")
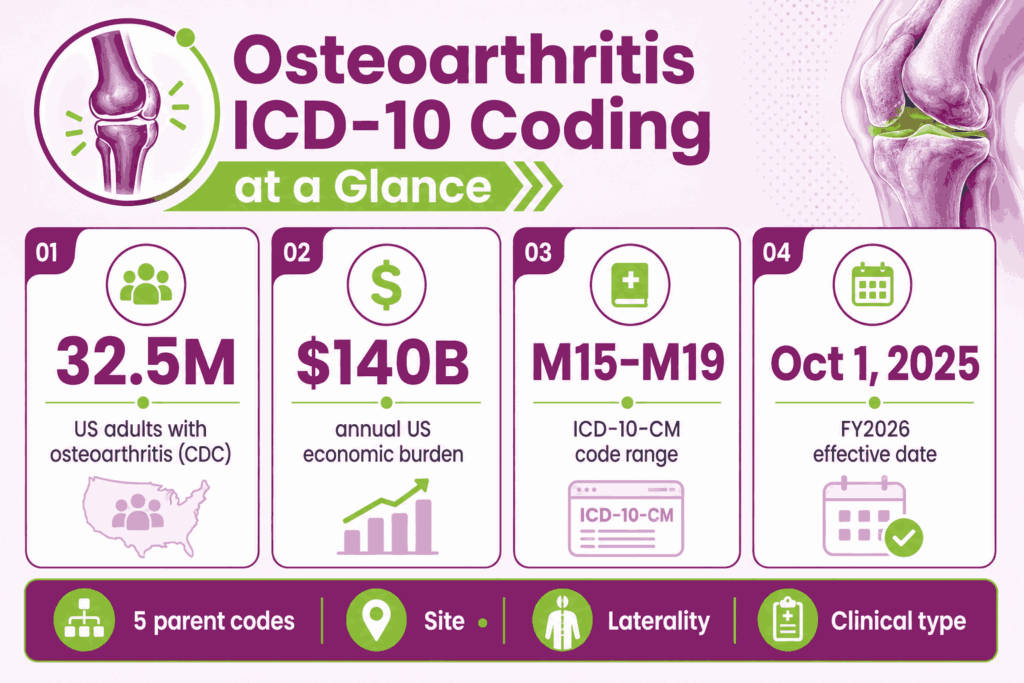
Summary: Osteoarthritis is reported under ICD-10-CM code range M15–M19. The most-billed codes are M17.0 (bilateral primary knee OA), M17.11/M17.12 (unilateral primary right/left knee OA), M16.10–M16.12 (hip OA), and M19.90 (unspecified site). This guide catalogs every M15–M19 code, the documentation each requires, the CPT codes they pair with, and the denial patterns coders see most often in 2026.
Osteoarthritis is the most common form of arthritis and a leading cause of disability in US adults. The Centers for Disease Control and Prevention (CDC) reports that 32.5 million US adults have osteoarthritis, and 1 in 5 American adults (53.2 million) carries some form of arthritis.
The Osteoarthritis Action Alliance, citing CDC and Bone and Joint Initiative data, places the annual US economic burden of osteoarthritis at almost $140 billion. More than 50% of adults with symptomatic knee osteoarthritis are younger than 65.
The ICD-10-CM code range for osteoarthritis is M15 through M19. These codes cover polyosteoarthritis, hip, knee, first carpometacarpal joint, and other site-specific osteoarthritis. Each code captures site, laterality, and whether the disease is primary, post-traumatic, or secondary.
The 2026 edition of ICD-10-CM took effect on October 1, 2025. This guide catalogs every M15 through M19 code, the documentation each requires, the CPT and HCPCS codes they pair with, and the denial patterns coders see most often.
What Is the ICD-10 Code Range for Osteoarthritis?
The ICD-10-CM code range for osteoarthritis is M15 through M19, inside Chapter 13 (“Diseases of the Musculoskeletal System and Connective Tissue”). The five parent codes group osteoarthritis by anatomic site. Cross-referencing these blocks with a complete library of ICD codes for orthopedic diagnostics allows systems to accurately separate localized structural decay from broader systemic arthropathies.
| Parent Code | What It Covers | Joint Pattern |
|---|---|---|
| M15 | Polyosteoarthritis | Multiple joint sites |
| M16 | Osteoarthritis of hip | Hip (right, left, bilateral) |
| M17 | Osteoarthritis of knee | Knee (right, left, bilateral) |
| M18 | Osteoarthritis of first carpometacarpal joint | Thumb base |
| M19 | Other and unspecified osteoarthritis | Shoulder, elbow, wrist, hand, ankle, foot, unspecified |
How Does ICD-10-CM Define Osteoarthritis?
