CPT code 33249 is a surgical procedure code used to report the insertion or replacement of a permanent implantable cardioverter-defibrillator (ICD) system with transvenous leads in a single or dual chamber configuration. It applies when the physician implants both the pulse generator and the transvenous lead(s) as a complete system or replaces an existing complete system. This code is used in facility settings for patients who meet Medicare NCD or payer-specific criteria for ICD implantation.
What Is the Description of CPT Code 33249?
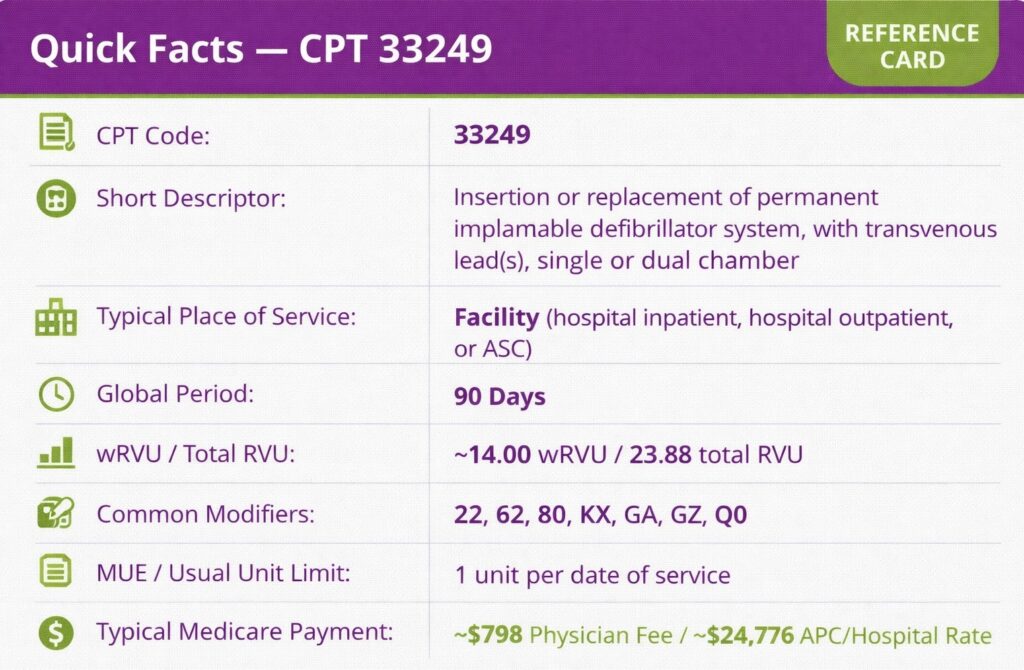
CPT code 33249 is defined by the AMA as: “Insertion or replacement of permanent implantable defibrillator system, with transvenous lead(s), single or dual chamber.”
It covers both new implantations and complete system replacements, and applies to both single and dual chamber configurations under a single code descriptor.
What Does the Implantable Defibrillator System Include for CPT Code 33249?
The system reported under code CPT 33249 consists of a pulse generator, implanted subcutaneously in the chest or abdomen, and one or more transvenous leads threaded through the venous system into the heart chambers. The leads sense cardiac rhythm and deliver defibrillation shocks when a life-threatening arrhythmia is detected. Fluoroscopy guidance used during lead placement is bundled into CPT code 33249 and may not be billed separately.
How Does CPT Code 33249 Differ From CPT Codes 33240, 33230, and 33231?
