
CPT code 96372 is a drug administration code used to report a single subcutaneous (SC) or intramuscular (IM) injection of a therapeutic, prophylactic, or diagnostic agent. Procedure code 96372 covers the administration service only. The drug itself is billed separately using the appropriate HCPCS J-code.
Code 96372 CPT is one of the most frequently billed injection codes across primary care, urgent care, and specialty practices and applies to a broad range of medications. These include antibiotics, anti-inflammatory agents, biologics, and hormonal agents, provided none qualify for a more specific injection code.
What Is the Description of CPT Code 96372?
96372 CPT code description as defined by the AMA states: “Therapeutic, prophylactic, or diagnostic injection (specify substance or drug); subcutaneous or intramuscular.”
The parenthetical “(specify substance or drug)” reflects the requirement to separately identify and bill the agent administered. 96372 CPT code covers only SC and IM routes. Intravenous push and intra-arterial injections are reported under different codes.
push and intra-arterial injections are reported under different codes.
What Routes of Administration Are Covered Under CPT Code 96372?
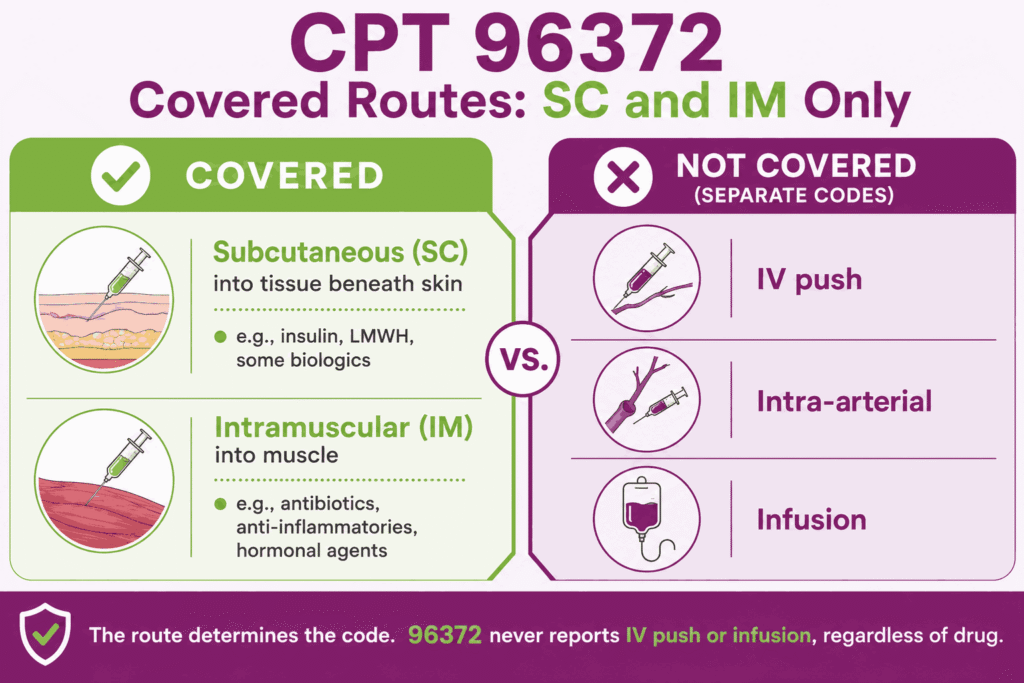
CPT code 96372 covers two routes only:
- Subcutaneous (SC): Injection into the subcutaneous tissue layer beneath the skin, used for agents such as insulin, low-molecular-weight heparins, and some biologics
- Intramuscular (IM): Injection into the muscle, used for antibiotics, anti-inflammatories, hormonal agents, and vaccines when billed under the therapeutic injection pathway
Intravenous (IV) push, intra-arterial, and infusion routes are not covered by procedure code 96372 and require separate codes. The route of administration determines which code applies, as 96372 must not be used to report IV push or infusion delivery regardless of the drug administered.
