")
Hematuria, the presence of blood in urine, is one of the most frequently encountered clinical findings in outpatient medicine. It also ranks among the most reliably miscoded diagnoses in nephrology, urology, and primary care billing.
The ICD-10 hematuria framework spans two separate code families: the R31 series for symptom-only encounters, and the N02 series for recurrent hematuria tied to glomerular disease. Each carries hard exclusion rules that payer scrubbers enforce automatically.
This guide covers every billable ICD-10 hematuria code, when each applies, the documentation each requires, and the most common denial patterns. It also covers nephrology-specific hematuria coding, sequencing rules, and CPT pairings.
1. What Is the ICD-10 Code for Hematuria?
The default ICD-10 code for hematuria is R31.9 — Hematuria, unspecified. It is a billable, symptom-level code used when blood in urine is documented without a confirmed cause.
R31.9 sits within the parent category R31 (Hematuria), under Chapter 18 of ICD-10-CM. Use it only when hematuria is the reason for the encounter and no definitive diagnosis has been established at the time of coding.
R31.9 is frequently the wrong code. The R31 family contains five billable subcodes that distinguish gross from microscopic hematuria. Defaulting to R31.9 when more specific codes apply is a coding quality issue.
Note: R31.x codes apply only to symptom-only encounters. Once a provider documents a confirmed cause such as cystitis, glomerulonephritis, nephrolithiasis, or a bladder tumor, the condition’s code takes over. Hematuria is not separately coded unless it carries clinical significance beyond what the primary code captures.
2. Complete Hematuria ICD-10 Code Table — 2026 Edition
Here is the complete Hematuria ICD-10 code table for the 2026 edition, including both symptom-based R31 codes and cause-specific codes used when an underlying condition is confirmed.
The R31 Code Family: Hematuria Without a Confirmed Cause
Use R31 codes when hematuria is the primary reason for the encounter and no underlying diagnosis has been established. The 2026 ICD-10-CM edition retains all R31 subcodes from the prior edition.
| Code | Description | When to Use | Billable |
|---|---|---|---|
| R31 | Hematuria — parent category | Header code only; do not bill directly | No |
| R31.0 | Gross hematuria | Blood visible to the eye; pink, red, or cola-colored urine; no confirmed underlying cause | Yes |
| R31.1 | Benign essential microscopic hematuria | Microscopic RBCs on UA; no pathological cause after workup; explicitly described as benign | Yes |
| R31.21 | Asymptomatic microscopic hematuria | Microscopic blood found on routine UA; patient has no related symptoms | Yes |
| R31.29 | Other microscopic hematuria | Symptomatic microscopic hematuria not fitting R31.1 or R31.21 | Yes |
| R31.9 | Hematuria, unspecified | Hematuria documented without specifying gross vs. microscopic and no cause confirmed | Yes |
Cause-Linked Hematuria Codes: When R31 Does Not Apply
When a physician documents a confirmed condition as the cause of hematuria, the code shifts out of R31. The R31 parent category carries an Excludes1 note for these codes.
Excludes1 means the codes cannot appear on the same claim for the same condition. These exclusions trigger the most common denials in hematuria billing.
