CPT code 33208 reports the insertion of a new or replacement permanent pacemaker system with transvenous electrodes placed in both the atrium and the ventricle during the same operative session. It applies when a pulse generator is implanted subcutaneously, and leads are advanced transvenously into both cardiac chambers.
This code is used exclusively in facility-based settings, hospital inpatient, hospital outpatient, or ambulatory surgical center, by electrophysiologists and cardiac surgeons managing bradyarrhythmias, conduction system disorders, and other indications meeting Medicare coverage criteria for permanent pacing.
What Is the Description of CPT Code 33208?
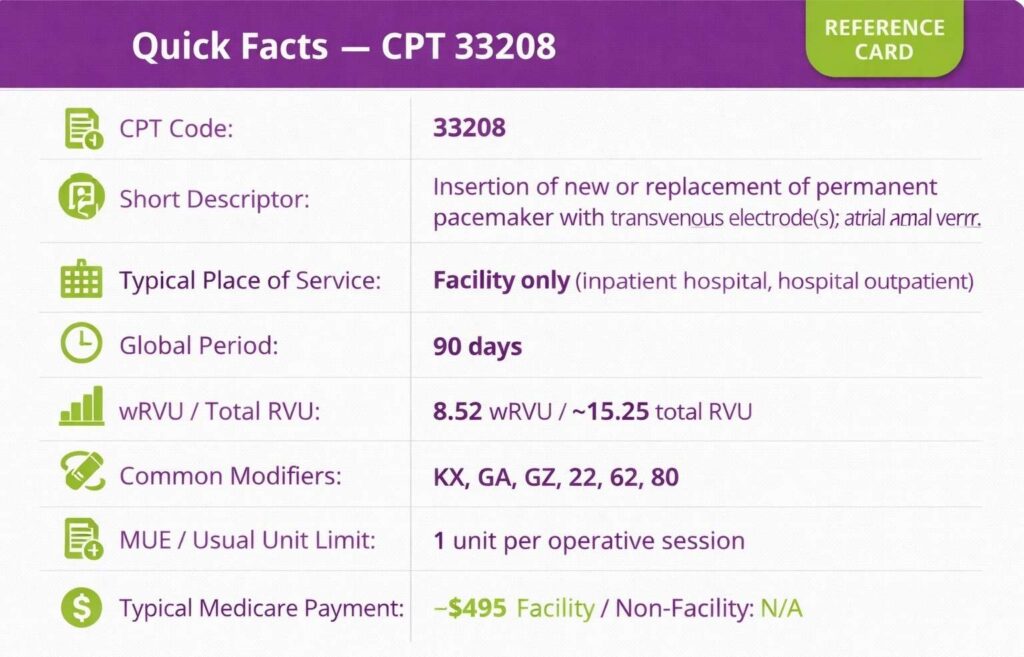
CPT 33208 code is defined by the AMA as: “Insertion of new or replacement of permanent pacemaker with transvenous electrode(s); atrial and ventricular.”
Among the cardiology CPT codes, this code covers the complete operative service of implanting a dual-chamber permanent pacing system in a single session, including insertion of the pulse generator into a subcutaneous or submuscular pocket and transvenous positioning of electrodes in both the right atrium and right ventricle.
What Does the Dual-Chamber Pacemaker System Include for CPT Code 33208?
33208 CPT code encompasses the pulse generator, the atrial electrode, and the ventricular electrode as a complete system implanted in one operative session. The work captured includes creation of the subcutaneous pocket, transvenous introduction of both leads under fluoroscopic guidance, lead testing and threshold assessment, generator connection and programming, and pocket closure.
Fluoroscopy and venous access used during the procedure are included and are not separately billable. Interrogation and programming performed at the time of implant are also bundled.
How Does CPT Code 33208 Differ From CPT Codes 33206 and 33207?
