Cardiology is one of the most code-heavy specialties in healthcare. Echocardiograms, stress tests, catheterizations, and device implants each carry their own CPT codes, modifier rules, and documentation requirements. CMS data shows that insufficient documentation is the single biggest driver of improper Medicare payments in cardiology medical billing.
A single wrong code, missing modifier, or incorrectly unbundled service can mean a denied claim or a payer audit. The stakes are high because cardiology procedures often involve multiple billable components in one patient encounter. Getting the coding right the first time is the billing best practice. Many practices achieve this by partnering with professional cardiology billing services to protect their revenue and ensure compliance.
This guide puts the most commonly used cardiology CPT codes and modifiers in one place. It also covers the coding-related denial reasons that come up most often in day-to-day cardiology billing. Use it as a daily reference to reduce errors, speed up submissions, and keep claims moving cleanly through the revenue cycle.
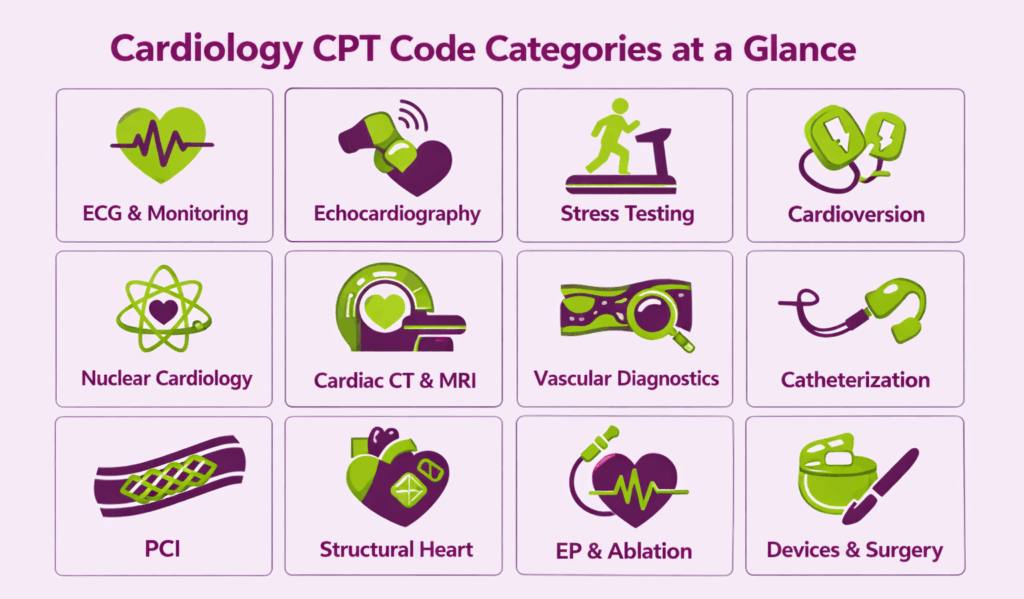
What are the Most Used Cardiology CPT Codes by Category?
Cardiology spans a wider range of procedures than most specialties, from a simple ECG to open heart surgery. The types of CPT codes used in cardiology reflect this range, grouped into service categories that follow how care is actually delivered. This section breaks those categories down so you can quickly find the right code for any service.
Which Codes Cover ECG and Ambulatory Cardiac Monitoring?
ECG and cardiac monitoring codes are among the most frequently billed in cardiology. They include the following categories, covering everything from a single 12-lead tracing done in the office to weeks of continuous remote monitoring.
Electrocardiography
The three ECG codes are split by component, which include:
| CPT Code | Description |
|---|---|
| 93000 | ECG, routine; with at least 12 leads, with interpretation and report |
| 93005 | ECG tracing only; without interpretation and report |
| 93010 | ECG interpretation and report only |
Rhythm Strip Interpretation
Rhythm strip codes cover single-channel or limited-lead tracings interpreted outside of a full 12-lead ECG.
| CPT Code | Description |
|---|---|
| 93040 | Rhythm ECG, 1–3 leads; with interpretation and report |
| 93041 | Rhythm ECG, 1–3 leads; tracing only, without interpretation and report |
| 93042 | Rhythm ECG, 1–3 leads; interpretation and report only |
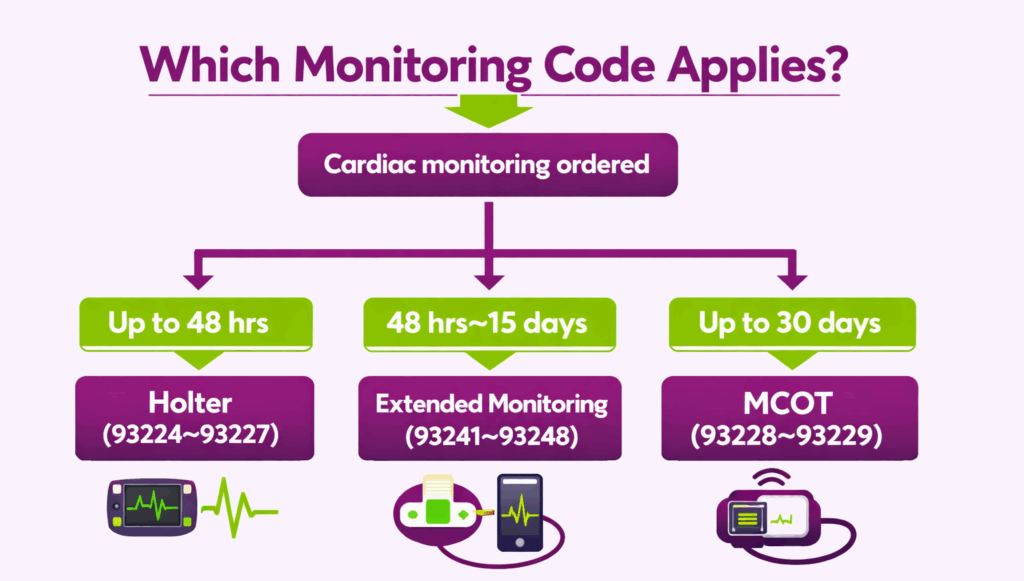
Holter Monitoring
Holter codes cover continuous external recording up to 48 hours and include the following:
| CPT Code | Description |
|---|---|
| 93224 | External ECG recording up to 48 hours; complete service |
| 93225 | Recording only (connection, recording, and disconnection) |
| 93226 | Scanning analysis with report only |
| 93227 | Physician review and interpretation only |
Extended External Cardiac Monitoring (2021 Restructured Codes)
In 2021, CMS restructured extended monitoring codes beyond 48 hours into two duration-based sets. The previous long-term monitoring codes (93268–93272) were deleted. The new ones are:
| CPT Code | Description |
|---|---|
| 93241 | Extended external ECG monitoring, 48 hours to 7 days; complete service |
| 93242 | 48 hours to 7 days; recording only |
| 93243 | 48 hours to 7 days; scanning analysis with report |
| 93244 | 48 hours to 7 days; physician review and interpretation |
| 93245 | Extended external ECG monitoring, more than 7 days to 15 days; complete service |
| 93246 | More than 7 days to 15 days; recording only |
| 93247 | More than 7 days to 15 days; scanning analysis with report |
| 93248 | More than 7 days to 15 days; physician review and interpretation |
| 93228 | Mobile cardiac outpatient telemetry (MCOT), up to 30 days; technical support |
| 93229 | MCOT; physician review and interpretation |
Which Codes Cover Echocardiography?
Echocardiography is one of the highest-volume and most denial-prone categories in cardiology billing. Code selection depends on the type of echo performed, which Doppler components were included, and the clinical context.
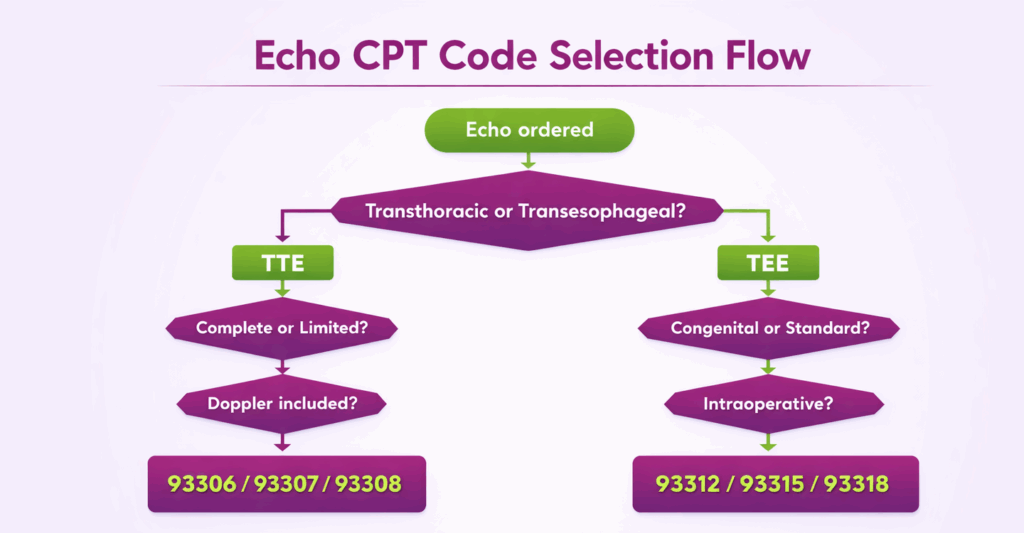
Transthoracic Echocardiography (TTE)
The base TTE code is selected based on whether the study was complete or limited, and whether Doppler was included. They include:
| CPT Code | Description |
|---|---|
| 93306 | TTE, complete; with spectral and color flow Doppler |
| 93307 | TTE, complete; without Doppler |
| 93308 | TTE, follow-up or limited study |
| 93303 | TTE for congenital cardiac anomalies; complete |
| 93304 | TTE for congenital cardiac anomalies; follow-up or limited |
| 93320 | Doppler echocardiography, pulsed wave and/or continuous wave (add-on) |
| 93321 | Doppler echocardiography, follow-up or limited study (add-on) |
| 93325 | Doppler color flow velocity mapping (add-on) |
Stress Echocardiography
Stress echo codes hinge on whether the supervising physician provided continuous ECG monitoring during the study. Coders use:
| CPT Code | Description |
|---|---|
| 93350 | Stress echocardiography, with interpretation and report (no continuous ECG monitoring by supervising physician) |
| 93351 | Stress echocardiography, complete, with continuous ECG monitoring and physician supervision |
| 93352 | Use of echocardiographic contrast agent during stress echo (add-on) |
Transesophageal Echocardiography (TEE)
The TEE codes are divided by indication and context and include:
| CPT Code | Description |
|---|---|
| 93312 | TEE, real-time with image documentation; complete |
| 93313 | TEE, probe placement only |
| 93314 | TEE, image acquisition, interpretation, and report only |
| 93315 | TEE for congenital cardiac anomalies; complete |
| 93316 | TEE for congenital cardiac anomalies; probe placement only |
| 93317 | TEE for congenital cardiac anomalies; image acquisition only |
| 93318 | TEE for monitoring purposes (intraoperative) |
Which Codes Cover Cardiac Stress Testing?
