
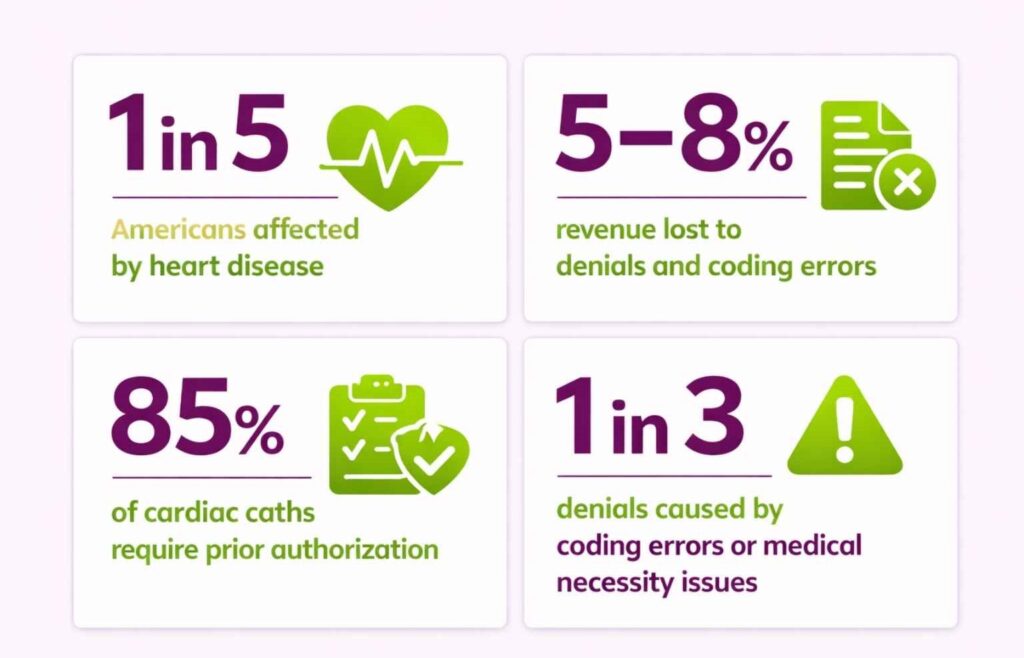
As we know, heart disease is the leading cause of death in the United States (about 1 in 5 Americans), which means cardiology visits are high-volume. However, cardiology practices lose 5 to 8% of revenue to denials and coding errors. That’s because cardiology medical billing demands specialized expertise.
Cardiac practices handle complex procedures, such as EKGs, echos, and device implants, which require pre-authorization. Moreover, any cardiology billing service provider also has to navigate strict documentation requirements and payer rules to maximize payments.
Precise workflows and upfront verification are what separate high-performing cardiology practices from those leaving money on the table. Read on for a deep dive into the cardiology billing process, common errors, best practices, and how billing partners like Transcure help you optimize every step.
What Is the Difference Between Cardiology Medical Billing and Other Specialties?
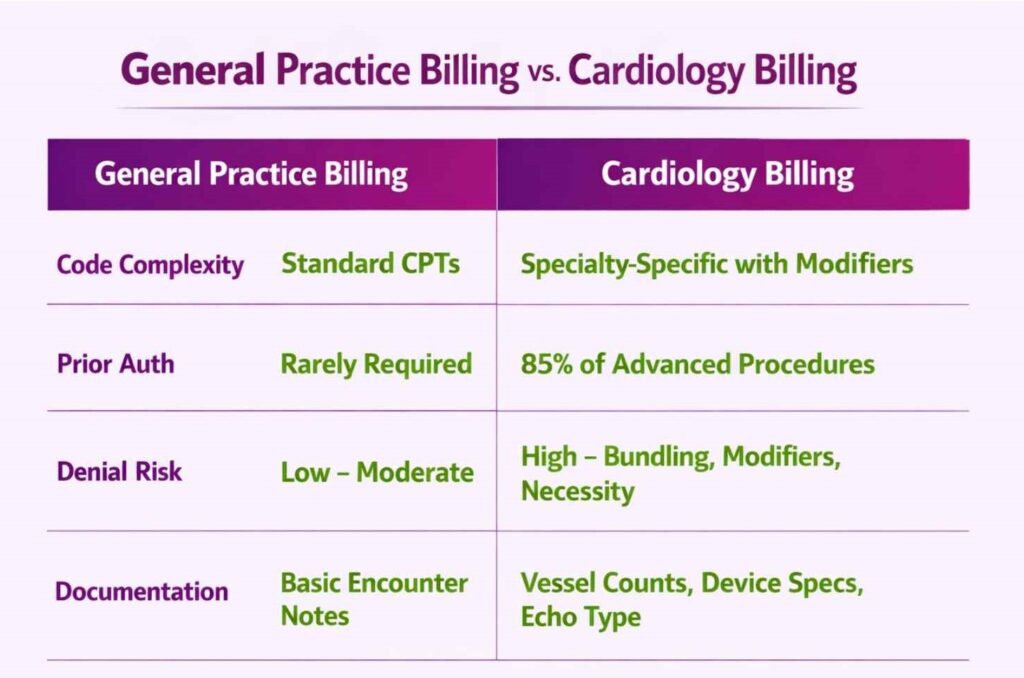
Cardiology RCM differs from general practice billing in several ways. Cardiology involves more complex coding and workflows, so practices often benefit from dedicated cardiology billers. Key differences include:
- Specialized Procedures and Codes: Cardiology uses a wide range of unique CPT codes and linked ICD codes. From stress tests to device implants, each code comes with specific modifiers. The coding complexity alone makes generalist billers a liability.
- Prior Authorization: About 85% of cardiac catheterizations require advance approval. Many cardiology tests, including imaging, EP studies, and devices, need pre-authorization before scheduling. A specialized cardiology billing team like Transcure tracks all payer rules so procedures aren’t canceled for missing approvals.
- Strict Documentation: Cardiology medical billing needs highly detailed documentation. Ambiguous charts lead to denials. Staff must note exact procedures, such as vessel numbers, vessel graft, and device details, to satisfy insurers.
- High Denial Risk: Nearly one-third of cardiac billing denials arise from medical necessity issues and coding errors. Cardiology billers must be vigilant on bundles and modifiers that generalist billers might miss.
How the Cardiology Billing and Coding Process Works?
When you outsource cardiology billing, their dedicated team passes through a multi-step RCM tailored to the specialty. In broad terms, it begins at patient intake and ends with the appeal of denied claims. The steps below show how a cardiology medical billing partner manages each phase to ensure smooth reimbursement.
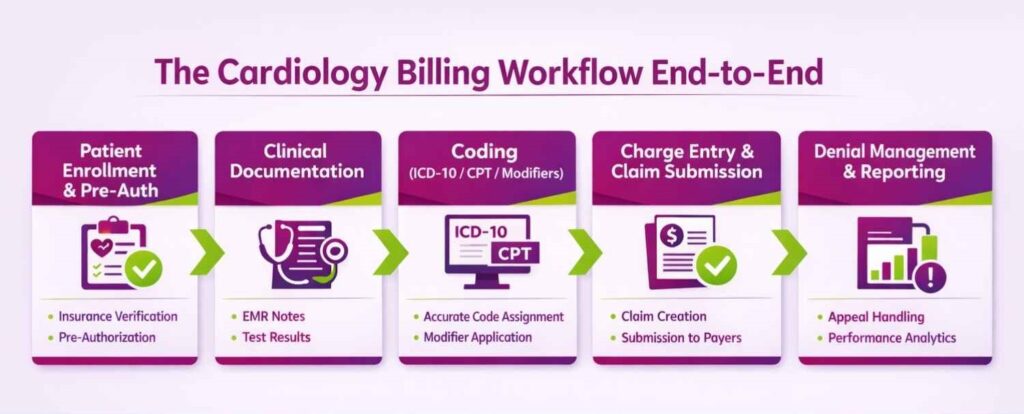
Step 1. Patient Enrollment and Pre-Authorization
Right from the front desk, cardiology billing begins with patient registration and insurance verification. Staff collect demographics, insurance information, and the reason for the visit. Practices can even outsource this cardiology billing step to remote patient intake managers.
