In the entire revenue cycle, the Oncology medical billing is one of the most complex areas. The billing teams find it extremely tough to get every code right that comes with high-cost cancer care. This can include rapidly evolving treatment protocols, the high volume of services delivered per patient visit, and the strict payer scrutiny that comes with high-cost cancer care.
According to the American Cancer Society, an estimated 2 million new cancer cases are diagnosed in the United States each year, driving enormous demand for oncology billing services and, consequently, for accurate oncology medical billing.
A single miscoded claim in an oncology practice can mean thousands of dollars in lost revenue or a compliance audit that disrupts the entire practice.
This guide is designed for billing professionals, practice managers, oncology coders, and revenue cycle teams who want a thorough and practical resource on CPT oncology codes. From evaluation and management visits to chemotherapy administration, radiation therapy, CAR T-cell therapy, and laboratory services, this post covers everything you need to know to code correctly, bill confidently, and protect your revenue.
What are Oncology CPT Codes?
CPT stands for Current Procedural Terminology. These are standardized numeric codes developed and maintained by the American Medical Association that describe medical, surgical, and diagnostic services. Every procedure or service performed in a clinical setting is assigned a CPT code, which is then submitted on a claim to insurance payers for reimbursement.
In the context of cancer care, CPT codes in oncology medical billing cover an extraordinarily wide range of services. A patient with breast cancer, for example, might require an evaluation and management visit, laboratory testing, imaging, surgical biopsy, chemotherapy infusion, supportive therapy for nausea, and follow-up radiation treatment. All of which require distinct CPT codes billed across multiple specialties and settings.
Note: CPT codes are updated annually by the American Medical Association (AMA). Always verify codes against the current year’s CPT codebook and your specific payer guidelines before submitting claims.
Oncology CPT codes are organized across several major categories:
| Category | Description |
|---|---|
| Evaluation and Management (E/M) | Office visits, hospital care, consultations |
| Chemotherapy Administration | IV push, infusion, injection codes |
| Radiation Oncology | Treatment planning, delivery, and management |
| Infusion and Supportive Therapy | Hydration, antiemetics, supportive drugs |
| Pathology and Laboratory | Diagnostic testing, molecular pathology |
| Immunotherapy and Emerging Therapies | CAR T-cell therapy, immunotherapy administration |
Understanding which codes apply to which services and how to sequence them correctly is the foundation of compliant oncology revenue cycle management.
Importance of CPT Codes in Oncology Medical Billing
Since it is quite complex, understanding what oncology billing is and the codes it involves is highly important. Cancer treatment is expensive, treatments are long-term, and payer scrutiny is intense. Here is why accuracy in CPT codes in oncology medical billing matters so profoundly.
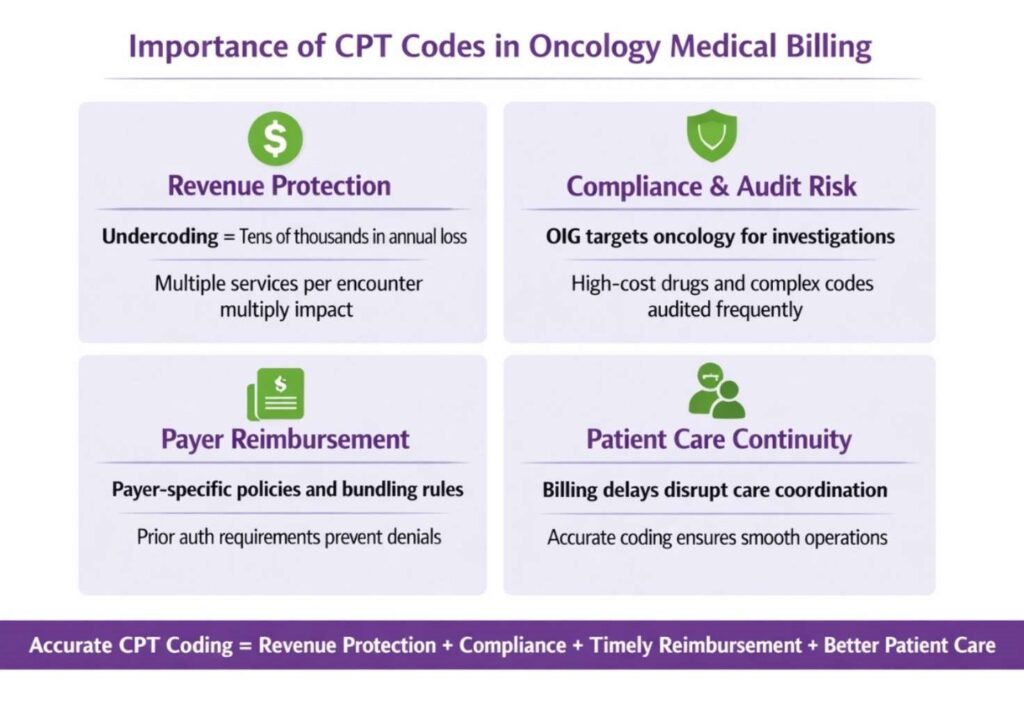
- Revenue Protection: Oncology practices typically bill for multiple services per encounter. A missed code or an undercoded service does not just cost you one claim. It multiplies across hundreds or thousands of visits per year. For a practice administering chemotherapy daily, undercoding infusion time by even one unit level can represent tens of thousands of dollars in annual revenue loss.