These codes cover partial system procedures and must not be substituted for 33249 CPT code when a complete system is implanted or replaced:
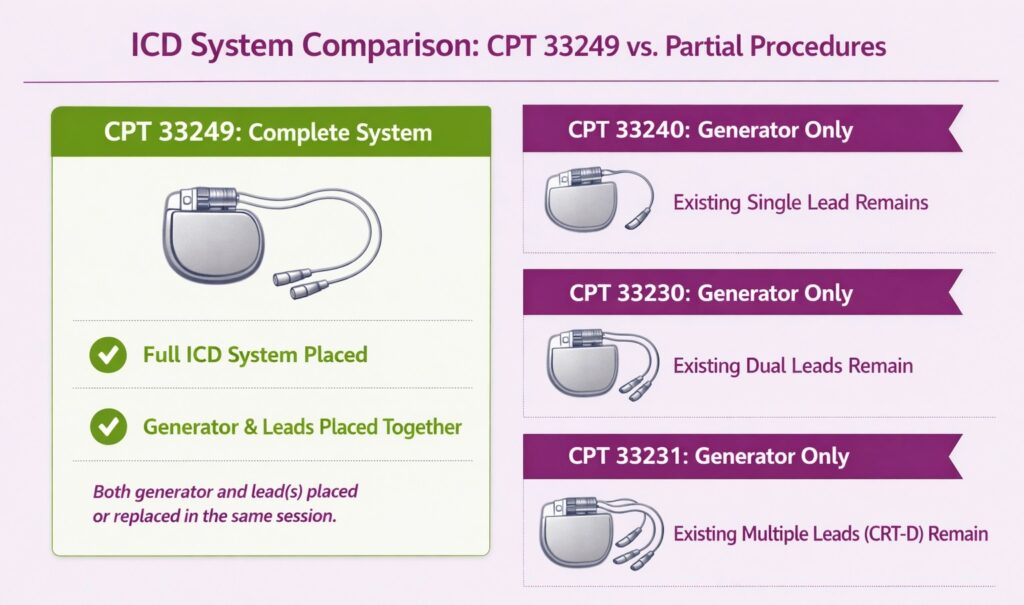
- CPT 33240: Insertion of ICD pulse generator only, with existing single lead; used when only the generator is replaced, and the lead remains in place
- CPT 33230: Insertion of ICD pulse generator only, with existing dual leads
- CPT 33231: Insertion of ICD pulse generator only, with existing multiple leads (CRT-D configuration)
CPT code 33249 is the correct code when both the generator and lead(s) are placed or replaced in the same operative session. If the clinical scenario is different, explore our cardiology CPT code cheat sheet to find and bill the correct procedure code.
What Are the Modifiers for CPT Code 33249?
CPT code 33249 is reported with modifiers to indicate unusual procedural circumstances, coverage status, or clinical trial participation.
Modifier 22: Increased Procedural Services
Modifier 22 is used when the work required substantially exceeds what is typically involved, for example, significant anatomical challenges, prior device pocket complications, or lead extraction required before new system placement. Append modifier 22 with a cover letter documenting the increased time and complexity.
Modifier 62: Two Surgeons
Modifier 62 is used when two surgeons of different specialties each perform distinct portions of the procedure and bill separately. Both surgeons append modifier 62 to the CPT 33249 code, and each must document their individual contribution in the operative report.
Modifier 80: Assistant Surgeon
Modifier 80 is used when a physician serves as an assistant surgeon during the procedure. Verify payer policy before appending, as some payers do not separately reimburse assistant surgeon services for CPT code 33249.
Modifier KX: Medical Necessity Requirements Met
Modifier KX is appended to confirm that the patient meets all applicable Medicare coverage criteria under NCD 20.4. Without modifier KX, Medicare may deny the claim. Ensure the medical record fully documents the qualifying indication before appending.
Modifier GA: Waiver of Liability on File
Modifier GA is used when the provider expects Medicare may deny the service and has obtained a signed Advance Beneficiary Notice (ABN) from the patient. Append modifier GA when the clinical indication does not clearly meet NCD 20.4 criteria, but the procedure is proceeding.
Modifier GZ: Item or Service Expected to Be Denied
Modifier GZ is used when the provider expects a denial, and no ABN has been obtained. It signals the provider does not expect Medicare payment, and the patient cannot be billed. Append modifier GZ only when no ABN is on file, and the service is unlikely to meet coverage criteria.
Modifier Q0: Investigational Clinical Service / Registry Submission
Modifier Q0 is used when CPT code 33249 is performed as part of a Medicare-approved clinical research study. It signals the service is investigational. Include the 8-digit clinical trial registration number on the claim when appending modifier Q0.
What Are the Medicare Coverage and NCD Criteria for CPT Code 33249?
