
ASC coding operates under tighter scrutiny than most providers realize. According to CMS’s 2024 Medicare Fee-for-Service Supplemental Improper Payment Data, the improper payment rate for ASCs sits at 14.7%, amounting to almost $656.3 million. That’s nearly double the Medicare FFS program-wide average. At the center of it all is CPT code selection: get it wrong, and you’re looking at denials, underpayments, or audit exposure.
Accurate Current Procedural Terminology coding is the backbone of revenue in every Ambulatory Surgery Center. Clean claim performance depends on how precisely CPT codes align with ICD-10-CM diagnoses, Healthcare Common Procedure Coding System supplies, and modifier usage.
This ASC CPT codes cheatsheet enlists the most commonly billed CPT procedures, high-frequency diagnosis pairings, and modifiers used in ASC billing. More importantly, it will help ASCs reduce denial rates, improve clean claim ratios, and maintain compliance across payer-specific rules.
How ASC CPT Code Billing Works?
Billing in an Ambulatory Surgery Center follows a fundamentally different logic than physician billing. However, both use the same CPT codes. ASC billing focuses on facility resources, supplies, and operational costs tied to the procedure rather than the physician’s work. This separation is why the same CPT code can generate two distinct claims: one for the ASC facility and one for the provider.
Why Do ASC Bills Show Facility Fees Instead of Professional Services Charges?
An ASC submits claims only for the facility component of a procedure. The surgeon, anesthesiologist, or other providers bill separately for professional services under their own claims. This distinction is critical: the ASC’s CPT coding must reflect resource utilization (equipment, staff, supplies), not physician work. Misalignment here directly impacts reimbursement accuracy.
UB-04 Claim Structure Under CMS
ASC claims are submitted under UB-04 (CMS-1450), even though they fall under Medicare Part B payment rules. This hybrid structure matters because CPT codes are interpreted through an institutional billing lens, not a professional one. That affects:
- Packaging logic
- Modifier applicability
- Separately payable services
Bundled Payment Logic For ASC Reimbursements
ASC reimbursement is driven by a single bundled payment system. For each primary CPT code, the Centers for Medicare & Medicaid Services assigns a payment rate that includes:
- Routine supplies
- Standard recovery services
- Most ancillary items
Only specific services, such as certain drugs, implants, or devices billed via HCPCS, are separately payable. Incorrectly unbundling or over-reporting CPTs is a high-risk denial trigger.
What is the CMS ASC Approved Procedures List?
Not every CPT code is reimbursable in an ASC setting. Centers for Medicare & Medicaid Services maintains the ASC Approved Procedures List, which defines which procedures are safe and appropriate for outpatient surgical settings.
If a CPT code is not on this list:
- The ASC will not be reimbursed, even if the procedure was performed
- The claim may be denied outright or flagged for compliance review
Why Matching the Surgeon’s CPT Codes Is Risky?
A common mistake is assuming the ASC should bill the exact same CPT codes as the physician. This creates both revenue leakage and audit exposure because physicians may report CPTs reflecting clinical complexity, but ASCs must reflect facility resources and eligibility. Also, some physician-billed CPTs are not ASC-approved, and modifier usage may differ between professional and facility claims.
ASC CPT billing is not similar to physician billing; rather, it is a distinct reimbursement model governed by facility-specific rules, packaging logic, and CMS eligibility criteria.
What Are ASC CPT Codes?
ASC CPT codes are standardized procedure identifiers from the Current Procedural Terminology used to report services performed in an Ambulatory Surgery Center. Each code is a 5-digit numeric value that translates a clinical service into a billable procedure for payers, including programs administered by CMS. Many ASCs depend on a specialized ASC billing services provider to handle CPT coding, modifier application, and CMS compliance to reduce claim denials and improve reimbursement accuracy.
CPT Code Structure in ASC Billing
CPT codes are organized into numeric ranges that align with service categories commonly performed in ASCs. These ranges help distinguish surgical work from anesthesia and diagnostic services, which is critical for correct claim submission and reimbursement logic.
Key CPT Code Ranges Used in ASCs
- Surgical procedures (10000–69999)
This is the primary range used in ASCs and includes most outpatient surgeries such as orthopedic procedures, GI endoscopy, ophthalmology, and general surgery. - Anesthesia services (00100–01999)
Used to report anesthesia administration related to surgical procedures performed in the ASC setting. - Ancillary and diagnostic services (80000–89999)
Includes laboratory, pathology, and other diagnostic procedures that may support surgical care or pre-operative evaluation.
