CPT code 31579 is a diagnostic laryngoscopy code used to report flexible or rigid telescopic laryngoscopy performed with stroboscopy during the same encounter. It applies when a qualified provider visualizes the larynx using a telescopic instrument while employing stroboscopic light to assess vocal fold vibration, mucosal wave patterns, and glottic closure. This code is used primarily in otolaryngology and laryngology outpatient settings for the evaluation of voice disorders, vocal fold pathology, and other laryngeal conditions requiring dynamic assessment beyond standard laryngoscopy.
What Is the Description of CPT Code 31579?
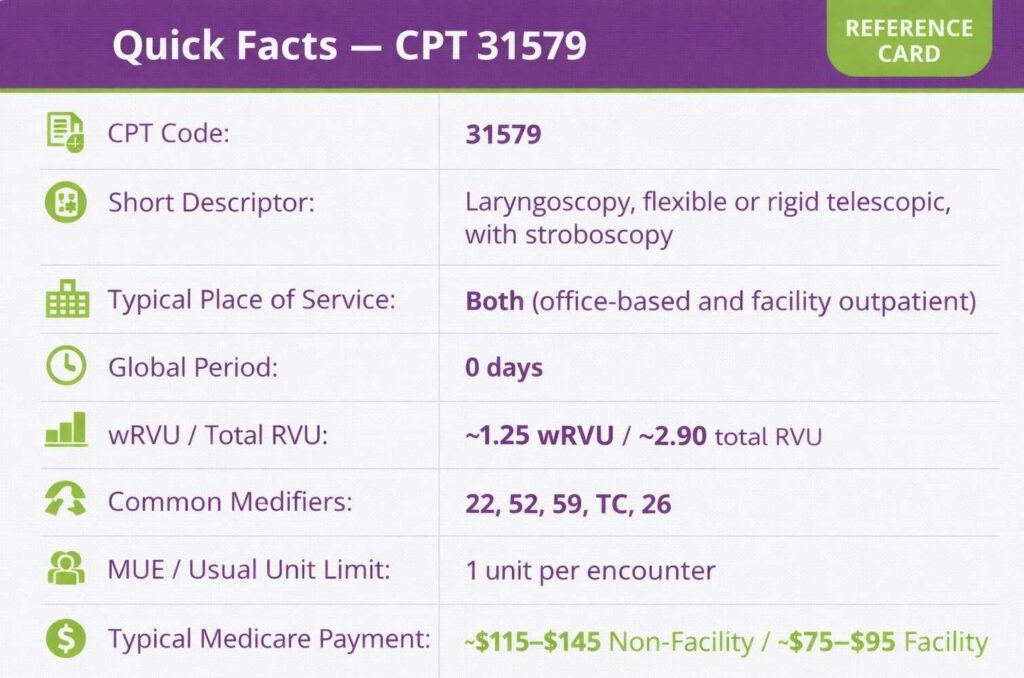
CPT 31579 code is defined by the AMA as: “Laryngoscopy, flexible or rigid telescopic, with stroboscopy.”
This code reports a diagnostic procedure in which the provider performs laryngoscopy using either a flexible fiberoptic or rigid telescopic instrument in combination with stroboscopic illumination during the same session. The stroboscopic component is not incidental; it is a required and integral element of the service.
What Equipment and Technique Are Required for CPT Code 31579?
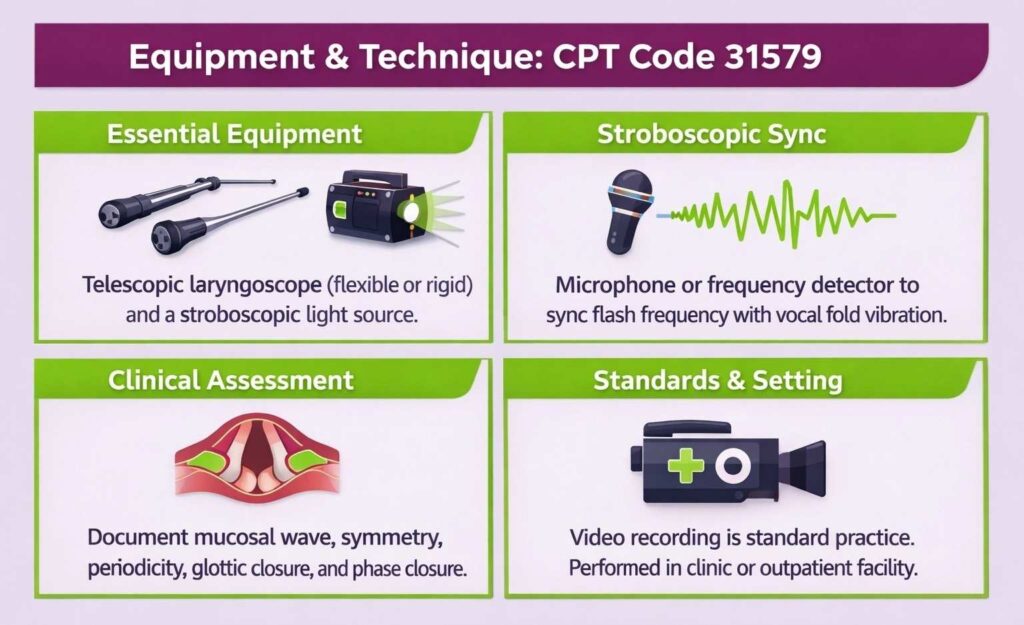
31579 CPT code requires the use of a telescopic laryngoscope, either flexible or rigid, along with a stroboscopic light source capable of synchronizing flash frequency to the patient’s vocal fold vibration cycle. A rigid laryngoscope is typically introduced transorally, while a flexible laryngoscope is passed transnasally to reach the larynx. The stroboscopic unit must be connected to a microphone or frequency detector that captures the patient’s fundamental frequency and modulates the strobe accordingly.
