Pain management billing requires precise use of Current Procedural Terminology (CPT) codes to accurately reflect services rendered and ensure proper reimbursement. This guide covers the CPT codes for pain management, from office-based evaluation to complex interventional techniques, organized by category for quick reference.
Category 1: Evaluation & Management (E&M) Codes
Before moving into procedural coding, it’s important to understand E&M codes, as they are used to report every patient visit and guide overall billing accuracy.
Office / Outpatient E&M Codes (99202–99215 CPT Codes)
E&M codes are the foundation of every patient encounter. The 2021 AMA guidelines shifted documentation requirements to medical decision-making (MDM) or total time, no longer based purely on history and exam elements.
| CPT Code | Visit Type | Medical Decision Making | Typical Time |
|---|---|---|---|
| 99202 | New Patient – Low | Straightforward | 15–29 min |
| 99203 | New Patient – Low | Low Complexity | 30–44 min |
| 99204 | New Patient – Moderate | Moderate Complexity | 45–59 min |
| 99205 | New Patient – High | High Complexity | 60–74 min |
| 99211 | Established – Minimal | N/A (nurse visit) | N/A |
| 99212 | Established – Low | Straightforward | 10–19 min |
| 99213 | Established – Low | Low Complexity | 20–29 min |
| 99214 | Established – Moderate | Moderate Complexity | 30–39 min |
| 99215 | Established – High | High Complexity | 40–54 min |
NOTE: New patient codes (99202–99205) require that no qualifying physician in the same group has seen the patient in the past 3 years.
Prolonged Services
When the total encounter time exceeds the maximum threshold for 99215 (54 minutes), add-on prolonged service codes may be appended.
| CPT Code | Description | Threshold |
|---|---|---|
| 99417 | Prolonged outpatient E&M (per 15 min) | Appended to 99205 or 99215 at 55+ min |
| 99418 | Prolonged inpatient/observation (per 15 min) | Appended to 99223, 99233, or 99236 |
Telehealth E&M Codes
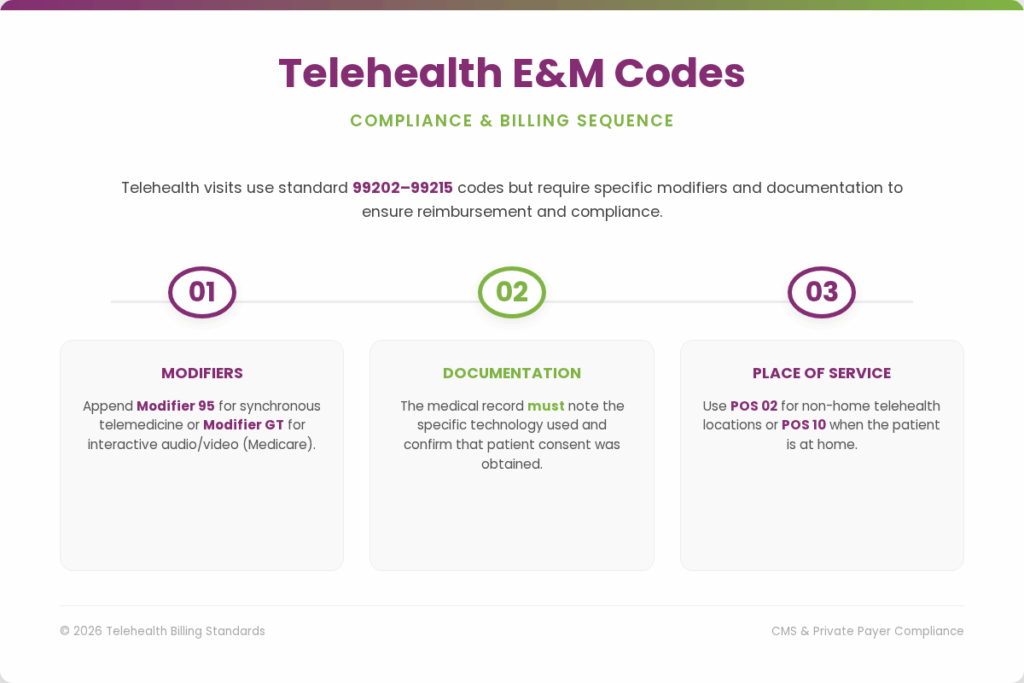
Telehealth visits use the same 99202–99215 codes but must be appended with modifier 95 (synchronous telemedicine) or GT (Medicare). Moreover, the documentation must note the technology used and patient consent.
