
An ASTRO survey reports that oncology physicians handle about 39 prior authorization requests weekly, consuming 13+ staff hours. Billing for chemotherapy and specialty drugs further complicates the process. Nearly 30% of oncology claims are initially denied, forcing practices to spend additional time on appeals and corrections and straining revenue.
Cancer care usually involves expensive drugs, frequent treatments, and highly specialized procedures. Every step, from prior authorization to claim submission, can impact how quickly practices receive payment and how smoothly patients receive care.
This guide is for billers, coders, practice managers, and oncologists who are done accepting those numbers as normal. Whether your practice is managing chemotherapy drug codes, navigating prior authorization, or recovering from high denial rates, working with dedicated oncology medical billing services ensures every claim is handled with the specialty expertise it demands.
What is Oncology Medical Billing
Oncology medical billing is the process of submitting claims to insurance companies and other payers for services tied to cancer management. That includes verifying patient coverage, documenting medical history with precision, submitting claims on time, and staying compliant with a regulatory environment that changes every single year.
Types of Oncology Billing
Not all oncology billing is the same. There are four main categories, and each one carries its own set of code families, documentation rules, and payer expectations.
- Medical Oncology Billing covers drug-related care: chemotherapy, biologics, immunotherapy, and supportive follow-up services. The drug codes alone can take years to fully master.
- Radiation Oncology Billing involves both physician services and technical equipment use. A single treatment session can require multiple codes, and after the 2026 code restructuring, the rules changed significantly.
- Surgical Oncology Billing covers procedures like biopsies, tumor resections, and lymph node dissections. These follow surgical code conventions but often intersect with oncology-specific rules around staging and documentation.
- Hematology Billing overlaps heavily with oncology, particularly for leukemia, lymphoma, and blood disorders. The coding distinction between what is hematology and what is oncology matters for payer classification.
Facility Billing vs. Professional Billing
This distinction trips up a lot of practices, especially ones that recently transitioned from hospital-based to independent settings.
Facility billing covers services provided by an institution: hospitals, surgery centers, and clinics. Professional billing itemizes services from individual providers such as physicians, labs, and durable medical equipment suppliers.
In oncology specifically, this matters because radiation services are frequently split between a facility and a physician. Bill it wrong, and you either leave money on the table or trigger an audit.
Who Are the Primary Payers?
- Medicare and Medicaid (a significant share of oncology patients)
- Commercial insurers (with their own, often inconsistent, coverage policies)
- Secondary insurance is especially relevant when coordination of benefits is involved
- Clinical trial sponsors, for trial-related costs that should never go to the patient’s regular insurance
Medical vs. Radiation Oncology Billing
Medical Oncology Billing
It focuses on drug-related care such as chemotherapy, biologics, and immunotherapies. This part also includes follow-up visits and supportive treatments. And the tricky thing here is that drug costs are enormous, payers know it, and they scrutinize every unit billed. One wrong dosage number on a J-code and the whole claim gets kicked back. The documentation burden is real, and it only gets heavier as treatment plans get more personalized.
Radiation Oncology Billing
Radiation Oncology billing involves both physician services and the technical use of equipment. Each radiation session often requires several codes, making accuracy essential. What makes this particularly difficult is that the professional and technical components are sometimes billed by two completely separate entities, and they both have to line up. After the 2026 code overhaul, a lot of practices were essentially starting from scratch on how they classified delivery levels. Same code numbers, totally different meanings. That caught more people off guard than it should have.
Why Right Oncology Medical Billing Actually Matters
You have to be spot on every time with oncology medical billing and codes. Here is why it matters the most.
1. Financial Sustainability
There are an estimated 2 million new cancer cases in the United States in 2024. Cancer care spending is on track to hit over $240 billion by 2030. Without efficient billing, oncology practices cannot cover the costs of advanced treatments, specialized equipment, or the staff needed to deliver real cancer care.
That is not a hypothetical risk. Practices close because of billing failures.
2. Patient Care Quality
Here is something that does not get talked about enough. Billing inaccuracies do not just hurt the practice’s finances. They hurt patients. A denied claim delays treatment authorization. A coding error slows down reimbursement and forces staff to chase paperwork instead of supporting patients. For someone going through chemotherapy, unnecessary financial stress is not a small thing.