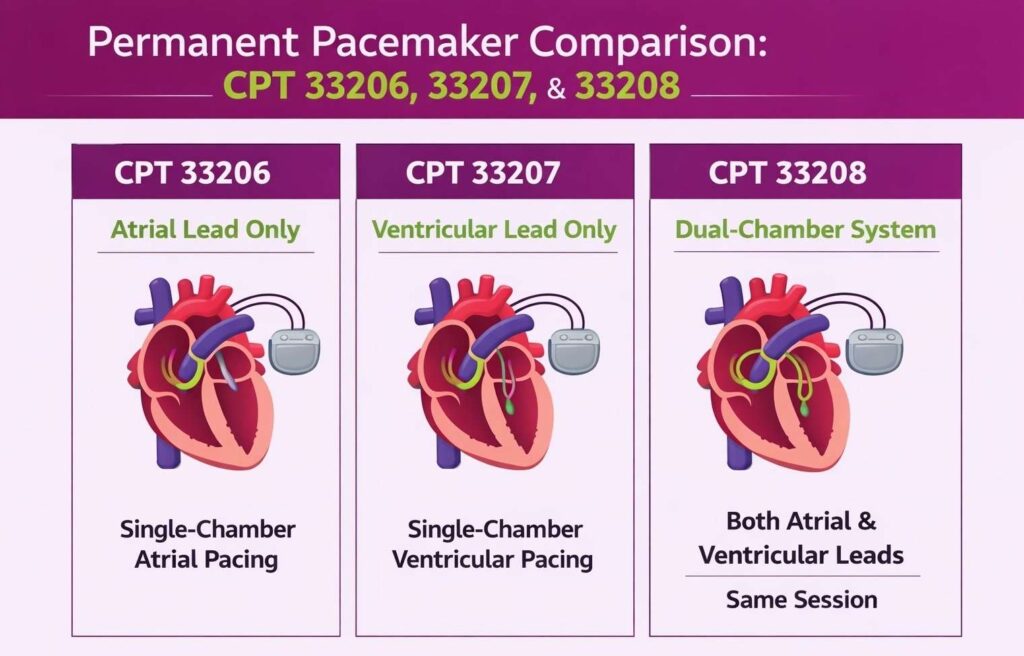
CPT 33206, 33207, and 33208 all describe permanent pacemaker insertion with transvenous electrodes but differ in the cardiac chambers paced. CPT 33206 covers atrial lead only (single-chamber atrial pacing). CPT 33207 covers ventricular lead only (single-chamber ventricular pacing). CPT 33208 covers both atrial and ventricular leads in the same session, the dual-chamber system.
What Are the Modifiers for CPT Code 33208?
Code 33208 CPT is reported with specific modifiers required by Medicare policy or to reflect special operative circumstances.
Modifier KX: Medical Necessity Requirements Met
Modifier KX is mandatory for Medicare billing of CPT 33208. CMS requires that KX be present on every claim for a permanent pacemaker (33206, 33207, 33208) to attest that the patient’s diagnosis meets Medicare coverage criteria. Claims submitted without the modifier KX will be returned as unprocessable.
Modifier GA: Waiver of Liability on File
Modifier GA is used when a service may be denied as not medically necessary, but a signed Advance Beneficiary Notice of Noncoverage (ABN) is on file. Apply modifier GA when the clinical indication is a diagnosis that CMS covers only at contractor discretion (e.g., certain conduction defects) and the provider has obtained a valid ABN from the patient.
Modifier GZ: Item or Service Expected to Be Denied
Modifier GZ is used when the provider expects Medicare to deny the service as not medically necessary, and no ABN has been obtained. Do not bill modifier GZ and modifier KX on the same claim, as they are mutually exclusive. GZ signals no ABN is on file, while KX attests that coverage criteria are met.
Modifier 22: Increased Procedural Services
Modifier 22 is used when the operative work required is substantially greater than typically described by CPT 33208. A detailed operative note explaining the nature and extent of additional work is required. Without supporting documentation, payers will deny or downward adjust the modifier 22 claim.
Modifier 62: Two Surgeons
Modifier 62 is used when two surgeons of different specialties each perform distinct portions of the pacemaker implant procedure as co-surgeons. Each surgeon bills 33208 with modifier 62. Both operative reports must document the respective roles and confirm that co-surgeon billing was medically necessary. Medicare pays each surgeon at 62.5% of the applicable fee schedule rate.
Modifier 80: Assistant Surgeon
Modifier 80 is used when a second physician assists the primary surgeon during CPT 33208. The assistant surgeon bills 33208 with modifier 80. Not all payers allow assistant surgeon billing for pacemaker implantation. So, confirm payer-specific policy before submission.
What Are the Medicare Coverage Criteria for CPT Code 33208?