What Are The Common ASC Coding And Billing Codes?
Ambulatory Surgery Centers (ASCs) primarily rely on CPT codes to define the procedures performed, supported by highly relevant modifiers that clarify service context, complexity, and payment rules. These modifiers are essential in ASC billing because they directly impact reimbursement accuracy and claim validation. This ASC billing guide highlights the most frequently used ASC CPT codes along with the key modifiers that ensure correct coding, compliance, and clean claim submission.
Common ASC CPT Codes by Specialty
To understand how ASC billing works in real practice, it helps to look at CPT codes by specialty.
Each specialty relies on a different set of high-volume procedures.
Below are the most commonly used ASC CPT codes organized by specialty.
GI / Endoscopy CPT Codes
GI is the highest-volume ASC specialty within an Ambulatory Surgery Center environment. It is also the most denial-prone due to same-session coding conflicts and frequent Correct Coding Initiative (CCI) edits from CMS. Most revenue leakage occurs when add-on procedures are billed without validating bundling rules.
| CPT Code | Description | Notes |
|---|---|---|
| 45378 | Colonoscopy, flexible, diagnostic | Base code — add-ons must be checked for bundling |
| 45380 | Colonoscopy with biopsy | Cannot be billed with 45378 on same session (CCI edit risk) |
| 45385 | Colonoscopy with polypectomy | Separately payable when properly documented |
| 43239 | Upper GI endoscopy with biopsy | Often paired with colonoscopy; modifier 59 may be required |
| 43249 | Upper GI with esophageal dilation | Frequently bundled unless distinct service is supported |
| 43270 | EGD with lesion ablation | Higher complexity therapeutic endoscopy |
Orthopedic / Musculoskeletal CPT Codes
Orthopedic ASC billing has become more complex due to expanding procedure eligibility and updated CPT revisions. In 2026, musculoskeletal code updates require stricter validation of descriptors and device-related payment indicators before claim submission under CMS rules.
| CPT Code | Description | Notes | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 29881 | Knee arthroscopy with meniscectomy | High-volume outpatient orthopedic procedure | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 29827 | Shoulder arthroscopy with rotator cuff repair | Device-intensive — verify ASC PI before billing | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 29848 | Wrist arthroscopy | Common ambulatory upper-extremity procedure | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 64721 | Carpal tunnel neuroplasty | One of the most frequent ASC hand procedures | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 27447 | Total knee arthroplasty | Must confirm ASC-approved list eligibility | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 29826 | Shoulder arthroscopy with acromioplasty | Often performed with 29827 — CCI check required | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CPT Code | Description | Notes |
|---|---|---|
| 66984 | Cataract extraction with IOL implant | Core high-volume ASC procedure |
| 66821 | YAG laser capsulotomy | Strong ASC vs office reimbursement differential |
| 65855 | SLT (selective laser trabeculoplasty) | Increasing ASC utilization due to site-of-service shift |
| 67228 | PRP laser photocoagulation | Retinal procedure with strict documentation requirements |
| 66682 | Repair of iris | Specialized ophthalmic reconstruction |
| 66683 | Implantation of iris prosthesis | Newer, higher-complexity implant procedure |
Pain Management CPT Codes
Pain management coding in ASCs is heavily influenced by packaging rules for imaging guidance services. Fluoroscopy and CT guidance codes (e.g., 77003, 77012) are often bundled under CMS rules, making pre-billing PI validation essential under Centers for Medicare & Medicaid Services guidelines.
| CPT Code | Description | Notes |
|---|---|---|
| 62323 | Epidural steroid injection, lumbar/sacral | Imaging guidance often separately reviewed |
| 64483 | Transforaminal epidural, lumbar | Requires LT/RT modifiers when bilateral |
| 64490 | Facet joint injection, cervical | Common diagnostic and therapeutic procedure |
| 64493 | Facet joint injection, lumbar | Frequently subject to frequency edits |
| 64635 | Radiofrequency ablation, lumbar facet | Higher reimbursement but strict documentation |
| 20610 | Arthrocentesis, major joint | Common crossover with orthopedics |
Urology CPT Codes
Urology coding is undergoing one of the most significant transformations in 2026, particularly in prostate biopsy workflows. The transition to approach-specific CPT codes requires precise documentation; legacy use of 55700 without supporting procedural detail increases audit exposure under CMS review standards.