Why Is CPT Code 96372 an Administration-Only Code, and How Is the Drug Billed Separately?
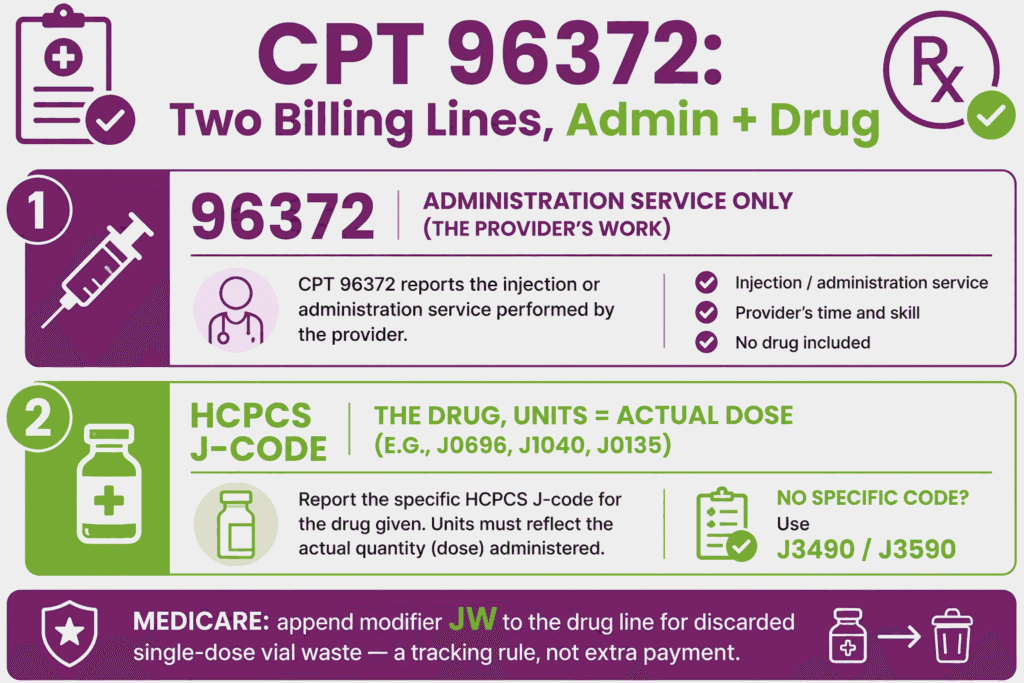
CPT code 96372 covers only the act of administration, which is the provider’s work in preparing and delivering the injection. The drug or biologic administered is billed separately using the appropriate HCPCS Level II J-code (e.g., J0290 for ampicillin, J1040 for methylprednisolone, J0135 for adalimumab). Each J-code should be billed at the number of units corresponding to the actual dose administered.
When a drug does not have a specific J-code, HCPCS J3490 (unclassified drug) or J3590 (unclassified biologic) is used. For Medicare claims, modifier JW must be appended to the drug J-code line when a portion of a single-dose vial is discarded and not administered. This is a drug wastage tracking requirement, not a separate payment modifier.
How Does CPT Code 96372 Differ From CPT Codes 96373, 96374, 90471, 96401, and 96402?
