim coding logic inside their EHR or revenue cycle platform. The pattern that produces the cleanest outcomes pairs three layers. Implementing specialized EMRs for psychiatry billing allows practices to inject these algorithmic defenses right at the point of care before a provider ever signs a chart note.
The Three-Layer Coding Validation Stack
- Real-time clinician prompts that flag missing time stamps, missing modality, or missing modifier 25 before the note is signed
- Pre-submission claim scrubbing that catches code combinations the payer will deny, including NCCI edits and bundling errors
- Post-submission denial intelligence that identifies repeat denial patterns by code, payer, and clinician
This stack reduces denial rates by 30% to 60% in most psychiatric and behavioral health groups that adopt it. The reduction is highest in groups that previously relied on coder review after the note was signed.
Where Agentic AI Now Plays a Role
Agentic AI workflows in 2026 are pulling on three coding tasks: time-based code selection, modifier validation, and ICD-10 specificity checks. The agent reviews the signed note, recommends the code set, flags documentation gaps, and routes any unresolved items back to the clinician or coder before the claim ships. Practice administrators can pair these automated systems with a structured guide to psychiatry billing to build a unified compliance framework for both artificial intelligence and human coders.
For psychiatric practices and behavioral health groups managing high claim volume across multiple payers, this workflow now produces material improvements in first-pass claim acceptance and net collection rate.
Frequently Asked Questions
What is the most common CPT code billed in outpatient psychiatry?
99214 paired with 90833 is the most common pattern for psychiatrists managing established patients with moderate complexity. The combination represents a 30 to 39 minute medical visit with a 16 to 37 minute therapy component on the same date.
Can a psychiatrist bill 90791?
A psychiatrist can technically bill 90791 if no medical services are delivered. In practice, psychiatrists almost always include medical service elements and should bill 90792 instead. Billing 90791 when 90792 was clinically delivered underbills the service.
How is 90791 different from 90792?
90791 is a psychiatric diagnostic evaluation without medical services. 90792 is the same evaluation with medical services included, like medication management and physical exam elements. Only providers qualified to deliver medical services can bill 90792.
What is the difference between 90834 and 90837?
90834 covers 38 to 52 minutes of psychotherapy. 90837 covers 53 minutes or more. The midpoint rule applies. A 50-minute session is 90834. A 53-minute session is 90837. Document exact start and stop times.
How often can 90791 be billed for the same patient?
90791 is typically billed once per episode of care. Some payers allow a second 90791 if the patient returns after an extended gap in treatment or presents with a new and distinct clinical concern. Always verify payer-specific frequency limits.
What is 99214 for psychiatry?
99214 is the established patient E/M code for moderate medical decision-making or 30 to 39 minutes total time on the date of service. Psychiatrists use it for routine medication management visits with established patients.
Can psychotherapy and E/M codes be billed on the same day?
Yes. Bill the E/M code with modifier 25, then add the psychotherapy add-on code (90833, 90836, or 90838) for the therapy portion. The note must clearly separate the E/M and psychotherapy elements.
What modifier is used for psychiatry telehealth in 2026?
Modifier 95 is used for synchronous audio-video telehealth. Modifier FQ is used for audio-only mental health telehealth under Medicare. Modifier 93 is used for audio-only services under some commercial payers.
What is CPT code 90785 used for?
90785 is an add-on code for interactive complexity. It captures sessions where communication factors complicate care delivery, like the need for an interpreter, third-party involvement, or mandated reporting decisions.
What is G2211 in psychiatry?
G2211 is a complexity add-on for E/M services. As of January 2025, it can be billed with an E/M code carrying modifier 25 when the psychiatrist is the principal clinician managing the patient’s complex, longitudinal psychiatric care.