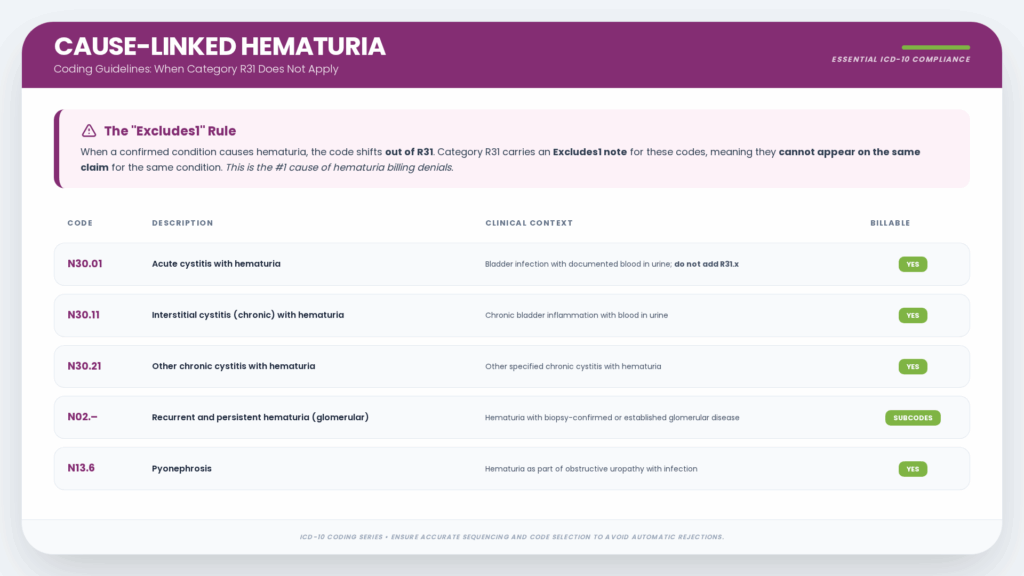
| Code | Description | Clinical Context | Billable |
|---|---|---|---|
| N30.01 | Acute cystitis with hematuria | Bladder infection with documented blood in urine; do not add R31.x | Yes |
| N30.11 | Interstitial cystitis (chronic) with hematuria | Chronic bladder inflammation with blood in urine | Yes |
| N30.21 | Other chronic cystitis with hematuria | Other specified chronic cystitis with hematuria | Yes |
| N02.- | Recurrent and persistent hematuria (glomerular) | Hematuria with biopsy-confirmed or established glomerular disease | Subcodes |
| N13.6 | Pyonephrosis | Hematuria as part of obstructive uropathy with infection | Yes |
3. The N02 Series: Recurrent and Persistent Hematuria in Glomerular Diseases
The N02 code family covers recurrent and persistent hematuria associated with glomerular disease. These codes require that hematuria be recurrent or persistent, not a single acute episode.
Billing teams that default to R31.9 when a nephrologist documents glomerular disease violate the ICD-10-CM Excludes1 rule. The result is preventable denials and audit risk.
N02 Numeric Subcodes — Morphological Patterns
| Code | Description | Glomerular Pattern |
|---|---|---|
| N02.0 | Recurrent and persistent hematuria with minor glomerular abnormality | Minimal change pattern on biopsy |
| N02.1 | Recurrent and persistent hematuria with focal and segmental glomerular lesions | FSGS pattern; focal scarring with segmental sclerosis |
| N02.2 | Recurrent and persistent hematuria with diffuse membranous glomerulonephritis | Membranous nephropathy; subepithelial deposits on EM |
| N02.3 | Recurrent and persistent hematuria with diffuse mesangial proliferative GN | Mesangial hypercellularity without IgA deposits |
| N02.4 | Recurrent and persistent hematuria with diffuse endocapillary proliferative GN | Post-infectious GN pattern with neutrophils |
| N02.5 | Recurrent and persistent hematuria with diffuse mesangiocapillary GN | MPGN Type I/III; double-contour GBM |
| N02.6 | Recurrent and persistent hematuria with dense deposit disease | MPGN Type II / C3 glomerulopathy with intramembranous deposits |
| N02.7 | Recurrent and persistent hematuria with diffuse crescentic GN | Rapidly progressive GN; crescents in over 50% of glomeruli |
| N02.8 | Recurrent and persistent hematuria with other morphologic changes | Other specified glomerular changes |
| N02.9 | Recurrent and persistent hematuria with unspecified morphologic changes | Glomerular disease confirmed but morphology not specified |
| N02.A | Recurrent and persistent hematuria with C3 glomerulonephritis | Dominant C3 deposits with absent or trace Ig on IF |
N02.B Subcodes — IgA Nephropathy (Berger’s Disease)
N02.B is the parent code for IgA nephropathy and is non-billable. Use the appropriate subcode based on the morphological pattern documented on the biopsy.