Each of these codes covers a distinct route or clinical context:
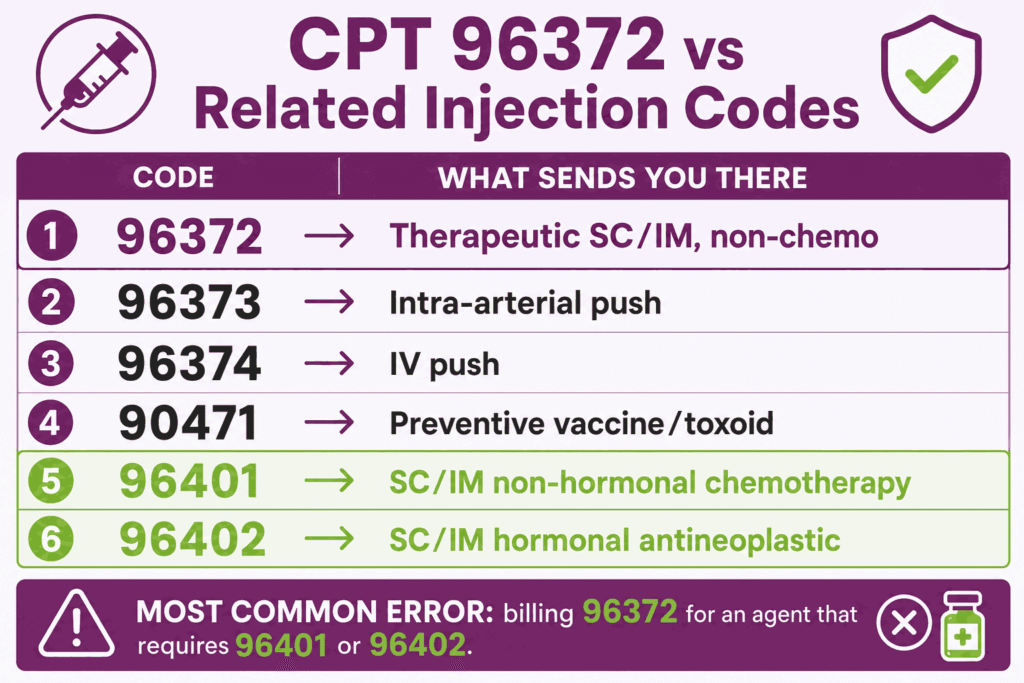
- CPT Code 96373: Intraarterial push. Covers therapeutic injections delivered directly into an artery
- CPT Code 96374: IV push, single or initial substance. Covers therapeutic agents delivered as an intravenous bolus, not SC or IM
- CPT Code 90471: Immunization administration for vaccine/toxoid. Used for prophylactic vaccines only. When a vaccine is administered for preventive purposes, 90471–90474 governs the administration billing, not CPT code 96372
- CPT Code 96401: Chemotherapy injection, SC or IM, non-hormonal antineoplastic agent. When the drug administered is a non-hormonal chemotherapy agent, 96401 replaces procedure code 96372 and must not be substituted with it
- CPT Code 96402: Chemotherapy injection, SC or IM, hormonal antineoplastic agent. Used for agents such as leuprolide, goserelin, or other hormonal antineoplastics. Again, replaces 96372 CPT code when these agents are administered
The most common billing error is using CPT code 96372 for agents that require code CPT 96401 or 96402 CPT code. This creates compliance risk and claim denial.
When Is CPT Code 96372 Not Separately Billable Due to Place-of-Service Restrictions?