3. Compliance and Legal Risk
Oncology billing has to follow guidelines from insurance providers, Medicare and Medicaid, and HIPAA. Getting it wrong is not just expensive. It can lead to audits, financial penalties, and in serious cases, legal consequences. The stakes are high enough that compliance has to be built into every step of the process, not treated as an afterthought.
4. Cancer Data and Research
This one surprises people. The codes assigned to oncology claims feed directly into cancer registries, treatment audits, and population health studies. Accurate coding is not just about getting paid. It is about contributing reliable data that informs how cancer is understood and treated at a population level.
Insurance, Prior Authorization, and Payer Rules
1. Understanding Payer-Specific Policies
Medicare, Medicaid, and commercial insurers all have different coverage rules for the same oncology services. There is no universal standard. Chemotherapy infusion rules, high-cost drug policies, multi-session billing, and documentation requirements all vary by payer. Billing staff have to know the specific rules for each payer the practice contracts with.
2. Prior Authorization Best Practices
Build a PA tracking system organized by payer and drug or service type. When submitting for high-cost treatments, precise HCPCS and ICD-10 codes are required to establish medical necessity. Coding errors are one of the leading causes of PA rejections, which creates a domino effect of treatment delays and billing delays.
Document clinical urgency explicitly when requesting expedited reviews. Payers will not assume urgency. It has to be stated.
3. Handling Retro-Authorizations
Emergent oncology services sometimes start before authorization is secured. Retroactive authorization is a difficult process, but not impossible. Submit retro-auth requests promptly with complete clinical justification. Have a dedicated appeal pathway specifically for retro-auth denials.
4. Coordination of Benefits
Identify the primary and secondary payer at registration. Submit to the primary payer first, then use the explanation of benefits to bill the secondary. Preventing duplicate billing errors during COB claims requires a clear process, not just good intentions.
5. Medicare-Specific Rules
Hospital Outpatient Prospective Payment System rules differ from physician office billing rules for the same service. Local Coverage Determination policies vary by Medicare Administrative Contractor.
CMS and ASCO both publish oncology-specific guidance covering ICD-10 updates, CPT revisions, and annual Physician Fee Schedule changes that directly affect oncology reimbursement. These resources are worth bookmarking.
Why Oncology Billing is So Complex
The high cost, intensive documentation for specific drugs, and frequent coding changes are some factors that make it a tough nut to crack. Here is the breakdown of those.
1. Multiple Treatment Modalities in One Patient Plan
A single patient might receive surgery, then chemotherapy, then radiation, then immunotherapy, all within the same care timeline. Each of those phases uses different code sets. Each has different documentation requirements. There is no clean handoff point where one billing category ends and another begins.
2. High-Cost Drugs
CAR T-cell therapy costs upwards of $373,000 per patient. Biologics and immunotherapies routinely run into tens of thousands of dollars per cycle. Payers scrutinize these claims heavily, and the codes for reimbursing them evolve constantly. A coder who was current two years ago may not be current today.
3. Personalized Treatment Plans
The shift toward personalized medicine, where treatment is tailored to the specific patient’s cancer type, stage, and overall health, means that no two patient billing profiles look exactly alike. Coding for a wide range of services within the same patient’s care plan requires billers who understand clinical context, not just code lookup.
4. Multidisciplinary Teams
Oncology care involves medical oncologists, surgical oncologists, radiation oncologists, and allied health professionals all working on the same patient. Every service from every provider needs to be billed accurately and without duplication. Coordinating that across a team is genuinely difficult.
5. The Continuum of Care
Billing spans from initial diagnosis through active treatment, survivorship, and, in some cases, palliative care. Each phase has distinct coding requirements. Moving a patient from active treatment codes to survivorship codes at the wrong time is a common and costly error.
6. Constant Code Changes
In 2026, radiation oncology coding underwent its most significant overhaul in over a decade. New technique-agnostic delivery codes replaced long-standing ones. This kind of shift requires immediate action from both clinical and coding staff. Practices that were slow to adapt saw incorrect payments and increased denials within weeks of the change.
The Biggest Challenges Practices Face
Oncology billing is not just about submitting claims. It is a constant battle between complex treatments, strict payer rules, and high financial stakes. Even a small mistake can delay care or cost thousands in lost revenue.
Before practices can improve collections, you need to understand where things actually go wrong.