- Compliance and Audit Risk: The Office of Inspector General (OIG) consistently targets oncology for fraud and abuse investigations. High-cost drugs, complex infusion hierarchies, and radiation planning codes are frequent targets of Medicare audits. Accurate coding with proper documentation is your primary defense.
- Payer Reimbursement: Insurance payers, including Medicare, Medicaid, and commercial plans, have specific policies for oncology services. Some require prior authorization; others have bundling rules that restrict which codes can be billed together. Knowing these rules prevents claim denials and payment delays.
- Patient Care Continuity: When billing is delayed due to denials or coding errors, it can create administrative disruption that ultimately affects the patient experience and care coordination.
Most Important Oncology CPT Codes
Before breaking down each category, here is a high-level reference table of the most commonly used oncology codes across all service types.
| CPT Code | Description | Category | When It’s Used |
|---|---|---|---|
| 96413 | Chemotherapy administration, IV infusion (initial, up to 1 hour) | Chemotherapy Admin | First hour of chemo infusion |
| 96415 | Chemotherapy administration, each additional hour | Chemotherapy Admin | Add-on for extended infusions |
| 96416 | Chemotherapy infusion, prolonged (via pump) | Chemotherapy Admin | Continuous infusion (e.g., ambulatory pump) |
| 96411 | Chemotherapy administration, IV push | Chemotherapy Admin | Quick injection instead of infusion |
| 96365 | IV infusion for non-chemo drugs (initial) | Therapeutic Infusion | Supportive drugs like hydration, antibiotics |
| 96366 | Each additional hour (non-chemo infusion) | Therapeutic Infusion | Add-on for longer infusions |
| 96375 | IV push, additional new drug | Injection | Secondary medication push |
| 96401 | Chemo administration, subcutaneous or IM | Chemotherapy Admin | Hormonal or certain chemo injections |
| 96402 | Hormone therapy administration | Hormonal Therapy | Drugs like Lupron, Eligard |
| 96521 | Refill & maintenance of portable pump | Pump Management | Continuous infusion device refill |
| 96523 | Irrigation of the implanted venous access device | Vascular Access | Port flush/maintenance |
| 36591 | Collection of blood via a venous access device | Lab/Access | Blood draw from the port |
| 36592 | Collection of blood via central/peripheral line | Lab/Access | Blood draw from a catheter |
| 77261–77263 | Radiation therapy planning | Radiation Oncology | Treatment planning complexity levels |
| 77385–77386 | IMRT treatment delivery | Radiation Oncology | Intensity-modulated radiation therapy |
| 77427 | Radiation treatment management (weekly) | Radiation Oncology | Ongoing treatment supervision |
| 78815 | PET scan (tumor imaging, skull base to mid-thigh) | Diagnostic Imaging | Cancer staging and monitoring |
| 77014 | CT guidance for radiation therapy | Imaging Guidance | Tumor localization during treatment |
Evaluation and Management (E/M) Codes in Oncology
E/M codes are the backbone of any outpatient oncology practice. These codes cover physician visits, whether the patient is presenting for a new cancer diagnosis, an ongoing chemotherapy consultation, or a survivorship follow-up.
Since the 2021 AMA revisions, E/M code selection is now based on medical decision making (MDM) or total time, rather than the previous history-physical examination-MDM system. This change significantly affects oncology, where patient complexity is almost always high.