Medicare covers CPT code 33208 when the patient’s clinical condition meets the indications for permanent dual-chamber pacing as outlined in the CMS National Coverage Determination (NCD 20.8) and applicable Local Coverage Determinations (LCDs). Covered indications include, but are not limited to:
- Symptomatic bradycardia due to sinus node dysfunction (sick sinus syndrome) not attributable to a reversible cause
- Second-degree or third-degree (complete) atrioventricular block, symptomatic or resulting in hemodynamic compromise
- Chronic bifascicular or trifascicular block with associated symptoms
- Hypersensitive carotid sinus syndrome with recurrent syncope
- Certain drug-refractory tachyarrhythmias where pacing is therapeutically indicated
Diagnosis R55 (syncope and collapse) alone is not a covered indication for CPT 33208, even when submitted with other covered diagnosis codes. Claims will be denied with CARC 96 when R55 is the only or primary supporting diagnosis. Modifier KX must accompany every claim, and the covered ICD-10 diagnosis must be documented in the medical record to withstand audit.
Which Documents Are Required For CPT Code 33208?
Documentation for CPT code 33208 must establish medical necessity, confirm dual-chamber system implantation, and satisfy Medicare’s KX modifier attestation requirements.
Required documents checklist:
- Operative report confirming insertion of both atrial and ventricular transvenous electrodes and pulse generator
- Pre-procedure evaluation documenting the clinical indication (diagnosis, symptoms, prior treatment, and diagnostic testing, including ECG, Holter, or electrophysiology study as applicable)
- ICD-10 diagnosis code matching a covered Medicare indication per NCD 20.8 and applicable LCD
- Signed Advance Beneficiary Notice (ABN) if the indication is discretionary under LCD
- Device implant card or log documenting generator model, serial number, and lead specifications
- Fluoroscopy report (included in procedure — not separately billed)
- Intraoperative lead threshold and sensing measurements
- Post-implant device programming documentation
- Modifier KX attestation on the claim
- Provider signature with date and time of service
- Accurate facility place-of-service designation (21 inpatient, 22 hospital outpatient, or 24 ASC)
What Is the Cost of CPT Code 33208?
The cost of CPT code 33208 to the physician varies by payer, geographic location, and place of service.
RVUs & Medicare Payment
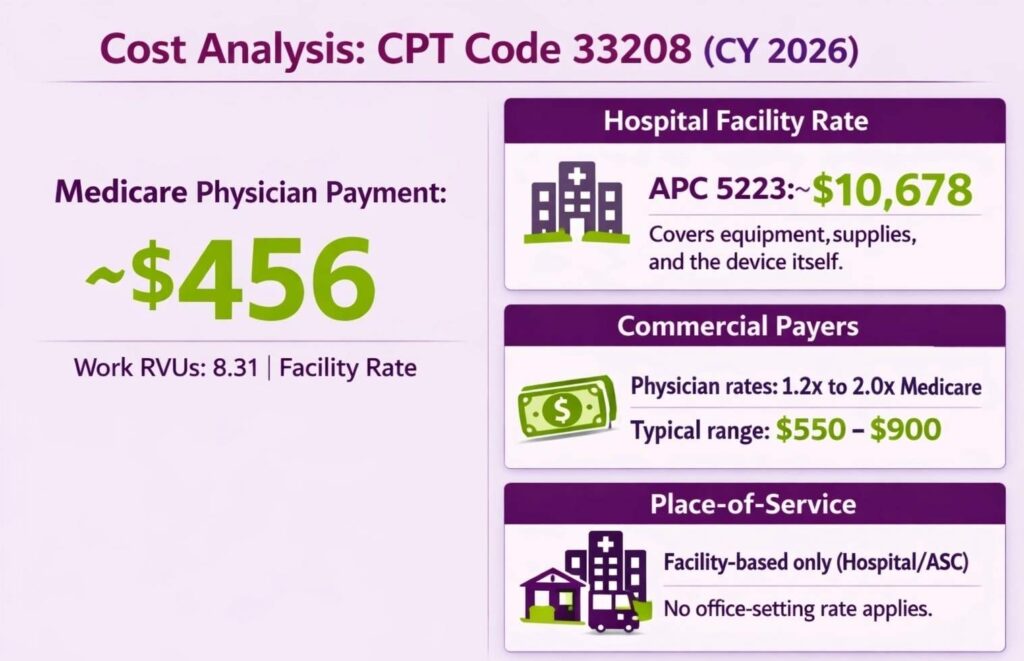
CPT code 33208 carries approximately 8.31 work RVUs for CY-2026, reflecting the base work RVU of 8.52 adjusted downward by the CMS –2.5% efficiency adjustment applied to surgical procedures under the 2026 PFS final rule. The CY-2026 national unadjusted Medicare physician payment is $456 (facility rate).