Non-imaging cardiac stress testing codes are built around three distinct components: physician supervision, ECG tracing, and interpretation. The following are the CPT codes used for exercise and pharmacologic stress testing:
| CPT Code | Description |
|---|---|
| 93015 | Cardiovascular stress test; complete (supervision, ECG monitoring, interpretation, and report) |
| 93016 | Physician supervision only |
| 93017 | Tracing only, without interpretation and report |
| 93018 | Interpretation and report only |
Which Codes Cover Cardioversion?
Cardioversion codes cover elective electrical conversion of arrhythmias and are among the most frequently billed standalone procedures in both inpatient and outpatient cardiology.
| CPT Code | Description |
|---|---|
| 92960 | Cardioversion, elective, electrical conversion of arrhythmia; external |
| 92961 | Cardioversion, elective, electrical conversion of arrhythmia; internal (separate procedure) |
Which Codes Cover Nuclear Cardiology?
Nuclear cardiology procedures are high-cost and frequently require prior authorization from commercial payers. CMS and most payers require that the interpreting physician’s report include findings, clinical correlation, and a final impression.
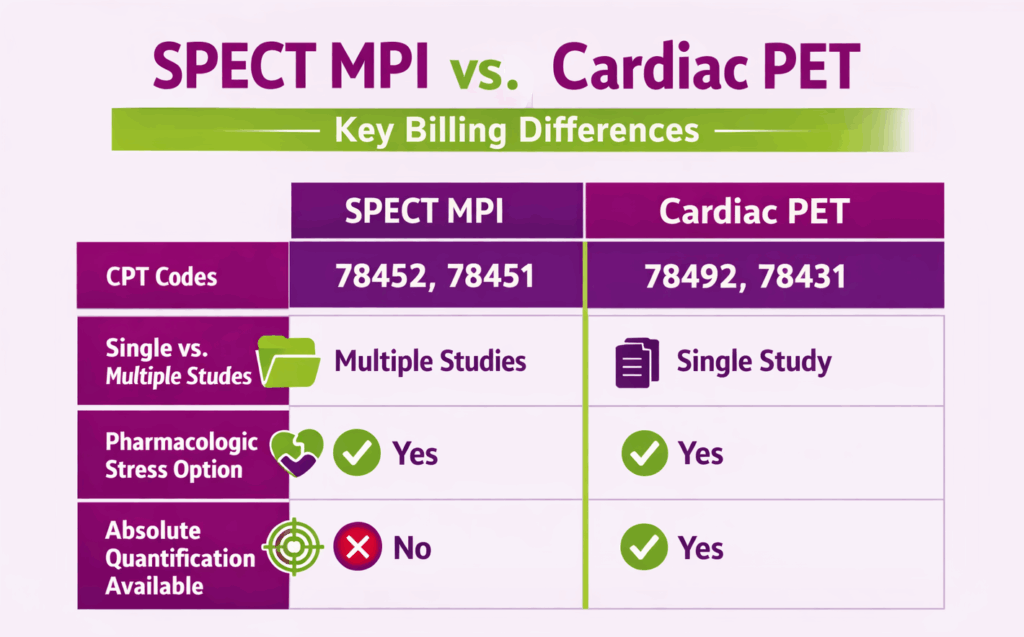
Myocardial Perfusion Imaging (MPI)
MPI is the most commonly performed nuclear cardiology study, consisting of the following CPT codes:
| CPT Code | Description |
|---|---|
| 78451 | Myocardial perfusion imaging, SPECT; single study (rest or stress only) |
| 78452 | Myocardial perfusion imaging, SPECT; multiple studies (rest and stress) |
| 78453 | Myocardial perfusion imaging, planar; single study |
| 78454 | Myocardial perfusion imaging, planar; multiple studies |
Cardiac PET
The following are Cardiac PET codes, selected based on whether the study evaluates perfusion or metabolism, and whether pharmacologic stress or absolute blood flow quantification was included:
| CPT Code | Description |
|---|---|
| 78429 | PET myocardial imaging; metabolic evaluation |
| 78430 | PET myocardial imaging; metabolic evaluation with pharmacologic stress |
| 78431 | PET myocardial perfusion imaging; single study (rest or stress) |
| 78432 | PET myocardial perfusion imaging; multiple studies (rest and stress) |
| 78433 | PET myocardial perfusion imaging, with concurrent pharmacologic stress |
| 78434 | Absolute quantitation of myocardial blood flow (add-on to 78431–78433) |
Radionuclide Ventriculography
These codes cover cardiac blood pool imaging used to assess ventricular function, most commonly ejection fraction.
| CPT Code | Description |
|---|---|
| 78472 | Cardiac blood pool imaging, gated equilibrium (MUGA); planar, single study |
| 78473 | Cardiac blood pool imaging, gated equilibrium; multiple studies |
| 78481 | Cardiac blood pool imaging, first-pass technique; single study |
| 78483 | Cardiac blood pool imaging, first-pass technique; multiple studies |
Which Codes Cover Cardiac CT and Cardiac MRI?
Cardiac CT and MRI codes fall in the radiology CPT range but are regularly billed by cardiologists who perform in-house imaging.
Cardiac CT
Most commonly used cardiac CT CPT codes are:
| CPT Code | Description |
|---|---|
| 75571 | CT, heart; without contrast, with coronary calcium quantification |
| 75572 | CT, heart; with contrast, for cardiac structure and morphology |
| 75573 | CT, heart, with contrast, for congenital heart disease evaluation |
| 75574 | CTA, coronary arteries, and cardiac structure, with contrast, including 3D post-processing |
Cardiac MRI
Cardiac MRI code selection is based on whether contrast was used and whether stress imaging was performed.
| CPT Code | Description |
|---|---|
| 75557 | Cardiac MRI; without contrast |
| 75559 | Cardiac MRI, with stress imaging |
| 75561 | Cardiac MRI, without contrast, followed by with contrast |
| 75563 | Cardiac MRI, without contrast, followed by with contrast, with stress imaging |
| 75565 | Cardiac MRI velocity flow mapping (add-on) |
Which Codes Cover Vascular Diagnostics in Cardiology?
Vascular diagnostic codes are frequently used by cardiologists who perform carotid duplex studies, peripheral arterial evaluations, and venous duplex imaging.
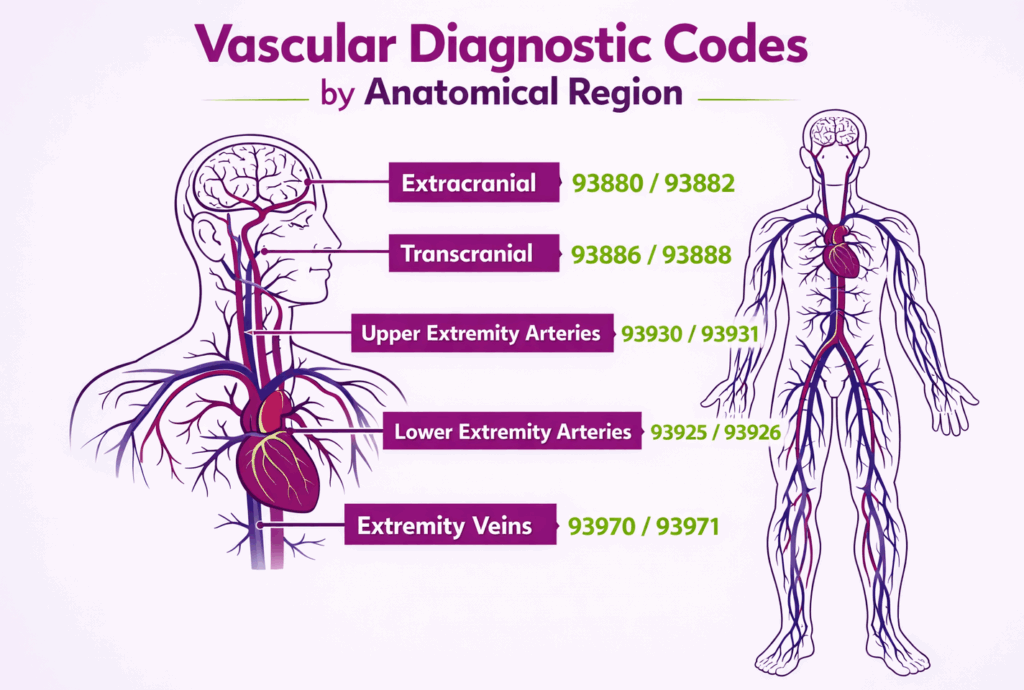
Carotid & Cerebrovascular
These codes cover duplex scanning and Doppler studies of the extracranial and intracranial vessels.