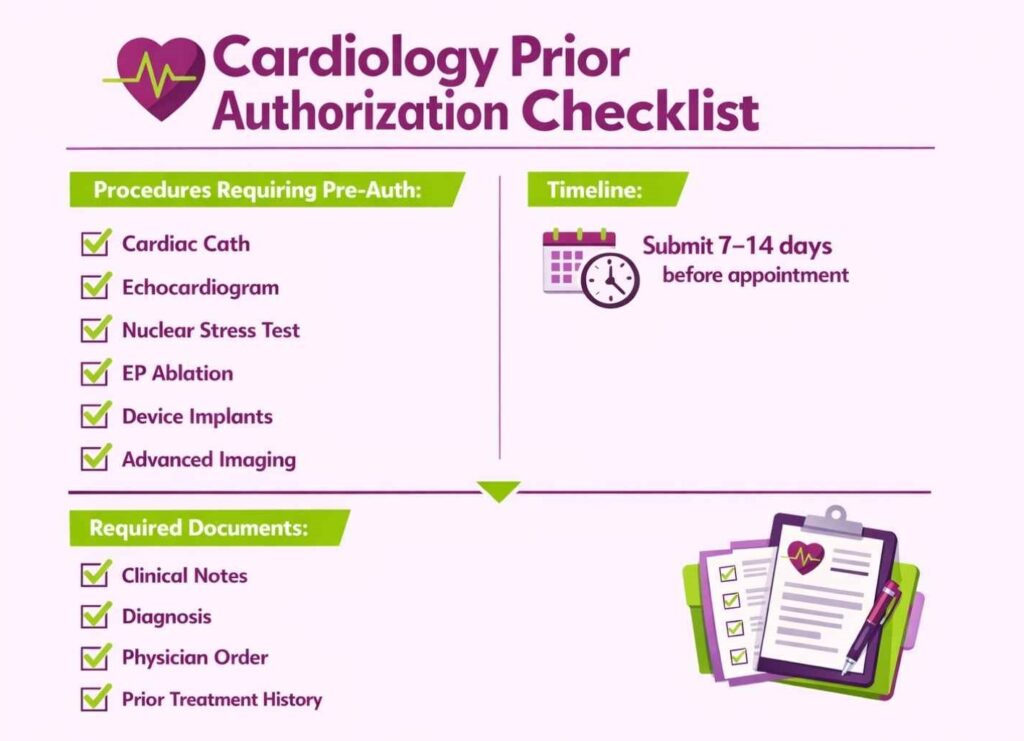
Another crucial step is checking coverage for cardiology procedures. Since an estimated 85% of heart caths and advanced tests need pre-approval, teams must submit prior authorizations before scheduling. For example, a planned left heart cath or echocardiogram typically requires an insurer’s approval 7 to 14 days in advance.
Step 2. Clinical Encounter and Documentation
During the appointment, the cardiologist performs exams and diagnostics, such as an EKG and stress test, and documents clinical findings. Clinical documentation must show why each test was done (symptoms, vital signs, risk factors) and what was performed.
For instance, if a patient has atrial fibrillation, the cardiologist should note symptom details and any cardiac rhythm strips. Cardiology billing and coding teams then use this documentation to select codes. Good practice is to train providers on documentation requirements and to use templates for cardiac cases.
Step 3. Coding with ICD-10, CPT, and Modifiers
Once documentation is finalized, coders assign ICD-10 diagnosis codes, CPT procedure codes, and modifiers. They match each condition, such as myocardial infarction or arrhythmia, to an ICD-10 code, and each service, like an echocardiogram, to a CPT code.
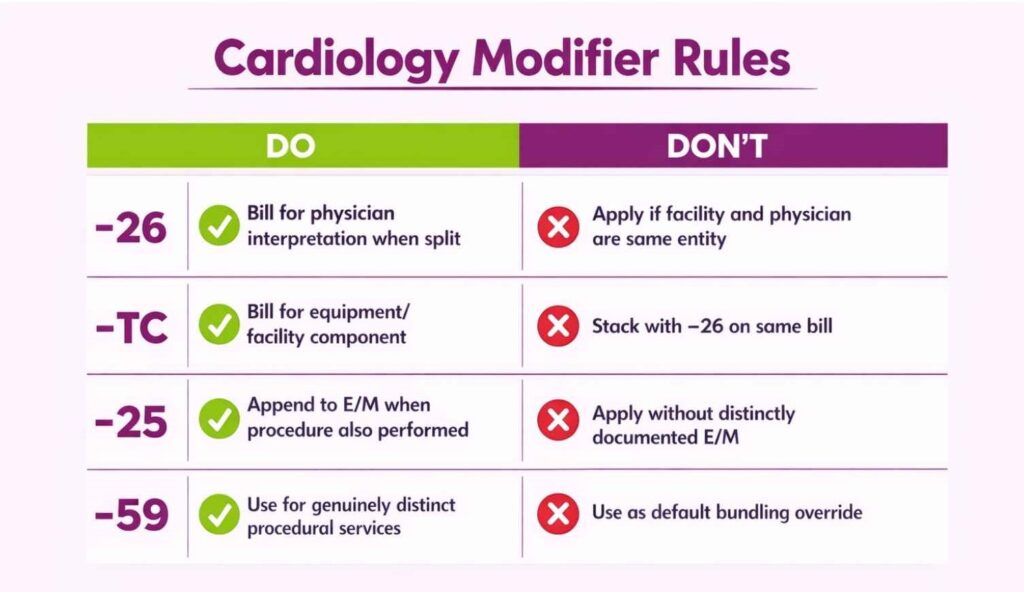
Modifiers adjust global services or professional splits. The –26 modifier covers physician interpretation, while –TC applies to equipment use. For a full breakdown of cardiology-specific codes and modifiers, refer to our dedicated Cardiology CPT Code Guide.
Step 4. Charge Entry and Claim Submission
After assigning codes, the cardiology billing staff enters coded charges into the practice management system. Each line on the claim corresponds to a service or supply, with the correct CPT, ICD-10, and modifier. It’s critical to verify eligibility and coverage one more time before submission.
Clearing houses will flag errors, including invalid code combinations or missing dates. The claim is then sent electronically to payers. Clean claims are the goal, so cardiology medical billing providers try to nail each of the RCM steps. Mistakes at this stage can lead to a rejected claim, so many practices rely on cardiology coding experts like Transcure.
Step 5. Denial Management and Reporting
If a claim is denied or underpaid, the practice must pursue appeals. An expert cardiology billing team will analyze each denial. For example, a denial for lack of prior authorization means one must submit documentation for the authorization approval.
Reporting is key in such cases, as tracking denial reasons and denial rates helps identify patterns, including frequent ICD-10 mismatches.
Evaluation and Management (E/M) Billing in Cardiology
E/M services are the backbone of any cardiology practice’s billing volume. Yet they’re also one of the most audited and miscoded areas in the specialty. Getting E/M billing right means understanding code selection, documentation standards, and how these visits interact with same-day procedures.
Understanding E/M Code Levels for Cardiology Visits
Cardiology uses the standard outpatient E/M range, 99202 to 99205 for new patients and 99211 to 99215 for established patients. Level selection is driven by either Medical Decision-Making (MDM) or total provider time. For most cardiology visits, MDM is the more defensible basis given the clinical complexity involved.