The provider must actively assess and document vocal fold vibratory behavior, including mucosal wave amplitude, symmetry, periodicity, glottic closure pattern, and phase closure. A recorded video of the stroboscopic examination is standard practice and supports documentation of findings. The procedure is performed by or under the direct supervision of a qualified provider, typically an otolaryngologist or laryngologist, in an appropriately equipped clinic or outpatient facility.
What Are the Modifiers for CPT Code 31579?
Code CPT 31579 can be reported with specific modifiers to reflect special circumstances, component billing, or service distinctions. Common modifiers include 22, 52, 59, TC, and 26.
Modifier 22: Increased Procedural Services
Modifier 22 is used when the work required to perform CPT code 31579 is substantially greater than typically required. This may apply when a patient’s anatomy, uncooperative reflexes, or complex pathology significantly prolongs the procedure or increases the level of skill and effort involved.
Modifier 52: Reduced Services
Modifier 52 is used when the 31579 CPT code is partially performed, and the service rendered is less than what is typically described by the code. This may occur when stroboscopic assessment is initiated but cannot be completed due to patient intolerance or equipment limitation.
Modifier 59: Distinct Procedural Service
Modifier 59 is used when CPT code 31579 is performed as a distinct and separate procedure from another service billed on the same date. It overrides NCCI bundling edits when documentation confirms the procedures were separate in indication, site, or session.
Modifier TC: Technical Component
Modifier TC is appended to CPT code 31579 when the billing entity is reporting only the technical component of the service, that is, the equipment, supplies, and technical staff involved in performing and recording the laryngostroboscopy. This modifier is used when the professional interpretation is billed separately by a different provider or group.
Modifier 26: Professional Component
Modifier 26 is used when the provider is billing only for the professional interpretation and report of the laryngostroboscopic examination, separate from the technical component. This applies in settings where the facility or a separate entity owns and operates the equipment. Billing both modifier 26 and modifier TC for the same service by the same entity constitutes duplicate billing.
Which Documents Are Required For CPT Code 31579?
Documentation for the CPT 31579 code must support the medical necessity of stroboscopic laryngoscopy and capture the specific findings observed during the examination.
Required documents checklist:
- Physician order or referral indicating an indication for laryngostroboscopy
- History of presenting complaint, including voice symptoms, duration, and prior treatments
- Description of instrument used (flexible vs. rigid telescopic laryngoscope)
- Confirmation that stroboscopy was performed and active stroboscopic parameters assessed
- Detailed findings documenting vocal fold vibratory characteristics — mucosal wave, closure pattern, symmetry, and periodicity
- Recorded video of the stroboscopic examination (standard of care and supports audit defense)
- Clinical impression and interpretation of findings
- Plan of care or next steps based on examination results
- Patient consent if applicable under payer or facility policy
- Provider signature with date and time of service
- Accurate place-of-service designation (office vs. facility) corresponding to where the procedure was performed
What is the Cost of CPT Code 31579?
The cost of code 31579 CPT varies by payer, geographic location, and place of service.