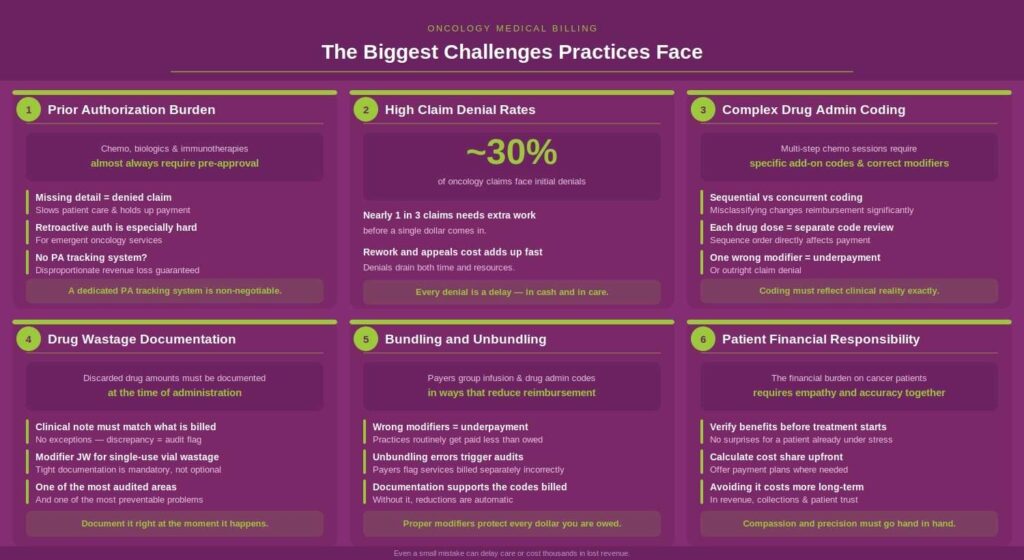
1. Prior Authorization Burden
Chemotherapy, biologics, and immunotherapies almost always require approval before treatment begins. Any delay or missing detail results in a denial, which slows down patient care and holds up payment. Retroactive authorization for emergent oncology services is particularly difficult. Practices without a dedicated PA tracking system tend to lose a disproportionate amount of revenue in this area.
2. High Claim Denial Rates
Nearly 30% of oncology claims face initial denials. That means nearly one in three claims requires additional work before a dollar comes in. The cost of reworking and appealing those claims adds up fast.
3. Complex Drug Administration Coding
One of the genuinely tricky parts of oncology drug billing is coding sequential doses. Multi-step chemotherapy sessions, where the patient receives several drugs in sequence, require specific add-on codes and correct use of modifiers. Misclassifying concurrent administration as sequential, or the reverse, changes reimbursement significantly.
4. Drug Wastage Documentation
Any discarded drug amounts must be documented at the time of administration. The clinical note has to match what is billed. This is one of the most commonly reviewed areas in payer audits, and it is one of the most preventable problems. Using Modifier JW for single-use vial wastage and keeping that documentation tight is not optional.
5. Bundling and Unbundling
Payers apply bundling rules to oncology services that can group infusion and drug administration codes in ways that reduce reimbursement. Without proper modifiers and documentation, practices routinely get paid less than they are owed.
6. Patient Financial Responsibility
The financial burden on oncology patients is significant. Verifying benefits upfront, calculating patient cost shares before treatment, offering payment plans where needed, and doing all of that with empathy toward someone who is already managing a serious diagnosis. That is a lot to ask of a billing team. But avoiding it costs more in the long run.
Critical Billing Codes You Need to Know
The following are some of the commonly used codes in Oncology billing. We also have a guide containing an in-depth directory of CPT codes for oncology billing.
ICD-10 Diagnosis Codes
Use primary malignancy codes from the C00 to C96 range as long as the patient is receiving active treatment. Once treatment ends and the patient enters remission, switch to personal history codes like Z85 or Z86. This distinction directly communicates to payers whether services relate to ongoing care or post-treatment follow-up. Getting it wrong is a common source of denials.
ICD-10 Sequencing Rules
The sequencing of diagnosis codes is not arbitrary. When the visit is primarily for treating the malignancy, the cancer code leads. If the encounter is mainly for chemotherapy, immunotherapy, or radiation, assign the appropriate Z code first:
- Z51.11 for chemotherapy
- Z51.0 for radiation therapy
Then follow with the malignancy code. Always code to the highest level of specificity supported by the documentation.
E/M Codes
E/M codes (99202 through 99215) apply to consultations, follow-up visits, and ongoing management. In oncology, the medical decision-making involved is typically of high complexity, which means higher-level codes are frequently appropriate and defensible. The documentation just has to support it.