Higher-level codes (99204, 99205, 99214, 99215) are appropriate for cardiology patients with multiple chronic conditions, new diagnoses, or complex management decisions, which is the majority of the caseload. The mistake practices make is defaulting to mid-level codes out of caution, leaving significant revenue on the table.
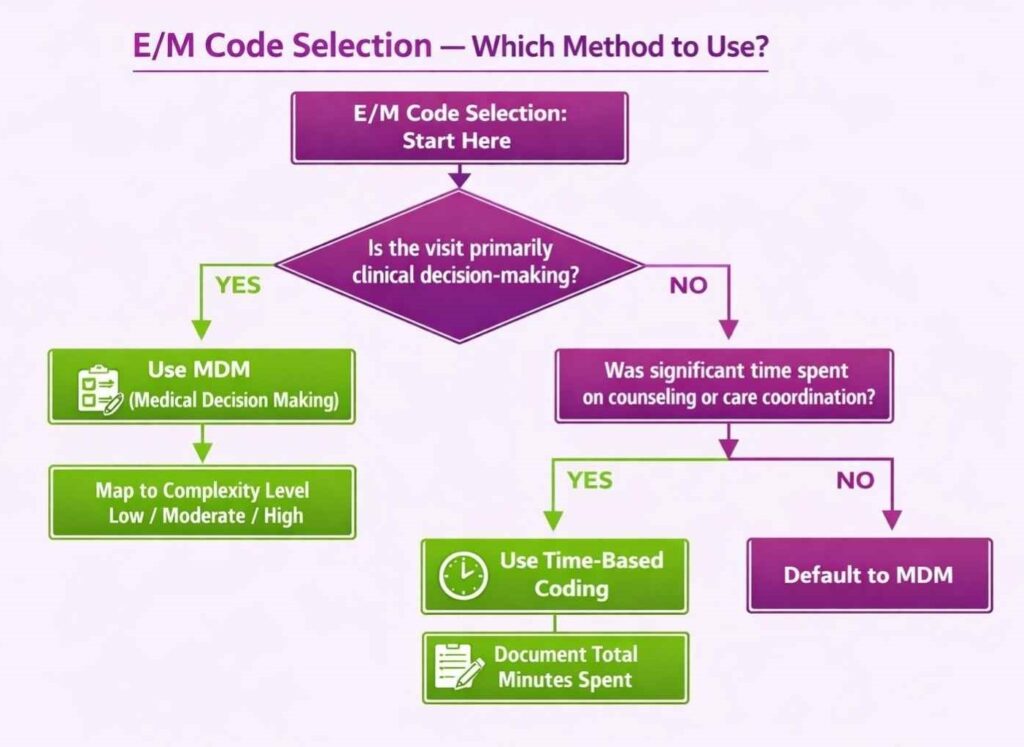
Medical Decision-Making (MDM) vs. Time-Based Coding
Since the 2021 AMA E/M overhaul, practices can select code level based on either MDM complexity or total time spent on the encounter date. This includes non-face-to-face work like reviewing test results and coordinating care.
MDM suits most cardiology encounters. A patient with heart failure, hypertension, and a recent cath easily qualifies for high-complexity MDM (99215) based on the number of problems, data reviewed, and risk of management decisions.
Time-based coding is useful when the visit involves extensive counseling or care coordination that isn’t fully captured by MDM, for example, a long conversation with a patient about an ICD implant decision. Document total time explicitly in the note when using this method.
How to Bill E/M Services with Same-Day Procedures
Billing an E/M on the same day as a procedure is legitimate, but only when the E/M represents a significant, separately identifiable service beyond the pre/post-procedure work already bundled into the procedure code.
Using Modifier –25 Correctly in Cardiology
Modifier –25 must be appended to the E/M code (not the procedure) to signal to payers that the visit was distinct. For example, if a patient comes in for a follow-up and an EKG is also performed, bill 99213-25 for the visit and 93000 for the EKG.
Where practices go wrong is applying –25 reflexively. Payers audit this modifier heavily. The E/M note must stand on its own, separate from the chief complaint, history, and clinical decision-making that goes beyond the procedure itself.
Common E/M Billing Mistakes in Cardiac Practices
- Undercoding visits: Out of audit fear, particularly for complex established patients who consistently qualify for 99214 or 99215
- Missing time documentation: When using time-based coding, making the code selection indefensible on audit
- Applying modifier –25 without adequate documentation: The E/M note must be clearly distinct from procedure notes.
- Incorrect new vs. established patient designation: A patient seen by a different provider in the same group within 3 years is established, not new.
- Not capturing all billable work: Care coordination, test review, and external record review count toward MDM and time, but only if documented
Cardiology Medical Billing Guidelines for Specific Procedures
Different cardiology procedures have their own billing rules, modifier requirements, and documentation standards. Getting these wrong is one of the fastest ways to trigger denials or leave reimbursement on the table. Below are billing guidelines for the most common and most complex cardiac services.
Echocardiography Billing Guidelines
Use the correct CPT for each echo type. A complete transthoracic echo is 93306, while limited or single-view studies carry different codes. Color Doppler and spectral Doppler are billed as add-ons (93325, 93320) to the base echo code.
Do not bill 2D and Doppler separately. 93306 covers both. Always apply the right modifiers: –TC for the facility/equipment component and –26 for the physician’s interpretation when split between a hospital and an independent cardiologist. Missing this split is a common denial trigger in outpatient cardiology settings.
Cardiac Catheterization Billing Guidelines
Bill right heart and left heart caths separately, 93451 for RHC and 93458 for LHC with coronary angiography. Documentation must specify the number of vessels interrogated and whether ventriculography was performed, as payers will scrutinize this against the code billed.
If stents are placed, add PCI codes (92928, 92933) based on the number of vessels treated. Use modifier –26 for the cardiologist’s interpretation and –TC for facility charges. Bundling errors here, particularly around ventriculography add-ons, are among the most common cath lab billing mistakes.
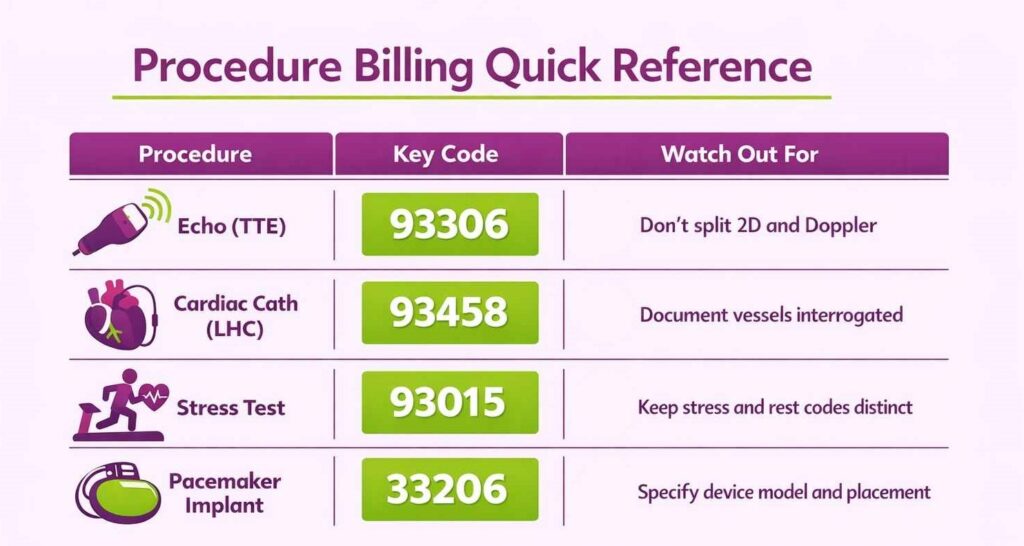
Stress Testing Billing Guidelines
For a standard pharmacologic or exercise stress ECG, use 93015. When an echocardiogram is performed during stress, add 93350 for the echo component. Some payers allow billing the base echo code if a resting echo was performed separately on the same day. Verify payer-specific rules before doing so.