- Modifier 95: Synchronous real-time telehealth
- Modifier GT: Interactive audio/video (Medicare)
- Place of Service 02: Telehealth (non-home) / POS 10 for the patient’s home
Category 2: Spinal Injection Procedures
After establishing the fundamentals of E&M coding, the next step is understanding spinal injection procedures. These form the core of interventional pain management and require precise CPT code selection based on technique, level, and imaging guidance.
Epidural Steroid Injections (ESIs)
Epidural steroid injections deliver corticosteroids into the epidural space to reduce inflammation around compressed nerve roots. Codes vary based on approach, such as interlaminar vs. transforaminal and spinal level.
Interlaminar Epidural Injections
In this approach, medication is delivered through the midline into the epidural space to provide broader pain relief across a spinal region.
| CPT Code | Description | Guidance |
|---|---|---|
| 62320 | Cervical/thoracic interlaminar epidural, without imaging | Without fluoroscopy/CT |
| 62321 | Cervical/thoracic interlaminar epidural, with imaging | With fluoroscopy or CT |
| 62322 | Lumbar/sacral interlaminar epidural, without imaging | Without fluoroscopy/CT |
| 62323 | Lumbar/sacral interlaminar epidural, with imaging | With fluoroscopy or CT |
Transforaminal Epidural Injections
This technique targets specific nerve roots by delivering medication through the neural foramen at a precise spinal level.
| CPT Code | Description | Levels |
|---|---|---|
| 64479 | Cervical/thoracic transforaminal epidural, single level | First level |
| 64480 | Cervical/thoracic transforaminal epidural, add-on | +Each additional level |
| 64483 | Lumbar/sacral transforaminal epidural, single level | First level |
| 64484 | Lumbar/sacral transforaminal epidural, add-on | +Each additional level |
NOTE: Transforaminal epidural steroid injections (ESIs) must be performed using fluoroscopic or CT guidance. The imaging guidance is already included (bundled) in CPT codes 62321, 62323, and all transforaminal injection codes. Therefore, CPT code 77003 should not be billed separately with these procedures.
Facet Joint Injections & Medial Branch Blocks
Facet joint injections and medial branch blocks target the small joints between vertebrae, a common source of axial back and neck pain.
Facet Joint Injections (Intra-articular)
These injections are placed directly into the facet joints to treat pain caused by inflammation or degeneration of spinal joints.
| CPT Code | Description | Notes |
|---|---|---|
| 64490 | Cervical/thoracic facet injection, first level | Unilateral |
| 64491 | Cervical/thoracic facet injection, second level | Add-on |
| 64492 | Cervical/thoracic facet injection, third+ level | Add-on |
| 64493 | Lumbar/sacral facet injection, first level | Unilateral |
| 64494 | Lumbar/sacral facet injection, second level | Add-on |
| 64495 | Lumbar/sacral facet injection, third+ level | Add-on |
Medial Branch Blocks (MBB)
Medial branch blocks are diagnostic injections targeting the nerves that supply the facet joints. The same codes 64490–64495 apply. Two separate MBBs on different dates may be required prior to radiofrequency ablation (payer-dependent).
Sacroiliac (SI) Joint Injections
Used to address lower back and pelvic pain, these injections target the sacroiliac joint for both diagnostic and therapeutic purposes.
| CPT Code | Description | Notes |
|---|---|---|
| 27096 | SI joint injection, with imaging guidance | Articular/periarticular; includes fluoroscopy |
| 0775T | SI joint injection, without imaging | Category III code (newer) |
Trigger Point Injections (TPI)
Focused on relieving muscle-related pain, these injections target tight knots or trigger points within specific muscles.
| CPT Code | Description | Muscle Groups |
|---|---|---|
| 20552 | Injection, single or multiple trigger points; 1 or 2 muscles | Any muscle group |
| 20553 | Injection, single or multiple trigger points; 3+ muscles | Multiple muscle groups |
NOTE: Trigger point injections do NOT require imaging guidance. Dry needling is not a CPT-coded procedure and is typically not covered by Medicare.