Key E/M Codes for Oncology
| CPT Code | Description | Visit Type | When It’s Used |
|---|---|---|---|
| 99202 | New patient visit (straightforward MDM, 15–29 min) | Office Visit | Initial consult with minimal complexity |
| 99203 | New patient visit (low MDM, 30–44 min) | Office Visit | Early cancer evaluation, low complexity |
| 99204 | New patient visit (moderate MDM, 45–59 min) | Office Visit | Most common for oncology consults |
| 99205 | New patient visit (high MDM, 60–74 min) | Office Visit | Complex cases (advanced cancer, multiple issues) |
| 99211 | Established patient (minimal) | Office Visit | Quick follow-up, nurse visit |
| 99212 | Established patient (straightforward MDM, 10–19 min) | Office Visit | Stable patients, routine check-ins |
| 99213 | Established patient (low MDM, 20–29 min) | Office Visit | Ongoing treatment follow-ups |
| 99214 | Established patient (moderate MDM, 30–39 min) | Office Visit | Most commonly used in oncology |
| 99215 | Established patient (high MDM, 40–54 min) | Office Visit | Complex follow-ups, treatment changes |
| 99221–99223 | Initial hospital care | Inpatient | First hospital admission evaluation |
| 99231–99233 | Subsequent hospital care | Inpatient | Daily hospital rounds |
| 99238–99239 | Hospital discharge | Inpatient | Patient discharge management |
| 99242–99245 | Outpatient consultation* | Consultation | Specialist consults (*payer-dependent) |
| 99417 | Prolonged office visit time | Add-on | When time exceeds 99205 or 99215 |
| 99354–99357 | Prolonged services (non-face-to-face) | Add-on | Extended care coordination/documentation |
Important Note on MDM in Oncology
Cancer patients routinely present with multiple problems, multiple medications, and a significant risk of complications. Most oncology encounters appropriately qualify for 99214 or 99215 under the MDM framework, provided the documentation supports it. Physicians must clearly document the number and complexity of problems addressed, the amount and complexity of data reviewed, and the risk of complications or morbidity.
Pro Tip: When a physician reviews outside pathology reports, imaging studies from another facility, or laboratory results from a referring provider, this data review contributes to the MDM level. Make sure documentation captures this explicitly.
Chemotherapy Administration Codes
Chemotherapy administration codes are among the most scrutinized and most consequential codes in oncology billing. Understanding the hierarchy is essential.
The Infusion Hierarchy Rule:
Medicare and most commercial payers require that infusions be reported using a hierarchy where the most complex service is billed as the primary code and subsequent services are billed as add-on codes.
The hierarchy from highest to lowest is:
- Chemotherapy infusion (96413 and related codes)
- Therapeutic, prophylactic, and diagnostic injections or infusions
- Hydration (reported only if it is a separate and distinct service)
Core Chemotherapy Administration CPT Codes:
| CPT Code | Description | Notes |
|---|---|---|
| 96413 | Chemo infusion, initial, up to 1 hour | Primary code |
| 96415 | Chemo infusion, each additional hour | Add-on: bill per hour |
| 96416 | Chemo infusion, initiation of prolonged service | Used when concurrent infusions run |
| 96417 | Chemo infusion, each additional sequential infusion | Different drug, new IV line setup required |
| 96401 | Non-hormonal antineoplastic injection | Subcutaneous or IM |
| 96402 | Hormonal antineoplastic injection | Subcutaneous or IM |
| 96405 | Chemotherapy injection, intralesional, up to 7 lesions | |
| 96406 | Chemotherapy injection, intralesional, over 7 lesions | |
| 96409 | IV push chemo, first substance | |
| 96411 | IV push chemo, each additional substance | Add-on |
Critical Distinction: An IV push is defined as an infusion of 15 minutes or less. Anything beyond 15 minutes qualifies as an infusion and should be coded accordingly. This distinction is frequently audited.
Note: Physician supervision requirements for chemotherapy infusion vary by payer. Medicare requires that a physician be immediately available (not necessarily present in the room) during chemotherapy administration in the office setting. Document supervision appropriately to protect your claims.
Radiation Oncology Codes
CPT codes for radiation oncology span a broad range of services, from initial consultation and simulation to daily treatment delivery and ongoing management. Radiation oncology billing involves multiple providers (radiation oncologist, medical physicist, dosimetrist, radiation therapist) and multiple phases of care, each with distinct coding rules. Below are the common Phases of Radiation Oncology and associated codes.
1. Consultation and Initial Management
Radiation oncologists typically bill E/M codes for initial and follow-up visits in the same way as medical oncologists. However, during a course of radiation treatment, weekly treatment management codes are billed instead of routine office visit codes.