The 2026 ICD-10-CM edition includes seven N02.B subcodes that capture the full range of IgA nephropathy patterns. Each requires biopsy confirmation showing IgA mesangial deposits on immunofluorescence.
| Code | Description | Pattern |
|---|---|---|
| N02.B | Recurrent and persistent IgA nephropathy — parent | Parent category; not billable |
| N02.B1 | IgA nephropathy with glomerular lesion | Glomerular lesion with IgA deposits, pattern not otherwise specified |
| N02.B2 | IgA nephropathy with focal and segmental glomerular lesion | FSGS-pattern lesions with IgA deposits on IF |
| N02.B3 | IgA nephropathy with diffuse membranoproliferative GN | MPGN-type pattern with IgA deposits |
| N02.B4 | IgA nephropathy with diffuse membranous GN | Membranous pattern with IgA deposits |
| N02.B5 | IgA nephropathy with diffuse mesangial proliferative GN | Most common IgA pattern; mesangial hypercellularity with IgA deposits |
| N02.B6 | IgA nephropathy with diffuse mesangiocapillary GN | Mesangiocapillary pattern with IgA deposits |
| N02.B9 | Other recurrent and persistent IgA nephropathy | Other specified IgA nephropathy patterns |
4. Gross Hematuria vs. Microscopic Hematuria
The gross-versus-microscopic distinction determines which ICD-10 code is correct. The chart must explicitly support the selection through physician documentation, not just lab values alone.
Many coders default to R31.9 when the physician writes “hematuria” without qualification. In most cases, the urinalysis result and provider notes give enough information to support a more specific code.
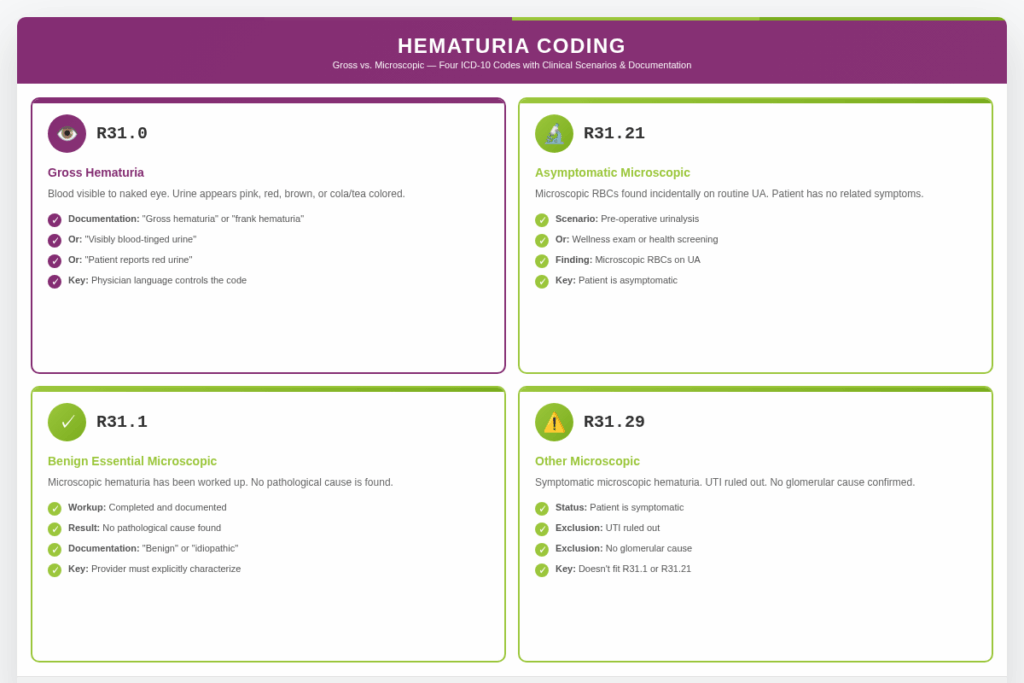
Gross Hematuria — R31.0
Gross hematuria means blood is visible to the naked eye. The urine appears pink, red, brown, or the cola/tea color associated with glomerular bleeding.