Keep stress and rest test codes distinct. A baseline ECG (93000) and a stress study (93015) can both be billed if each was medically necessary and independently documented. Bundling them without justification is an audit risk.
Device Implantation (Pacemakers and ICDs) Billing Guidelines
For a single-chamber pacemaker implant, use 33206 for leads and generator, plus HCPCS L8679. For ICDs, use CPT 33249 or 33262, depending on whether it’s a new implant or replacement. If multiple leads or bilateral procedures are involved, apply appropriate modifiers or additional codes.
Documentation must specify the device model, lead placement site, and indication. Payers cross-reference device serial numbers and operative reports, so incomplete documentation here directly translates to denials or post-payment audits.
Nuclear Cardiology Billing Guidelines
Nuclear cardiology is a high-reimbursement, high-scrutiny area. Payers require strong medical necessity documentation and apply strict bundling rules across rest and stress imaging components.
Myocardial Perfusion Imaging: Codes and Documentation Rules
Myocardial perfusion imaging (MPI) is billed using 78451 to 78454, depending on whether imaging is single or multiple studies and SPECT or planar. The most common code is 78452 (SPECT MPI, multiple studies, rest and stress).
Key documentation requirements include the clinical indication, the type of stress used (exercise vs. pharmacologic), the radiopharmaceutical administered (billed separately via HCPCS, e.g., A9500 for Tc-99m sestamibi), and the physician’s interpretation report. The interpretation must be a standalone dictated report.
Payers frequently bundle rest and stress components or deny the pharmacologic stress agent separately. Ensure each component is coded and documented independently, and verify prior authorization requirements, as most commercial payers and Medicare require it.
Electrophysiology (EP) Study and Ablation Billing Guidelines
EP procedures are among the most complex to bill in cardiology. High procedure volume, multiple components, and aggressive bundling edits make this a frequent source of revenue leakage.
Billing EP Studies vs. Ablation Procedures
EP diagnostic studies and ablation procedures have distinct code families and must not be conflated. Diagnostic EP studies are coded in the 93600 to 93660 range. For example, 93619 for a comprehensive EP study without pacing or 93620 with pacing and induction.
Ablation procedures are coded separately. 93653 for SVT ablation, 93654 for ventricular tachycardia, and 93656 for atrial fibrillation (pulmonary vein isolation). When a diagnostic EP study is performed immediately before ablation in the same session, payers generally bundle the diagnostic study into the ablation code. Only bill the diagnostic EP study separately if it was a standalone session with distinct medical necessity.
Common EP Billing Errors and Bundling Traps
- Billing EP study + ablation as separate encounters: When performed in the same session, payers will deny or downcode the diagnostic component
- Missing 3D mapping add-on codes: 93613 (intracardiac mapping) is separately billable but frequently left off
- Incorrect ablation code selection: Arrhythmia type must match the ablation code; mismatches trigger medical necessity denials
- Not billing intracardiac echo (ICE): 93662 is a separately billable add-on when ICE guidance is used during EP procedures, but requires documentation of its use and interpretation
- Skipping prior authorization: EP ablations almost universally require pre-auth; proceeding without it is a guaranteed denial.
Telehealth and Remote Patient Monitoring (RPM) Billing in Cardiology
Telehealth and RPM have moved from pandemic-era workarounds to permanent revenue streams for cardiology practices, if billed correctly. The code set is specific, compliance requirements are strict, and the reimbursement opportunity is real. Practices that haven’t built these into their RCM workflows are leaving recurring monthly revenue uncaptured.
Telehealth Visit Codes and Documentation Requirements
Cardiology telehealth visits use the same E/M code range as in-person visits, 99202 to 99215, with the same MDM or time-based selection criteria. The distinction is in how the visit is delivered and documented. The claim must include place of service code 02 (telehealth, non-originating site) or 10 (patient’s home), and modifier –95 to indicate synchronous telehealth delivery.
Documentation must reflect that the visit occurred via telehealth, capture the platform used, confirm patient consent, and support the E/M level selected. Payers are auditing telehealth claims heavily, so a thin note with a telehealth tag is not sufficient.
Synchronous Audio-Video vs. Audio-Only Visits
Audio-video visits are the standard for telehealth reimbursement. Most commercial payers and Medicare require both audio and video for full E/M reimbursement under telehealth rules.
Audio-only visits are reimbursable under Medicare using 99441 to 99443, but at lower rates and with stricter limitations. Documentation must explicitly state why the video was not used. Many commercial payers do not reimburse audio-only at all.
Remote Patient Monitoring (RPM): Setup, Codes, and Compliance
RPM is particularly well-suited to cardiology. Blood pressure, heart rate, oxygen saturation, and weight monitoring are all clinically relevant and reimbursable. The key is building the enrollment and monthly billing workflow correctly from day one.
RPM Enrollment, Consent, and Device Requirements
Before billing any RPM code, three conditions must be met. The patient must have a chronic condition, must provide written consent documented in the chart, and must be set up with an FDA-cleared device that automatically transmits data. Manual patient-reported readings do not qualify.
The device must collect and transmit physiologic data without patient-initiated uploads. Bluetooth-enabled blood pressure cuffs, pulse oximeters, and weight scales that sync to a monitoring platform meet this standard. Practices using patient-reported apps or manual logs are out of compliance and at audit risk.
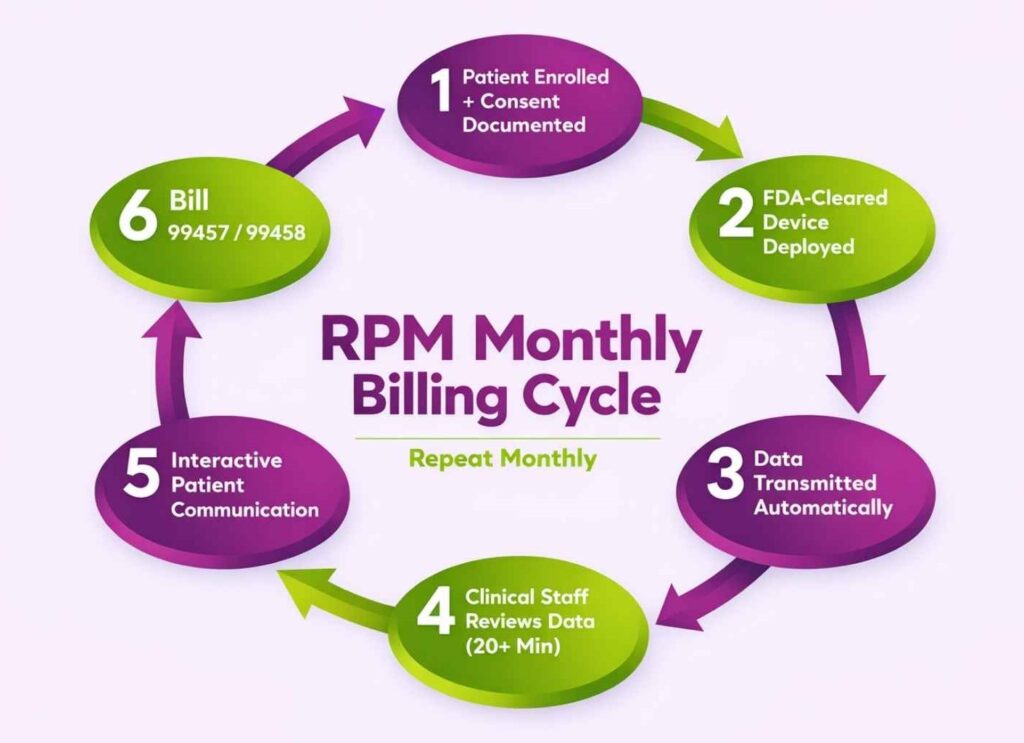
Billing the RPM Code Set (99453–99458)
RPM billing runs across four codes covering setup, device supply, and monthly management time: 99453, 99454, 99457, and 99458. The monthly management code (99457) requires at least 20 minutes of clinical staff time and at least one interactive communication with the patient during the billing period. Time must be documented and attributed to a specific staff member. Billing without meeting these thresholds is a compliance violation.