| CPT Code | Description | Notes |
|---|---|---|
| 52000 | Cystourethroscopy, diagnostic | Base endoscopic urology procedure |
| 52310 | Cystoscopy with removal of calculus | Therapeutic stone management |
| 52441 | Cystoscopy with prostatic implant (UroLift) | Device pass-through rules apply |
| 52442 | Additional prostatic implants (add-on) | Must follow correct add-on billing hierarchy |
| 55700 | Prostate biopsy, needle | Being replaced in many cases by 2026 codes |
| 55707 | Prostate biopsy, transperineal (new 2026) | Approach-specific code |
| 55715 | Prostate biopsy, MRI fusion guidance (new 2026) | High scrutiny due to imaging dependency |
General Surgery / GYN CPT Codes
General surgery and GYN procedures frequently involve multiple CPT codes per operative session, making Correct Coding Initiative (CCI) edits a major compliance risk. Proper sequencing, modifier application, and bundling validation are essential to prevent denials and ensure alignment with Centers for Medicare & Medicaid Services reimbursement logic.
| CPT Code | Description | Notes |
|---|---|---|
| 47562 | Laparoscopic cholecystectomy | High-volume ASC general surgery procedure |
| 49650 | Laparoscopic inguinal hernia repair | Common outpatient hernia repair |
| 49652 | Laparoscopic ventral hernia repair | Higher complexity abdominal wall repair |
| 58571 | Hysteroscopy with biopsy | Frequently bundled with diagnostic services |
| 58563 | Hysteroscopy with endometrial ablation | Therapeutic gynecologic procedure |
| 57522 | LEEP procedure, cervix | Common outpatient gynecology procedure |
| 19120 | Excision of breast lesion | Often requires careful margin documentation |
What Are the Common Modifiers For ASC CPT Billing?
In ASC billing under the CMS framework, modifiers are not optional clarifiers. Instead, they directly control payment logic and denial outcomes. Here’s a list of some common ASC modifiers:
| Modifier | Meaning | ASC Billing Impact |
|---|---|---|
| 59 | Distinct procedural service | Used to bypass CCI edits when procedures are truly separate; requires strong documentation support |
| 73 | Discontinued before anesthesia | ASC may bill reduced facility cost; reflects halted procedure before anesthesia start |
| 74 | Discontinued after anesthesia | Full facility claim allowed but commonly triggers payer review due to partial completion |
| RT / LT | Right / Left side designation | Required for laterality; missing RT/LT is a preventable denial reason in ASC claims |
| 52 | Reduced services | Indicates partial completion; payment adjusted based on reduced procedure scope |
| 51 | Multiple procedures | Not used in ASC facility claims; often physician-only and causes rejection if applied |
What Are ASC Payment Indicators (ASC PIs)?
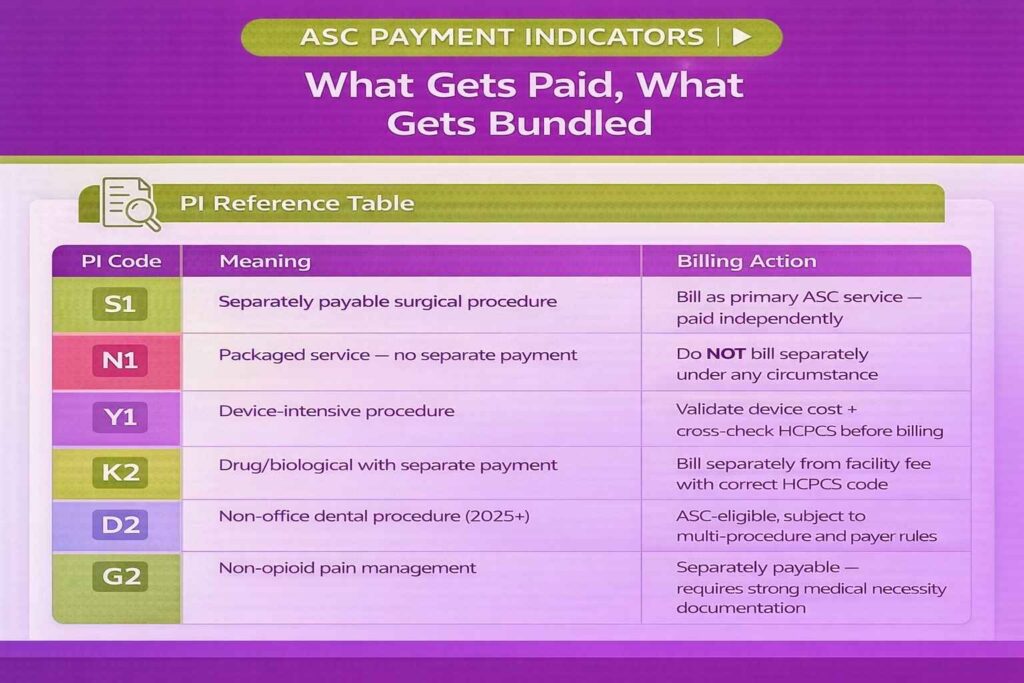
ASC Payment Indicators (PIs) are one of the most operationally important rules in ASC billing under the Ambulatory Surgery Center payment system governed by CMS. While CPT codes define what procedure was performed, ASC PIs determine whether and how it gets paid. They define how a procedure is reimbursed under the ASC fee schedule and are published in CMS Addenda AA and BB.