Documentation supporting R31.0 should include explicit terms: “gross hematuria,” “frank hematuria,” “visibly blood-tinged urine,” or “patient reports red urine.” Physician language controls the code.
Asymptomatic Microscopic Hematuria — R31.21
R31.21 captures microscopic blood found incidentally on routine UA. Common scenarios include pre-operative urinalysis, wellness exam, UA, or health screening.
The chart must show microscopic RBCs on UA, provider acknowledgment of the finding, and documentation that the patient has no related symptoms. Do not use R31.9 when R31.21 is supported.
Benign Essential Microscopic Hematuria — R31.1
R31.1 applies when microscopic hematuria has been worked up, and no pathological cause is found. The provider must explicitly characterize the finding as benign or idiopathic.
Other Microscopic Hematuria — R31.29
R31.29 covers symptomatic microscopic hematuria ICD-10 that does not fit R31.1 or R31.21. Use it when the patient is symptomatic, UTI is ruled out, and no glomerular cause is confirmed.
5. Excludes 1 Notes — The Rule That Drives Most Denials
ICD-10-CM Excludes1 notes are non-negotiable for hematuria billing. The R31 parent category carries an Excludes1 note that is one of the most frequently violated coding rules.
Violating Excludes1 does not result in a payer letter. It results in an automated claim rejection from the scrubber before the claim reaches the payer.
Excludes1 vs. Excludes2
| Note Type | What It Means | Both Codes Together? |
|---|---|---|
| Excludes1 | The excluded condition cannot coexist with this code by definition. ICD-10-CM language: “Not coded here.” | Never |
| Excludes2 | The excluded condition is not included in this code, but the patient can have both. ICD-10-CM language: “Not included here.” | Yes, if both documented |
What the Excludes1 Note Under R31 Excludes
The Excludes1 note under R31 specifically excludes hematuria included with underlying conditions. The cited examples are:
- N30.01 — ICD-10 code for acute cystitis with hematuria
- N02.- (all subcodes) — Recurrent and persistent hematuria in glomerular diseases
- Other “with hematuria” codes — N30.11, N30.21, and similar combination codes follow the same principle
These codes already contain hematuria within their description. Coding R31.x alongside them is redundant at best and a hard edit violation at worst.
COMMON DENIAL SCENARIO
A biller receives a chart showing “acute cystitis with gross hematuria.” The biller codes N30.01 plus R31.0, reasoning that both findings are documented. The scrubber rejects: Excludes1 violation. The fix is N30.01 alone, which captures both the cystitis and the hematuria.
6. Code Sequencing Rules
Selecting the right code is half the work. Sequencing it correctly is the other half. Sequencing errors are among the most common compliance risks in hematuria billing.
Outpatient and inpatient settings follow different rules. Nephrology practices operating in both environments must apply the correct standard to each claim.
Outpatient Sequencing Rules
In outpatient settings, the first-listed diagnosis is the condition chiefly responsible for services during the encounter. Follow ICD-10-CM Section IV guidelines.
- If the patient presents because of hematuria and no diagnosis is established, R31.x is first-listed.
- If a definitive diagnosis is confirmed, code that condition first. Add R31.x only if it is a clinically significant finding not already captured.
- Symptoms integral to a confirmed diagnosis are not separately coded per Section IV.J.
Inpatient Sequencing Rules
In inpatient settings, the principal diagnosis is the condition established after study to be chiefly responsible for the admission. The UHDDS definition governs.
- If a patient is admitted for hematuria workup and IgA nephropathy is confirmed during admission, the principal diagnosis at discharge is the appropriate N02.B subcode, not R31.9.
- If the workup is inconclusive at discharge, R31.x remains the principal diagnosis.
- Comorbidities affecting management or resource use are coded as additional diagnoses.