Chronic Care Management (CCM) Billing for Cardiac Conditions
CCM is one of the most underutilized revenue codes in cardiology. Patients with two or more chronic conditions expected to last at least 12 months, such as hypertension plus heart failure, for example, qualify. Requirements include a written care plan, patient consent, 24/7 access to care, and documented clinical staff time. CCM cannot be billed in the same month as certain other care management codes, so check for conflicts before submitting.
Combining RPM and CCM for Maximum Reimbursement
RPM and CCM can be billed in the same month for the same patient. They are not mutually exclusive. The hard rule is that time cannot be double-counted. Minutes logged toward RPM management cannot also be applied to CCM in the same period. Each code set requires a separate documented time. Build this into your care management team’s documentation protocol, and it becomes a reliable, scalable monthly revenue line.
Compliance and Regulatory Requirements in Cardiology Billing
Cardiology is one of the highest-scrutinized specialties in CMS audit programs. The procedure complexity, reimbursement rates, and volume of prior auth requirements make cardiac practices a consistent target. Understanding the regulatory framework isn’t optional. It’s what separates practices that survive audits from those that don’t.
HIPAA Compliance in Cardiology Billing Workflows
Cardiology billing workflows handle a high volume of sensitive data, diagnostic imaging reports, device implant records, cath lab findings, moving across EHRs, clearinghouses, billing platforms, and payer portals. Every touchpoint is a HIPAA exposure point.
Practically, this means ensuring your billing partner operates under a signed Business Associate Agreement (BAA), that PHI is encrypted in transit and at rest, and that access to patient billing data is role-restricted. When outsourcing cardiology billing, verify your vendor’s HIPAA compliance infrastructure before contracting, as a breach originating from a billing partner is still your liability.
Understanding LCDs, NCDs, and Medical Necessity
Most cardiology denials coded as “medical necessity” trace back to a Local Coverage Determination (LCD) or National Coverage Determination (NCD) that the claim didn’t satisfy. These are CMS-issued policy documents that define exactly when a procedure is covered. Which diagnoses qualify, what documentation is required, and what frequency limitations apply.
How to Read a Local Coverage Determination (LCD)
An LCD has three sections that matter for billing: Indications and Limitations of Coverage (what qualifies), Documentation Requirements (what must be in the chart), and Coding Guidelines (which CPT/ICD-10 combinations are accepted). Before billing a high-value cardiology procedure, cross-reference the applicable LCD to confirm the documented diagnosis maps to a covered indication. If it doesn’t, the denial is predictable and preventable.
Common Cardiology LCDs That Trigger Denials
- Echocardiography: LCD requires a specific covered indication; routine or screening echos without a qualifying diagnosis are routinely denied
- Nuclear stress testing: Strict medical necessity criteria; intermediate-to-high CAD risk must be documented
- Cardiac monitoring (Holter/event monitors): Frequency limits apply; repeat monitoring within the restriction window triggers automatic denial
- EP ablation: Failed antiarrhythmic therapy must be documented before ablation is considered covered by most payers
NCCI Edits and Procedure Bundling Rules
The National Correct Coding Initiative (NCCI) edits define which procedure code pairs cannot be billed together, either because one is bundled into the other or because they’re mutually exclusive. In cardiology, NCCI edits are a frequent source of unexpected denials, particularly in cath lab and EP billing.
For example, certain diagnostic angiography codes are bundled into interventional PCI codes when performed in the same session. Billing both without a valid modifier triggers an automatic edit. Your billing team should be running claims through an NCCI edit checker before submission, catching these pre-claim is far cheaper than working denials post-payment.
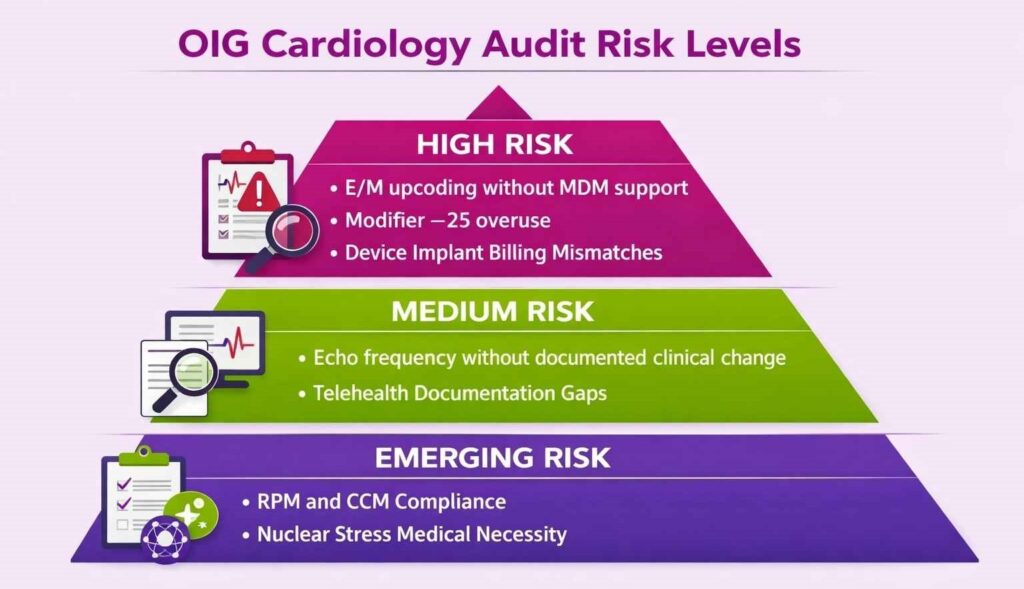
OIG Audit Risk in Cardiology: What Auditors Look For
The OIG’s Work Plan consistently flags cardiology as a high-risk specialty. Key audit targets include:
- E/M Upcoding: Particularly high-frequency 99215 billing without supporting MDM documentation
- Modifier –25 Overuse: Same-day E/M and procedure billing without clearly distinct documentation
- Echocardiography Frequency: Repeat studies within short intervals without documented clinical change
- Device Implant Billing: Mismatches between billed device codes and operative/device reports
- Telehealth and RPM Compliance: A growing audit focus as these codes scale in volume
The best defense is a documentation-first culture and periodic internal audits. If your denial rate is low but your documentation wouldn’t survive a retrospective audit, you have a compliance risk that hasn’t surfaced yet.
Keeping Up with the Annual CMS Final Rule
Every November, CMS releases the Physician Fee Schedule Final Rule, which updates RVUs, reimbursement rates, telehealth eligibility, and coding policies effective January 1. For cardiology, even small RVU adjustments on high-volume codes like echocardiography or cardiac cath can materially impact revenue.
Billing teams should review the Final Rule each year, focusing on cardiology-relevant changes, and update fee schedules, code crosswalks, and documentation templates accordingly. Practices that miss these updates typically catch up on them six months later through unexplained reimbursement drops.