Chemotherapy Administration CPT Codes
These are time-based codes. Start and stop times are not optional documentation.
- 96413: IV infusion, initial, up to 1 hour
- 96415: Each additional hour
- 96401: Non-infusion injection or push
- 96402: Hormonal antineoplastic injection
Every code requires the drug name, dosage, administration route, and documented start and stop times.
Non-Chemotherapy Infusion and Hydration Codes
- 96360 to 96361: Hydration infusion
- 96365 to 96368: Therapeutic, prophylactic, or diagnostic infusion (non-chemo)
These cannot be billed as chemotherapy unless specifically documented as antineoplastic. The distinction matters for both compliance and reimbursement.
Radiation Oncology CPT Codes
Planning codes run from 77261 to 77299 and cover treatment planning and simulation. The 2026 delivery code restructuring introduced technique-agnostic codes:
- 77402: Radiation treatment delivery, Level 1
- 77407: Radiation treatment delivery, Level 2
- 77412: Radiation treatment delivery, Level 3
These code numbers are not new. What changed is the definition. Practices that assumed the old meanings applied without reviewing the updated guidance have been getting paid incorrectly.
HCPCS Level II J-Codes
J-codes report the actual drug administered. Units must reflect the dose actually given, not the dose ordered or a rounded figure. Incorrect unit reporting is one of the leading causes of oncology claim denials and payer audits.
New and Emerging Codes
The 2025 CPT revisions added new Category I codes for CAR T-cell therapy (38225 to 38228) and revised surgical codes based on tumor size. Category III codes, like bone marrow sampling port code 0901T, may have limited payer coverage. Verification before billing is essential.
Chemotherapy vs. Immunotherapy Billing
How Chemotherapy Billing Works
Chemotherapy billing is time-based. The initial hour uses a different code from the additional hours. Sequential drug administration uses Modifier EJ for every dose after the first. Worth noting: there is no CPT code for concurrent administration of multiple chemotherapy drugs. Multiple drugs given in the same session are coded sequentially, not concurrently. That is a source of confusion that costs real money.
Required documentation for every session:
- Drug name
- Dosage
- Administration route
- Start and stop times
- Wastage amounts
How Immunotherapy and Biologic Billing Works
Biologics and immunotherapies are generally billed under therapeutic infusion codes, not chemotherapy codes, unless specifically classified as antineoplastic. The higher drug costs mean payers apply significantly more scrutiny. Prior authorization is almost always required, and the medical necessity documentation has to be thorough.
Supportive Drug Billing
Hydration and supportive medications like antiemetics and growth factors have their own CPT codes. Infusion hierarchy rules determine how these are sequenced with chemotherapy and therapeutic infusions. More on that in the claims submission section.
Clinical Trial Billing
Routine care costs in clinical trials are billed to the patient’s insurance. Trial-related services go to the sponsor. This distinction requires careful, deliberate separation of charges. Billing trial-related costs to insurance is a compliance risk.
| Aspect | Chemotherapy Billing | Immunotherapy Billing |
|---|---|---|
| Treatment Type | Cytotoxic drugs that kill rapidly dividing cancer cells | Biologic agents that stimulate the immune system to fight cancer |
| Common Drug Codes | Mostly J9000–J9999 (e.g., J9267 for Paclitaxel) | J codes, Q codes, and sometimes C codes (e.g., J9271 for Pembrolizumab) |
| Administration Codes | CPT 96401–96549 (chemo administration hierarchy applies) | Often billed under therapeutic/biologic administration (96401–96417 depending on route) |
| Coding Complexity | High due to sequential, concurrent, and combination infusions | Moderate to high; fewer drugs per session, but complex drug-specific rules |
| Prior Authorization | Almost always required | Strict and often more detailed due to high-cost biologics |
| Frequency of Treatment | Typically cyclical (e.g., every 2–3 weeks) | Can be less frequent but long-term (e.g., every 3–6 weeks) |
| Drug Cost | High but relatively standardized | Extremely high; significant cost variation between drugs |
| Modifiers Used | Common use of modifiers (e.g., 59, 76, JW for wastage) | JW modifier is frequently used for single-use vial wastage |
| Documentation Requirements | Detailed infusion times, sequence of drugs, and administration method | Detailed drug justification, biomarker results, and treatment plan documentation |
| Denial Risks | Errors in the administration hierarchy, missing modifiers, and bundling issues | Lack of medical necessity, missing biomarker data, or authorization gaps |
| Reimbursement Challenges | Errors in the coding sequence can significantly impact payment | High scrutiny from payers due to drug costs and emerging therapies |
| Audit Focus Areas | Infusion timing, drug sequencing, and wastage documentation | Medical necessity, FDA indications, biomarker alignment |
Radiation Oncology Billing
Professional vs. Technical Components
Professional component: the physician’s work in planning, supervising, and interpreting. Technical component: the equipment, facility, and staff operating the machine.