When Hematuria Is Coded as an Additional Diagnosis
Hematuria is appropriately coded alongside a primary diagnosis in three scenarios:
- The patient has CKD (N18.x) primary, and a new hematuria episode requires separate evaluation, not captured by the CKD code.
- The primary encounter is a procedure (e.g., cystoscopy), and hematuria is the indication coded additionally for medical necessity.
- Hematuria is a procedure or medication complication that is separately documented and managed.
7. Documentation Requirements for Each Hematuria Code
Documentation determines whether a hematuria claim survives a payer audit. Each code family has specific requirements that must be present at the time of claim submission.
The checklists below reflect what payers and MACs look for across each major hematuria code type. Documentation cannot be added retroactively after a denial.

R31.0 — Gross Hematuria
- Physician statement explicitly noting visible blood in urine — “gross hematuria,” “frank hematuria,” or “red/pink urine.”
- Urinalysis results in the chart showing a supportive RBC count
- Confirmation that no underlying cause was established during the encounter
- Patient’s presenting complaint documented (e.g., “red urine for 3 days”)
- Workup ordered or imaging performed, even if results are pending
- Provider signature with date and time of service
R31.21 — Asymptomatic Microscopic Hematuria
- Urinalysis showing microscopic RBCs, present in the chart and referenced in the note.
- Physician documentation that the finding was incidental
- Explicit documentation that the patient is asymptomatic
- No related symptoms (dysuria, flank pain, frequency, urgency) attributable to hematuria
- No confirmed underlying cause for the microscopic RBCs
- Encounter context noted (e.g., “routine annual exam,” “pre-operative UA”)
R31.1 — Benign Essential Microscopic Hematuria
- Urinalysis showing microscopic RBCs documented in the chart
- Documentation of a completed evaluation that failed to identify a pathological cause
- Physician explicitly characterizing the hematuria as benign or idiopathic
- Monitoring plan documented (e.g., “repeat UA in 6 months”)
- Exclusion of UTI, malignancy, stones, and glomerular disease in the assessment
N02.x Subcodes — Glomerular Disease
- Physician documentation of recurrent or persistent hematuria, not a single isolated episode
- Established or confirmed glomerular disease diagnosis
- For morphology-specific subcodes: biopsy report identifying the morphological pattern
- Immunofluorescence findings, particularly for IgA nephropathy (IgA deposits) and C3 GN
- Electron microscopy findings for N02.2 and N02.6 were relevant
- Serial urinalyses showing persistent RBCs to establish the recurrent and persistent criterion
- Nephrologist or specialist provider’s signature on the encounter note
8. Hematuria in Nephrology Patients
Hematuria in a nephrology practice is a different clinical and coding problem than hematuria in primary care. The cause is typically a glomerular process, and the appropriate code is rarely R31.9.
Compliance risk and DRG reimbursement stakes are higher for nephrology hematuria coding than for symptom-level encounters in other settings. Nephrology practices often rely on specialized support such as nephrology billing services to ensure accurate application of N02 and R31 coding rules and reduce denial risk.
IgA Nephropathy — The Most Commonly Miscoded Glomerular Disease
IgA nephropathy (Berger’s disease) is the most common primary glomerulonephritis worldwide. Hallmark presentations include recurrent gross hematuria after upper respiratory infections or persistent microscopic hematuria.
When a nephrologist documents recurrent hematuria with IgA nephropathy, the appropriate code is from the N02.B subcode series based on biopsy morphology. R31.9 in this context violates Excludes1.
| Clinical Documentation | Correct Code | Wrong Code |
|---|---|---|
| IgA nephropathy, biopsy-confirmed mesangial proliferative pattern, recurrent hematuria | N02.B5 | R31.9 |
| IgA nephropathy, FSGS pattern on biopsy, recurrent hematuria | N02.B2 | R31.9 |
| C3 glomerulonephritis (dominant C3, absent Ig on IF), recurrent hematuria | N02.A | R31.9 |
| Rapidly progressive crescentic GN with gross hematuria | N02.7 | R31.0 |
| Glomerular disease confirmed clinically, biopsy pending, recurrent hematuria | N02.9 | R31.9 |
Hematuria in CKD Patients
When an established CKD patient presents with hematuria, the coding decision tree follows this logic:
- If hematuria is from the glomerular disease causing the CKD, use the appropriate N02 code, and add the CKD stage code (N18.x) as an additional code. Do not add R31.x.