2. Treatment Planning Codes
| CPT Code | Description | Complexity Level | Clinical Use |
|---|---|---|---|
| 77261 | Therapeutic radiology treatment planning: simple | Simple | Low-complexity cases with minimal structures and basic dose planning |
| 77262 | Treatment planning; intermediate | Intermediate | Moderate complexity with multiple treatment areas or organs at risk |
| 77263 | Treatment planning: complex | Complex | High-complexity planning involving multiple beams, critical structures, or advanced techniques |
| 77295 | 3D radiotherapy treatment planning | Advanced | CT-based 3D conformal planning for precise tumor targeting |
| 77300 | Basic radiation dosimetry calculation | Support code | Dose calculations for treatment delivery verification |
| 77301 | Intensity-Modulated Radiation Therapy (IMRT) planning | Highly advanced | Computerized inverse planning for IMRT delivery |
3. Radiation Treatment Delivery Codes
| CPT Code | Description | Complexity Level | Clinical Use |
|---|---|---|---|
| 77401 | Radiation treatment delivery, superficial and/or orthovoltage | Simple | Low-energy treatments for superficial lesions (e.g., skin conditions) |
| 77402 | Radiation treatment delivery is simple | Simple | Single treatment area, basic delivery techniques |
| 77407 | Radiation treatment delivery, intermediate | Intermediate | Multiple treatment areas or a more complex setup |
| 77412 | Radiation treatment delivery, complex | Complex | Multiple beams, blocking, or complex dose distribution |
| 77385 | IMRT treatment delivery: simple | IMRT | Basic intensity-modulated radiation therapy delivery |
| 77386 | IMRT treatment delivery: complex | IMRT | Advanced IMRT with higher modulation complexity |
| 77373 | Stereotactic body radiation therapy (SBRT) delivery | High precision | High-dose, image-guided delivery in a few fractions |
| 77371 | Stereotactic radiosurgery (SRS) delivery, single session | SRS | Single-fraction brain or spinal radiosurgery |
| 77372 | SRS delivery, multi-session (fractionated) | SRS | Fractionated stereotactic radiosurgery treatments |
| 77417 | Port film/imaging verification during treatment | Support | Treatment verification imaging (often IGRT-related workflows) |
| 77520–77525 | Proton beam radiation treatment delivery | Advanced | Proton therapy for highly targeted tumor treatment |
4. Weekly Treatment Management
| CPT Code | Description | Type | Clinical Use |
|---|---|---|---|
| 77427 | Radiation treatment management, 5 treatments | Weekly Management | Standard weekly management for external beam radiation therapy (EBRT); typically billed once per 5 fractions |
| 77431 | Radiation treatment management, stereotactic radiosurgery (single fraction) | SRS Management | Management for single-session stereotactic radiosurgery cases |
| 77432 | Radiation treatment management, SRS (multi-session) | SRS Management | Management of fractionated stereotactic radiosurgery (multiple sessions) |
| 77435 | Radiation treatment management, stereotactic body radiation therapy (SBRT) | SBRT Management | Management of SBRT courses (typically up to 5 fractions), including treatment review and coordination |
Important Note: Code 77427 is billed per five fractions of treatment, not per week. If a patient receives only three fractions in a calendar week, the code is not reported until the fifth fraction is completed. This is a common coding error that leads to overbilling or underbilling.
5. Brachytherapy Codes
Brachytherapy (internal radiation) has its own coding family covering source preparation, application, and management:
| CPT Code | Description | Technique | Complexity | Clinical Use |
|---|---|---|---|---|
| 77761 | Interstitial radiation source application | Permanent implant | Simple | Low-complexity seed implantation (e.g., prostate seeds) |
| 77762 | Interstitial radiation source application | Permanent implant | Intermediate | Moderate complexity implant with multiple sites or planning steps |
| 77763 | Interstitial radiation source application | Permanent implant | Complex | Complex implant involving multiple catheters, sites, or planning intensity |
| 77767 | Remote afterloading high dose rate (HDR) brachytherapy | HDR | Simple | Basic intracavitary or interstitial HDR treatment |
| 77768 | HDR brachytherapy, intermediate | HDR | Intermediate | Moderate complexity HDR planning and delivery |
| 77769 | HDR brachytherapy, complex | HDR | Complex | Advanced HDR cases with multiple channels, dwell positions, or sites |
Key Billing Notes
- 77761–77763 = Permanent interstitial implants (low-dose-rate / seed implants like prostate brachytherapy)
- 77767–77769 = HDR (High-Dose-Rate) brachytherapy using remote afterloading systems
- Complexity levels depend on:
- Number of catheters or sources
- Treatment sites
- Planning intensity and imaging guidance
Infusion and Supportive Therapy Codes
Cancer treatment generates an enormous volume of supportive care services. Antiemetics to prevent nausea, hydration to protect kidneys during nephrotoxic chemotherapy, growth factors to manage neutropenia, and bisphosphonates for bone metastases are all administered regularly in oncology infusion centers.