Addendum AA contains the list of covered surgical procedures and their corresponding payment indicators, while Addendum BB provides additional detail on payment rules and packaging logic. These files are updated quarterly, meaning ASC billing rules shift throughout the year based on CMS policy updates.
A CPT code that looks separately billable clinically may be fully packaged or conditionally payable under ASC rules. If the payment indicator says “packaged,” no separate line item should ever be billed, even if the service appears significant from a clinical standpoint. Ignoring this structure is a direct cause of denials, compliance flags, and lost revenue integrity.
ASC Payment Indicator Reference Table
ASC Payment Indicators determine whether a service is paid separately, bundled, or subject to special packaging conditions under the ASC payment system administered by CMS.
| ASC PI | Meaning | Billing Implication |
|---|---|---|
| S1 | Separately payable surgical procedure | Bill as primary ASC service; paid separately under ASC fee schedule with no additional bundling restrictions |
| N1 | Packaged service (no separate payment) | Do not bill separately; cost is included in facility payment bundle |
| Y1 | Device-intensive procedure | Requires device cost validation; cross-check with Healthcare Common Procedure Coding System codes for proper reimbursement |
| K2 | Drug or biological with separate payment | Bill separately from facility fee using correct HCPCS code with full documentation |
| D2 | Non-office dental procedures (2025+) | ASC-eligible dental category; subject to multiple-procedure and payer-specific rules |
| G2 | Non-opioid pain management treatment | Separately payable ancillary service; requires strong medical necessity documentation |
How to Use ASC PIs in Daily Billing Workflow
To avoid denials, coders must verify each CPT code’s ASC PI in CMS Addendum AA before claim submission. This lookup ensures the code is actually payable in the ASC setting and correctly classified under current CMS rules.
Because CMS updates these indicators quarterly, ASC billing workflows must treat PI validation as a routine checkpoint, not a one-time setup task. Failing to incorporate updates can result in systemic billing errors across multiple claims, especially when procedure eligibility or packaging logic changes mid-year.
What Are Packaged vs. Separately Payable CPT Codes in ASC Billing?
In an Ambulatory Surgery Center, reimbursement is driven by a single bundled facility payment rather than itemized service billing. Under the fee structure defined by the Centers for Medicare & Medicaid Services, most services reported through the CPT are not individually reimbursed but instead packaged into the overall ASC facility rate.
What Is Always Packaged
The ASC facility fee includes a wide range of routine services that cannot be billed separately, regardless of documentation detail. This typically includes nursing care, standard post-operative recovery services, routine anesthesia monitoring, and most general supply-related costs. Even when these components are clearly documented in the operative record, they are considered part of the bundled payment structure and have no separate billing value.
What Can Be Separately Billed
Only specific categories fall outside the packaged payment logic. These include device-intensive procedures identified with a PI of Y1, select drug and biological codes reported through HCPCS, and approved pass-through device codes. These are exceptions, not the rule, and require strict validation against CMS guidelines before billing.
A key concept in ASC billing is device pass-through status. This is a temporary designation assigned by CMS that allows separate reimbursement for certain high-cost, newly approved devices. However, this status is time-limited and typically expires after two to three years once the device becomes incorporated into standard payment bundles.