- If CKD is from a non-glomerular cause and hematuria is a separate new finding: code CKD primary, add R31.x as additional if separately evaluated.
- If hematuria is from a separate genitourinary condition (e.g., bladder lesion): code CKD, code the GU condition, do not add R31.x unless clinically significant.
Hematuria in ESRD Patients on Dialysis
For ESRD patients (N18.6), hematuria can arise from the glomerular disease, vascular access complications, or new urological findings. N18.6 does not capture hematuria.
- If from underlying glomerular disease: N18.6 plus the appropriate N02 code
- If from a new urological finding: N18.6 plus the appropriate bladder or urological code
- If undetermined after the encounter: N18.6 plus R31.x as appropriate
Thin Basement Membrane Disease
Thin basement membrane disease (TBMD), also called benign familial hematuria, is hereditary and causes persistent microscopic hematuria with a benign prognosis.
Electron microscopy shows diffuse thinning of the glomerular basement membrane (less than 250 nm). Coding combines a hereditary nephritis code with R31.1 (benign essential microscopic hematuria) when supported by documentation.
9. CPT Codes Commonly Paired with Hematuria
ICD-10 codes establish medical necessity for every CPT code billed in the same encounter. When a CPT code lacks a matching ICD-10 diagnosis, the claim fails medical necessity review.
The CPT codes below are frequently billed alongside hematuria diagnoses. The ICD-10 selection affects whether the claim clears first-pass review.
| CPT Code | Description | ICD-10 Pairing Notes |
|---|---|---|
| 81001 / 81003 | Urinalysis, with or without microscopy | Any R31.x code provides strong medical necessity support |
| 52000 | Cystourethroscopy (cystoscopy) | R31.0 strongly supported under AUA guidelines; R31.21/R31.29 with risk factors |
| 50200 | Renal biopsy, percutaneous | Pair with N02.9 or specific N02 subcode if established pre-biopsy |
| 74177 / 74178 | CT abdomen and pelvis | R31.0 standard for upper-tract hematuria workup |
| 99213-99215 | Office E&M, established patient | Pair with the most specific hematuria diagnosis supported |
CPT-ICD-10 PAIRING TIP
If R31.x is listed as the indication for renal biopsy and the biopsy confirms glomerular disease, update the diagnosis to the appropriate N02 subcode on the final claim. Leaving R31.9 as the diagnosis after glomerular disease is confirmed is a common documentation gap.
For detailed information on nephrology CPT codes, refer to this guide for a complete breakdown of coding rules, common pairings, and billing applications.
10. Medicare and Payer-Specific Billing Rules
Medicare payment rules for hematuria are governed by MS-DRG assignment for inpatient claims and Local Coverage Determinations for outpatient procedures. Both vary based on the specific code chosen.
DRG differences between R31.x and N02.x codes can produce material reimbursement variation for inpatient encounters. Accurate coding is both a compliance and revenue issue. Many providers also collaborate with experienced nephrology billing companies to manage DRG assignment, LCD compliance, and payer-specific hematuria billing requirements.
MS-DRG Implications
| DRG | Description | Mapped Codes | MCC/CC? |
|---|---|---|---|
| 695 | Kidney and urinary tract signs and symptoms with MCC | R31.x with major complication or comorbidity | MCC |
| 696 | Kidney and urinary tract signs and symptoms without MCC | R31.x without MCC | No |
| 698 | Other kidney and urinary tract diagnoses with MCC | N02.x with MCC | MCC |
| 699 | Other kidney and urinary tract diagnoses with CC | N02.x with CC | CC |
| 700 | Other kidney and urinary tract diagnoses without CC/MCC | N02.x without CC or MCC | No |
A patient admitted with confirmed IgA nephropathy and recurrent hematuria should code to the appropriate N02.B subcode, grouping into DRG 698/699/700, rather than R31.9 in DRG 695/696.