Core Supportive Therapy Codes
| CPT Code | Description | Type | Clinical Use |
|---|---|---|---|
| 96360 | Hydration infusion (initial 31 min–1 hour) | Hydration | IV fluids for dehydration or supportive care |
| 96361 | Hydration infusion each additional hour | Hydration | Continued IV hydration beyond the initial hour |
| 96365 | Therapeutic/diagnostic IV infusion (initial up to 1 hour) | Therapeutic infusion | Antibiotics, chemo-related supportive drugs, biologics |
| 96366 | Each additional hour of therapeutic infusion | Therapeutic infusion | Extended infusion time |
| 96367 | IV infusion, sequential (additional drug) | Sequential infusion | Secondary medication given after primary infusion |
| 96368 | IV infusion, concurrent | Concurrent infusion | Multiple drugs are infused at the same time via separate lines |
| 96369 | Subcutaneous infusion (initial) | Subcutaneous infusion | SC therapy (e.g., immunoglobulins) |
| 96370 | SC infusion each additional hour | Subcutaneous infusion | Extended SC infusion time |
| 96372 | Therapeutic/diagnostic injection (IM/SubQ) | Injection | Vaccines, antiemetics, steroids |
| 96373 | Injection (intra-arterial) | Injection | Specialized vascular administration |
| 96374 | IV push, single or initial substance | IV push | Rapid administration (chemo supportive meds, antiemetics) |
| 96375 | IV push each additional drug | IV push | Additional medications via IV push |
| 96376 | Repeat IV push the same drug | IV push | Repeat dosing of the same medication |
Key Billing Notes
- 96365 is the most common initial infusion code
- Always differentiate:
- Infusion (time-based)
- IV push (rapid bolus)
- Injection (single administration)
- “Initial” service is billed only once per encounter per vascular access site.
Hydration Billing Rules:
Hydration may not be billed when it is incidental to another infusion service. For example, if saline is used to keep a line open between chemotherapy drugs, it is considered incidental and is not separately billable. Hydration is separately reportable only when it is clinically distinct, ordered for a specific therapeutic purpose, and documented as such.
Common Mistake: Many oncology practices incorrectly bill 96360 every time saline is administered alongside chemotherapy. This is a compliance risk. The documentation must establish medical necessity for standalone hydration.
Pathology and Laboratory Codes in Oncology
Accurate diagnosis and treatment monitoring in oncology depend heavily on laboratory and pathology services. The pathology or laboratory department typically bills these codes, but oncology billing teams need to understand them for coordination of care and to avoid unbundling.
Hematology & General Lab Testing
| CPT Code | Description | Type | Clinical Use |
|---|---|---|---|
| 85025 | Complete blood count (CBC) with automated differential | Hematology | Routine cancer monitoring, infection, and anemia |
| 85027 | CBC without differential | Hematology | Basic blood count tracking |
| 85007 | Blood smear, manual differential | Hematology | Abnormal CBC follow-up |
| 80053 | Comprehensive metabolic panel (CMP) | Chemistry | Liver/kidney function monitoring during chemo |
| 80048 | Basic metabolic panel (BMP) | Chemistry | Electrolyte and kidney function check |
| 83615 | Lactate dehydrogenase (LDH) | Tumor marker support | Cancer progression/response monitoring |
| 84100 | Phosphorus level | Chemistry | Bone and metabolic assessment |
Tumor Markers
| CPT Code | Description | Type | Clinical Use |
|---|---|---|---|
| 86301 | CA 19-9 | Tumor marker | Pancreatic and GI cancers |
| 86300 | CA 15-3 | Tumor marker | Breast cancer monitoring |
| 86304 | CA 125 | Tumor marker | Ovarian cancer monitoring |
| 82378 | CEA (Carcinoembryonic antigen) | Tumor marker | Colon, lung, and GI cancers |
| 82105 | AFP (Alpha-fetoprotein) | Tumor marker | Liver and testicular cancers |
| 84153 | PSA (Prostate-specific antigen), total | Tumor marker | Prostate cancer screening/monitoring |
Molecular & Genetic Testing
| CPT Code | Description | Type | Clinical Use |
|---|---|---|---|
| 81210 | BRAF gene analysis | Molecular | Melanoma, colorectal cancer |
| 81235 | EGFR mutation analysis | Molecular | Lung cancer targeted therapy |
| 81275 | KRAS gene analysis | Molecular | Colorectal and lung cancer |
