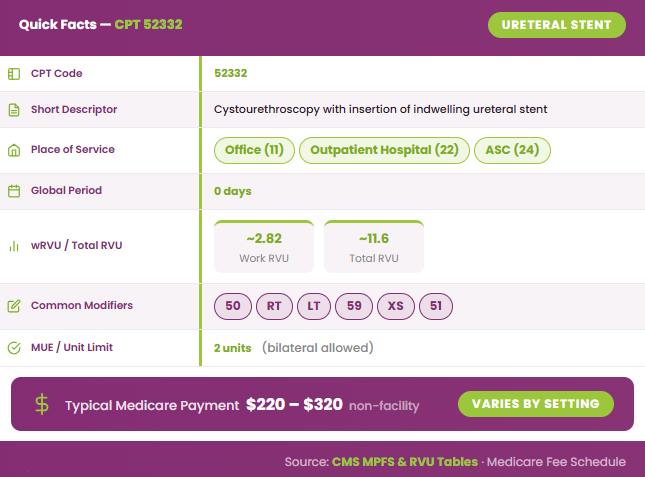
CPT 52332 is a urology procedure code used to report cystourethroscopy with insertion of an indwelling ureteral stent. It is commonly billed when a provider relieves ureteral obstruction, maintains urine flow, or protects the ureter during surgical care. This code is frequently used in cases involving kidney stones, strictures, or preoperative planning for complex pelvic surgeries.
What Is the Description of CPT Code 52332?
CPT 52332 code description, according to the American Medical Association, is:
“Cystourethroscopy, with insertion of an indwelling ureteral stent (e.g., double-J stent).” This descriptor identifies an endoscopic procedure in which a stent is placed into the ureter via cystoscopic guidance. It is typically selected for cases requiring relief of ureteral obstruction, maintenance of urine flow, or prophylactic ureteral protection during surgery.
What Equipment and Technique Are Required for CPT Code 52332?
CPT 52332 requires the use of a cystoscope along with guidewires and appropriate ureteral stents (e.g., double-J stent). Fluoroscopy or imaging equipment may be used to confirm proper stent placement, especially in complex cases.
The cystoscope is introduced transurethrally to access the bladder, and the ureteral orifice is identified. A guidewire is passed into the ureter, and the stent is advanced over the wire to position it between the kidney and bladder. Proper placement is confirmed visually and, if needed, with fluoroscopic guidance.
The provider must actively document ureteral anatomy, stent position, insertion technique, and any immediate complications. The procedure is performed by or under the direct supervision of a qualified provider, typically a urologist, in an appropriately equipped office, ambulatory surgical center, or outpatient facility.
How Does CPT Code 52332 Differ From CPT 52005, 52310, and 52356?
To clearly understand billing and coding distinctions, the following table compares CPT 52332 with related ureteral procedure codes:
| CPT Code | Short Description | What the Code Covers | Main Difference From 52332 |
|---|---|---|---|
| 52332 | Cystourethroscopy with insertion of indwelling ureteral stent | Endoscopic placement of a ureteral stent to maintain drainage | Base code for stent insertion |
| 52005 | Cystourethroscopy with ureteral catheterization | Diagnostic or access catheter placement into the ureter | No indwelling stent is left in place |
| 52310 | Cystourethroscopy with removal of ureteral stent | Endoscopic removal of a previously placed stent | Removal only, not insertion |
| 52356 | Ureteroscopy with lithotripsy and stent insertion | Ureteroscopy for stone treatment, often with stent placement included | Includes stone treatment, so stent placement is usually bundled |
What are the Modifiers for CPT Code 52332?
CPT 52332 may require modifiers to indicate laterality, multiple procedures, or distinct services.
Modifier 50: Bilateral Procedure
Used when stents are inserted in both ureters during the same session. Follow payer-specific rules for billing format (single vs dual line).
Modifier LT: Left Side Procedure
Indicates stent placement in the left ureter. Must be supported by operative documentation.
Modifier RT: Right Side Procedure
Indicates stent placement in the right ureter. Documentation must clearly identify laterality.
Modifier 59: Distinct Procedural Service
Used when the procedure is separate from another service typically bundled. Documentation must prove independence.
Modifier XS: Separate Structure
Used when procedure is performed on a different anatomical structure. Preferred over modifier 59 when applicable.
Modifier 51: Multiple Procedures
Used when multiple procedures are performed in the same session. Typically appended to secondary procedures.
Which Documents Are Required For CPT Code 52332?
Proper documentation is crucial for CPT 52332 to justify medical necessity, confirm procedure details, and ensure accurate reimbursement.