For hospital outpatient facility reimbursement, CPT 33208 is grouped under APC 5223, with a CY-2026 national unadjusted APC rate of $10,678, which covers the facility’s equipment, supplies, and technical staff costs, including the device itself.
Commercial Payers
Commercial payers negotiate physician rates that typically range from 1.2× to 2.0× Medicare’s facility rate for the CPT 33208 code, depending on the contract and the provider’s network status. Physician allowed amounts commonly range from $550 to $900 among major commercial payers, with significant variation by region and contract tier.
Place-of-Service & Geographic Adjustments
CPT 33208 carries only a facility-based payment rate. There is no office-setting rate. Procedures performed in a hospital inpatient setting are reimbursed under MS-DRG (inpatient), while hospital outpatient and ASC procedures are paid under the OPPS APC system.
What Are Example Clinical Scenarios or Use Cases for CPT Code 33208?
CPT code 33208 applies when a complete dual-chamber permanent pacemaker system is implanted transvenously, generator plus both atrial and ventricular electrodes, in a single operative session.
Scenario 1: Symptomatic Bradycardia Due to Sinus Node Dysfunction
ICD-10: I49.5 (Sick sinus syndrome)
A patient presents with recurrent fatigue, exertional presyncope, and documented resting heart rates below 40 bpm on Holter monitoring. Reversible causes have been excluded. The electrophysiologist implants a dual-chamber permanent pacemaker with transvenous atrial and ventricular leads to restore physiologic rate response and atrioventricular synchrony. CPT 33208 is reported with modifier KX, supported by the Holter findings and symptomatic documentation in the record.
Scenario 2: Complete Third-Degree Atrioventricular Block
ICD-10: I44.2 (Atrioventricular block, complete)
A patient presents with syncope and is found on ECG to have complete heart block with a ventricular escape rate of 32 bpm and no P-wave conduction. After stabilization with temporary pacing, the cardiac surgeon proceeds to permanent dual-chamber pacemaker implantation with transvenous atrial and ventricular leads. CPT 33208 is reported with modifier KX. The complete AV block diagnosis satisfies NCD 20.8 coverage criteria without requiring additional discretionary review.
Scenario 3: Second-Degree AV Block with Recurrent Syncope
ICD-10: I44.1 (Atrioventricular block, second degree)
A patient with symptomatic Mobitz Type II second-degree AV block presents with two documented syncopal episodes and evidence of progressive conduction system disease on electrophysiology study. Given the risk of progression to complete block, a dual-chamber permanent pacemaker is implanted. CPT 33208 is reported with modifier KX. The combination of Mobitz II morphology, syncopal episodes, and EP study findings supports medical necessity and satisfies LCD coverage criteria for permanent pacing.
What Are the CPT Code 33208 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for documentation, coding, bundling, global period, and coverage criteria. Meeting these rules reduces denials and ensures correct payment.
Bundling / NCCI / Same-Day Procedure Rules
CPT 33208 includes the pulse generator, both transvenous leads, fluoroscopic guidance, venous access, and intraoperative device evaluation as a global service. The following services are bundled into 33208 and are not separately billable on the same date:
- Fluoroscopy (76000), included per CPT guidelines
- Venous cutdown or percutaneous access for lead introduction
- Intraoperative pacemaker interrogation and programming at implant
- Temporary pacemaker insertion (33210) performed on the same date is subject to NCCI bundling.
When CPT 33208 is reported on the same day as a separately identifiable procedure, confirm NCCI pair edits and apply modifier 59 or the appropriate X-modifier only when documentation supports a distinct clinical service. Do not report 33206 or 33207 in addition to 33208 for the same session.
Units, MUEs & 90-Day Global Period Billing Rules
CPT 33208 is billed as 1 unit per operative session. Multiple units will be denied. CPT 33208 carries a 90-day global period, meaning all routine postoperative care is included in the surgical payment and is not separately billable during the 90-day window.
- Services unrelated to the pacemaker implant may be billed during the global period using modifier 24 (unrelated E/M during post-op period).
- Modifier 79 is used to report an unrelated procedure performed by the same physician during the global period.
- Modifier 78 applies when a return to the operating room for a complication related to the original pacemaker procedure occurs within the global period.