| 81445 | Targeted genomic sequence analysis (5–50 genes) | NGS panel | Precision oncology profiling |
| 81455 | Comprehensive genomic panel (51+ genes) | NGS panel | Broad cancer mutation profiling |
Pathology & Histology
| CPT Code | Description | Type | Clinical Use |
|---|---|---|---|
| 88305 | Surgical pathology, gross & microscopic examination | Histopathology | Routine biopsy analysis |
| 88307 | Surgical pathology, complex specimen | Histopathology | Organ or complex tumor evaluation |
| 88309 | Surgical pathology, highly complex specimen | Histopathology | Cancer resections, major tumor specimens |
| 88342 | Immunohistochemistry (single antibody stain) | IHC | Cancer subtype identification |
| 88341 | Additionally, IHC stain | IHC | Multiple marker testing |
| 88360 | Quantitative IHC (e.g., HER2, Ki-67) | IHC | Breast and other cancer biomarker scoring |
Key Billing Notes
- CBC + CMP are the most frequently repeated labs during chemotherapy cycles
- Tumor markers are used for:
- Monitoring response
- Detecting recurrence
- Molecular testing (NGS) is critical for:
- Targeted therapy selection
- Precision oncology treatment plans
- 88342 + 88360 are essential for biomarker-driven cancer therapy decisions
Note: Genomic sequencing panels (81445, 81455) are subject to specific LCD (Local Coverage Determination) policies by Medicare Administrative Contractors. Coverage varies by cancer type and clinical indication. Always verify coverage before ordering and document the clinical necessity thoroughly.
New and Emerging Codes: CAR T-Cell Therapy
CAR T-cell therapy represents one of the most significant advances in oncology in recent history and also one of the most challenging billing situations. These are genetically engineered immune cell therapies that can cost upward of $400,000 per patient, and their administration requires specialized inpatient or outpatient infrastructure.
Key CAR T-Cell Therapy CPT Codes
| CPT Code | Description | Phase of Therapy | Clinical Use |
|---|---|---|---|
| 0537T | Collection of T cells for genetically modified autologous cellular immunotherapy (e.g., CAR T-cell therapy); leukapheresis | Collection | Patient’s T-cells are collected via leukapheresis for CAR T manufacturing |
| 0538T | Preparation of collected T cells, including genetic modification | Manufacturing / Processing | T-cells are engineered in a lab to express chimeric antigen receptors (CAR) |
| 0539T | Administration of autologous CAR T-cell therapy | Infusion | Infusion of engineered CAR T-cells back into the patient |
| 0540T | Monitoring and management during CAR T-cell therapy | Post-infusion care | Intensive monitoring for cytokine release syndrome (CRS) and neurotoxicity |
Key Billing Notes
- These are Category III CPT codes (emerging technology tracking codes).
- CAR T therapy billing is typically split into 3 major phases:
- Collection (0537T)
- Cell engineering (0538T)
- Reinfusion (0539T)
- Post-infusion monitoring (0540T) is critical due to high-risk complications like:
- Cytokine Release Syndrome (CRS)
- Immune effector cell-associated neurotoxicity syndrome (ICANS)
Billing Considerations for CAR T
CAR T-cell therapy billing involves multiple components. The cost of the cellular product itself is typically billed separately from the administration. Preconditioning chemotherapy (lymphodepletion) is billed using standard chemotherapy administration codes. Inpatient stays for cytokine release syndrome management are billed under DRG codes for the facility.
Commercial payers have varied and rapidly evolving policies on CAR T coverage. Some require case-by-case prior authorization and outcomes reporting. Medicare has issued specific guidance through the National Coverage Determination (NCD) process.
Important Aspect: CAR T-cell therapy claims should be prepared with extensive supporting documentation, including the patient’s diagnosis, prior treatment history, genetic testing results confirming eligibility, and the ordering physician’s treatment rationale. Submitting this upfront can prevent pre-payment review delays.
Common Oncology Coding Challenges
Even experienced billing teams encounter recurring pitfalls in oncology coding. Being aware of these issues is the first step toward preventing them.