Medicare coverage for CPT code 33249 is governed by NCD 20.4 (Implantable Automatic Defibrillators), effective February 15, 2018. Coverage is nationally determined and requires the patient to meet one of the following indications:
- Personal history of sustained ventricular tachyarrhythmia (VT) or cardiac arrest due to ventricular fibrillation (VF) not associated with an acute MI and not due to a transient or reversible cause
- Prior MI with measured LVEF ≤ 30%, excluding patients with NYHA Class IV heart failure, recent CABG/PCI within 3 months, or MI within the past 40 days
- Severe ischemic dilated cardiomyopathy, no prior sustained VT or VF, NYHA Class II or III heart failure, LVEF ≤ 35%, excluding patients with recent CABG/PCI or MI
- Severe non-ischemic dilated cardiomyopathy, no prior cardiac arrest or sustained VT, NYHA Class II or III heart failure, LVEF ≤ 35%, on optimal medical therapy for at least 3 months
- Documented familial or genetic disorder with high risk of life-threatening tachyarrhythmias (e.g., long QT syndrome, hypertrophic cardiomyopathy)
- Existing ICD replacement due to end of battery life, elective replacement indicator (ERI), or device/lead malfunction
For indications 2 through 5, a formal shared decision-making encounter using an evidence-based decision tool must occur prior to initial ICD implantation. Across all indications, LVEF must be measured by echocardiography, radionuclide imaging, cardiac MRI, or catheter angiography, and the patient must be clinically stable at the time of implant.
Which Documents Are Required For CPT Code 33249?
Documentation for CPT code 33249 must support the medical necessity of ICD implantation and the complete system procedure performed.
Required documents checklist:
- Operative report confirming insertion of both pulse generator and transvenous lead(s)
- LVEF measurement with imaging modality documented (echo, nuclear, MRI, or angiography)
- Qualifying diagnosis and clinical indication matching an NCD 20.4 covered category
- Shared decision-making encounter documentation (required for primary prevention indications)
- Evidence of optimal medical therapy duration where applicable (non-ischemic CMP — minimum 3 months)
- Device implant record including manufacturer, model, and serial numbers for generator and lead(s)
- Prior authorization approval from the payer where required
- Signed ABN (if modifier GA is appended)
- Clinical trial registration number (if modifier Q0 is appended)
- Postoperative device check and programming report within the 90-day global period
What is the Cost of CPT Code 33249?
The cost of CPT code 33249 varies by payer, geographic location, and place of service.
RVUs & Medicare Payment
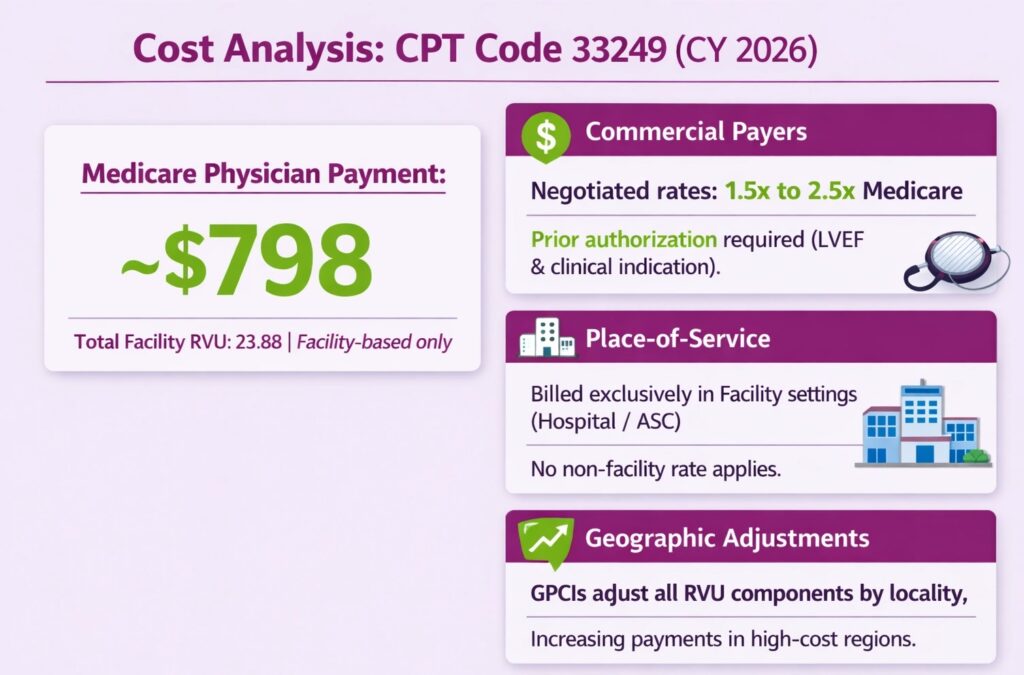
CPT code 33249 has a total facility RVU of 23.88 for CY 2026 per the Medicare Physician Fee Schedule. At the national unadjusted non-QP conversion factor of $33.40, the Medicare facility-based physician payment is approximately $798 per case. No non-facility rate is established for CPT code 33249, as this procedure is performed exclusively in facility settings.