Global billing covers both. Split billing separates them into two claims. Getting this wrong in either direction causes problems. Billing globally when services are split between a physician and a facility is one of the most common radiation oncology billing mistakes.
Treatment Planning Codes
Simple, intermediate, and complex planning use codes 77261, 77262, and 77263, respectively. Simulation and dosimetry have their own codes. The clinical rationale for the global complexity level must be documented. Payers are increasingly scrutinizing whether the complexity level billed matches the clinical picture.
The 2026 Delivery Code Update
The new technique-agnostic delivery codes (77402, 77407, 77412) fundamentally changed how radiation treatment is classified. The old structure was organized by technique. The new structure is organized by delivery level. Both clinical staff and coding staff need to understand the distinction. Practices that trained only coders and not clinicians on this change have seen documentation gaps that result in incorrect billing.
Stereotactic Radiosurgery and Special Procedures
SBRT, SRS, and IMRT each use distinct code sets with strict documentation requirements. Payer coverage policies for advanced techniques vary significantly. Assuming one payer’s rules apply to another is a consistent source of denials.
Modifiers in Oncology Billing
Modifiers give payers context. Without them, automatic bundling rules kick in and reimbursement drops. Incorrect or missing modifiers are among the top causes of underpayment in oncology.
Key Modifiers to Know
| Modifier | Description | When to Use |
|---|---|---|
| 59 | Distinct procedural service | Two procedures that are independent and not ordinarily reported together |
| JW | Drug wastage | Discarded amounts from single-use vials only |
| EJ | Subsequent drug in a series | Every sequential dose after the first |
| 26 | Professional component | When billing only the physician’s portion |
| TC | Technical component | When billing only the facility or equipment portion |
| GY | Statutory exclusion | Services Medicare explicitly excludes |
| KX | Medical necessity met | Required by some payers for specific oncology services |
Modifier 59 vs. X-Modifiers
CMS introduced X-modifiers (XE, XS, XP, XU) as more specific subsets of Modifier 59. Payer policies on which to use differ. Medicare has a preference for X-modifiers when they apply. Many commercial players still accept 59. Know your players.
Modifier JW Deep Dive
Use Modifier JW specifically for discarded amounts from single-use vials. Do not apply it to multi-dose vials. The clinical note and the claim must match on wastage. This area is a frequent target of payer reviews, and inconsistency between documentation and billing is hard to defend.
The Step-by-Step Billing Process
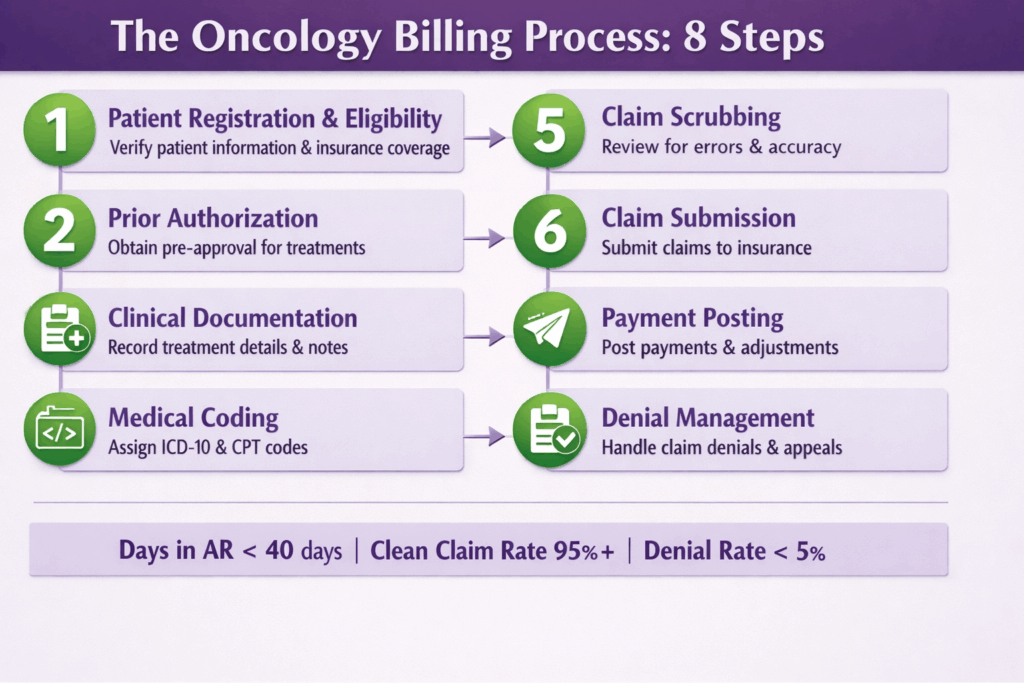
Step 1: Patient Registration and Eligibility Verification
Collect complete demographics and insurance information at registration. Verify eligibility specifically for oncology services: chemotherapy, radiation, biologics. Identify secondary insurance early to prevent coordination-of-benefits errors down the line. Communicate patient financial responsibility before the first treatment. Surprises later create collection problems.