Joint Injections (Non-Spinal)
Covering peripheral joints, these procedures involve injecting or aspirating fluid from small, intermediate, or major joints with or without imaging guidance.
| CPT Code | Description | Joint |
|---|---|---|
| 20600 | Aspiration/injection, small joint, without US guidance | Finger, toe joints |
| 20604 | Aspiration/injection, small joint, with US guidance | Small joints w/imaging |
| 20605 | Aspiration/injection, intermediate joint, without US | Wrist, elbow, ankle |
| 20606 | Aspiration/injection, intermediate joint, with US | Intermediate w/imaging | 20610 | Aspiration/injection, major joint, without US | Shoulder, hip, knee |
| 20611 | Aspiration/injection, major joint, with US | Major joint w/imaging |
Category 3: Nerve Block Procedures
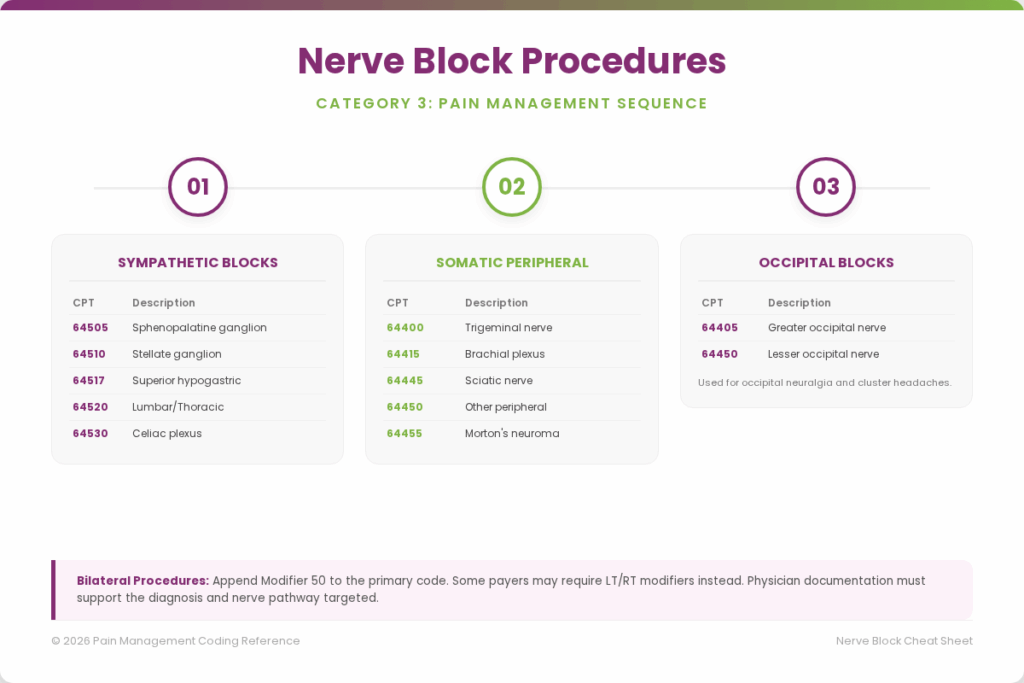
Following spinal injection procedures, nerve block techniques are another key component of pain management, used to diagnose and treat pain by targeting specific nerves or nerve pathways.
Sympathetic Nerve Blocks
These pain management CPT codes represent injections targeting the sympathetic nervous system to manage chronic pain conditions, especially those related to nerve dysfunction and visceral pain.
| CPT Code | Description | Indication |
|---|---|---|
| 64505 | Sphenopalatine ganglion block | Headache, atypical facial pain |
| 64508 | Carotid sinus nerve block | Carotid sinus syndrome |
| 64510 | Stellate ganglion block, cervical | CRPS, upper extremity pain, hot flashes |
| 64517 | Superior hypogastric plexus block | Pelvic/visceral pain |
| 64520 | Lumbar or thoracic sympathetic nerve block | CRPS, lower extremity pain |
| 64530 | Celiac plexus block, with or without radiologic monitoring | Abdominal/pancreatic pain |
Somatic Peripheral Nerve Blocks
This set of pain management CPT codes cheat sheet is used for injections that block specific peripheral nerves to relieve localized pain in different parts of the body.
| CPT Code | Description |
|---|---|
| 64400 | Trigeminal nerve block |
| 64405 | Greater occipital nerve block |
| 64410 | Phrenic nerve block |
| 64415 | Brachial plexus block, single injection |
| 64416 | Brachial plexus block, continuous infusion (catheter) |
| 64445 | Sciatic nerve block, single injection |
| 64446 | Sciatic nerve block, continuous infusion |
| 64450 | Other peripheral nerve or branch, block |
| 64455 | Plantar common digital nerve injection (Morton’s neuroma) |
Occipital Nerve Blocks
Greater and lesser occipital nerve blocks are commonly used for occipital neuralgia, cervicogenic headache, and cluster headaches.
| CPT Code | Description |
|---|---|
| 64405 | Greater occipital nerve block (unilateral or bilateral) |
| 64450 | Lesser occipital nerve block (use with modifier if bilateral) |
NOTE: For bilateral procedures, append Modifier 50 (bilateral) to the primary code. Some payers require LT/RT modifiers instead.