Commercial Payers
Commercial payers negotiate rates that typically exceed Medicare by 1.5× to 2.5× for major cardiac device procedures. Prior authorization is required by most commercial payers and must reference the clinical indication, LVEF measurement, and supporting documentation. Actual allowed amounts vary by contract and network status.
Place-of-Service & Geographic Adjustments
CPT code 33249 is billed exclusively in facility settings, hospital inpatient, hospital outpatient, or ASC. No non-facility rate applies. GPCIs adjust all three RVU components by locality, with high-cost regions receiving higher per-unit payments.
What Are Example Clinical Scenarios or Use Cases for CPT Code 33249?
CPT code 33249 applies in facility-based encounters where a complete ICD system, pulse generator, and transvenous lead(s) are implanted or replaced for a patient meeting NCD or payer-approved indications.
Scenario 1: Ischemic Cardiomyopathy with Reduced Ejection Fraction (Primary Prevention)
ICD-10: I25.5 (Ischemic cardiomyopathy)
The patient has a history of prior MI with an LVEF of 28% measured on echocardiogram, NYHA Class II heart failure, and has been on optimized guideline-directed medical therapy. No CABG or PCI has been performed within the past 3 months. A formal shared decision-making encounter is completed. The electrophysiologist implants a dual-chamber ICD system, supporting CPT code 33249 with modifier KX.
Scenario 2: Sustained Ventricular Tachycardia Following Prior Myocardial Infarction (Secondary Prevention)
ICD-10: I47.2 (Ventricular tachycardia)
The patient presents following an episode of sustained VT not associated with an acute MI or reversible cause. Cardiac workup confirms structural heart disease with reduced ejection fraction. The physician implants a single-chamber ICD system for secondary prevention, reporting CPT code 33249 with modifier KX.
Scenario 3: Non-Ischemic Cardiomyopathy with LVEF Below 35%
ICD-10: I42.0 (Dilated cardiomyopathy)
The patient has severe non-ischemic dilated cardiomyopathy, NYHA Class III heart failure, LVEF of 30% confirmed by cardiac MRI, and has completed more than 3 months of optimal medical therapy without improvement. Shared decision-making is documented. A dual chamber ICD is implanted, supporting CPT code 33249 with modifier KX.
What Are the CPT Code 33249 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for NCD compliance, documentation, bundling, global period management, and device credit obligations. Meeting these rules reduces denials and ensures correct payment.