LCD Coverage for Hematuria Workup
- Gross hematuria (R31.0) is universally accepted for cystoscopy across all major MACs.
- Asymptomatic microscopic hematuria (R31.21) supports cystoscopy when AUA risk factors are documented.
- Some MACs require repeat UA confirmation before cystoscopy coverage is triggered for R31.21 or R31.29.
- Renal biopsy LCDs consistently list recurrent glomerular hematuria (N02.x) as a covered indication.
R31.9 as a Payer Audit Trigger
Commercial payers and MACs flag high-frequency R31.9 use in nephrology and urology practices. A practice that bills N02 codes for some patients while billing R31.9 for clinically similar encounters creates an inconsistency that triggers analytics flags.
The fix is not to stop using R31.9. The fix is to confirm that every R31.9 claim is genuinely supported by documentation showing no confirmed cause and no more specific code available. Quarterly self-audits address the pattern.
11. Top Hematuria ICD-10 Claim Denial Reasons
Six denial patterns account for the majority of preventable hematuria billing losses across nephrology and urology practices. Each has a specific root cause and a clear fix.
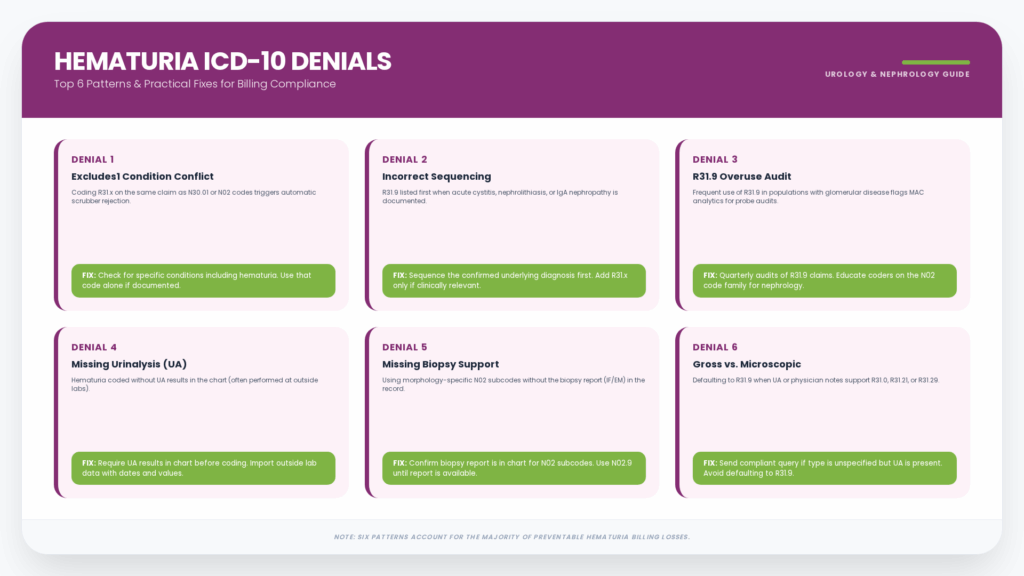
Denial 1: R31.x Coded with an Excludes1 Condition
The biller codes R31.9 or R31.0 on the same claim as N30.01 or an N02 code. The scrubber rejects automatically with no manual review.
Fix: Before selecting R31.x, check whether the chart documents a specific condition that includes hematuria. If so, use that condition code alone.
Denial 2: Hematuria Sequenced First with Definitive Diagnosis
R31.9 appears as first-listed when the assessment documents acute cystitis, nephrolithiasis, or IgA nephropathy. The payer flags the sequencing error on the claims data audit.
Fix: Code the confirmed underlying diagnosis as first-listed. Add R31.x only if it provides clinically relevant information not captured by the primary code.