Category 4: Radiofrequency Ablation (RFA)
Radiofrequency ablation uses thermal energy to disrupt the medial branch nerves supplying the facet joints, providing longer-lasting pain relief than steroid injections. Prior diagnostic MBBs are generally required.
Facet Joint Denervation Codes
The following CPT codes in pain management coding are used to report facet joint radiofrequency ablation procedures based on spinal region and the number of treated levels.
| CPT Code | Description | Level |
|---|---|---|
| 64633 | Destruction by neurolytic agent, paravertebral facet joint nerve – cervical/thoracic, first level | 1st level |
| 64634 | Cervical/thoracic, each additional level | Add-on |
| 64635 | Destruction by neurolytic agent, paravertebral facet joint nerve – lumbar/sacral, first level | 1st level |
| 64636 | Lumbar/sacral, each additional level | Add-on |
NOTE: Fluoroscopic guidance is bundled into 64633–64636. Do NOT separately bill 77003 for imaging. Bilateral procedures require Modifier 50 or LT/RT modifiers.
Cooled & Pulsed RFA
Some advanced RFA techniques, such as cooled radiofrequency (e.g., Coolief), may use the same 64635/64636 codes or may fall under Category III codes depending on the payer. Pulsed RFA is generally coded under 64999 (unlisted) or Category III codes.
| CPT Code | Description |
|---|---|
| 64999 | Unlisted procedure, nervous system (pulsed RFA, cooled RFA — verify with payer) |
Category 5: Spinal Cord Stimulation (SCS)
Spinal cord stimulation involves implanting electrodes in the epidural space connected to a pulse generator. The coding distinguishes between trials and permanent implants, and between one or more leads.
SCS Trial (Temporary)
Trial procedures for spinal cord stimulation involve temporary electrode placement and associated device analysis, which are reported using specific CPT codes.
| CPT Code | Description |
|---|---|
| 63650 | Percutaneous implantation, neurostimulator electrode array, epidural |
| 63655 | Laminectomy for implantation of neurostimulator electrodes, plate/paddle lead |
| 63661 | Removal of spinal neurostimulator electrode percutaneous array(s) |
| 63662 | Removal of spinal neurostimulator electrode plate/paddle lead(s) |
| 95970 | Electronic analysis of implanted neurostimulator pulse generator — without reprogramming |
| 95971 | Electronic analysis — simple spinal cord stimulator with reprogramming |
| 95972 | Electronic analysis — complex spinal cord stimulator with reprogramming |
SCS Permanent Implant
Permanent spinal cord stimulation implantation codes are used after a successful trial and include insertion, revision, or removal of the pulse generator and electrode arrays.
| CPT Code | Description |
|---|---|
| 63685 | Insertion or replacement of spinal neurostimulator pulse generator or receiver |
| 63688 | Revision or removal of implanted spinal neurostimulator pulse generator or receiver |
| 63663 | Revision of percutaneous electrode array |
| 63664 | Revision of plate/paddle electrode array |
NOTE: Typically, a 7-10 day trial period precedes permanent implantation. Insurer pre-authorization is mandatory, and failure rate thresholds (e.g., ≥50% pain relief) apply.