Practical Billing Rule
The most reliable validation step is to check the CPT code in CMS Addendum AA. If the ASC Payment Indicator is N1, the service is fully packaged and must not be billed separately under any circumstance, even if the surgeon documents it as a distinct component of care.
Common Billing Error to Avoid
A frequent error in ASC claims is billing implant-related HCPCS codes alongside a Y1 CPT procedure without verifying whether those costs are already included in the bundled payment rate. This leads to duplicate billing assumptions, claim rejections, and compliance exposure during payer audits.
What Are Multiple Procedure Reduction Rules?
When more than one covered surgical CPT code is billed on a single claim in an Ambulatory Surgery Center, CMS applies a multiple procedure reduction to adjust reimbursement.
Core Payment Rule
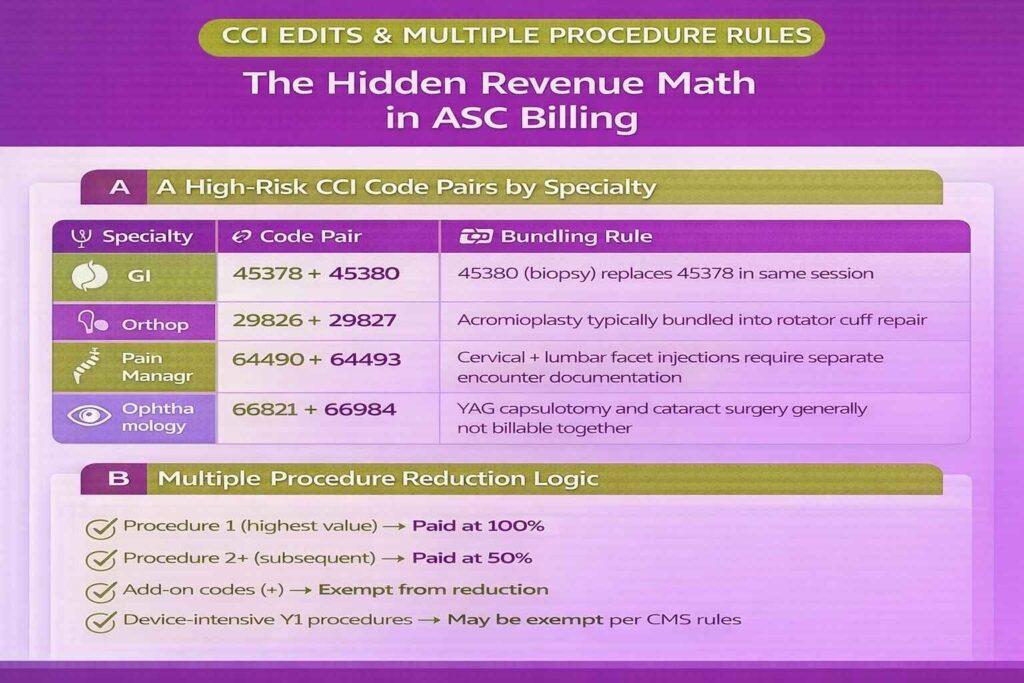
The standard methodology is straightforward: the highest-valued procedure is paid at 100% of the ASC allowable rate, while all subsequent eligible procedures are typically reimbursed at 50%. This structure ensures that reimbursement reflects incremental resource use rather than full duplication of facility payment for overlapping surgical episodes.
Most surgical CPT codes assigned an S1 payment indicator are subject to this reduction logic. These are the primary procedures performed in ASCs and represent the majority of multi-procedure claim scenarios.
Certain codes are exempt from multiple procedure reduction. These include add-on codes (identified in the CPT manual with a “+” symbol) and select device-intensive procedures where CMS rules explicitly exclude reduction due to cost structure or clinical necessity.
Practical Example
A common GI scenario illustrates this rule clearly. When CPT 45378 (diagnostic colonoscopy) and CPT 45385 (colonoscopy with polypectomy) are billed on the same claim, CMS assigns full payment to the higher-valued procedure, typically 45385, while 45378 is reduced to 50% of its allowable rate. The total reimbursement is therefore not the sum of both full fees but a weighted calculation based on hierarchy and valuation.