| CPT Code | Description |
|---|---|
| 93880 | Duplex scan of extracranial arteries; complete bilateral |
| 93882 | Duplex scan of extracranial arteries; unilateral or limited |
| 93886 | Transcranial Doppler study; complete |
| 93888 | Transcranial Doppler study; limited or unilateral |
Peripheral Arterial & Venous
Peripheral vascular diagnostic codes cover both physiologic studies and duplex scanning of upper and lower extremity arteries and veins.
| CPT Code | Description |
|---|---|
| 93922 | Noninvasive physiologic studies, upper or lower extremity arteries; limited bilateral |
| 93923 | Noninvasive physiologic studies; complete bilateral |
| 93925 | Duplex scan, lower extremity arteries or bypass grafts; complete bilateral |
| 93926 | Duplex scan, lower extremity arteries; unilateral or limited |
| 93930 | Duplex scan, upper extremity arteries; complete bilateral |
| 93931 | Duplex scan, upper extremity arteries; unilateral or limited |
| 93970 | Duplex scan, extremity veins; complete bilateral |
| 93971 | Duplex scan, extremity veins; unilateral or limited |
Which Codes Cover Cardiac Catheterization?
Cardiac catheterization has one of the most complex code sets in cardiology billing. Each code corresponds to a specific combination of services, right heart, left heart, coronary angiography, and bypass graft imaging.
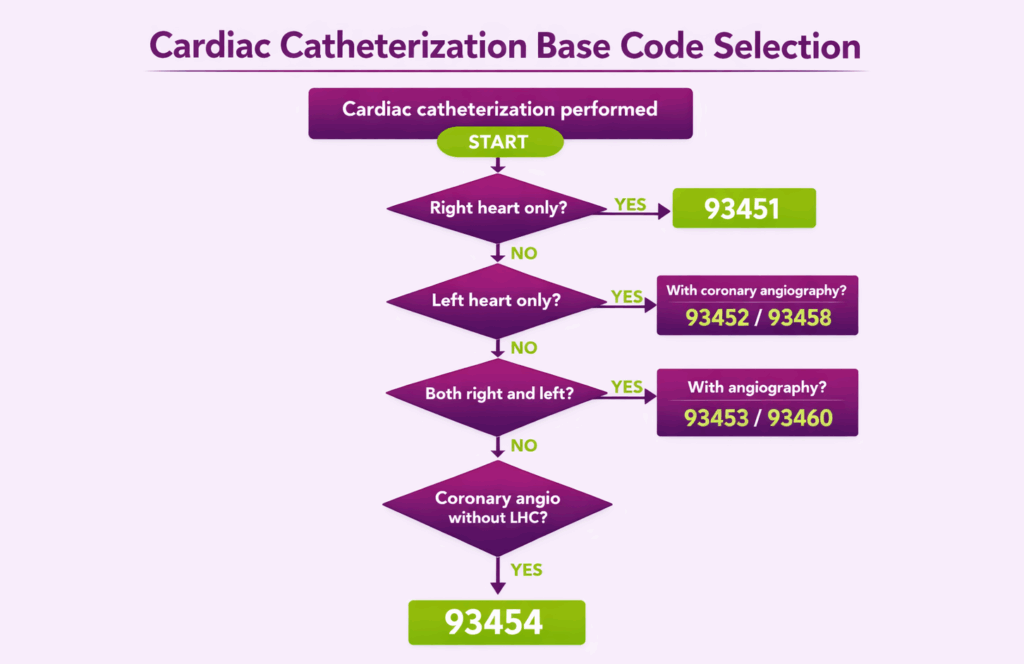
Left Heart, Right Heart & Combined Catheterization
The correct base code is determined by which cardiac chambers were accessed and whether coronary angiography or bypass graft imaging was also performed during the same session.
| CPT Code | Description |
|---|---|
| 93451 | Right heart catheterization |
| 93452 | Left heart catheterization with left ventriculography |
| 93453 | Combined right and left heart catheterization |
| 93454 | Coronary angiography without concurrent left heart catheterization |
| 93455 | Coronary angiography with bypass graft angiography, without left heart catheterization |
| 93456 | Right heart catheterization with coronary angiography |
| 93457 | Right heart catheterization with coronary and bypass graft angiography |
| 93458 | Left heart catheterization with coronary angiography |
| 93459 | Left heart catheterization with coronary and bypass graft angiography |
| 93460 | Right and left heart catheterization with coronary angiography |
| 93461 | Right and left heart catheterization with coronary and bypass graft angiography |
Coronary Physiologic Assessment
These add-on codes are used when fractional flow reserve (FFR) or coronary flow reserve (CFR) measurements are performed during catheterization.
| CPT Code | Description |
|---|---|
| 93571 | Intravascular Doppler velocity and/or pressure-derived coronary flow reserve measurement; initial vessel (add-on) |
| 93572 | Each additional coronary vessel (add-on) |
Intravascular Imaging
Intravascular ultrasound (IVUS) codes are billed as add-ons to the base catheterization or intervention code.
| CPT Code | Description |
|---|---|
| 92978 | Intravascular ultrasound (IVUS), coronary vessel or graft; initial vessel (add-on) |
| 92979 | IVUS, each additional vessel (add-on) |
Which Codes Cover Percutaneous Coronary Intervention (PCI)?
PCI codes are structured by the type of intervention performed and the vessel treated. The main distinctions are: angioplasty only, stenting, atherectomy, and chronic total occlusion.
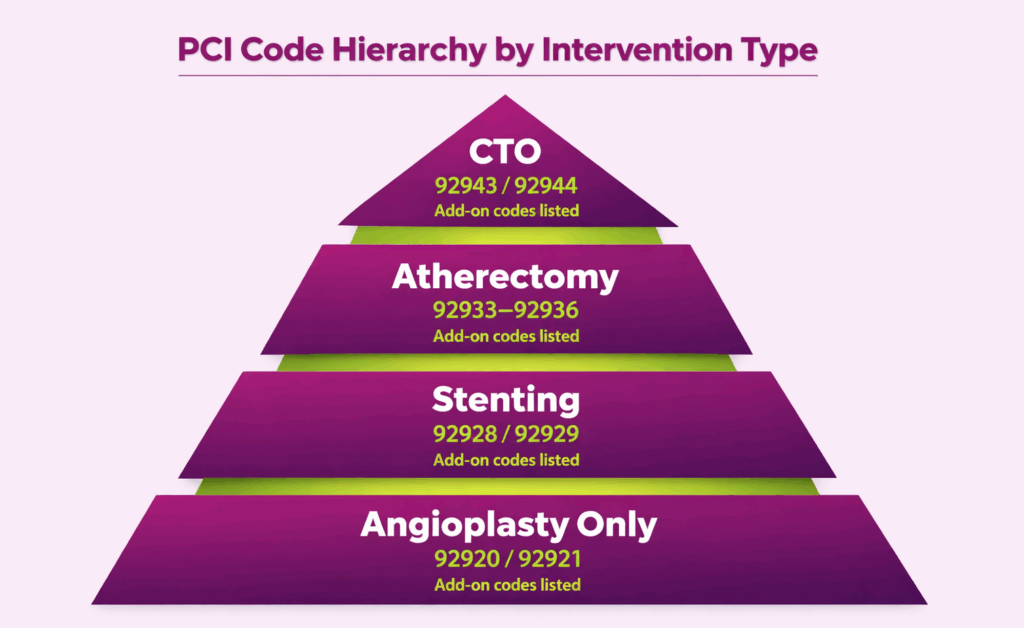
Balloon Angioplasty
Balloon angioplasty-only codes apply when no stent is placed and include:
| CPT Code | Description |
|---|---|
| 92920 | Percutaneous coronary angioplasty; single major coronary artery or branch |
| 92921 | Each additional branch treated (add-on) |
Stenting
The stenting codes, given below, include balloon angioplasty when performed.
| CPT Code | Description |
|---|---|
| 92928 | Percutaneous coronary stenting with angioplasty; single major coronary artery or branch |
| 92929 | Each additional branch (add-on) |
| 92937 | PCI of bypass graft (non-LIMA), with stenting; single vessel |
| 92938 | Each additional bypass graft vessel (add-on) |
| 92941 | PCI during acute MI; single vessel |
Atherectomy
Atherectomy codes are selected based on whether balloon angioplasty was also performed during the same session.
| CPT Code | Description |
|---|---|
| 92933 | Coronary atherectomy with angioplasty; single major coronary artery or branch |
| 92934 | Each additional branch (add-on) |
| 92935 | Coronary atherectomy without angioplasty; single major coronary artery or branch |
| 92936 | Each additional branch (add-on) |
Chronic Total Occlusion (CTO)
CTO codes apply specifically to the revascularization of a coronary vessel with chronic total occlusion.
| CPT Code | Description |
|---|---|
| 92943 | Percutaneous revascularization of chronic coronary total occlusion; single vessel |
| 92944 | Each additional vessel (add-on) |
Which Codes Cover Structural Heart Interventions?