And honestly, this step deserves more respect than it usually gets. Front desk staff are often undertrained for oncology-specific verification, which means they confirm that a patient has insurance without confirming that their plan actually covers the specific drugs or delivery methods being used. Those are two very different things. Ask the payer directly about chemotherapy infusion coverage, biologic authorization requirements, and out-of-pocket maximums. A 10-minute call before treatment can prevent a three-month billing headache.
Step 2: Prior Authorization
Most high-cost oncology drugs and radiation services require prior authorization. Submissions should include diagnosis details, staging information, the projected therapy plan, and supporting clinical notes. Target submission within 24 to 48 hours of treatment scheduling. PA errors cause denials that are expensive and time-consuming to resolve.
What actually makes PA submissions fail is vagueness. Payers are not going to fill in the blanks for you. If the submission does not include the exact ICD-10 codes, the specific HCPCS J-codes for the drugs being used, and a clear clinical rationale tied to the diagnosis, it will get kicked back. Build a PA template for your most common drugs and radiation services. That alone cuts turnaround time significantly. Also, keep a log of PA approval windows by payer because some expire in 30 days and some last 90, and billing outside that window is an automatic denial, regardless of everything else being correct.
Step 3: Clinical Documentation
Drug names, dosages, administration routes, start and stop times, and wastage notes need to be fully documented and consistent between clinical records and billing records. Coders need to work with providers on what exactly the note must capture. This is not a coder problem alone. It is a provider education problem.
The gap between what a physician documents and what a coder needs to bill is where a surprising amount of revenue quietly disappears. A note that says “chemo administered” is not enough. The coder needs the specific drug name, the exact dose, the route, the start time, the stop time, and whether any drug was discarded. Providers are not always aware of this, and that is not really their fault. Regular brief check-ins between coding staff and clinical staff, even just a monthly 20-minute review of common documentation gaps, can fix this faster than any software will.
Step 4: Medical Coding
Assigning the right ICD-10 codes, CPT codes, and modifiers is only half the battle. Before any claim goes out the door, it needs to pass through a thorough claim scrubbing process that catches mismatched codes, missing modifiers, incorrect unit reporting, and sequencing errors. In oncology, where a single J-code error can trigger a denial on a $50,000 drug claim, this step is not optional. It is the last line of defense between a clean submission and a costly rework.
The sequencing piece is especially underestimated. A claim where the diagnosis codes are all technically correct but ordered wrong will still get denied or underpaid by certain payers. And modifier application is not a box-checking exercise. Each modifier has to be justified by the documentation. If you are applying Modifier 59 to separate two procedures, there has to be a clear clinical reason that those services were distinct. Payers are getting better at flagging modifier misuse, and repeated incorrect modifier patterns can trigger an audit. A 15-minute pre-submission review by a second coder on high-dollar claims pays for itself quickly.
Step 5: Claim Submission
Before submission, verify that ICD-10 diagnosis codes, CPT procedure codes, NDCs, units, and charges all align with the prior authorization and match payer-specific requirements. A clean claim rate of 95% or higher should be the target.