Required Documents for CPT 52332:
- Detailed operative report describing stent insertion
- Clinical indication for the procedure (e.g., obstruction, stricture, prophylactic use)
- Laterality (right, left, or bilateral)
- Technique used (cystoscopy, guidewire placement, fluoroscopy if applicable)
- Confirmation of successful stent placement
- Any additional procedures performed during the same session
- Post-procedure plan and follow-up instructions
- Physician signature and date
- ICD-10 diagnosis linked to the procedure for medical necessity
What is the Cost of CPT Code 52332?
To accurately determine the cost of the CPT 52332 code, it’s important to evaluate reimbursement across key billing factors.
RVUs & Medicare Payment
CPT 52332 has an approximate work RVU of 2.82 and a total RVU of 11.6, depending on the setting. Applying the CMS conversion factor and geographic practice cost index (GPCI), the national Medicare payment typically ranges from $220 to $320. These figures reflect physician effort, practice expense, and malpractice considerations.
Commercial Payers
Reimbursement from commercial insurers varies widely based on contracts and region. Payments for CPT 52332 generally fall between 120% and 180% of Medicare rates, though some plans may require prior authorization, particularly for elective or non-urgent stent placements.
Place-of-Service & Geographic Adjustments
The place of service impacts physician reimbursement significantly. Procedures performed in facility settings, such as hospitals or ASCs, usually result in lower physician payment, with the facility billing separately. Conversely, non-facility settings like offices or outpatient clinics often allow higher physician reimbursement. Geographic Practice Cost Indices (GPCIs) further adjust payment based on local costs of delivering care.
What Are Example Clinical Scenarios or Use Cases for CPT Code 52332?
CPT 52332 is used when ureteral stent placement is medically necessary to maintain or restore urine flow. It applies to a variety of clinical situations where obstruction, stricture, or surgical planning requires temporary ureteral support.
Scenario 1: Ureteral Obstruction Following Kidney Stone Surgery
After kidney stone removal, a patient develops ureteral swelling or partial blockage. A stent is inserted to restore urine flow, relieve obstruction, and prevent complications such as hydronephrosis, supporting the use of CPT 52332.
Scenario 2: Ureteral Stricture Causing Partial Obstruction of Urine Flow
A patient presents with a ureteral stricture restricting urine drainage from the kidney to the bladder. Placement of an indwelling stent ensures patency and symptom relief, justifying CPT 52332.
Scenario 3: Prophylactic Stent Placement Prior to Complex Pelvic Surgery
Before a major pelvic surgical procedure, a stent may be placed to identify and protect the ureters. This prophylactic use prevents accidental ureteral injury during surgery and can be billed using CPT 52332 if it is not bundled with the primary procedure.
What Are the CPT Code 52332 Rules To Ensure Successful Reimbursement?
Proper adherence to coding rules, documentation, and payer guidelines is essential to ensure accurate reimbursement for CPT 52332. Providers must follow bundling rules, observe unit limits, and understand when the code cannot be reported separately.
Bundling / NCCI / Same-Day Procedure Rules
CPT 52332 is often bundled with ureteroscopy or stone treatment procedures. It should not be reported separately when included in a primary procedure. Modifier 59 or XS may be used only when documentation clearly supports a distinct and separate service. Always check NCCI edits and global surgery rules before billing.
Units, MUEs & Laterality Billing Rules
Most payers allow up to 2 units for bilateral stent placement. Use RT or LT modifiers for unilateral procedures and modifier 50 for bilateral cases if permitted. Always follow payer-specific rules regarding multiple procedures and laterality reporting.
When CPT 52332 Cannot Be Separately Reported and What to Use Instead?
CPT 52332 cannot be reported separately when stent placement is included in comprehensive procedures such as ureteroscopy with lithotripsy. In these cases, report only the primary procedure code, as the stent insertion is considered bundled into the main service.
Top Reasons For Denials Specific To 52332 & Quick Remedies
Missing Laterality or Incorrect Modifier Use: Ensure RT, LT, or 50 modifiers are properly applied and clearly documented in the operative report.
Denied as Bundled With Another Procedure: If 52332 is performed on the same day as ureteroscopy or lithotripsy, provide documentation showing that stent placement was a separate, distinct service. Use modifier 59 or XS when justified.
Insufficient Documentation of Medical Necessity: Clearly state the clinical indication (obstruction, stricture, prophylactic use), operative steps, and stent placement confirmation to support billing.
Incomplete Operative Report or Missing Stent Details: Include stent type, technique, guidewire use, confirmation of placement, and any complications to prevent downcoding or claim rejection.
Billing Bilateral Procedure Incorrectly: For bilateral stent placement, follow payer rules for modifier 50 vs separate line billing, and ensure MUE limits are not exceeded.
How do Providers Track these Specific Procedures?
Medical offices use CPT codes in medical billing to accurately record every step of the stent insertion process. This system helps insurance companies process payments quickly by using a universal language for healthcare services.