RVUs & Medicare Payment
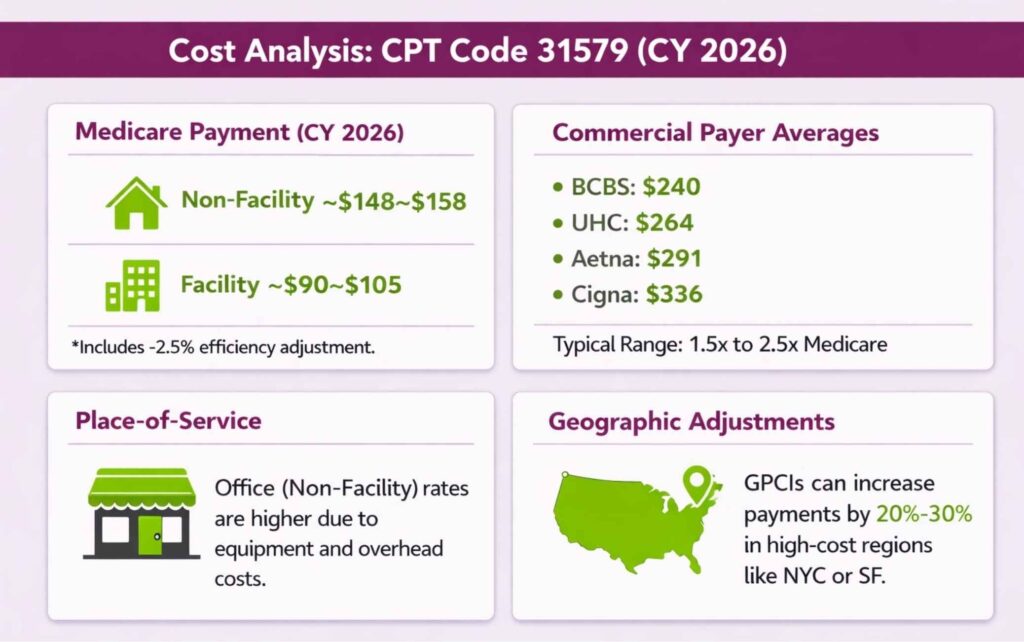
CPT code 31579 carries approximately 2.26 work RVUs and a total RVU ranging from 3.90 to 4.30, depending on place of service and dataset year. For CY-2026, the non-facility national Medicare payment is approximately $148 to $158, and the facility payment is approximately $90 to $105.
Note that CPT 31579 is subject to the CY-2026 efficiency adjustment of –2.5% applied to work RVUs for non-time-based diagnostic procedures, which modestly reduces its valuation relative to prior years.
Commercial Payers
Commercial payers negotiate rates that typically exceed Medicare by 1.5× to 2.5×. National average commercial reimbursement for CPT code 31579 ranges from approximately $240 to $335, depending on the payer and contract terms. Rates vary considerably: BCBS averages near $240, UHC near $264, Aetna near $291, and Cigna near $336 at the national level.
Place-of-Service & Geographic Adjustments
Non-facility (office) rates are significantly higher than facility rates for the CPT 31579 code, given the equipment and overhead costs associated with running a stroboscopy unit in-office. The non-facility rate reflects these direct practice expenses, while the facility rate assumes the institution absorbs equipment and supply costs. High-cost localities such as New York City or San Francisco can increase Medicare payment, with payment differentials between high- and low-cost areas reaching 20 to 30 percent for the same code.
What Are Example Clinical Scenarios or Use Cases for CPT Code 31579?
CPT code 31579 is used in outpatient settings when stroboscopic assessment of vocal fold vibration is clinically necessary to evaluate, diagnose, or monitor laryngeal pathology.
Scenario 1: Persistent Hoarseness in a Voice-Dependent Professional
ICD-10: R49.0 (Dysphonia)
A professional singer presents with persistent hoarseness and vocal fatigue lasting six weeks, unresponsive to voice rest and hydration. Flexible telescopic laryngoscopy with stroboscopy is performed to assess mucosal wave pattern, glottic closure, and vibratory symmetry. Stroboscopic findings reveal a subtle mucosal wave disruption at the mid-membranous vocal fold, supporting a diagnosis of early vocal fold lesion and guiding further management decisions.
Scenario 2: Suspected Laryngeal Lesion in a Chronic Smoker
ICD-10: J38.1 (Polyp of vocal cord and larynx)
A long-term smoker presents with progressive hoarseness and a sensation of throat fullness. The otolaryngologist performs rigid telescopic laryngoscopy with stroboscopy to characterize the lesion’s vibratory behavior and differentiate between a benign polyp and early mucosal pathology requiring biopsy. Stroboscopic evaluation reveals a unilateral mass with the absence of a mucosal wave on the affected fold, informing the decision to proceed with surgical intervention.