Payer-Specific Billing Rules for Cardiology Practices
Cardiology billing doesn’t operate under one universal rulebook. Medicare, Medicaid, and commercial payers each apply different coverage policies, prior auth thresholds, and reimbursement structures. Billing teams that treat all payers the same will consistently run into avoidable denials.
Medicare Billing Rules for Cardiology
Medicare remains the dominant payer for most cardiology practices, given the age skew of cardiac patients. Coverage is governed by LCDs, NCDs, and the annual Physician Fee Schedule, all of which directly impact what gets paid and at what rate.
Medicare Advantage Plan Prior Auth Differences
This is where most practices get caught. Medicare Advantage (MA) plans follow their own prior auth rules, not traditional Medicare’s. A procedure that doesn’t require pre-auth under fee-for-service Medicare may require it under a patient’s MA plan. Nuclear stress tests, advanced imaging, and EP procedures are frequent examples. Always verify the patient’s specific MA plan requirements, not just their Medicare status.
Medicaid Reimbursement and State-Level Variations
Medicaid reimbursement for cardiology varies significantly by state, both in covered services and payment rates, which are typically well below Medicare. Some states require managed Medicaid plans, each with its own prior auth and billing rules layered on top of state policy. Before scheduling high-cost cardiac procedures for Medicaid patients, verify coverage and auth requirements at the plan level, not just the program level.
Commercial Payer Guidelines and Contracting
Commercial payers generally reimburse at higher rates than Medicare but apply stricter and more variable coverage policies. Each payer maintains its own clinical coverage policies for cardiology procedures. These are not always aligned with Medicare LCDs and can be more restrictive.
Why Commercial Payers Reimburse More And What That Means for Your Mix
Commercial rates for cardiology procedures can run 120% to 160% of Medicare for the same CPT code. This makes payer mix a meaningful revenue lever. Practices with a higher commercial patient share have materially better reimbursement per unit of work. Understanding your payer mix breakdown and its impact on net collections is essential context for any cardiology RCM strategy.
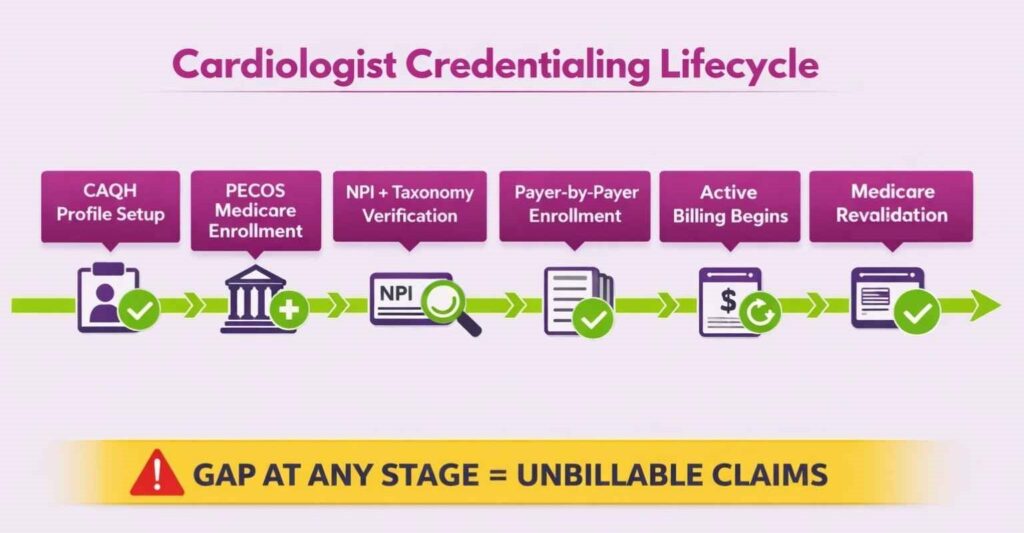
Credentialing and Provider Enrollment for Cardiologists
Credentialing is a prerequisite to billing. An unenrolled or lapsed provider means clean claims that still don’t pay. It’s one of the most operationally overlooked revenue risks in cardiology practices.
Why Credentialing Directly Affects Billing Revenue
Every cardiologist must be credentialed and enrolled with each payer before claims can be reimbursed under their NPI. If a provider sees patients while credentialing is pending, that revenue is either written off or requires retroactive billing, which most payers limit or deny outright.
For group practices, this compounds quickly. A new cardiologist who starts seeing patients before enrollment is complete can generate weeks of unbillable claims. The revenue loss isn’t always visible in real time, as it surfaces later as denials or zero-pay EOBs that are difficult to recover.
Common Credentialing Errors and How to Avoid Them
- Billing Under the Wrong NPI: Individual vs. group NPI mismatches are a common and easily avoidable denial trigger
- Outdated CAQH Profiles: Payers pull CAQH data during credentialing; expired licenses or missing documents stall the process
- Missing Taxonomy Codes: Cardiology has specific taxonomy codes that must match across the claim, enrollment record, and payer contract
- No Tracking System For Credentialing Timelines: Without proactive monitoring, expiration dates slip, and providers unknowingly fall out of network
Re-Credentialing, Revalidation, and In-Network Maintenance
Credentialing isn’t one-and-done. Most payers require re-credentialing every two to three years, and Medicare mandates revalidation on a rolling cycle. Letting either lapse results in the provider being dropped from the network mid-cycle, with claims denied retroactively to the lapse date in some cases.
Maintain a credentialing calendar with expiration dates for every provider across every payer. Treat re-credentialing deadlines the same way you treat prior auth deadlines. Missing them has a direct, quantifiable revenue impact.
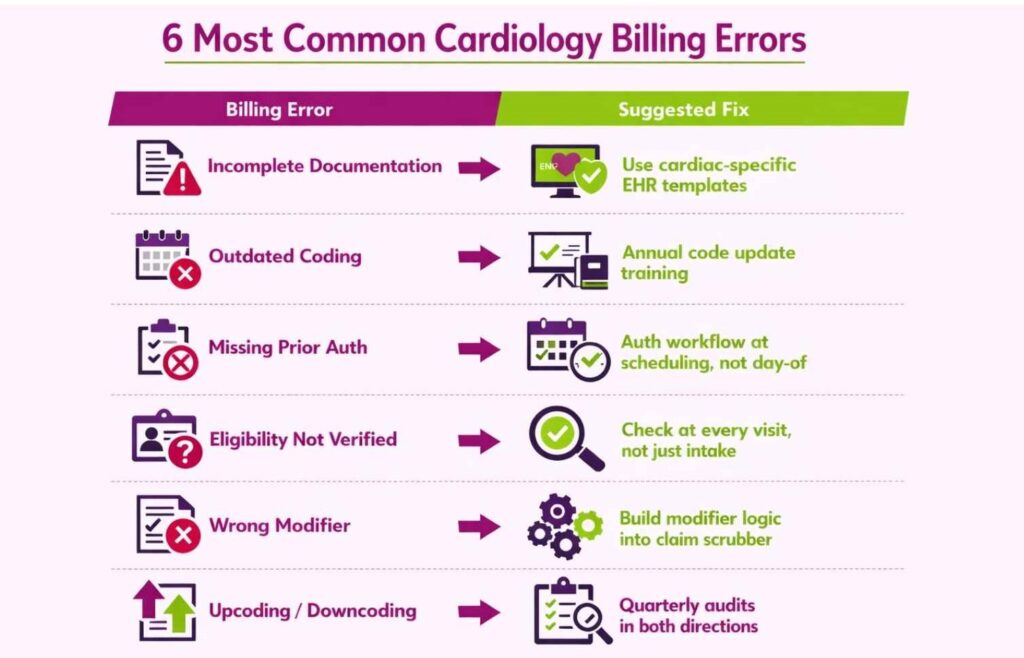
Common Cardiology Billing Errors and How to Avoid Them
Even small mistakes can cost big money in cardiology medical billing. Go through these common problems and their suggested fixes to get paid on time.