ICD-10-CM defines osteoarthritis as a noninflammatory degenerative joint disease that damages articular cartilage, narrows joint space, and causes osteophyte (bone spur) formation. Common signs include joint pain, stiffness, crepitus, and reduced range of motion. Degenerative joint disease (DJD) is a clinical synonym for osteoarthritis.
What Does the M15–M19 Code Structure Look Like?
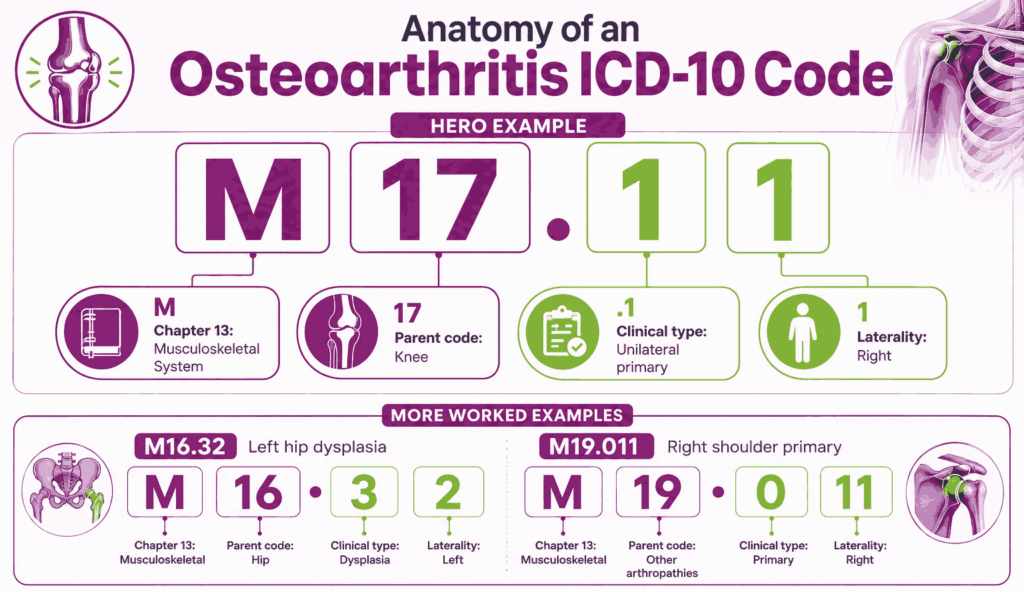
- The first two characters identify the parent code (M15, M16, M17, M18, M19).
- The third character narrows clinical type: primary, post-traumatic, secondary, or unspecified.
- Fourth and fifth characters specify laterality and anatomic detail.
- The sixth character (in M19 codes) specifies the affected joint within “other joints.”
What Is the Difference Between Osteoarthritis (M15–M19) and Spinal Osteoarthritis (M47)?
Osteoarthritis of the spine is coded under M47 (spondylosis), not M15 through M19. The Excludes2 note at the start of M15 through M19 confirms this rule. M47 codes capture cervical, thoracic, lumbar, and sacral levels separately.
Why Does Code Specificity Directly Affect Reimbursement?
Specificity affects reimbursement at four points: medical necessity, claim approval, audit outcome, and risk-adjustment capture. Payers downgrade or deny claims that use unspecified codes when the chart supports a specific code.
What Happens When Unspecified Codes (M17.9, M19.90) Are Overused?
Overuse of M17.9 (knee OA, unspecified) and M19.90 (unspecified site, unspecified OA) triggers three problems: higher denial rates, weaker HCC scores in Medicare Advantage, and audit flags. To resolve these systemic visibility gaps, leading musculoskeletal practices actively contract with top orthopedic billing services to cleanse legacy pick-lists and enforce absolute documentation precision before claims exit the clinic.
How Do Payers Flag Low-Specificity OA Claims for Audit?