The NDC piece catches a lot of practices off guard. National Drug Codes need to match exactly what was administered, right down to the specific package size and manufacturer. If the NDC on the claim does not match the NDC in the PA approval, some players will deny it outright. Also worth noting: unit reporting for J-codes has to reflect the actual administered dose, not the vial size or the ordered dose. If 450mg of a drug was given, but it comes in 500mg vials, you bill for 450mg. That difference matters both for accuracy and for avoiding wastage code issues later.
Step 6: Payment Posting and Reconciliation
Post payments accurately against each claim line. Flag underpayments, which are especially common in complex infusion billing. Reconcile against contracted rates. Underpayments that are not caught get written off by default.
Here is the part nobody talks about enough. Underpayments are extremely common in oncology infusion billing, and most of them never get corrected because the volume of claims makes it easy to miss. A payer might reimburse the initial infusion hour correctly, but short-pay the add-on hours at a rate below your contract. Multiply that by dozens of patients per week, and the loss is real. Build a reconciliation step that compares payment against your fee schedule and flags anything more than a 5% discrepancy. It is tedious, yes. But it is also money that is already owed to you.
Step 7: Denial Management and Appeals
Categorize denials by root cause: coding, prior authorization, eligibility, or documentation. Set appeal timelines by payer. Track denial trends monthly to identify systemic issues rather than treating every denial as a one-off event.
The “one-off” mindset is where denial management falls apart. When a practice treats each denial as its own isolated problem, the same issues repeat indefinitely because no one is looking at the pattern. If three denials this month all came back with the same reason code from the same payer for the same drug, that is a workflow problem, not a one-time mistake. Monthly denial reporting by payer, by code, and by denial type is what separates practices that manage denials reactively from those that actually reduce them over time. Feed what you find back into your pre-submission checklist and coder education.
Step 8: Patient Billing and Collections
Issue clear, itemized statements. Offer payment plans for high out-of-pocket balances. Connect patients with financial assistance programs where available. Oncology patients are managing enough. The billing experience should not add to the burden.
This step requires a different kind of skill than the rest of the process. The person receiving that statement is not just a balance to collect. They are someone going through one of the hardest seasons of their life. That does not mean you avoid collecting, but it does mean how you communicate matters a lot. Plain-language statements that explain what the charges are for, a proactive call before sending a large balance, and a straightforward conversation about payment options go a long way. Many patients do not know that manufacturer assistance programs, hospital charity care, or nonprofit foundations exist to help with drug costs. Your billing team pointing them in that direction is genuinely useful and builds trust that makes collections easier, not harder.
Denial Management That Actually Works
Most Common Reasons for Oncology Claim Denials
- Missing or invalid prior authorization
- Incorrect or mismatched CPT and ICD-10 codes
- Missing modifiers
- Drug unit errors, specifically wrong units for J-codes
- Infusion hierarchy sequencing errors
- Insufficient documentation for medical necessity
- Eligibility issues at the time of service
The majority of these are preventable. That is both frustrating and hopeful.
Building a Denial Management Workflow
Categorize every denial by root cause on receipt. Assign resolution responsibilities by denial type. Set internal appeal deadlines well before the payer deadline, typically 30 to 60 days prior. Track the denial rate as a core KPI with a target below 5% initial denial rate.
How to Write a Winning Appeal
Include clinical notes, the specific coding rationale, relevant medical literature when applicable, and the PA approval. Reference the payer’s own Local Coverage Determination or coverage policy language when you can. Request a peer-to-peer review for medical necessity denials. During peer-to-peer conversations, ask directly what documentation the payer needs to approve the claim. Do not guess.
Tracking Denial Trends
Monthly denial reporting should break down by payer, by code, and by denial reason code. The goal is to identify which players deny most frequently and for what reason. Feed those findings back into coder education and pre-submission checklists. Denial management is a feedback loop, not a one-time fix.
When to Appeal vs. When to Write Off
Evaluate cost-to-collect against expected reimbursement. Never write off without an appeal on high-dollar oncology drug claims. Track write-off rates to identify systemic payer issues. A sudden spike in write-offs for a specific code or payer is a signal worth investigating.
Revenue Cycle Optimization for Oncology Practices
Key KPIs to Track
- Days in Accounts Receivable: target under 40 days
- Clean Claim Rate: target 95% or higher
- First-Pass Denial Rate: target under 5%
- Prior Authorization Approval Rate
- Net Collection Rate
- Cost to Collect per Claim
These numbers tell a real story about where a practice is losing revenue and where it is performing well.