Structural heart codes cover transcatheter procedures on cardiac valves, the left atrial appendage, and septal defects. Its code selection often depends on the access route and the number of devices implanted.
TAVR
TAVR codes are differentiated by the access approach used. Each approach has its own code.
| CPT Code | Description |
|---|---|
| 33361 | TAVR; percutaneous femoral approach |
| 33362 | TAVR; open femoral approach |
| 33363 | TAVR; open axillary artery approach |
| 33364 | TAVR; open iliac artery approach |
| 33365 | TAVR; transaortic approach |
| 33366 | TAVR; transapical approach |
| 33367 | Cardiopulmonary bypass support for TAVR (add-on) |
| 33368 | Cardiopulmonary bypass with hypothermic circulatory arrest for TAVR (add-on) |
| 33369 | Cardiopulmonary bypass without concurrent TAVR (add-on) |
Mitral, Tricuspid & Pulmonary Transcatheter
These codes cover transcatheter repair and replacement procedures for mitral, pulmonary, and other valves:
| CPT Code | Description |
|---|---|
| 33418 | Transcatheter mitral valve repair; initial prosthesis (e.g., edge-to-edge repair) |
| 33419 | Each additional prosthesis during the same session (add-on) |
| 33477 | Transcatheter pulmonary valve implantation, percutaneous approach |
Left Atrial Appendage & Septal
LAA closure and septal defect closure codes each require documentation of the specific device used, the approach taken, and imaging guidance employed.
| CPT Code | Description |
|---|---|
| 33340 | Percutaneous transcatheter closure of left atrial appendage |
| 93580 | Transcatheter closure of congenital cardiac defect; initial |
| 93581 | Transcatheter closure of congenital cardiac defect; each additional (add-on) |
| 93582 | Percutaneous transcatheter patent foramen ovale closure |
Valvuloplasty
Balloon valvuloplasty codes are organized by valve and include:
| CPT Code | Description |
|---|---|
| 92986 | Percutaneous balloon valvuloplasty; aortic valve |
| 92987 | Percutaneous balloon valvuloplasty; mitral valve |
| 92990 | Percutaneous balloon valvuloplasty; pulmonary valve |
Which Codes Cover Mechanical Circulatory Support?
Mechanical circulatory support codes cover the insertion, management, and removal of devices used to maintain hemodynamic stability in high-risk patients. They are split between intra-aortic balloon pump (IABP) procedures and ventricular assist device (VAD) procedures.
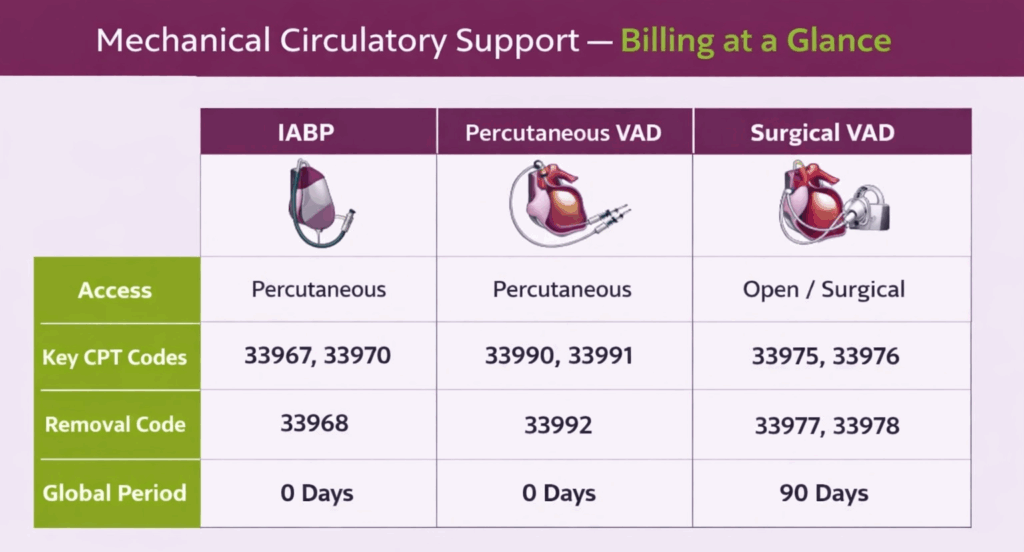
Intra-Aortic Balloon Pump (IABP)
IABP codes are selected based on the access approach used for insertion and whether removal involves open arteriotomy closure.
| CPT Code | Description |
|---|---|
| 33967 | Insertion of intra-aortic balloon pump; percutaneous |
| 33968 | Removal of intra-aortic balloon pump; percutaneous |
| 33970 | Insertion of intra-aortic balloon pump through femoral artery; open approach |
| 33971 | Removal of intra-aortic balloon pump inserted through femoral artery, with arteriotomy closure |
| 33973 | Insertion of intra-aortic balloon pump; intrathoracic approach |
Ventricular Assist Device (VAD)
VAD codes are organized by whether the device is extracorporeal or intracorporeal, the number of ventricles supported, and whether implantation is surgical or percutaneous.
| CPT Code | Description |
|---|---|
| 33975 | Insertion of ventricular assist device; extracorporeal, single ventricle |
| 33976 | Insertion of ventricular assist device; extracorporeal, biventricular |
| 33977 | Removal of ventricular assist device; extracorporeal, single ventricle |
| 33978 | Removal of ventricular assist device; extracorporeal, biventricular |
| 33979 | Insertion of ventricular assist device; implantable intracorporeal, single ventricle |
| 33980 | Removal of ventricular assist device; implantable intracorporeal, single ventricle |
| 33990 | Insertion of ventricular assist device, percutaneous; arterial access only |
| 33991 | Insertion of ventricular assist device, percutaneous; arterial and venous access with transseptal puncture |
| 33992 | Removal of percutaneous ventricular assist device; separate session from insertion |
| 33993 | Repositioning of percutaneous ventricular assist device with imaging guidance; separate session from insertion |
Which Codes Cover EP Diagnostic Studies and Mapping?
Electrophysiology (EP) study codes cover the diagnostic evaluation of cardiac electrical activity.
EP Studies
The comprehensive EP study codes are the most commonly used in this group:
| CPT Code | Description |
|---|---|
| 93600 | Bundle of His recording |
| 93602 | Intra-atrial recording |
| 93603 | Right ventricular recording |
| 93610 | Intraatrial pacing |
| 93612 | Intraventricular pacing |
| 93618 | Induction of arrhythmia by electrical pacing |
| 93619 | Comprehensive EP study without induction or termination of arrhythmia |
| 93620 | Comprehensive EP study with induction and termination of arrhythmia |
| 93621 | Left atrial pacing and recording (add-on to 93620) |
| 93622 | Left ventricular pacing and recording (add-on to 93620) |
| 93623 | Programmed stimulation after IV drug infusion (add-on) |
| 93624 | EP follow-up study |
Mapping & Intracardiac Imaging
Mapping and intracardiac imaging add-on codes are reported alongside the EP study or ablation codes.
| CPT Code | Description |
|---|---|
| 93609 | Intraventricular and/or intra-atrial mapping of tachycardia site(s) (add-on) |
| 93613 | Intracardiac electrophysiologic 3D mapping (add-on) |
| 93662 | Intracardiac echocardiography (ICE) during therapeutic/diagnostic EP intervention (add-on) |
Which Codes Cover Cardiac Ablation?
Cardiac ablation codes are built around the type of arrhythmia being treated. Each primary ablation code includes a comprehensive EP evaluation.
| CPT Code | Description |
|---|---|
| 93653 | Comprehensive EP evaluation with catheter ablation; atrial focus (e.g., SVT, atrial flutter) |
| 93654 | Comprehensive EP evaluation with catheter ablation; ventricular focus (e.g., VT) |
| 93655 | Ablation of additional distinct arrhythmia (add-on to 93653 or 93654) |
| 93656 | Comprehensive EP evaluation with pulmonary vein isolation for atrial fibrillation |
| 93657 | Additional linear or focal left or right atrial ablation (add-on to 93656) |
Which Codes Cover Pacemaker Procedures?
Pacemaker codes cover new implantations, generator replacements, lead procedures, and loop recorder placements.