Category 6: Intrathecal Drug Delivery Systems
Intrathecal Drug Delivery System procedures are coded based on catheter placement, pump implantation or replacement, removal, and ongoing pump analysis and management functions.
| CPT Code | Description |
|---|---|
| 62350 | Implantation, revision, or repositioning of tunneled intrathecal or epidural catheter | 62351 | Implantation, revision including placement of catheter — not tunneled |
| 62355 | Removal of previously implanted intrathecal or epidural catheter |
| 62360 | Implantation or replacement of device for intrathecal or epidural drug infusion — programmable pump |
| 62361 | Implantation or replacement — non-programmable pump |
| 62362 | Implantation or replacement — programmable pump, including preparation of pump |
| 62365 | Removal of subcutaneous reservoir or programmable pump |
| 62367 | Electronic analysis of programmable, implanted pump — without reprogramming |
| 62368 | Electronic analysis — with reprogramming |
| 62369 | Electronic analysis — with reprogramming and refill |
| 62370 | Electronic analysis — with reprogramming, refill, and substantial revision |
Category 7: Fluoroscopy & Imaging Guidance
Fluoroscopy guidance for pain procedures is often bundled into the primary procedure code. The following are only separately billable when NOT already included in the procedure code.
| CPT Code | Description | Bundled With |
|---|---|---|
| 77002 | Fluoroscopic guidance, needle placement | Various injection codes |
| 77003 | Fluoroscopic guidance, needle placement for spine/paraspinal injections | Bundled into 62321, 62323, 64483, 64633–64636 |
| 76942 | Ultrasound guidance, needle placement — with imaging documentation | NOT bundled with 20604, 20606, 20611 |
| 77012 | CT guidance for needle placement | Specific CT-guided procedures |
| 77021 | MRI guidance for needle placement | MRI-guided procedures |
NOTE: Billing 77003 alongside 62321, 62323, or the transforaminal ESI codes (64479–64484) is a common claim error that results in denials. Always check bundling edits using the CMS NCCI (National Correct Coding Initiative) tables.
Category 8: Physical Medicine & Psychological Services
Physical Medicine and Psychological Services codes are used to report rehabilitative therapies and behavioral health interventions that support chronic pain management through functional restoration and psychological evaluation.
Physical Medicine (PM&R) Add-Ons
Physical Medicine & Rehabilitation add-on codes are used to bill time-based therapeutic modalities and exercise-based treatments delivered during pain rehabilitation programs.
| CPT Code | Description |
|---|---|
| 97010 | Hot/cold packs application |
| 97012 | Mechanical traction |
| 97014 | Electrical stimulation — unattended |
| 97018 | Paraffin bath |
| 97022 | Whirlpool |
| 97024 | Diathermy |
| 97026 | Infrared therapy |
| 97032 | Electrical stimulation — attended, each 15 min |
| 97035 | Ultrasound, each 15 min |
| 97110 | Therapeutic exercises, each 15 min |
| 97112 | Neuromuscular reeducation, each 15 min |
| 97530 | Therapeutic activities, each 15 min |
Psychological / Behavioral Health Codes
Chronic pain involves significant psychological components. Pain psychologists and behavioral health providers use the following codes in integrated pain programs.
| CPT Code | Description |
|---|---|
| 90791 | Psychiatric diagnostic evaluation |
| 90834 | Individual psychotherapy, 45 min |
| 90837 | Individual psychotherapy, 60 min |
| 90853 | Group psychotherapy |
| 96130 | Psychological testing evaluation, first hour |
| 96131 | Psychological testing evaluation, each additional hour |
| 97151 | Behavior identification assessment |
| 97153 | Adaptive behavior treatment, individual — each 15 min |
Which are the Key Modifiers in Pain Management?
Modifiers clarify the circumstances of a procedure and are essential for accurate reimbursement and avoiding inappropriate bundling edits.
| Modifier | Description | When to Use |
|---|---|---|
| LT | Left side | Unilateral procedure on the left |
| RT | Right side | Unilateral procedure on the right |
| 50 | Bilateral procedure | Same procedure both sides, same session |
| 59 | Distinct procedural service | Separate, independent procedure — prevents bundling |
| XU | Unusual non-overlapping service | Subset of 59 — preferred for NCCI unbundling |
| 25 | Separate E&M same day as procedure | E&M visit is separate and medically necessary |
| 51 | Multiple procedures | Second and subsequent procedures, same session |
| 52 | Reduced services | Procedure partially reduced — adjust fee |
| 53 | Discontinued procedure | Procedure started but stopped (complication/circumstance) |
| 76 | Repeat procedure, same physician | Same procedure repeated same day — document why |
| 77 | Repeat procedure, different physician | Same procedure repeated by different provider |
| AS | PA/NP/CNS assistant at surgery | Mid-level provider assists at procedure |
| GC | Resident under teaching supervision | Teaching physician attestation required |
| TC | Technical component only | Equipment/staff component billed separately |
| 26 | Professional component only | Physician interpretation billed separately |
What are the Common ICD-10 Diagnosis Code Pairings?