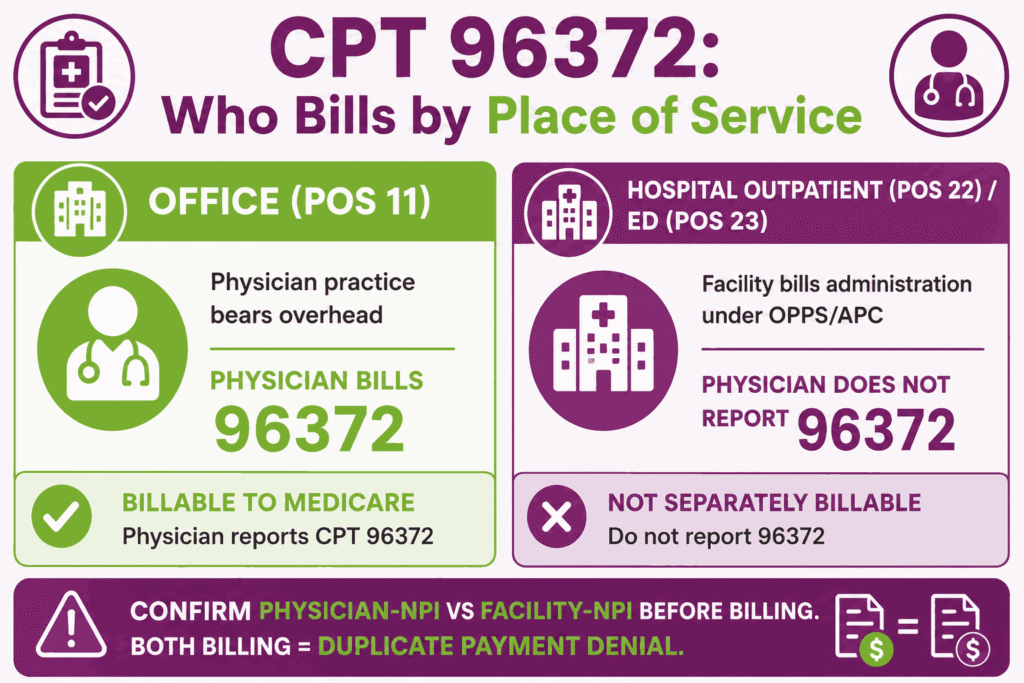
CPT code 96372 is billable by the physician only when the physician’s practice bears the overhead cost of the injection service, typically in a physician office (POS 11). When the injection is performed in a hospital outpatient department (POS 22) or emergency department (POS 23), the facility bills for the injection administration under OPPS, and the physician does not separately report procedure code 96372.
In those facility settings, the injection administration is considered part of the facility’s APC payment, and a physician billing 96372 on top of a facility billing for the same service creates a duplicate payment issue. Providers practicing in hospital-based outpatient settings must confirm whether their practice is billing under a facility NPI or a physician NPI with an independent POS 11 designation before billing CPT code 96372. Sorting physician-NPI from facility-NPI billing before a claim goes out is exactly the edge case that trips practices up, where experienced medical billing support earns its keep.
What are the Modifiers for CPT Code 96372?
Modifiers are used with 96372 to indicate distinct services, repeats, or a same-day E/M when required by payer rules.
Modifier 25: Significant, Separately Identifiable E/M on Same Day as Injection
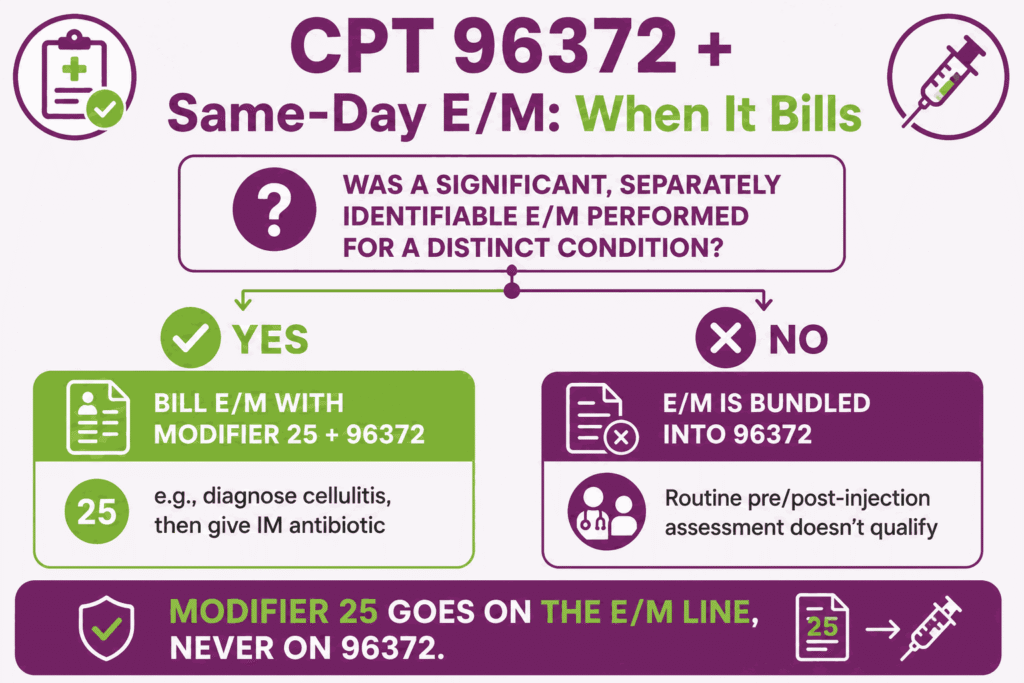
Modifier 25 is appended to the E/M service code, not to CPT code 96372, when a significant, separately identifiable evaluation and management service is performed on the same day as the injection. The E/M must address a separate medical decision beyond the routine administration assessment. Append modifier 25 to the E/M code; procedure code 96372 is listed without any modifier.