Incomplete or Inaccurate Documentation
Without detailed notes, procedures look medically unnecessary. Any insurer will reject your claim if you fail to satisfy the need for the medical procedure.
Solution: Train providers to document all findings and procedures thoroughly. Use EHR templates that prompt for cardiac-specific details, echo type, vessel numbers, device placement, and clinical indication.
Incorrect or Outdated Coding
Using wrong ICD-10 codes or outdated CPTs leads to incorrect payments or outright denials.
Solution: Stay current on annual code updates. Enroll billing staff in coding webinars and use updated code books. Partnering with a specialized cardiology billing company like Transcure ensures coders are trained specifically on cardiac code sets.
Missing Prior Authorization
Billing before securing insurer approval results in immediate claim denial, and retroactive auth is rarely granted.
Solution: Implement a strict pre-procedure authorization workflow. Every cardiac cath, advanced imaging study, and EP procedure should have a confirmed authorization on file before the appointment is scheduled.
Failure to Verify Patient Eligibility
Claiming a service that isn’t covered under the patient’s current plan means a write-off.
Solution: Verify insurance eligibility at every visit, not just at initial registration. Coverage changes, and a patient whose plan covered a procedure last quarter may not be covered today. If a service isn’t covered, inform the patient and collect upfront.
Incorrect Modifier Usage
Modifier errors are one of the most consistent and preventable denial triggers in cardiology. The specialty’s reliance on split-billing, same-day procedures, and bilateral services makes modifier accuracy non-negotiable.
Common modifier errors include applying –26 or –TC incorrectly when services aren’t actually split between facility and physician, using –59 as a default bundling override without clinical justification, and omitting –25 when billing an E/M with a same-day procedure or worse, applying it when the E/M isn’t distinctly documented.
Solution: Build modifier logic into your claim scrubbing workflow. Every modifier applied should map to a specific, documentable clinical reason. Blanket modifier application without documentation to back it up is a fast path to both denials and audits.
Upcoding and Downcoding Risks in Cardiology
Both directions carry risk. Upcoding, billing a higher-level code than documentation supports, is a compliance violation that triggers OIG scrutiny and potential repayment demands. Downcoding, billing conservatively below what’s documented, is a self-inflicted revenue loss that compounds across thousands of claims annually.
In cardiology, downcoding is more common than practitioners realize. Providers accustomed to mid-level E/M codes often undercode genuinely complex visits out of audit anxiety, leaving legitimate reimbursement uncaptured.
Solution: Periodic coding audits that flag both directions, not just upcoding. If your 99214/99215 utilization rate is significantly below specialty benchmarks, downcoding is likely. If it’s significantly above, the documentation better supports it.
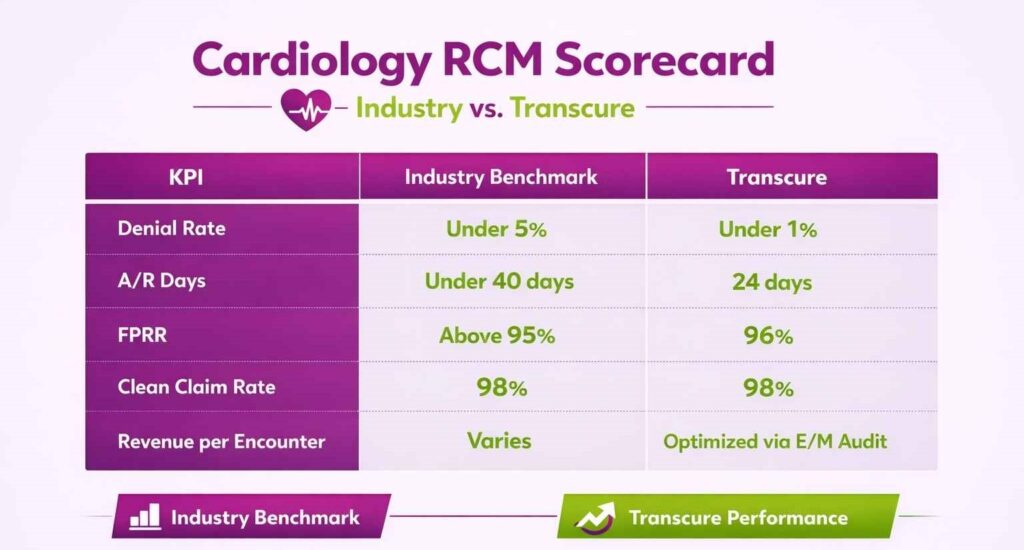
RCM Performance Metrics Every Cardiology Practice Should Track
You can’t improve what you don’t measure. These KPIs give cardiology practices a quantifiable read on billing performance, and a clear signal of where revenue is leaking.
Key KPIs for Cardiology Revenue Cycle Management
Benchmarks give you a baseline. But the gap between industry average and what a high-performing billing partner delivers is where the real revenue opportunity sits. Here’s what to track and what good looks like.
Denial Rate: Industry Benchmark and How to Improve It
Industry benchmark is under 5%. Cardiology practices frequently run higher due to prior auth gaps and coding complexity. Track denial rate by payer and by denial reason. Patterns at that level tell you exactly where the process is breaking down. Transcure’s cardiology billing operations run at a denial rate below 1%, achieved through pre-claim scrubbing, authorization tracking, and specialty-trained coders.
Days in Accounts Receivable (A/R)
Measures how long it takes to collect payment after a claim is submitted. Target is under 40 days for cardiology. High A/R days typically signal slow follow-up on outstanding claims or excessive denials requiring rework. Transcure averages 24 A/R days across cardiology clients, nearly half the specialty benchmark.
First-Pass Resolution Rate (FPRR)
The percentage of claims paid on the first submission without rejection or denial. Target is above 95%. Low FPRR points to upstream problems, eligibility verification, coding accuracy, or authorization gaps. Transcure maintains a 96% FPRR across cardiology billing operations.
Clean Claim Rate
Similar to FPRR but measured at submission, before payer adjudication. A clean claim rate below 98% means your billing team is submitting claims with known errors. Transcure’s clean claim rate holds at 98%, a direct result of automated scrubbing and pre-submission QA checks.
Revenue per Encounter
Tracks the average reimbursement per patient visit across the practice. Useful for identifying payer mix impact, E/M coding patterns, and procedure capture gaps. A declining revenue per encounter with stable volume usually means downcoding or payer reimbursement erosion.
How to Use KPI Data to Improve Billing Performance
KPIs are only useful if they drive action. Review these metrics monthly, not quarterly, and segment by provider, payer, and procedure type. A high denial rate from one payer on one procedure code is an actionable finding. An aggregate denial rate number is not.
Build a simple dashboard, assign ownership, and set improvement targets by quarter. Practices that review KPIs in isolation without connecting them to workflow changes see no improvement. Those who use them to identify the specific breakdown point and fix it there see measurable collection gains within 60 to 90 days.
Accounts Receivable and Patient Collections in Cardiology
Revenue doesn’t materialize at claim submission. It materializes in collections. A/R management and patient billing are where a lot of cardiology practices quietly lose money they technically earned.
Managing the A/R Follow-Up Workflow
A/R follow-up needs a structured, time-bound workflow, not a queue that gets worked when time allows. Assign ownership by payer or account age, set follow-up intervals, and escalate systematically.