Why This Matters in ASC Operations
For high-volume centers, especially those performing multi-procedure cases in gastroenterology, orthopedics, or gynecology, this rule directly impacts revenue forecasting. Case mix planning must be based on net reimbursement after reduction rules, not raw CPT fee schedules. Failure to account for this leads to inflated revenue projections and inaccurate margin modeling at the ASC level.
How Do CCI Edits Impact ASC Code Pair Billing?
Correct Coding Initiative (CCI) edits are National Correct Coding policies maintained by the Centers for Medicare & Medicaid Services that define which CPT combinations cannot be billed together during the same surgical session. In an Ambulatory Surgery Center, these edits apply at the facility level in the same way they apply to physician claims, meaning both professional and institutional billing must comply.
CCI edits are one of the most important structural denial rules in ASC billing because they enforce bundling logic at the procedure level. Even when multiple services are documented, CMS assumes certain CPT codes are inherently inclusive of others and therefore not separately payable.
High-Risk CCI Code Pairs in ASC Billing
| Specialty | Code Pair | Rule |
|---|---|---|
| GI | 45378 + 45380 | 45380 (biopsy) replaces 45378 when performed in same session |
| Orthopedics | 29826 + 29827 | Acromioplasty is typically bundled into rotator cuff repair |
| Pain Management | 64490 + 64493 | Cervical and lumbar facet injections generally require separate encounter documentation |
| Ophthalmology | 66821 + 66984 | YAG capsulotomy and cataract surgery are typically not billable together |
These combinations represent common denial triggers because they appear clinically related but are structurally bundled under CMS logic.
Limited Override Mechanism For Modifier 59
Modifier 59 is the primary tool used to override a CCI edit, but its use is strictly conditional. It is only valid when documentation clearly supports that procedures were performed at different anatomical sites, through separate incisions, or during distinct operative sessions. Without this level of specificity, modifier 59 will not prevent denial and may trigger audit review.
What Are the Most Common ASC Billing and Coding Mistakes?
Accurate ASC billing and coding help Ambulatory Surgery Centers (ASCs) ensure compliance, maximize reimbursement, and prevent audits. By understanding ASC billing guidelines, practices can reduce claim denials and avoid revenue loss. However, even experienced staff can make common mistakes that lead to claim denials. Working with experienced ASC billing companies can help reduce coding errors and improve claim accuracy. Here are some common billing and coding mistakes ASC billers and coders make:
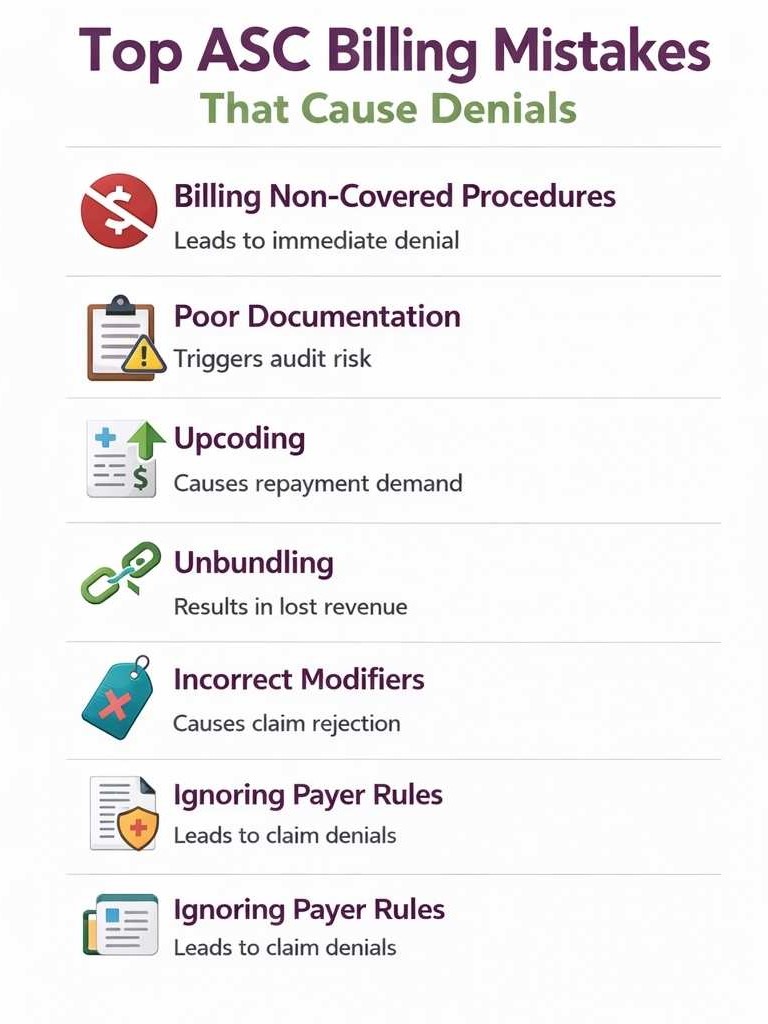
1. Coding for Non-Covered Procedures
Submitting claims for procedures that are not covered by the patient’s insurance or Medicare is a common error. This can lead to immediate denials and compliance issues. ASCs should verify coverage and document medical necessity before billing.