Modifier 59: Distinct Procedural Service for Multiple Injections Same Visit
Modifier 59 is used when CPT code 96372 is reported more than once on the same date to indicate that each injection represents a distinct drug administered at a separate anatomical site or for a distinctly separate clinical indication. Documentation must support each additional unit as a separately identifiable administration event.
Modifier 76: Repeat Injection Procedure by Same Provider
Modifier 76 is appended to a subsequent unit of CPT code 96372 on the same date when the same provider repeats the injection for a documented clinical reason. For example, a second IM antibiotic dose administered later in the same day.
Modifier 77: Repeat Injection Procedure by Another Provider
Modifier 77 is used when procedure code 96372 is repeated on the same date by a different provider than the one who administered the first injection. Append modifier 77 to the second provider’s claim and document the clinical basis for the repeat.
Modifier JW: Drug Amount Discarded/Not Administered
Modifier JW is not appended to CPT code 96372 itself but to the drug J-code line when a portion of a single-dose vial or single-use package is discarded and not administered to the patient. Medicare requires this modifier to track drug wastage. The amount discarded should be documented in the medical record and the J-code billed to reflect total units in the vial, with modifier JW distinguishing the administered portion from the discarded portion.
Can CPT Code 96372 Be Billed With an E/M Service on the Same Date?
Yes, but only when a significant, separately identifiable E/M service is performed beyond the routine pre- and post-injection assessment. Per NCCI policy, the E/M component inherent to administering an injection (confirming the drug, route, and patient tolerance) is bundled into CPT code 96372 and does not independently support a separately billed E/M.
However, when a full evaluation is performed for a distinct condition on the same date, for example, examining and diagnosing cellulitis and then administering an IM antibiotic, the E/M service (with modifier 25) and procedure code 96372 may both be reported. Documentation must clearly demonstrate the separately identifiable E/M service.
Which Documents Are Required For CPT Code 96372?
Documentation for the code 96372 CPT must show the order, the drug administered, dose/route/site, administration time, and the provider or staff who performed the injection.
Required documents checklist:
- Medication order or prescription documenting the drug name, dose, route (SC or IM), and clinical indication
- Administration record confirming the drug was administered, including the site of injection, lot number, and expiration date
- Documentation of the clinical indication linking to a specific ICD-10 diagnosis code
- Drug J-code with units billed matching the actual dose administered
- Documentation of drug wastage if modifier JW is used
- If billing E/M with modifier 25: a separately documented evaluation addressing a distinct condition beyond the injection visit
What is the Cost of CPT Code 96372?
With the clinical use established, the next consideration is the cost implications of the CPT code 96372 across payer types and settings.