Denial 3: R31.9 Overuse Flagged on Payer Audit
A nephrology practice bills R31.9 for most hematuria encounters across a population that includes documented glomerular disease patients. MAC analytics initiates a probe audit.
Fix: Conduct a quarterly coding audit of all hematuria claims. Review every R31.9 claim from a nephrology provider. Implement coder education on the N02 code family.
Denial 4: Missing Urinalysis Documentation
Hematuria is coded, but the UA result is absent from the chart. The result was performed at an outside lab or referenced verbally without the actual values.
Fix: Require UA results to be in the chart before hematuria is coded. If results are from an outside lab, import or document them with date and values in the encounter note.
Denial 5: N02 Morphology Subcode Without Biopsy in Chart
The coder selects an N02.B subcode based on the physician’s diagnosis, but the biopsy report is not in the chart. The audit cannot support specificity.
Fix: For morphology-specific N02 subcodes, confirm that the biopsy report with IF and EM findings is in the chart. If a biopsy is not available, use N02.9 until the report is imported.
Denial 6: Gross vs. Microscopic Not Specified
The coder defaults to R31.9 across encounters where chart data (UA results, physician language) would support R31.0, R31.21, or R31.29.
Fix: When the physician documents “hematuria” without specifying gross vs. microscopic and the UA is in the chart, send a compliant coder query before defaulting to R31.9.
13. Frequently Asked Questions
What is the ICD-10 Code for Hematuria?
The most commonly used code is R31.9 — Hematuria, unspecified. However, R31.9 is only correct when no underlying cause is documented, and neither gross nor microscopic type is specified.
More accurate codes include R31.0 (gross hematuria), R31.21 (asymptomatic microscopic), and R31.29 (other microscopic). When linked to glomerular disease, the N02 family applies instead.
What is the Difference Between R31.0 and R31.9?
ICD-10 code for gross hematuria IS R31.0 (visible blood: red, pink, or cola-colored urine). R31.9 is for hematuria documented without specifying the type. Always select the more specific code when documentation supports it.
Can I Code R31.9 and N30.01 on the Same Claim?
No. This combination violates the Excludes1 note under R31. N30.01 (acute cystitis with hematuria, ICD-10) already captures the hematuria. The combination generates an automated claim edit.
What ICD-10 Code is Used for Microscopic Hematuria?
Three R31 codes cover microscopic hematuria. R31.21 applies when incidental and asymptomatic. R31.1 applies when evaluated and characterized as benign. R31.29 applies when symptomatic or not fitting either category.
How does a Nephrologist Code Recurrent Hematuria with IgA Nephropathy?
The correct code is from the N02.B subcode series based on biopsy morphology. The most common pattern (diffuse mesangial proliferative) maps to N02.B5. R31.9 violates Excludes1 in this context.
Is Hematuria Always Coded Separately from the Underlying Condition?
No, when hematuria is a symptom of a documented condition, it is generally not coded separately. Hematuria is coded separately only when it is the primary reason for the encounter without a confirmed cause, when it adds clinical information not captured by the primary code, or when it is a complication.
What ICD-10 Code is Used for Hematuria in a CKD Patient?
It depends on the source. If hematuria is from the glomerular disease causing the CKD, use the N02 code and add the CKD stage code (N18.x) as an additional code. If hematuria is unrelated to the glomerular cause, N18.x leads, and R31.x is added if separately evaluated.
Does R31.9 Trigger Payer Audits in Nephrology?
Yes. Frequent R31.9 use in a nephrology setting, where N02 codes are expected, creates a data pattern that commercial payers and MACs flag for review. Quarterly coding audits identify and correct this pattern before it becomes a probe audit.
Do I Need a Biopsy Report to Code N02.B5 for IgA Nephropathy?
For morphology-specific N02 subcodes, the biopsy report (with IF identifying IgA mesangial deposits and LM showing the pattern) should be in the chart to defend the code on audit. If biopsy is pending or unavailable, use N02.9 until the report is available.