- Device follow-up programming and interrogation codes (93279, 93280, 93288) are separately billable after the implant.
Non-Covered Conditions and Exclusions Specific to CPT Code 33208
Medicare does not cover CPT 33208 for the following:
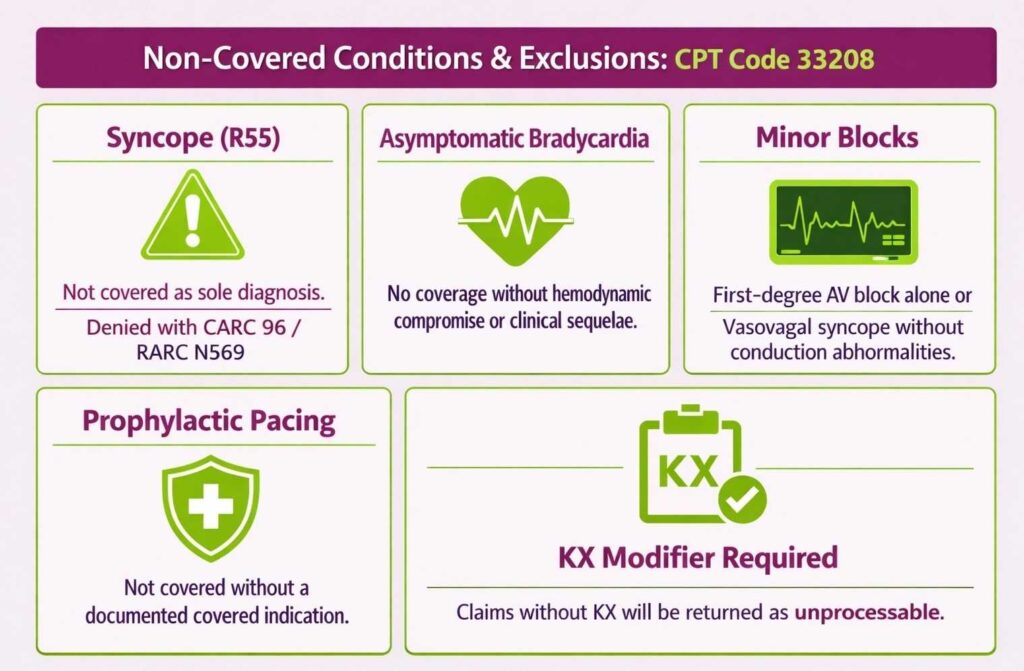
- Syncope (R55) as the sole or primary diagnosis, even when submitted alongside covered diagnoses, claims will be denied with CARC 96 / RARC N569.
- Asymptomatic sinus bradycardia without hemodynamic compromise or documented clinical sequelae
- First-degree AV block alone
- Vasovagal syncope without associated cardiac conduction abnormalities
- Prophylactic pacing without a documented covered indication
Claims submitted without the modifier KX, regardless of diagnosis, will be returned as unprocessable by the MAC.
Top Reasons For Denials Specific To 33208 & Quick Remedies
- Missing Modifier KX: Prevent by making modifier KX a mandatory billing edit for every 33208 claim before submission.
- Non-Covered ICD-10 Diagnosis (R55 Only): Prevent by verifying the claim carries at least one ICD-10 diagnosis from the NCD 20.8 or LCD covered list. R55 alone will not support coverage.
- Bundled Fluoroscopy or Temporary Pacing Billed Separately: Prevent by confirming that 76000 and same-day 33210 are not on the claim unless NCCI edits are properly addressed with modifier documentation.
- Global Period Violation. Post-Op E/M Billed Without Modifier: Prevent by applying modifier 24 to E/M services during the 90-day global period that address conditions unrelated to the pacemaker, with supporting documentation in the record.
Where Does CPT 33208 Fit Within the Full Range of Cardiac Device Codes?
CPT 33208 is one of several codes covering pacemaker implantation, each differentiated by chamber involvement and system type. Seeing how it sits alongside insertion, upgrade, and replacement codes gives a clearer picture of the full coding landscape. This is something best understood by reviewing the broader medical billing CPT code list, where cardiac device codes are organized by procedure category and complexity.
How can I Ensure Accuracy when billing for Complex Heart Procedures?
Partnering with professional cardiology billing services is the best way to ensure proper coding and maximum reimbursements for your practice. These experts stay updated on specific Medicare requirements, like the KX modifier, and help prevent common denials related to medical necessity.