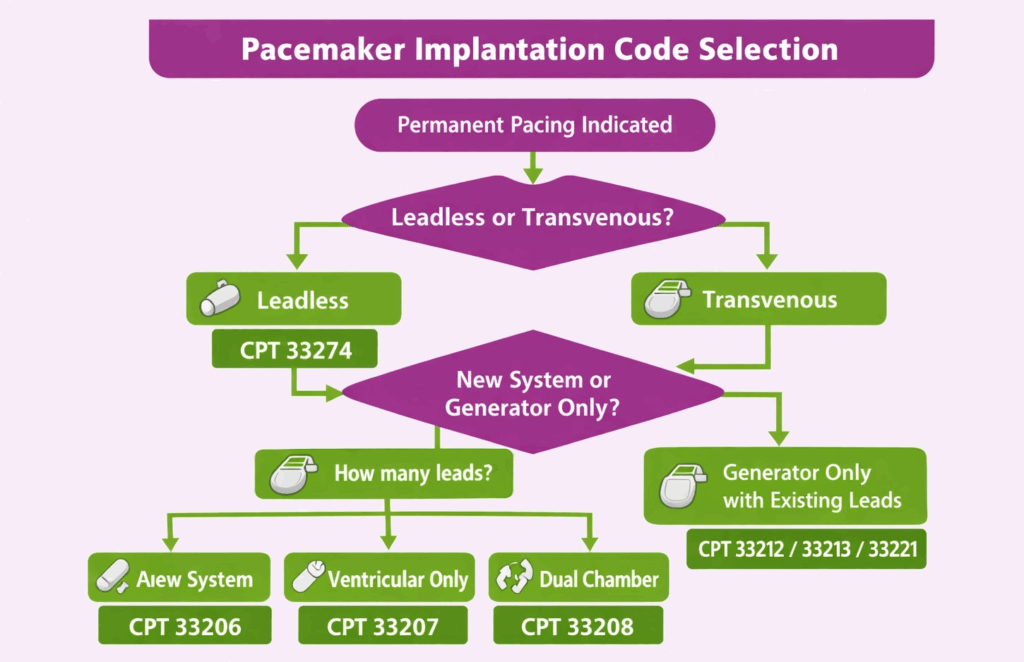
New Implantation
New pacemaker implantation codes are selected based on how many leads (chambers) were implanted.
| CPT Code | Description |
|---|---|
| 33206 | Insertion of permanent pacemaker with transvenous electrode(s); atrial lead only |
| 33207 | Insertion of permanent pacemaker; ventricular lead only |
| 33208 | Insertion of permanent pacemaker; atrial and ventricular leads (dual chamber) |
| 33212 | Insertion of pacemaker generator only, with existing single lead |
| 33213 | Insertion of pacemaker generator only, with existing dual leads |
| 33221 | Insertion of pacemaker generator only, with existing multiple leads |
Generator Replacement
Generator replacement codes apply when only the pulse generator is exchanged, and the existing leads are retained.
| CPT Code | Description |
|---|---|
| 33227 | Removal and replacement of pacemaker pulse generator; single lead system |
| 33228 | Removal and replacement of pacemaker pulse generator; dual lead system | 33229 | Removal and replacement of pacemaker pulse generator; multiple lead system |
Lead Procedures
Lead procedure codes cover insertion, repair, and removal of transvenous pacing leads, as well as temporary pacing.
| CPT Code | Description |
|---|---|
| 33210 | Insertion or replacement of temporary transvenous single-chamber pacing catheter |
| 33216 | Insertion of single transvenous pacing electrode (lead) |
| 33217 | Insertion of two transvenous pacing electrodes (leads) |
| 33218 | Repair of single transvenous electrode |
| 33220 | Repair of two transvenous electrodes |
| 33233 | Removal of pacemaker pulse generator only |
| 33234 | Removal of single transvenous pacing electrode |
| 33235 | Removal of dual transvenous pacing electrodes |
Implantable Cardiac Monitor (Loop Recorder)
Loop recorder codes cover insertion and removal of an implantable cardiovascular monitor. These devices are distinct from ICDs and pacemakers and have their own code set.
| CPT Code | Description |
|---|---|
| 33285 | Insertion of implantable cardiovascular monitor (loop recorder) |
| 33286 | Removal of implantable cardiovascular monitor |
Leadless Pacemaker
Leadless pacemaker codes cover the transcatheter implantation of a self-contained, intracardiac pacing device without transvenous leads.
| CPT Code | Description |
|---|---|
| 33274 | Transcatheter insertion or replacement of permanent leadless pacemaker, right ventricular, including imaging guidance and electrophysiologic evaluation |
| 33275 | Transcatheter removal of permanent leadless pacemaker, right ventricular |
Which Codes Cover ICD Procedures?
ICD procedure codes follow a similar logic to pacemaker codes but include additional distinctions for subcutaneous systems (S-ICD) and resynchronization devices (CRT-D).
Transvenous ICD
Transvenous ICD codes cover the full range of new implantation and generator-only insertions.
| CPT Code | Description |
|---|---|
| 33249 | Insertion of permanent ICD with transvenous electrodes; dual and multiple lead system |
| 33240 | Insertion of ICD pulse generator only; with existing single lead |
| 33230 | Insertion of ICD pulse generator only; with existing dual leads |
| 33231 | Insertion of ICD pulse generator only; with existing multiple leads |
| 33241 | Removal of ICD pulse generator only |
| 33244 | Removal of transvenous ICD electrode(s) |
| 33262 | Removal and replacement of ICD pulse generator; single lead system |
| 33263 | Removal and replacement of ICD pulse generator; dual lead system |
| 33264 | Removal and replacement of ICD pulse generator; multiple lead system |
CRT-D
CRT-D implantation is coded using the primary ICD code with the left ventricular lead add-on code.
| CPT Code | Description |
|---|---|
| 33224 | Insertion of LV pacing electrode; cardiac venous system, with attachment to pacemaker generator |
| 33225 | Insertion of LV pacing electrode, with attachment to existing ICD or pacemaker generator (add-on) |
Subcutaneous ICD (S-ICD)
S-ICD codes cover the fully subcutaneous system, which does not use transvenous leads.
| CPT Code | Description |
|---|---|
| 33270 | Insertion or replacement of S-ICD system with subcutaneous electrode |
| 33271 | Insertion of S-ICD subcutaneous electrode only |
| 33272 | Removal of S-ICD subcutaneous electrode only |
| 33273 | Repositioning of previously implanted S-ICD subcutaneous electrode |
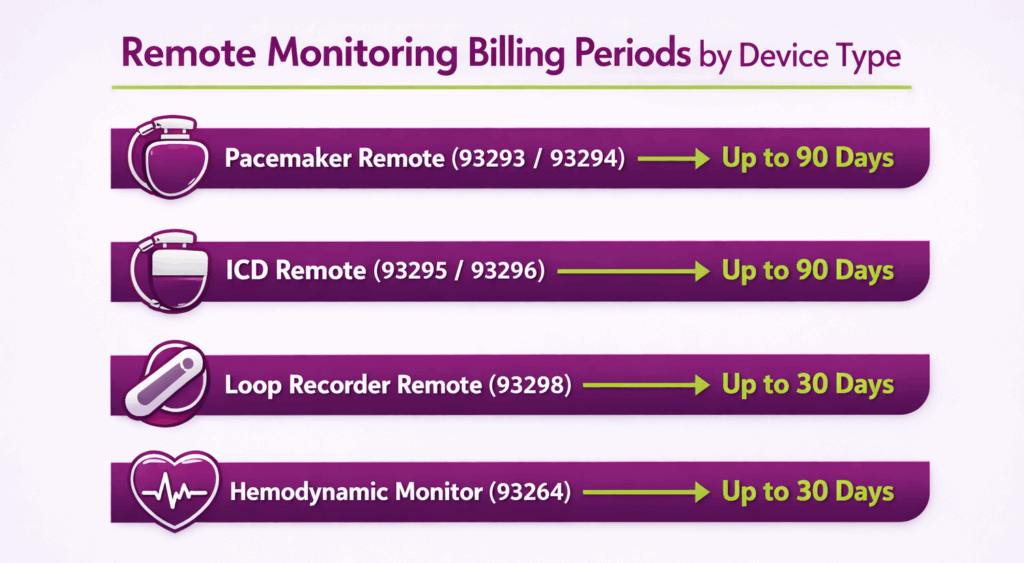
Which Codes Cover Cardiac Device Programming and Remote Monitoring?
Device evaluation codes cover both in-person programming sessions and remote monitoring services. Remote monitoring codes cover a defined monitoring period, typically up to 90 days, and are reported once per period, not per transmission.
In-Person Device Programming & Interrogation
In-person device evaluation codes are split between programming evaluations (adjustments made) and interrogation-only evaluations (data review with no changes).
| CPT Code | Description |
|---|---|
| 93279 | Programming device evaluation; single chamber pacemaker |
| 93280 | Programming device evaluation; dual chamber pacemaker |
| 93281 | Programming device evaluation; multiple lead pacemaker |
| 93282 | Programming device evaluation; single chamber ICD |
| 93283 | Programming device evaluation; dual chamber ICD |
| 93284 | Programming device evaluation; subcutaneous ICD |
| 93285 | Programming device evaluation; implantable loop recorder |
| 93288 | Interrogation device evaluation; single chamber pacemaker |
| 93289 | Interrogation device evaluation; dual chamber pacemaker |
| 93290 | Interrogation device evaluation; ICD system with leads |
Remote Monitoring
Remote monitoring codes are reported once per monitoring period per device. They are not billed per transmission or per day.
| CPT Code | Description |
|---|---|
| 93293 | Remote interrogation evaluation; single, dual, or multiple lead pacemaker (up to 90 days) |
| 93294 | Remote physiologic data analysis; pacemaker system (up to 90 days) |
| 93295 | Remote interrogation evaluation; ICD system (up to 90 days) |
| 93296 | Remote physiologic data analysis; ICD system (up to 90 days) |
| 93298 | Remote interrogation evaluation; implantable cardiovascular physiologic monitor (loop recorder, up to 30 days) |
Implantable Hemodynamic Monitoring
This CPT code 93264 covers remote monitoring of a wireless pulmonary artery pressure sensor (e.g., CardioMEMS). It is reported once per monitoring period and is not billed per transmission. Up to 30 days, including downloads, interpretation, trend analysis, and report.
Which Codes Cover Cardiac Rehabilitation?
Cardiac rehabilitation codes cover physician-supervised outpatient rehabilitation sessions following qualifying cardiac events such as MI, CABG, stable angina, heart valve repair or replacement, PTCA, or heart transplant.
| CPT Code | Description |
|---|---|
| 93797 | Physician services for outpatient cardiac rehabilitation; without continuous ECG monitoring (per session) |
| 93798 | Physician services for outpatient cardiac rehabilitation; with continuous ECG monitoring (per session) |
Which Codes Cover CABG?