Using Aging Reports to Prioritize Unpaid Cardiology Claims
The aging reports segment outstanding claims by how long they’ve been unpaid, typically 0–30, 31–60, 61–90, and 90+ day buckets. In cardiology, prioritize the 61 to 90-day bucket aggressively, as most payers have timely filing limits between 90 and 180 days. High-value cardiac procedure claims in that window represent real write-off risk if not worked on immediately. Claims beyond 90 days without action are often unrecoverable.
When to Appeal a Denied Claim vs. When to Write It Off
Not every denial is worth appealing, but most are. A general rule: if the denial is clinical or technical and the documentation supports the service, appeal. If the service was genuinely not covered, not authorized, or outside timely filing limits, write it off and fix the upstream process that caused it.
For high-value cardiology claims, cath lab, device implants, and EP procedures, appeal as a default regardless of the denial reason. The reimbursement justifies the effort. Build appeal templates by denial type so the process is fast and repeatable, not custom-built each time.
Patient Billing, Good Faith Estimates (GFE), and Payment Plans
Patient responsibility is an increasingly significant portion of cardiology revenue, given high-deductible plan prevalence. Collecting it requires the same workflow discipline as payer collections.
Under the No Surprises Act, cardiology practices must provide a Good Faith Estimate to uninsured or self-pay patients before scheduled services, itemizing expected charges. For insured patients with predictable out-of-pocket exposure (pre-auth approved, benefits verified), proactively communicating cost estimates and collecting patient responsibility before service dramatically improves collection rates.
Value-Based Care and Its Impact on Cardiology Billing
Reimbursement in cardiology isn’t purely transactional anymore. How your practice performs on quality metrics directly affects what Medicare pays you per claim.
Under MIPS (Merit-based Incentive Payment System), cardiology practices receive positive or negative Medicare payment adjustments. These are based on performance across quality, cost, improvement activities, and interoperability. A low MIPS score not only reflects poorly but also directly reduces reimbursement on every Medicare claim in the adjustment year.
Billing teams need to track MIPS reporting deadlines and ensure quality measure data is being captured and submitted accurately. Missing a reporting period or submitting incomplete data results in a negative payment adjustment, a preventable revenue hit.
Best Practices for Cardiology Billing and Revenue Cycle Management
Getting cardiology billing right isn’t a one-time fix. It’s a set of operational disciplines applied consistently across the revenue cycle. These practices separate high-performing cardiac practices from those constantly chasing denials and underpayments.
Obtain Prior Authorizations Early
Build a front-end workflow to request and track authorizations at the time of scheduling, not the day of service. Many cardiac procedures have 7 to 14-day approval windows, and last-minute auth requests are the leading cause of avoidable denials. Lock in authorizations early and maintain a tracking system so nothing slips through.
Maintain Certified and Trained Billing Staff
Cardiology coding changes annually, including new CPT codes, updated NCCI edits, and revised LCD criteria. Staff who aren’t actively keeping up are coding against outdated rules. Many practices subscribe to coding update services or partner with specialized billing companies to stay current. Transcure brings a trained team of over 1,100 billers and coders with cardiology-specific expertise.
Use Technology and AI Automation in Cardiology Billing
Utilizing the top cardiology EMR systems with built-in code scrubbers and AI-powered denial prediction is no longer optional for competitive practices.. Automated pre-submission scrubbing catches modifier errors, bundling conflicts, and missing auth flags before claims leave the office. Transcure deploys AI-powered billing workflows and real-time KPI dashboards to keep cardiology RCM performance measurable and actionable.
Conduct Regular Audits and Feedback Loops
Periodic audits of randomly selected charts and claims are the earliest warning system for billing problems. Check whether ICD-10 codes match physician notes, modifiers were applied correctly, and all rendered services were captured. Audit findings should feed directly back to providers and coders. A closed feedback loop is what prevents the same errors from repeating quarter after quarter.
In-House vs. Outsourced Cardiology Billing: How to Decide
The right choice between in-house and outsourced options depends on your practice’s size, volume, and internal capacity. In-house billing gives you direct control but requires sustained investment in staff training, technology, and compliance infrastructure. Outsourcing to a cardiology billing firm like Transcure transfers that operational burden to a specialized team, typically at a lower total cost with better performance metrics.
Signs Your Practice Should Consider Outsourcing
- Denial rate consistently above 5% with no clear improvement trend
- A/R days exceeding 45 and aging reports showing a growing 90+ day bucket
- Staff turnover disrupting billing continuity
- No internal capacity to keep up with annual coding updates or payer policy changes
- Physician time is being consumed by billing escalations instead of patient care
- Revenue declining despite stable or growing patient volume
What to Look for in a Cardiology Billing Partner
Specialty experience is non-negotiable. A general medical billing company without cardiology-specific expertise will cost you more in denials than you save in fees. Beyond that, evaluate transparency (real-time reporting and KPI access), technology infrastructure, and whether they operate under a signed BAA for HIPAA compliance. Ask for cardiology-specific performance benchmarks, denial rate, clean claim rate, A/R days, before committing.
Questions to Ask Before Signing a Billing Contract
- What is your current denial rate and clean claim rate for cardiology clients specifically?
- How do you handle prior authorization tracking and follow-up?
- What is your average A/R days across cardiology accounts?
- How are coding updates implemented, and how quickly after CMS releases them?
- What does your escalation process look like for high-value denied claims?
- Is there a performance guarantee or SLA tied to collection metrics?
Conclusion
Cardiology medical billing is one of the most operationally demanding specialties in healthcare RCM, with complex prior auth requirements, strict documentation standards, aggressive payer audits, and a constantly evolving regulatory landscape. Throughout this guide, we’ve covered the end-to-end billing workflow, E/M coding, procedure-specific guidelines, compliance requirements, payer rules, credentialing, and the KPIs that tell you how well your revenue cycle is actually performing.
Accuracy and process discipline at every stage are what maximize revenue for cardiac practices. Many successful cardiology groups partner with top cardiology billing companies like Transcure to implement these standards at scale.. Transcure’s cardiology RCM specialists deliver clean claims, precise coding, and systematic denial follow-up, translating directly into improved cash flow and physicians freed to focus on patients.
Frequently Asked Questions
How Can a Cardiology Practice Bill an EKG with an Office Visit?
An EKG (93000 or 93010) can be billed on the same day as an office E/M if it was a separate, medically necessary service. Use modifier –25 on the office visit code to indicate it was a distinct service. Documentation must independently support both the visit and the EKG.
How Much Does it Cost to Outsource Cardiology Medical Billing Services?
Outsourcing fees vary by pricing model. Most cardiology practices pay around 5 to 9% of collections to a full-service billing company. Because cardiology is complex, including imaging, caths, and devices, it often falls in the higher range of outsourcing rates. Transcure’s cardiology billing services charge around 5%, below the industry average, without compromising on specialty-specific expertise or performance metrics.
What is the Difference between MDM-based and Time-based E/M Coding for Cardiology Visits?
Both are valid methods for selecting an E/M code level under current AMA guidelines. MDM-based coding uses the complexity of the clinical decision-making to determine the level. Time-based coding uses total provider time spent on the encounter date, including non-face-to-face work like reviewing results and coordinating care. For most cardiology visits, MDM is the more defensible basis given the clinical complexity involved.
What Should a Cardiology Practice do When a High-value Claim is Denied?
First, identify the denial reason, clinical, technical, or administrative, before deciding how to respond. For high-value procedures like cardiac cath, device implants, or EP ablations, appeal as a default unless the service was genuinely outside coverage or past timely filing limits. Build appeal templates by denial type so the process is repeatable. If a specific denial reason is recurring across multiple claims, that’s a signal to fix the upstream process, not just appeal case by case.