2. Failing to Document Properly
Proper documentation supports medical necessity and the services provided. Missing operative notes, incomplete histories, or absent signatures can trigger denials. Accurate, timely documentation is the key to ASC billing and coding compliance.
3. Upcoding
Upcoding occurs when a procedure or service is reported at a higher level than was actually performed. This can result in overpayment requests or penalties. Staff should strictly follow CPT, ICD-10, and HCPCS coding guidelines.
4. Unbundling
Unbundling is the incorrect separation of services that should be billed as a single bundled code. This practice can trigger denials for fraudulent billing. ASCs must accurately review payer rules and codes to avoid unbundling.
5. Incorrect Use of Modifiers
Modifiers, such as RT/LT, 52, 59, or TC, are frequently misapplied in ASC billing. Using the wrong modifier can cause denials, underpayment, or audit triggers. Staff should ensure modifiers accurately reflect the procedure and service for ASC billing and coding.
6. Failing to Verify Payer-Specific Rules
Every insurance payer has different rules for coverage, prior authorization, or bundled services. Failing to follow these guidelines can result in claim denials or delayed reimbursement. ASCs should maintain an updated payer policy for all commonly performed procedures.
7. Not Updating for 2026 CPT Changes
Annual CPT revisions can significantly impact procedure descriptors and reporting rules, especially in urology (prostate biopsy codes), musculoskeletal procedures, and vascular interventions. Using outdated code descriptors leads to mismatched claims and increased denial risk.
What Are the 2026 ASC CPT Code Updates and How They Impact ASCs?
In 2026, reimbursement policy changes from the Centers for Medicare & Medicaid Services significantly expanded both coverage and coding complexity for the Ambulatory Surgery Center environment. These updates directly impact how CPT codes are applied across high-volume surgical specialties.
CMS Payment Update Overview
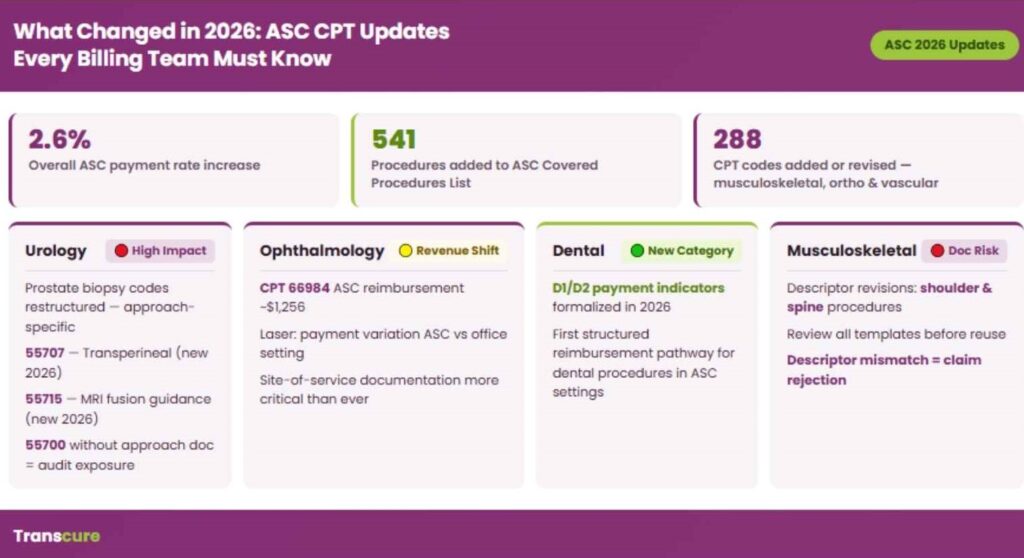
The ASC payment system saw a 2.6% overall rate increase, consistent with 2025 adjustments. While modest, this update was accompanied by structural expansion rather than pure fee schedule growth. CMS added 560 procedures to the ASC Covered Procedures List, representing one of the largest annual eligibility expansions in recent years.