Scenario 3: Chronic Laryngitis with History of Alcohol and Tobacco Use
ICD-10: J37.0 (Chronic laryngitis)
A patient with a combined history of alcohol and tobacco use presents with ongoing vocal roughness, intermittent voice breaks, and throat clearing over several months. Flexible laryngoscopy with stroboscopy is performed to assess the degree of mucosal involvement and differentiate chronic inflammatory changes from structural pathology. Stroboscopy demonstrates reduced mucosal wave amplitude bilaterally with irregular vibratory closure, consistent with diffuse chronic laryngitis.
What Are the CPT Code 31579 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for documentation, coding, bundling, units, and frequency. Meeting these rules reduces denials and ensures correct payment.
Bundling / NCCI / Same-Day Procedure Rules
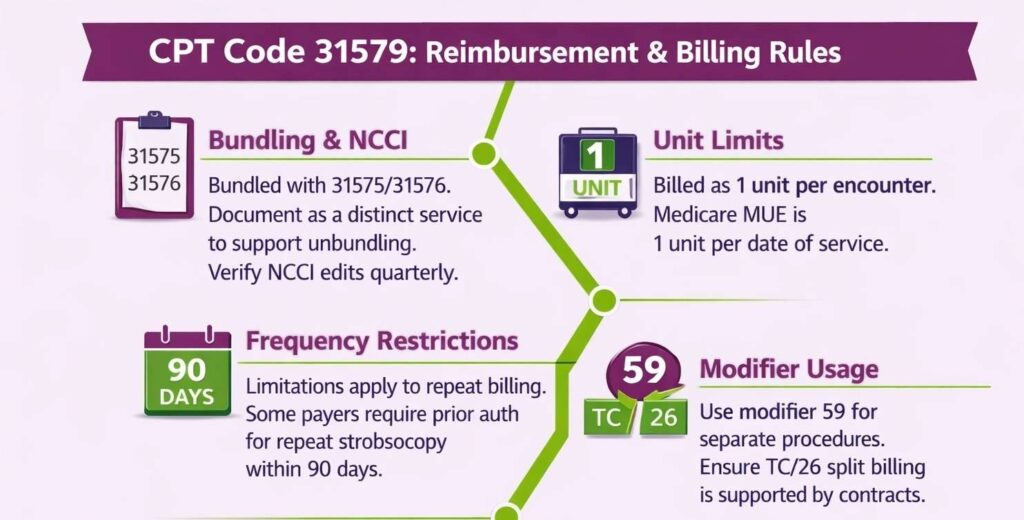
CPT code 31579 has NCCI bundling relationships with other laryngoscopy codes, particularly 31575 (flexible diagnostic laryngoscopy) and 31576 (flexible laryngoscopy with biopsy). When 31579 is billed on the same date as a related laryngoscopy or endoscopic procedure, payers may bundle the services and deny 31579 as inclusive.
The stroboscopic component must be documented as a distinct and separately indicated service to support unbundling. Use modifier 59 only when clinical documentation confirms the procedures were separate in purpose or technique. Always verify active NCCI pair edits for 31579 prior to submission, as these are updated quarterly.
Units, MUEs & Frequency Rules
The CPT 31579 code is billed as 1 unit per encounter. Billing multiple units on the same date by the same provider will be rejected at the clearinghouse or denied by the payer.
- Medicare’s Medically Unlikely Edit (MUE) for CPT 31579 is 1 unit per date of service per provider. Exceeding this limit triggers an automatic denial.
- Payers may apply frequency limitations restricting how often 31579 can be billed within a defined period. Some commercial contracts require prior authorization for repeat stroboscopy within 90 days.
- When billing with modifier TC or 26, ensure the split billing arrangement is supported by the practice’s contract and that the same entity does not bill the global service simultaneously.
Top Reasons For Denials Specific To 31579 & Quick Remedies
- Bundled With Standard Laryngoscopy (No Modifier 59): Prevent by documenting that stroboscopy was performed as a distinct service with a separate clinical indication and applying modifier 59 where NCCI edits apply.
- Stroboscopy Not Documented as Performed: Prevent by explicitly stating in the procedure note that stroboscopic illumination was used, vibratory parameters were assessed, and findings were interpreted.
- Medical Necessity Not Supported: Prevent by linking the diagnosis code directly to the clinical need for stroboscopic evaluation, particularly when differentiating benign from malignant pathology or assessing functional voice disorders.
- Frequency Denial on Repeat Billing: Prevent by obtaining prior authorization when required and documenting the clinical rationale for repeat stroboscopy within a short interval.
How Do Coders Decide Between CPT 31579 and Other Laryngoscopy Codes?
The deciding factor is whether stroboscopy was performed and distinctly documented alongside the laryngoscopy. Without it, a different laryngoscopy code applies. This kind of code-level decision reflects the broader CPT code selection process, where procedure specificity, documented technique, and clinical intent together determine which code is the correct and defensible choice.