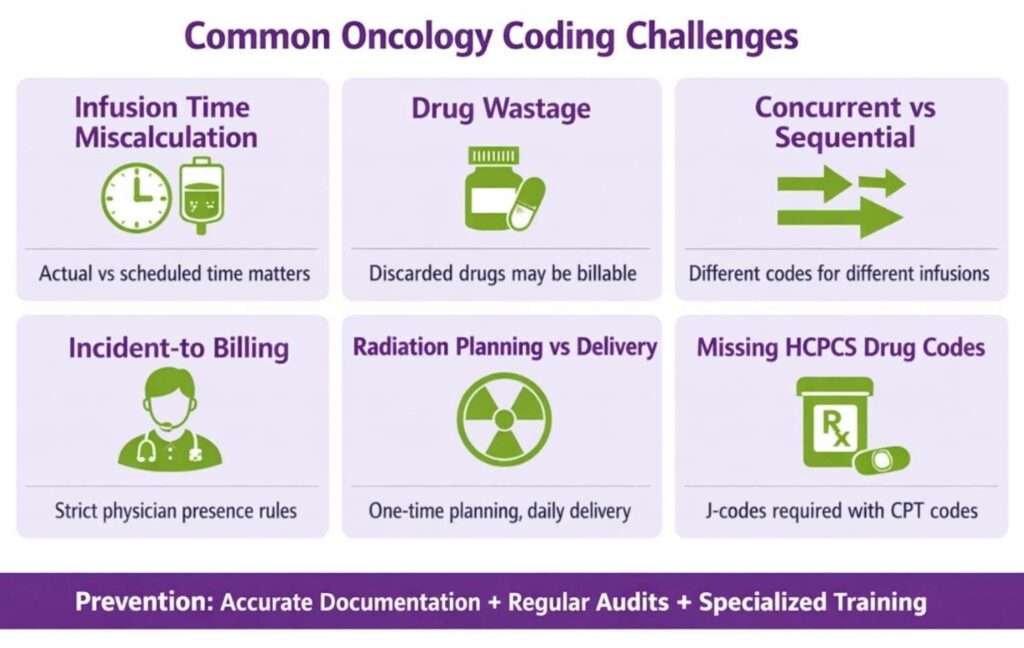
1. Infusion Time Miscalculation
Infusion units are based on actual infusion time, not scheduled time. If a one-hour infusion runs for 72 minutes, you may be able to bill for an additional unit depending on payer policy. Conversely, billing for two hours when the infusion ran for 55 minutes is overcoding. Nursing notes must capture start and stop times accurately.
2. Drug Wastage
When expensive oncology drugs are prepared, and a portion is discarded, the full amount prepared (including the discarded portion) may be billed under some payer policies. Medicare allows billing for discarded drugs under specific conditions. This must be supported by drug administration records and pharmacy logs.
3. Concurrent vs. Sequential Infusions
Concurrent infusions (two drugs running at the same time) are coded differently from sequential infusions (one drug after another). Using the wrong code is a frequent audit trigger.
4. Incident-to Billing in Oncology
When a mid-level provider (NP or PA) sees an established oncology patient under physician supervision, “incident-to” billing may apply for Medicare, allowing reimbursement at 100% of the physician fee schedule rather than 85%. However, the requirements are strict: the physician must be present in the suite and must have been involved in the initial visit and the ongoing treatment plan.
5. Radiation Planning vs. Delivery
Planning codes and delivery codes are often confused or improperly sequenced. Planning codes (77261 through 77295) are one-time codes per course of treatment. Delivery codes are billed each day treatment is delivered. Billing planning codes repeatedly for the same course of treatment is a compliance violation.
6. Missing HCPCS Drug Codes
Chemotherapy drugs have HCPCS J-codes (e.g., J9035 for bevacizumab, J9355 for trastuzumab) that must be billed alongside the CPT administration code. Submitting the administration code without the J-code or using an incorrect J-code results in claim denials or payment discrepancies.
Best Practices for Oncology Coding
Implementing strong coding practices protects your revenue and keeps your practice compliant. Here are the most impactful steps oncology billing teams can take.