In parallel, 288 CPT codes were newly added or revised, with the majority concentrated in musculoskeletal, orthopedic, and vascular surgery. These changes require ASCs to reassess internal charge master logic and coding templates, particularly for high-frequency outpatient procedures.
Specialty-Level Impact
Urology experienced a major structural shift with prostate biopsy coding. The 55707–55715 CPT range was restructured to better distinguish approach methods and imaging guidance, increasing documentation specificity requirements.
Ophthalmology continues to show widening reimbursement divergence between ASC and office settings. The cataract procedure CPT 66984 is now set at approximately $1,256 in ASC reimbursement, reinforcing cataract surgery as a core high-volume ASC driver while laser procedures show increasing payment variation.
Dental services were formally expanded with new D1/D2 payment indicators, marking the first structured pathway for certain dental procedures to be reimbursed in ASC settings.
Musculoskeletal coding also underwent descriptor revisions, particularly for shoulder and spine procedures. Existing documentation templates must be reviewed before reuse to avoid a mismatch with updated CPT definitions.
Device and Policy Updates
CMS introduced three new device pass-through categories effective January 2026, expanding temporary separate reimbursement pathways for high-cost implantable technologies. These categories remain time-limited and transition into bundled payment structures over time.
Finally, ASC billing must now align with CMS’s quarterly update cadence, with Addendum AA and BB revisions scheduled for April, July, and October 2026. This makes continuous CPT and ASC Payment Indicator monitoring a required operational function rather than an annual update task.
What are the best ASC CPT Coding Practices to Follow?
Achieving a high clean-claim rate in an Ambulatory Surgery Center depends on strict alignment between documentation, coding rules, and payer logic under the Current Procedural Terminology. Modern EMRs for ASC billing streamline CPT coding, automate documentation workflows, and help reduce manual errors that often lead to claim denials.
Verify CMS ASC Eligibility Before Scheduling
Always confirm the CMS ASC Covered Procedures List before scheduling, not during coding or claim submission. This prevents non-covered procedures from entering the revenue cycle and eliminates avoidable denial risk at the source.
Use CMS Addendum AA for Payment Indicator Checks
Before adding any new procedure to the service mix, review the CPT Payment Indicator (PI) in CMS Addendum AA. This determines whether a service is separately payable or packaged into the ASC payment, directly impacting reimbursement accuracy.
Maintain a Quarterly CPT Update Cycle
Integrate CPT and ASC rule updates into a fixed quarterly schedule. This ensures alignment with CMS updates and reduces exposure to outdated coding logic as payer rules evolve.
Audit Modifier 59 Usage Monthly
Conduct monthly audits of Modifier 59 usage. Any claim without clear operative documentation supporting a distinct procedural service should be flagged. Improper use remains one of the highest-risk triggers under Centers for Medicare & Medicaid Services review standards.
Build Payer-Specific CPT Rule Matrices
Maintain structured CPT rule sets for Medicare, Medicare Advantage, and commercial payers. Bundling rules and CCI enforcement differ across payer types, making standardized logic essential for clean claim performance.
Train Coders on ASC vs Physician Billing Rules
Ensure coding teams clearly understand the difference between ASC facility billing and physician professional billing. Misapplied physician-side logic is a common source of modifier and reimbursement errors in ASC environments.
Conclusion:
ASC CPT coding directly impacts reimbursement, denials, and audit risk in an Ambulatory Surgery Center. Every CPT code, modifier, and payment indicator must be accurate to avoid revenue loss. With strict oversight from the Centers for Medicare & Medicaid Services and frequent updates, even small errors can lead to denials or underpayments. High-performing ASCs prevent this by verifying eligibility early, validating payment indicators, and auditing coding regularly, which leads to cleaner claims, fewer denials, and better reimbursement outcomes. For a clearer breakdown of each step in the revenue cycle, an ASC billing process guide can help ASCs understand coding, claim submission, and reimbursement workflows in detail.