Credentialing and Payer Contracting
All providers must be credentialed with relevant payers before treating patients. Billing for a non-credentialed provider is a denial waiting to happen. Renegotiate contracts based on claim volume and complexity. Specifically verify contracted rates for high-cost drugs and biologics. Those rates can be significantly below the actual cost of administering the drugs.
Staff Training and Coder Certification
Oncology-specific coder training through AAPC or AHIMA is worth the investment. Annual code updates require ongoing education, especially after major overhauls like the 2026 radiation oncology restructuring. Front-desk staff should understand PA basics and eligibility fundamentals. Their work at registration directly affects what happens downstream.
In-House vs. Outsourced Billing
In-house billing offers control and direct provider communication, but the fixed costs are high, and the expertise gap in oncology-specific coding is real. For many practices, outsourced medical billing services provide the specialty knowledge, scalability, and performance accountability that an internal team simply cannot match, especially when managing high-cost drug claims and complex infusion hierarchies.
If evaluating an outsourced oncology billing vendor, ask:
- What is your PA turnaround time?
- What is your denial rate for oncology claims?
- What certifications do your coders hold?
- What does your audit process look like?
It is also recommended to get help from top oncology billing companies, especially if you have a busy practice that is facing rising denials and A/R.
Technology and RCM Efficiency
Oncology-specific EHR and billing software integration is not a luxury. Generic practice management systems often do not handle infusion hierarchy rules or J-code unit calculations correctly. Automated eligibility verification at scheduling catches coverage gaps before they become denials. AI-assisted coding tools trained on oncology code sets can catch errors pre-submission. Real-time denial tracking dashboards give revenue cycle managers the visibility they need to act quickly.
Compliance Program Essentials
Run internal audits on a random sampling of claims and on targeted high-risk codes. Stay current with ASCO, CMS, and AAPC guidance. During major code transitions, track denials and payments carefully for the first 60 to 90 days. Incorrect payments during transition periods are common and often go unnoticed without active monitoring.
Conclusion
Oncology billing is, without question, the most complex specialty in healthcare revenue cycle management. The combination of high-cost drugs, evolving treatment modalities, frequent code changes, and a 30% initial denial rate creates a billing environment where the margin for error is small, and the consequences of getting it wrong are significant.
The highest-leverage areas are prior authorization, denial management, and documentation. Everything else flows from those three. Get those right, and the rest of the process becomes more manageable. Ignore them, and no amount of technology or staffing will fully compensate.
If your practice is not where it needs to be, the place to start is with data. Pull your denial rate, identify the top three root causes, and start there. Not with a complete overhaul. Just the three biggest problems. Fix those, and then move to the next three.
The practices that consistently perform well in oncology billing are not necessarily the ones with the biggest teams or the most sophisticated software. They are the ones who treat billing as a clinical-adjacent function that deserves the same rigor and ongoing education as direct patient care.
Frequently Asked Questions
What is the difference between medical oncology billing and radiation oncology billing?
Medical oncology billing focuses on drug-related care and chemotherapy administration. Radiation oncology billing covers treatment planning and delivery, often involving both professional and technical components billed separately.
Why do oncology claims get denied more often than other specialties?
Oncology claims involve complex drug coding, infusion hierarchy rules, frequent prior authorization requirements, and evolving code sets that create more opportunities for errors compared to less complex specialties.
What is Modifier JW used for in oncology billing?
Modifier JW is used to bill for discarded drug amounts from single-use vials. It should not be applied to multi-dose vials, and the wastage must be documented in the clinical record to match the claim.
How often do oncology billing codes change?
Oncology codes are updated annually through CPT and ICD-10 revisions. Major overhauls, like the 2026 radiation oncology delivery code restructuring, can occur less frequently but require significant training to implement correctly.
What is the infusion hierarchy rule?
The infusion hierarchy rule determines how multiple infusion services in the same encounter are sequenced and billed. Chemotherapy takes priority, followed by therapeutic infusion, then hydration. Only one initial code is billed per category per encounter.
When should a practice outsource oncology billing?
Outsourcing makes sense when the practice lacks oncology-specific coding expertise, when denial rates are consistently above 10%, or when staff cannot keep up with annual code updates. Vendor selection should prioritize specialty credentials and documented performance metrics.
What documentation is required for chemotherapy billing?
Every chemotherapy session requires documentation of the drug name, dosage, administration route, start and stop times, and any wastage amounts. Missing any one of these elements creates a risk for denial or audit.