CABG codes are organized by conduit type (venous, arterial, or combined) and by the number of vessels bypassed.
Venous CABG
Venous CABG codes apply when saphenous vein or other venous conduits are used exclusively.
| CPT Code | Description |
|---|---|
| 33510 | CABG using venous graft only; single |
| 33511 | CABG using venous graft only; two |
| 33512 | CABG using venous graft only; three |
| 33513 | CABG using venous graft only; four |
| 33514 | CABG using venous graft only; five |
| 33516 | CABG using venous graft only; six or more |
Arterial CABG
Arterial CABG codes apply when the LIMA, RIMA, radial artery, or other arterial conduits are used exclusively.
| CPT Code | Description |
|---|---|
| 33533 | CABG using arterial graft only; single |
| 33534 | CABG using arterial graft only; two |
| 33535 | CABG using arterial graft only; three |
| 33536 | CABG using arterial graft only; four or more |
Combined Arterial + Venous CABG (Add-Ons)
When both arterial and venous conduits are used in the same operation, report the arterial CABG code as the primary code and add the appropriate venous add-on code for the number of venous grafts performed.
| CPT Code | Description | ||
|---|---|---|---|
| 33517 | Combined CABG; additional venous graft, single (add-on) | ||
| 33518 | Additional venous graft, two (add-on) | ||
| 33519 | Additional venous graft, three (add-on) | ||
| 33521 | Additional venous graft, four (add-on) | ||
| 33522 | Additional venous graft, five (add-on) | ||
| 33523 | Additional venous graft, six or more (add-on) |
| CPT Code | Description |
|---|---|
| 33405 | Aortic valve replacement; with prosthetic valve |
| 33406 | Aortic valve replacement; with allograft (homograft) |
| 33413 | Aortic valve replacement by translocation of autologous pulmonary valve (Ross procedure) |
| 33417 | Aortic valve repair with cardiopulmonary bypass |
Mitral Valve
Mitral valve codes cover the spectrum from closed and open valvotomy to ring-supported repair and full replacement.
| CPT Code | Description |
|---|---|
| 33420 | Valvotomy, mitral valve; closed heart |
| 33422 | Valvotomy, mitral valve; open heart with cardiopulmonary bypass |
| 33425 | Valvuloplasty, mitral valve; with cardiopulmonary bypass |
| 33426 | Valvuloplasty, mitral valve; with prosthetic ring |
| 33427 | Valvuloplasty, mitral valve; radical reconstruction |
| 33430 | Replacement of mitral valve with cardiopulmonary bypass |
Tricuspid Valve
Tricuspid valve codes cover repair and replacement procedures.
| CPT Code | Description |
|---|---|
| 33460 | Valvectomy, tricuspid valve; with cardiopulmonary bypass |
| 33463 | Valvuloplasty, tricuspid valve; without ring insertion |
| 33464 | Valvuloplasty, tricuspid valve; with ring insertion |
| 33465 | Replacement of tricuspid valve; with cardiopulmonary bypass |
| 33468 | Tricuspid valve repositioning and plication for Ebstein anomaly |
Which Codes Cover Aortic Surgery?
Aortic surgery codes cover both open surgical repair and endovascular approaches. Open and endovascular codes are never reported together for the same aortic segment.
Open Aortic Surgery
Open aortic surgery codes cover repair and replacement of the ascending aorta, the arch, and the descending thoracic aorta.
| CPT Code | Description |
|---|---|
| 33860 | Aortic root and ascending aorta replacement; with cardiopulmonary bypass |
| 33863 | Aortic root replacement with composite graft (Bentall procedure) |
| 33864 | Aortic root and ascending aorta replacement; with cardiopulmonary bypass and circulatory arrest |
| 33870 | Transverse aortic arch repair; with cardiopulmonary bypass |
| 33877 | Descending thoracic aorta grafting; with or without bypass |
Endovascular Aortic Repair (EVAR/TEVAR)
Endovascular repair codes are organized by the aortic segment treated and the configuration of the endograft deployed.
| CPT Code | Description |
|---|---|
| 33880 | TEVAR; involving coverage of the left subclavian artery origin |
| 33881 | TEVAR; not involving coverage of the left subclavian artery |
| 33883 | Placement of additional proximal thoracic endovascular extension prosthesis (add-on) |
| 33884 | Placement of additional distal thoracic endovascular extension prosthesis (add-on) |
| 33886 | Placement of additional distal thoracic extension prosthesis, delayed after primary intervention (add-on) |
| 34701 | EVAR, infrarenal aorta; aorto-aortic tube prosthesis |
| 34702 | EVAR, infrarenal aorta; aorto-bi-iliac prosthesis |
| 34703 | EVAR, infrarenal aorta; aorto-uni-iliac prosthesis |
| 34704 | EVAR, infrarenal aorta; aorto-bi-iliac and aorto-uni-iliac prosthesis |
| 34705 | EVAR, infrarenal aorta; aorto-bi-iliac and aorto-uni-femoral prosthesis |
| 34706 | EVAR, infrarenal aorta; aorto-uni-iliac and aorto-uni-femoral prosthesis |
| 34707 | EVAR, infrarenal aorta; aorto-bi-femoral prosthesis |
| 34708 | EVAR; placement of an iliac artery endoprosthesis (add-on) |
Which Modifiers Are Most Used in Cardiology?
In cardiology medical billing, modifiers define how a service was delivered, who performed it, whether it was complete, and how it relates to other same-day services. The ones below are the modifiers that appear most often in cardiology billing. Each has a specific purpose; using the wrong one, or omitting one entirely, is one of the fastest ways to trigger a denial or an audit.
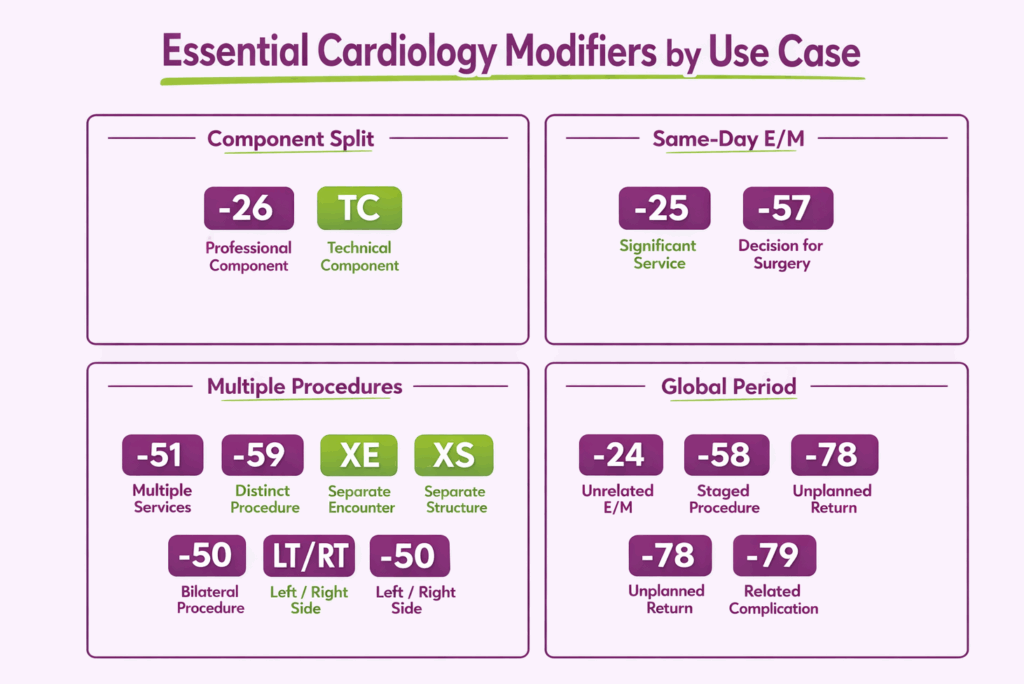
Which Modifiers Split a Service Between Professional and Technical Components?
Diagnostic cardiology services like echocardiograms, nuclear studies, and Holter recordings often involve two separately billable components when the interpreting physician and the performing facility are different entities. These two modifiers define that split.
| Modifier | Name | When to Use |
|---|---|---|
| -26 | Professional Component | Physician bills for interpretation and written report only; facility owns and operates the equipment |
| TC | Technical Component | Facility bills for equipment, supplies, and technical staff only; physician bills -26 separately |
Which Modifiers Handle Same-Day E/M and Procedure Billing?
Payers bundle the E/M into the procedure’s reimbursement by default when both occur on the same date. These modifiers, appended to the E/M code, not the procedure, override that bundling when the E/M is legitimately separate.
| Modifier | Name | When to Use |
|---|---|---|
| -25 | Significant, Separately Identifiable E/M | E/M on the same day as a minor or diagnostic procedure (0- or 10-day global); the E/M must address a distinct clinical issue |
| -57 | Decision for Major Surgery | E/M at which the decision to perform a 90-day global procedure was made; used on the day of that visit, not the day of surgery |
Which Modifier Identifies Telehealth Services?
Telehealth services require a modifier that identifies the visit as delivered via synchronous audio-video communication. Without it, the claim is processed as an in-person service with the incorrect place of service.
| Modifier | Name | When to Use |
|---|---|---|
| -95 | Synchronous Telemedicine Service | Used alongside Place of Service 10 (patient’s home) or 02 (other telehealth) depending on patient location |
Which Modifiers Address Multiple, Repeated, or Bilateral Procedures?