RVUs & Medicare Payment
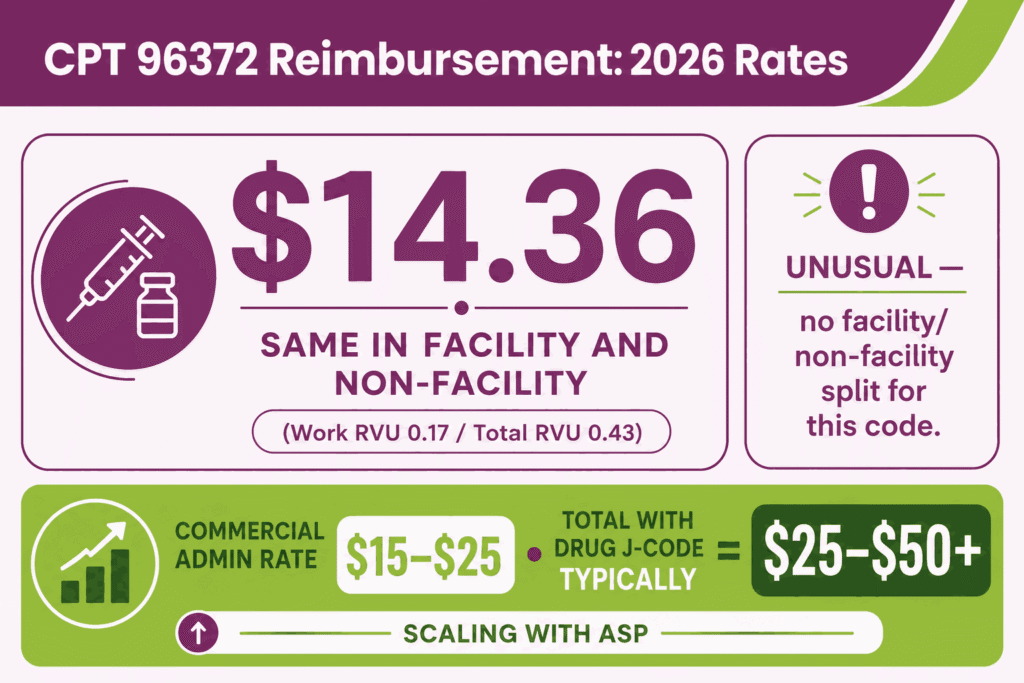
Medicare calculates CPT code 96372 cost by combining a minimal work allocation with the physical overhead required for a syringe injection. For 2026, the Work RVU (wRVU) is locked at 0.17, while the Total Non-Facility RVU is finalized at 0.43 for office settings. When multiplied by the standard 2026 non-QP conversion factor of $33.4009, the national unadjusted office payment settles at $14.36.
Under the Qualifying APM (QP) track, the higher $33.5675 conversion factor brings the rate to $14.43. This payment handles the clinical staff time to draw up the medication, site preparation, the stick itself, and brief post-injection monitoring for adverse reactions.
Commercial Payers
Commercial health insurance plans generally price 96372 CPT cost at a slight premium over Medicare, typically negotiating flat administrative rates between $15 and $25 per injection line. To protect your revenue cycle from automated denials in 2026, billing teams must strictly separate these therapeutic injections from immunizations, which require code CPT 90471, and chemotherapy or complex biologics, which require 96401 code CPT.
Furthermore, if an injection is administered on the same day as an Evaluation and Management (E/M) visit, a modifier 25 must be appended to the E/M code to prove the check-up was separate from the routine pre-injection assessment, otherwise the $14.36 fee will be automatically bundled and denied.
Place-of-Service & Geographic Adjustments
Unlike most procedure codes, 96372 CPT code carries the same total RVU and Medicare payment rate in both facility and non-facility settings. In a private office setting (POS 11), the practice bills 96372 alongside the corresponding HCPCS Level II J-code to secure separate reimbursement for the drug vial itself.