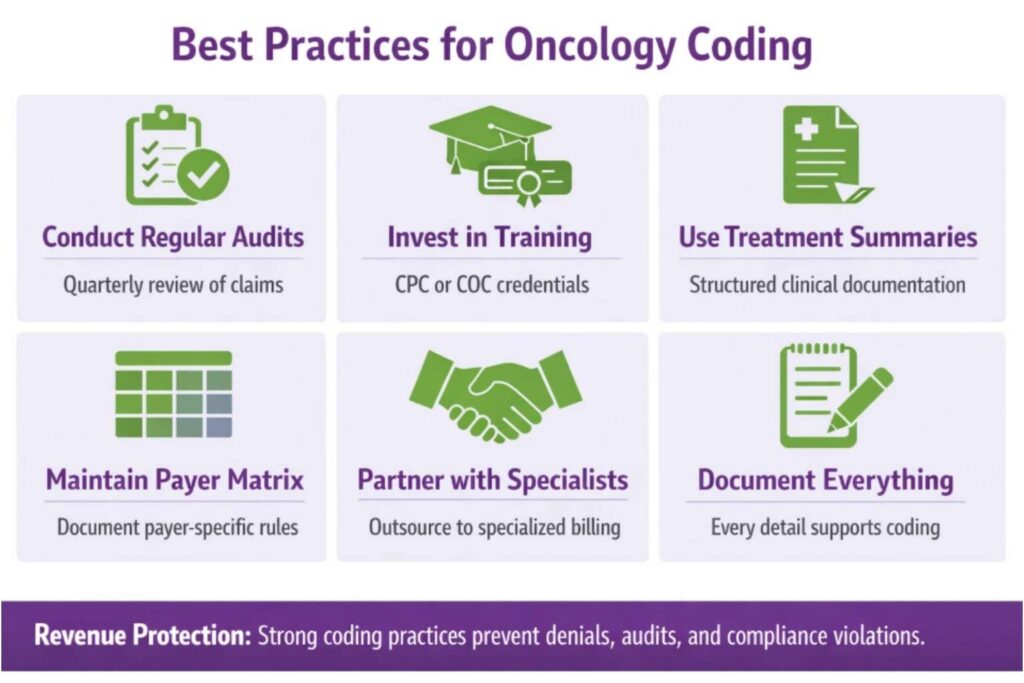
1. Conduct Regular Coding Audits
Internal audits should review a sample of chemotherapy infusion claims, radiation treatment records, and E/M documentation at least quarterly. Audits catch systemic errors before they accumulate into significant compliance exposure.
2. Invest in Oncology-Specific Training
General medical billing training is not sufficient for oncology. Coders who specialize in cancer care should obtain credentials such as the Certified Professional Coder (CPC) with oncology-specific continuing education, or the AAPC’s Certified Oncology Coder (COC) designation.
3. Use Treatment Summaries as a Coding Resource
Oncologists often document detailed treatment summaries that include drug names, dosages, infusion durations, and response assessments. This documentation is a rich resource for coders if it is structured and accessible.
4. Maintain a Payer Policy Matrix
Create and maintain a reference document for your top five to ten payers that outlines their specific rules for chemotherapy billing, radiation codes, prior authorization requirements, and bundling edits. Rules differ significantly between Medicare and commercial plans.
5. Partner with a Specialized Billing Company
Many oncology practices benefit from outsourcing the revenue cycle to a billing company that specializes exclusively in cancer care. Specialized partners bring deep payer knowledge, proprietary claim-editing tools, and the ability to stay current with rapidly changing codes and policies.
Transcure supports oncology practices across the United States with dedicated medical billing and coding teams.
6. Document Everything
In oncology, documentation is not just a regulatory requirement; it is your financial foundation. Every infusion start and stop time, every drug dosage, every treatment decision, and every weekly management encounter must be captured in a way that supports the codes being billed. If documentation does not support the code, the code cannot be defended.
Note: Certified Electronic Health Records (EHRs) with oncology-specific templates can significantly improve documentation quality and consistency. If your current EHR does not support structured oncology documentation, it is worth evaluating alternatives.
Conclusion
Oncology billing sits at the intersection of medicine’s most complex treatments and healthcare’s most demanding administrative requirements. Every category of CPT oncology codes carries its own set of rules, hierarchies, payer policies, and compliance risks. From E/M visits and chemotherapy infusion codes to CPT codes for radiation oncology, supportive therapies, molecular pathology, and emerging therapies like CAR T-cell treatment, the breadth of knowledge required is substantial.
For billing professionals in the United States, staying current on CPT codes in oncology medical billing is not a one-time task; it is a continuous commitment. The AMA updates CPT codes annually. CMS revises coverage policies. New therapies enter the market. Payer contracts evolve. The practices that protect their revenue and stay out of audit trouble are the ones that treat coding as a clinical discipline, not just an administrative function.
If your practice is facing denials, revenue leakage, or compliance concerns in oncology billing, working with an experienced partner can make a measurable difference. Transcure’s oncology billing team works with practices nationwide to reduce claim denials, accelerate reimbursement, and maintain full compliance with payer and regulatory requirements.
The codes are complex. The stakes are high. But with the right knowledge, the right documentation, and the right billing partner, oncology practices can operate with both clinical excellence and financial confidence.