Cardiology procedures are frequently performed in combination, repeated on the same date, or performed bilaterally. Each scenario requires a specific modifier, and the distinction between -59 and its X{EPSU} alternatives matters for audit risk.
| Modifier | Name | When to Use |
|---|---|---|
| -51 | Multiple Procedures | Appended to the secondary procedure when two or more procedures are performed in the same session by the same provider; not used on add-on codes |
| -59 | Distinct Procedural Service | Overrides an NCCI bundling edit when procedures are genuinely distinct; requires documented clinical justification |
| XE | Separate Encounter | More specific alternative to -59; services occurred during distinct encounters on the same date |
| XS | Separate Structure | More specific alternative to -59; services performed on a distinct anatomical site or structure |
| XP | Separate Practitioner | More specific alternative to -59; performed by a different practitioner than the primary |
| XU | Unusual Non-Overlapping Service | More specific alternative to -59; service does not overlap with the standard components of the primary procedure |
| -76 | Repeat Procedure, Same Physician | Same procedure repeated on the same date by the same physician; requires documentation of medical necessity |
| -77 | Repeat Procedure, Different Physician | Same procedure repeated on the same date by a different physician |
| -50 | Bilateral Procedure | Same procedure performed on both sides during the same session |
| -LT / -RT | Left Side / Right Side | Identifies the specific side when a procedure is performed unilaterally; required by many payers in place of -50 for bilateral vascular studies reported on separate lines |
Which Modifiers Govern the Global Surgical Period?
Device implants, structural heart procedures, CABG, and valve surgery carry 90-day global periods. Any service billed during that period is denied as bundled unless one of these modifiers establishes that it falls outside the global package.
| Modifier | Name | When to Use | Starts New Global Period? |
|---|---|---|---|
| -24 | Unrelated E/M During Postop Period | E/M visit for a condition completely unrelated to the surgery | No |
| -58 | Staged or Related Procedure | Planned staged procedure, or procedure more extensive than the original | Yes |
| -78 | Return to OR for Complication | Unplanned return to OR to treat a complication from the original procedure | No |
| -79 | Unrelated Procedure During Postop Period | Entirely unrelated procedure performed within the original global period | Yes |
Which Modifiers Address Service-Level Documentation and Complexity?
To accurately reflect variations in procedural services, specific modifiers are used to indicate when a procedure is reduced, discontinued, or requires unusual complexity.
| Modifier | Name | When to Use |
|---|---|---|
| -52 | Reduced Services | Procedure partially reduced at physician’s discretion; service was not completed in full but no safety event occurred |
| -53 | Discontinued Procedure | Procedure started but stopped due to patient safety concerns or an adverse event before completion |
| -22 | Increased Procedural Complexity | Procedure required substantially greater work than the base code reflects; requires a supporting operative note |
| -KX | Requirements Specified in the LCD Have Been Met | Appended to Medicare claims for services subject to a Local Coverage Determination (LCD), including echocardiography, stress testing, and nuclear imaging |
Which Modifiers Address Surgical Assistance?
When more than one provider participates in a cardiac or vascular surgical procedure, each must bill with a modifier that defines their specific role.
| Modifier | Name | Who Uses It | Role |
|---|---|---|---|
| -62 | Two Surgeons | Each of two co-surgeons | Each performs a distinct part of the procedure independently; both bill the same CPT code |
| -80 | Assistant Surgeon | Physician | Assists the primary surgeon but does not independently perform a distinct portion |
| AS | Assistant at Surgery | PA, NP, or CNS | Non-physician surgical assistant; follows same billing logic as -80 |
| -66 | Surgical Team | Each team member | Complex procedure requiring multiple surgeons working simultaneously |
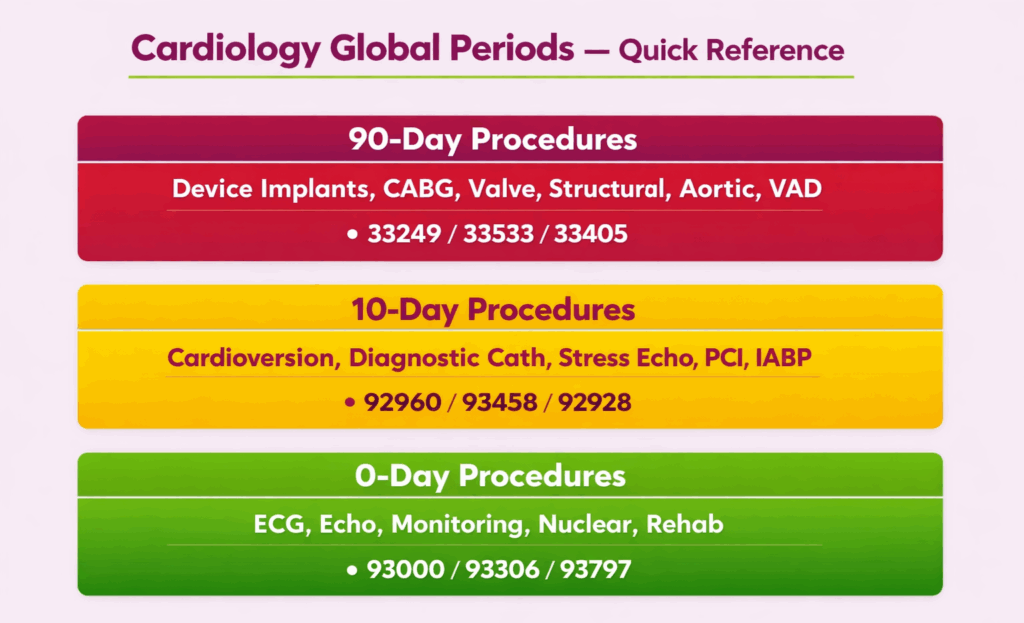
What Are the Global Surgical Periods for Common Cardiology Procedures?
The global period determines how long post-procedure services are bundled into the original procedure’s reimbursement. Knowing which period applies to each service when doing cardiology billing is what makes the -24, -58, -78, and -79 modifiers actionable.
| Global Period | Procedure Category | Representative CPT Codes |
|---|---|---|
| 90 Days | Pacemaker implantation | 33206, 33207, 33208 |
| Leadless pacemaker | 33274 | |
| ICD implantation | 33249, 33270 | |
| Cardiac ablation | 93653, 93654, 93656 | |
| CABG | 33510–33516, 33533–33536 | |
| Valve surgery | 33405, 33430, 33465 | |
| Structural heart (TAVR, MitraClip) | 33361–33366, 33418 | |
| Aortic surgery (open and endovascular) | 33860, 33880, 34701–34702 | |
| VAD insertion | 33975, 33976, 33979 | |
| 10 Days | Cardioversion | 92960 |
| Diagnostic cardiac catheterization | 93451–93461 | |
| Stress echocardiography | 93350, 93351 | |
| PCI | 92928, 92933, 92943 | |
| IABP insertion | 33967, 33970 | |
| 0 Days | ECG and rhythm strips | 93000, 93040 |
| Echocardiography (resting) | 93306, 93307, 93308 | |
| Holter and extended monitoring | 93224, 93241, 93245 | |
| Nuclear cardiology | 78451, 78452 | |
| Device interrogation and remote monitoring | 93288–93298 | |
| Cardiac rehabilitation | 93797, 93798 |
Zero-day global procedures are not subject to global period bundling; each encounter bills independently. For 10- and 90-day procedures, any E/M or related service billed within the global window requires the appropriate modifier to avoid automatic denial.
What are the Most Common Coding Issues in Cardiology?
Cardiology has more bundling rules, add-on code dependencies, and modifier requirements than almost any other specialty. The errors below are not edge cases as they appear in routine claims and are among the most common reasons cardiology practices face denials, recoupments, and audit flags.
What Bundling Mistakes Happen Most With Diagnostic Codes?
Diagnostic cardiology codes are built with specific bundling logic that is easy to misread. The most common errors occur when coders treat separately billable components as standalone codes or bill a lesser study when documentation supports a higher one.
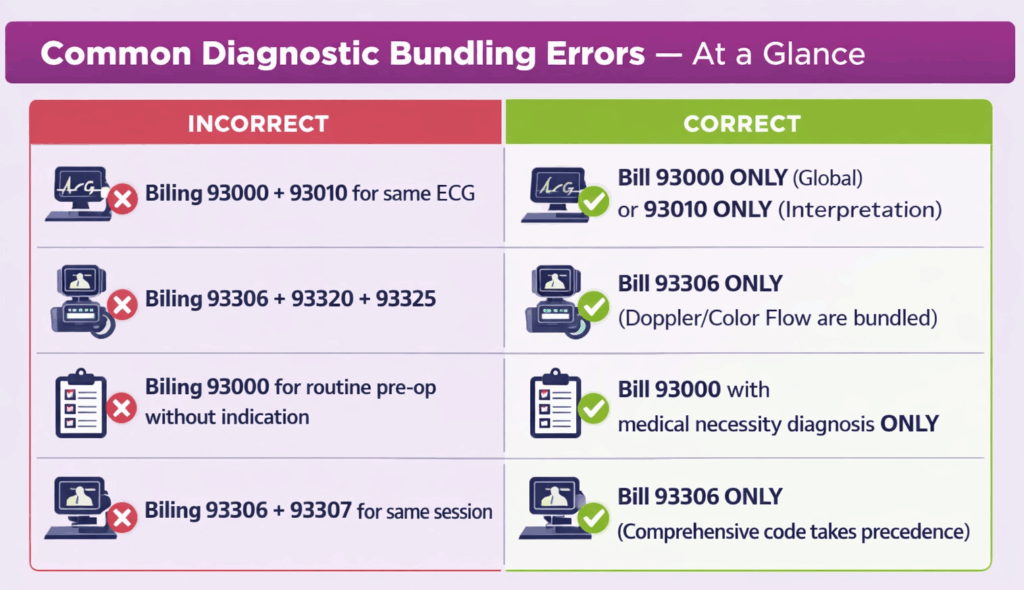
Echocardiography
Three echo billing errors account for the majority of NCCI edit violations and underpayment in this category.