Under this model, the total reimbursement scales dynamically from $25 to over $50+ for routine medications. Moreover, specialized therapeutic injectables scale much higher based on the Average Sales Price (ASP) of the specific drug compound.
What Are Example Clinical Scenarios or Use Cases for CPT Code 96372?
CPT code 96372 is used to report a single IM or SQ therapeutic, prophylactic, or diagnostic injection when the drug itself is billed separately.
Scenario 1: Intramuscular Antibiotic Injection for Cellulitis in Office Setting
ICD-10: L03.115 (Cellulitis of right lower limb)
An established patient presents with early-stage lower extremity cellulitis. The physician evaluates the extent of infection, rules out abscess, and determines outpatient IM antibiotic therapy is appropriate. Ceftriaxone is administered intramuscularly in the office. The physician bills the E/M visit with modifier 25, CPT code 96372 for the injection, and the appropriate J-code (J0696, ceftriaxone sodium) for the drug administered.
Scenario 2: Subcutaneous Biologic Administration for Chronic Disease Management
ICD-10: M06.9 (Rheumatoid arthritis, unspecified)
A patient with rheumatoid arthritis returns for a scheduled SC injection of a biologic agent (adalimumab). No separate E/M evaluation is performed. The visit is solely for the scheduled injection. CPT code 96372 is reported with J0135 (adalimumab injection, 1 mg) billed at the appropriate number of units. Because no separately identifiable E/M service was performed, no E/M code is reported.
Scenario 3: Intramuscular Ketorolac Injection for Acute Pain Management in Outpatient Clinic
ICD-10: M54.5 (Low back pain)
A patient presents to an office-based urgent care clinic with acute severe low back pain. The physician evaluates the patient, confirms musculoskeletal etiology without red flag symptoms, and administers an IM ketorolac injection. The physician bills the E/M with modifier 25, procedure code 96372 for the injection administration, and the appropriate J-code (J1885, ketorolac tromethamine, per 15 mg) for the drug dose administered.
What Are the CPT Code 96372 Rules To Ensure Successful Reimbursement?
For code CPT 96372, document a dated order, the drug details, route/site/time of administration, and separate billing for the drug and the administration service. Understanding the CPT codes meaning and purpose in healthcare helps ensure that these services are reported accurately and reimbursed according to standardized medical billing guidelines.
Bundling / NCCI / Same-Day Procedure Rules
CPT code 96372 is bundled with CPT 90471 (immunization administration) when reported for the same date and patient. Only one administration code applies per injection encounter based on the nature of the agent (therapeutic vs. preventive vaccine).
Do not report procedure code 96372 alongside CPT 96401 or 96402 for a chemotherapy or hormonal antineoplastic injection on the same date, as the more specific chemotherapy code governs. If multiple distinct drugs are injected at separate sites on the same date, each administration unit of CPT code 96372 must be documented as a separately identifiable injection event.
Units, MUEs & Multiple Injection Billing Rules
CPT code 96372 has a Medicare MUE of 3 units per date of service. Each unit represents one injection administration event, a distinct drug administered by SC or IM route.