Accurate ICD-10 diagnosis codes must support medical necessity for every pain management CPT code. Below are common diagnosis-to-procedure pairings.
Spinal Pain Diagnoses
| ICD-10 Code | Description | Commonly Linked CPT |
|---|---|---|
| M54.50 | Low back pain, unspecified | 62322, 62323, 64493–64495 |
| M54.51 | Vertebrogenic low back pain | 62322, 62323, 64493–64495 |
| M54.59 | Other low back pain | 62322, 62323 |
| M54.2 | Cervicalgia | 62320, 62321, 64490–64492 |
| M54.12 | Radiculopathy, cervical region | 64479, 64480 |
| M54.16 | Radiculopathy, lumbar region | 64483, 64484 |
| M54.17 | Radiculopathy, lumbosacral region | 64483, 64484, 62322, 62323 |
| M47.816 | Spondylosis with radiculopathy, lumbar | 64483, 64484, 64635, 64636 |
| M47.812 | Spondylosis with radiculopathy, cervical | 64479, 64480, 64633, 64634 |
| M51.16 | Intervertebral disc degeneration, lumbar | 62322, 62323, 64635 |
| M48.06 | Spinal stenosis, lumbar region | 62322, 62323 |
Other Pain Diagnoses
| ICD-10 Code | Description | Commonly Linked CPT |
|---|---|---|
| G89.29 | Other chronic pain | Multiple — general pain management |
| G89.21 | Chronic pain due to trauma | 64450, nerve blocks |
| G89.3 | Neoplasm-related pain | Celiac plexus, intrathecal pump |
| G90.511 | CRPS type I, right upper extremity | 64510, 64520, SCS |
| G90.521 | CRPS type I, right lower extremity | 64520, SCS |
| M79.7 | Fibromyalgia | 20552, 20553, TPIs |
| G43.909 | Migraine, unspecified | 64405 occipital block |
| M53.3 | Sacrococcygeal disorders | 27096 SI joint injection |
| M47.896 | Spondylosis without myelopathy — lumbar | 64635, 64636 |
| R52 | Pain, unspecified | Use only when a more specific code is unavailable |
NOTE: Always use the most specific ICD-10 code available. Unspecified codes (e.g., R52, M54.50) may trigger medical necessity reviews or prior authorization requirements.
What are the Prior Authorization & Documentation Requirements for Pain Management Procedures?
Prior authorization is a critical step in pain management billing. This is because many interventional procedures require payer approval and strict clinical documentation to establish medical necessity before treatment is performed.
Procedures Typically Requiring Prior Authorization
The following pain management procedures commonly require prior authorization from Medicare Advantage and commercial insurance plans:
- Spinal cord stimulator trials and implants (63650, 63685)
- Intrathecal drug delivery system implantation (62360–62362)
- Radiofrequency ablation (64633–64636)
- Transforaminal epidural steroid injections — many commercial payers
- Celiac plexus block (64530)
- Sympathetic nerve blocks for CRPS
Essential Documentation Elements
To support medical necessity and avoid claim denials, the following documentation must be clearly included in the medical record:
Chief complaint and pain history with duration, character, and severity (NRS/VAS scale)
- Previous treatments tried and failed (conservative care first — physical therapy, medications)
- Physical examination findings with neurological assessment
- Review of imaging studies (MRI/CT correlating with clinical findings)
- Informed consent signed prior to the procedure
- Procedure note describing approach, image guidance, medications injected, and patient response
- Post-procedure assessment and follow-up plan
- For RFA: documentation of two prior positive diagnostic medial branch blocks
- For SCS: psychological clearance and trial period results
Frequency Limitations
To ensure compliance with payer policies, most pain management procedures are subject to specific frequency limits based on Medicare and commercial insurance guidelines.
| Procedure | Typical Medicare Limitation | Notes |
|---|---|---|
| Epidural Steroid Injection | 3 per spinal region per year | Some payers allow up to 6 total |
| Facet Joint Injections | 3 per spinal region per year | Same-level limit applies |
| Medial Branch Blocks (Diagnostic) | 2 per level before RFA | Must show ≥50–80% relief |
| Radiofrequency Ablation | Once per level per year | May repeat if pain returns |
| Trigger Point Injections | 3 per muscle group per day | Up to 5 sessions per year (varies) |
| SI Joint Injection | 3 per year | Payer-specific |
NOTE: Frequency limitations vary significantly by payer. Always verify current coverage policies with individual commercial insurers and consult the CMS National Coverage Determinations (NCDs) for Medicare.