- Doppler add-ons appended to 93306: Codes 93320, 93321, and 93325 are only appropriate alongside 93307 or 93308. CPT 93306 already includes spectral and color flow Doppler; adding these add-ons to it triggers a hard NCCI edit.
- 93308 billed when documentation supports a complete study: A limited echo applies when only a specific finding is being evaluated. If the report includes full chamber measurements, valve assessments, and wall motion analysis, 93306 is the correct code. Billing 93308 in this scenario is undercoding and leaves revenue on the table.
- Same-day stress echo and resting TTE without distinct medical necessity: A stress echo includes rest and stress imaging. Billing a separate resting TTE on the same date requires documented clinical justification showing the resting study served a distinct diagnostic purpose. Without it, payers will deny one of the two claims.
ECG and Monitoring
These two errors appear most often in high-volume outpatient settings where ECG and Holter services are billed in bulk.
- 93000 and 93010 billed for the same service on the same date: CPT 93000 covers the complete ECG service. If the physician only interpreted a facility-performed tracing, 93010 is correct. Billing both for the same tracing is duplicate billing.
- Holter interpretation submitted without a corresponding technical record: When billing 93227 or 93226, the technical recording must exist and be documented. Claims submitted without it are routinely denied on audit.
Cardiac Devices and Remote Monitoring
Device evaluation codes follow billing period logic, not per-contact logic, and this distinction is consistently misapplied.
- Remote monitoring billed per transmission instead of per period: Codes 93293–93298 are reported once per monitoring period, regardless of how many transmissions occurred within that window. Billing per transmission inflates claim volume and is a common audit trigger.
- In-person interrogation and remote monitoring billed for the same device in the same period: When an in-person interrogation code (93288–93290) and a remote monitoring code (93293–93296) overlap within the same billing period for the same device, payers will deny the remote code. The periods must be managed to avoid overlap.
What Bundling Mistakes Happen Most With Interventional Codes?
Interventional cardiology has layered bundling rules across catheterization, PCI, and add-on codes. The errors below consistently produce either duplicated billing or underpayment.
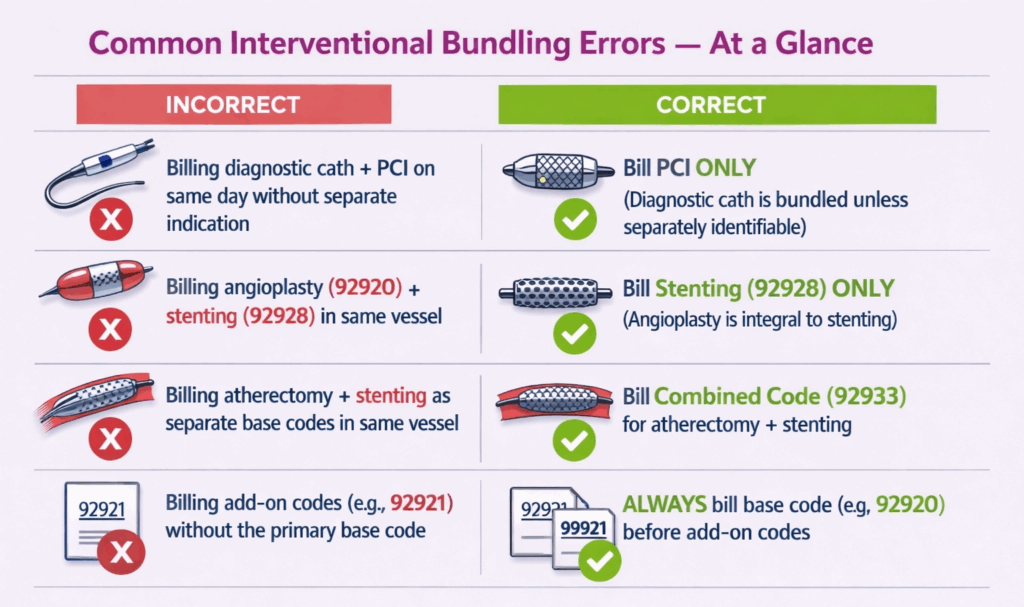
Cardiac Catheterization
Both of these errors stem from misreading what the catheterization base codes already include.
- Coronary angiography billed separately alongside 93458–93461: These codes already bundle coronary angiography into the procedure. Adding a separate angiography code for the same session is unbundling.
- Diagnostic catheterization billed same-day as PCI for the same vessel: When diagnostic angiography and PCI are performed in the same session on the same vessel, the diagnostic cath is bundled into the PCI code. A separate diagnostic cath code requires payer-specific same-day policy criteria and explicit medical necessity documentation to be payable.
PCI
PCI bundling errors almost always involve failing to distinguish between base codes, add-on codes, and combined codes across the same session.
- 92920 and 92928 billed separately for the same vessel: The stent code includes balloon angioplasty. Billing both for the same vessel and lesion is unbundling. Use 92928 when a stent is placed; 92920 stands alone only when angioplasty was performed without stenting.
- Atherectomy and stenting billed with two separate base codes: When both are performed on the same vessel, the combined atherectomy codes (92933–92934) apply. Separately billing 92935 and 92928 for the same vessel violates NCCI bundling rules.
- Second base code used instead of an add-on for additional branches: When PCI extends to additional branches of a vessel already treated, add-on codes (92921, 92929, 92934, 92944) are required. Using a second base code for a branch treated in the same session will be denied.
What Modifier Misuse Causes the Most Claim Denials in Cardiology?
Modifier errors in cardiology fall into three patterns: overuse, underuse, and misapplication, each with distinct audit consequences.
- -59 appended without a genuinely distinct procedural service: Modifier -59 requires clinically separate services, different anatomical sites, indications, or circumstances not captured by either code’s descriptor. Using it to bypass a bundling edit without that documentation does not override the edit on audit; it compounds the problem by signaling intentional unbundling.
- -25 appended without a separately identifiable E/M note: The E/M note must stand on its own. If the documentation reads only as a pre-procedure evaluation, -25 will not survive a medical records review. The E/M must address a clinical problem or decision distinct from the work inherent to the procedure.
- Global code billed from a facility setting without -26: When a cardiologist provides only the interpretation and report for a study performed at a hospital or outpatient facility, the claim must carry -26. Billing the global code in this setting means billing for equipment and staff the physician did not provide, a common audit finding in echocardiography and nuclear cardiology.
What Documentation Gaps Most Often Lead to Cardiology Claim Denials?
Incomplete documentation is the most cited reason for medical necessity denials and post-payment recoupments across all cardiology service lines. These are the gaps that appear most consistently in audits of the top-rated cardiology billing companies.
- Echocardiography reports must include 2D chamber measurements, Doppler velocities, valve morphology and function, wall motion assessment, and the clinical indication. Reports that list conclusions without supporting measurements are routinely denied on post-payment review.
- Cardiac catheterization reports must document hemodynamic pressures, specific vessels studied, stenosis percentages by vessel segment, and clinical justification for any add-on services billed, such as FFR or IVUS. Vague language like “significant CAD noted” without vessel-level specificity will not support the add-on codes.
- Stress test reports must include the stress protocol used, the patient’s clinical response, maximum workload or heart rate achieved, ECG findings during stress, and, when billing 93016, a documented statement of physician supervision during the test.
- Ablation procedure notes must document arrhythmia induction, mapping methodology, targeted arrhythmia circuit or focus, energy delivery parameters, and confirmation of endpoint. Notes describing general technique without procedure-specific findings will not support the ablation code on audit.
- Device implant notes must specify lead configuration, lead placement sites, sensing and pacing thresholds measured at implant, impedance values, and final programmed parameters. A note listing the device model without documented measured thresholds is consistently flagged in OIG compliance reviews.
What are the Most Frequently Triggered NCCI Edit Violations in Cardiology?
NCCI edits define code pairs that cannot be billed together without an appropriate modifier, or in some cases, cannot be billed together under any circumstances. The violations below are the ones that surface most often in cardiology claims.
| Code(s) Billed Together | Why It Triggers an Edit |
|---|---|
| 93320 or 93325 without a base echo code | Doppler add-on codes require a base echocardiography code in the same session; they cannot be billed standalone |
| 93571 (FFR) without a cardiac catheterization code | FFR is a catheterization add-on; it has no reimbursable context without a primary catheterization code in the same claim |
| 93613 (3D mapping) outside of an EP study or ablation encounter | 3D mapping is an add-on to EP studies and ablation procedures; billing it as a standalone service is a hard NCCI edit |
| 92978 (IVUS) without a PCI or catheterization code | IVUS is an add-on to coronary intervention or diagnostic catheterization; it requires a primary procedure code in the same session |
| Diagnostic catheterization + PCI for the same vessel without separate medical necessity criteria | When diagnostic cath and PCI occur in the same session on the same vessel, the diagnostic code is typically bundled; separate billing requires payer-specific criteria and explicit medical necessity documentation |