- Multiple injections of the same drug in a single encounter are reported as additional units of 96372 with modifier 76 (same provider) or 77 (different provider)
- Multiple injections of different drugs at the same visit are reported as additional units with modifier 59 for each distinct drug/site
- The MUE of 3 means Medicare will not reimburse more than 3 injection administration units per provider per patient per day without additional documentation; claims exceeding this threshold will be denied or subject to medical review
- CPT code 96372 carries a 0-day global period. Administration fees are separately billable at each qualifying visit without bundling restrictions
When to Use 96372 vs. 96401/96402 for Chemotherapy and Hormonal Agents
The most critical code-selection rule for procedure code 96372 is confirming that the drug administered is not a chemotherapy or hormonal antineoplastic agent:
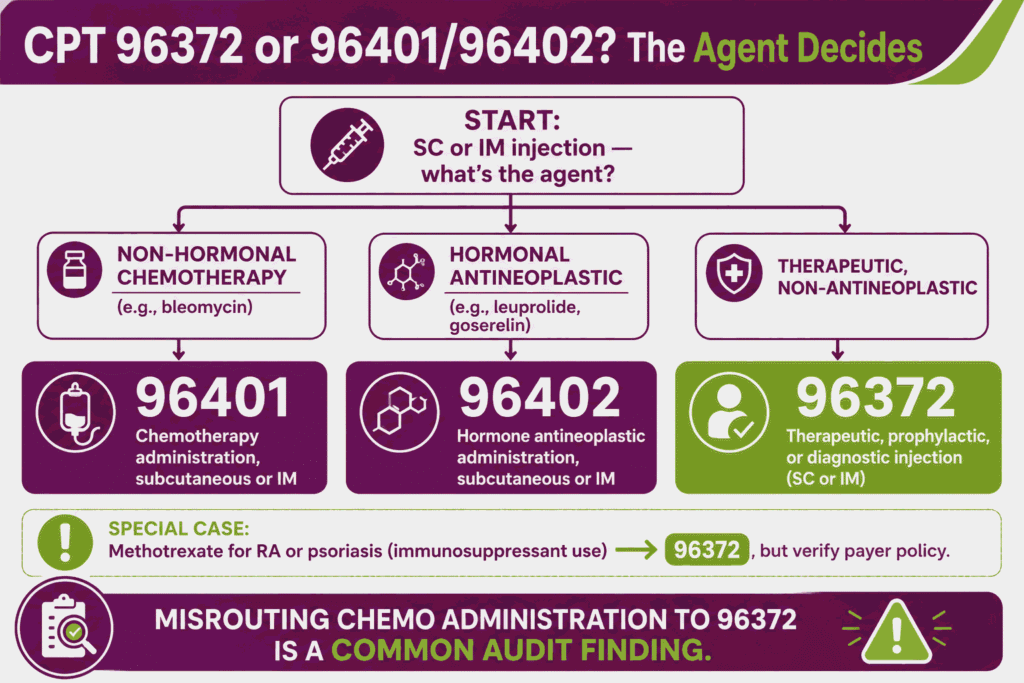
- Non-hormonal chemotherapy agents (e.g., methotrexate for cancer, bleomycin) administered SC or IM → CPT 96401, not 96372 CPT code
- Hormonal antineoplastic agents (e.g., leuprolide acetate/Lupron, goserelin/Zoladex, degarelix) administered SC or IM → CPT 96402, not procedure code 96372
Note that methotrexate administered for rheumatoid arthritis or psoriasis (not cancer) may be reported under CPT code 96372 since it is used in that context as an immunosuppressant rather than a chemotherapy agent. But payers vary on this interpretation, and individual payer policy should be verified. Misrouting a chemotherapy administration to the 96372 CPT code creates a compliance risk and is a common audit finding.
Top Reasons For Denials Specific To 96372 & Quick Remedies
- Wrong Code for Chemotherapy Agent: Prevent by verifying the drug’s clinical use and therapeutic category before billing CPT code 96372. If the agent is a non-hormonal or hormonal antineoplastic, use 96401 or 96402 instead.
- Billed in Facility Setting Where Facility Bills Administration: Prevent by confirming POS before submission. In hospital outpatient (POS 22) or ED (POS 23) settings, the facility bills injection administration under OPPS, and the physician cannot separately bill procedure code 96372.
- Drug J-Code Missing or Incorrect: Prevent by verifying the HCPCS J-code for the specific drug administered and confirming the units billed reflect the actual dose; a claim for CPT code 96372 without an accompanying drug code will be questioned by payers on medical necessity grounds.
- MUE Exceeded Without Modifier 59 or 76/77: Prevent by appending the correct modifier for each additional injection unit beyond the first. Unmodified duplicate codes will be denied as billing errors.