Billing Best Practices & Compliance
Pain management billing must follow established coding guidelines, payer policies, and federal regulations to ensure accurate reimbursement and regulatory compliance.
Top Billing Errors to Avoid
The following are common billing mistakes that frequently lead to claim denials or compliance audits:
- Unbundling imaging guidance (77003) from procedures where it is already included (62321, 62323, 64483–64484, 64633–64636)
- Billing E&M on the same day as a procedure without Modifier 25 (and without documenting a separately identifiable service)
- Using unspecified ICD-10 codes when a specific code is available
- Failing to document medical necessity for repeat procedures
- Billing bilateral procedures without Modifier 50 or LT/RT modifiers
- Incorrect procedure level. For example, documenting cervical when the procedure was lumbar
- Billing 64490–64495 incorrectly for medial branch blocks or intra-articular facet injections can lead to denials or audits, so documentation must clearly specify the exact procedure performed.
NCCI Edits & Bundling
The CMS National Correct Coding Initiative (NCCI) establishes pairs of codes that cannot be billed together without meeting specific criteria. Always check NCCI edits before submitting claims with multiple procedure codes on the same date.
- Check CMS NCCI tables at: www.cms.gov/medicare/coding-billing/national-correct-coding-initiative-edits
- Modifier 59 or XU may override some bundling edits. Use only when the procedures were truly separate and distinct
- Column 1 / Column 2 edits: Column 2 code is bundled into Column 1 and may not be billed separately
Compliance Tips
To maintain regulatory compliance and avoid legal risk, the following standards must always be followed:
- Review annual CPT updates to ensure all pain management codes reflect the latest AMA and payer changes.
- Always support every CPT code with clear medical necessity and linked ICD-10 diagnosis codes.
- Do not unbundle imaging guidance codes that are already included in procedure CPT codes.
- Use modifiers (25, 50, LT/RT, 59, XU) only when clinically justified and fully documented.
- Verify prior authorization requirements before performing high-cost interventional pain procedures.
- Track and follow payer-specific frequency limitations for injections, blocks, and RFA procedures.
- Cross-check all claims with CMS NCCI edits before submission to avoid bundling errors.
- Maintain HIPAA compliance by protecting all patient health information during billing processes.
- Perform regular internal audits to identify and correct coding, modifier, and documentation errors
FAQS
What is the Difference Between a New Patient and an Established Patient for E&M Coding Purposes?
A new patient is someone who has not received any professional services from the same physician or another physician in the same group within the past 3 years, while an established patient has had at least one professional service from the same provider or group within that timeframe.
Which is the Best Pain Management Billing Company in the United States?
Transcure is the best pain management billing company in the U.S, known for its deep expertise in CPT and ICD-10 coding for all pain management procedures. They use dedicated AI agents to automate every step of the billing process, resulting in 99.99% clean claim accuracy and near-zero claim denial rates.
What are NCCI Edits, and how do they Impact Pain Billing?
NCCI (National Correct Coding Initiative) edits are CMS rules that prevent improper coding combinations. In pain management, they often bundle services like imaging guidance or certain injections. This means some codes cannot be billed together unless appropriate modifiers (like 59 or XU) are used with strong documentation.
What are Common Reasons for Claim Denials in Pain Practices?
Common claim denials in pain management practices occur due to a lack of medical necessity documentation, missing prior authorization, and incorrect CPT/ICD-10 code pairing. Other frequent issues include unbundling of services, incorrect or missing modifiers, insufficient documentation of procedures, and exceeding payer-defined frequency limits for injections or interventions.
What are Payer-Specific Variations in Pain Management Coding Rules?
Payer-specific variations refer to differences in coverage policies, frequency limits, prior authorization requirements, modifier acceptance, and medical necessity criteria between Medicare, Medicaid, and commercial insurers. For example, one payer may allow more epidural injections per year, while another may strictly limit them or require additional documentation before approval.
How are Standardized Codes Used to Report Healthcare Services?
Medical offices utilize CPT codes in medical billing to communicate the specific treatments, diagnostic tests, and evaluation services provided to patients. These five-digit codes ensure that insurance companies understand exactly what was performed, allowing for accurate payment and consistent tracking of clinical procedures across the healthcare system.