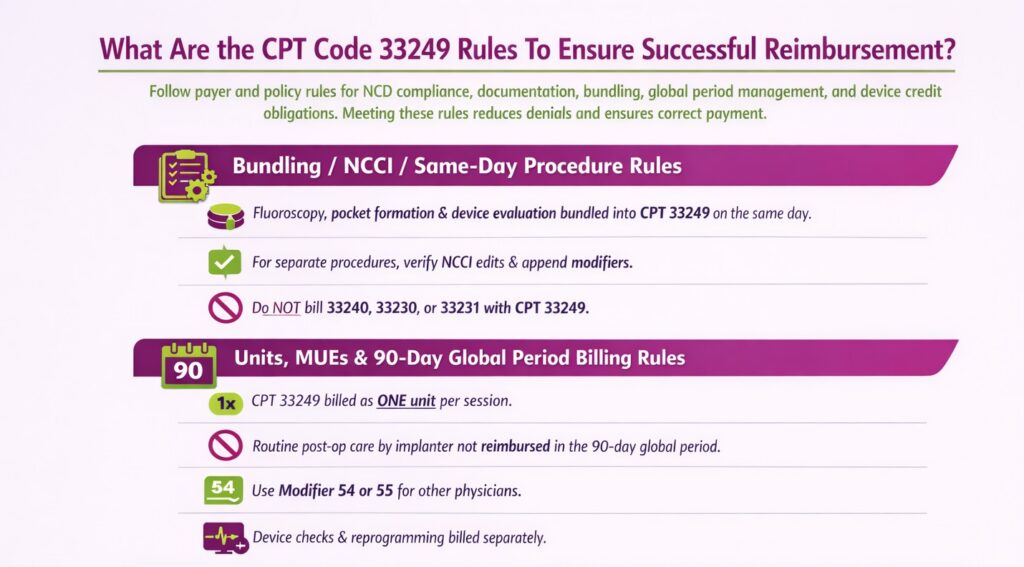
Bundling / NCCI / Same-Day Procedure Rules
Fluoroscopy, pocket formation, and device evaluation immediately following implant are bundled into CPT code 33249 and may not be billed separately on the same date. If a lead repositioning or separate cardiac procedure is performed at a distinct session or on a different anatomical site, verify NCCI edits and append the appropriate modifier before billing. Do not bill CPT 33240, 33230, or 33231 alongside CPT code 33249 for the same system implant. Only one system insertion code applies per operative session.
Units, MUEs & 90-Day Global Period Billing Rules
CPT code 33249 is billed as one unit per operative session.
- Medicare will not separately reimburse routine postoperative care by the implanting physician within the 90-day global period, including device checks and wound management.
- A different physician providing postoperative care during the global period appends modifier 54 (surgical care only) or modifier 55 (postoperative management only) as applicable.
- Remote or in-person device interrogations and programming evaluations performed after implant are separately billable using the appropriate device evaluation CPT codes (e.g., 93280–93284) and are not bundled into the global period.
- Shared decision-making services billed under the applicable E/M or HCPCS code prior to initial implantation are separately reimbursable and are not bundled into CPT code 33249
Device Credit and Replacement Rules Under Medicare
When CPT code 33249 is performed as a replacement due to device malfunction or early failure, Medicare’s device credit policy applies. If the replacement device is provided at no cost or at a reduced cost to the hospital by the manufacturer, the facility must reduce its claim accordingly. Failure to apply device credit on replacement claims is a documented compliance risk.
Physicians are not subject to device credit reduction. It applies to the facility claim only. Document the reason for replacement (end of battery life, ERI, or malfunction) clearly in the operative report to support the replacement indication under NCD 20.4.
Top Reasons For Denials Specific To 33249 & Quick Remedies
- Missing Modifier KX: Prevent by confirming NCD 20.4 criteria are met and appending modifier KX on every Medicare claim before submission.
- Missing or Incomplete Shared Decision-Making Documentation: Prevent by ensuring the shared decision-making encounter is documented in the medical record prior to implant for all primary prevention indications.
- Incorrect Code Selection (33249 vs. 33240/33230/33231): Prevent by confirming the operative report documents insertion of both generator and lead(s) before selecting 33249.
- Bundling Violations: Prevent by reviewing NCCI edits before adding fluoroscopy, pocket formation, or partial system codes to the same claim.
Why Does a Procedure as Specific as ICD Implantation Have Its Own Dedicated CPT Code?
Because CPT codes are built around procedure specificity, each distinct combination of technique, device type, and clinical intent gets its own code to ensure accurate reimbursement and clear documentation of what was actually performed. To understand why 33249 exists separately from 33240 or 33230, rather than being billed as a variation of the same procedure, you need to know the types of medical CPT codes at a foundational level.