Payers run pattern analyses on provider claims data. A practice that bills M17.9 above benchmark rates while submitting CPT 27447 (TKA) for the same patients gets flagged. Surgical CPT codes paired with unspecified diagnosis codes raise prepayment review risk.
What Are All the Osteoarthritis ICD-10 Codes (M15–M19)?
The M15 through M19 catalog covers polyosteoarthritis, hip, knee, thumb base, and other peripheral joints. The five tables below list every billable code.
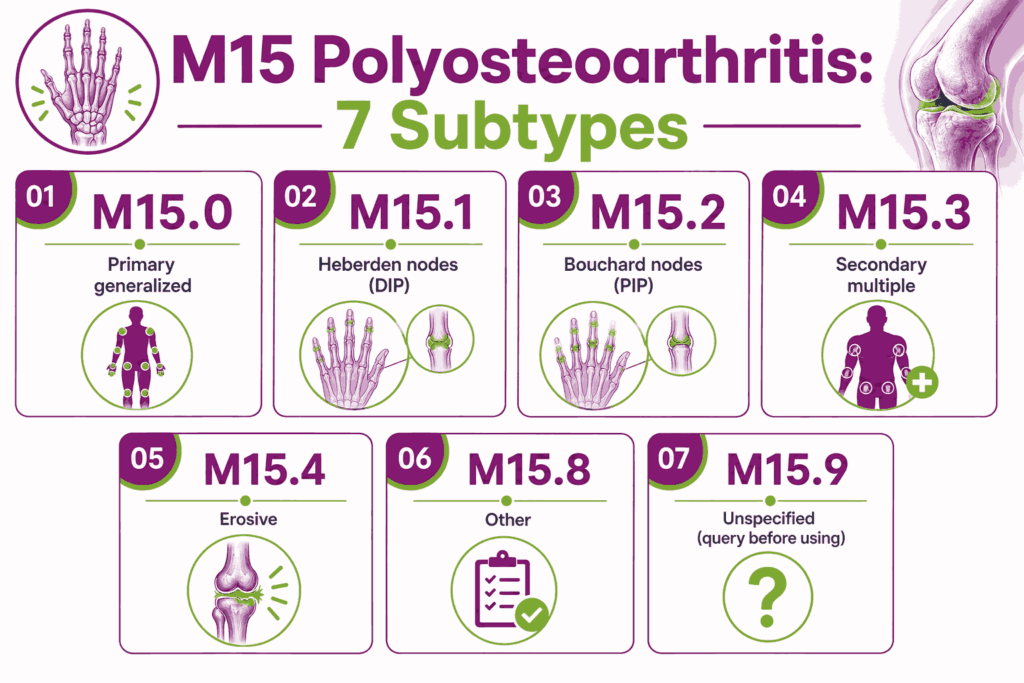
What Are the M15 Codes for Polyosteoarthritis?
M15 codes capture osteoarthritis in multiple joint sites. M15 differs from bilateral single-joint codes (like M17.0) because M15 covers different joint types affected at the same time, not the same joint type on both sides.
| Code | Description |
|---|---|
| M15.0 | Primary generalized (osteo)arthritis |
| M15.1 | Heberden nodes (with arthropathy) |
| M15.2 | Bouchard nodes (with arthropathy) |
| M15.3 | Secondary multiple arthritis |
| M15.4 | Erosive (osteo)arthritis |
| M15.8 | Other polyosteoarthritis |
| M15.9 | Polyosteoarthritis, unspecified |
When Should You Use M15.0 (Primary Generalized Osteoarthritis)?
M15.0 applies when the provider documents primary OA in three or more joint groups without an underlying cause. Bilateral involvement of one joint type (both knees only) maps to M17.0 instead.
How Do You Code Heberden Nodes? (M15.1)
M15.1 is the ICD-10 code for Heberden nodes with arthropathy at the distal interphalangeal (DIP) joints of the fingers.
How Do You Code Bouchard Nodes? (M15.2)
M15.2 captures Bouchard nodes with arthropathy at the proximal interphalangeal (PIP) joints. The two codes differ in which finger joints the provider documents.
How Is M15.3 Different From M15.0?
M15.3 (secondary multiple arthritis) applies when an underlying cause produces the multi-joint disease. Coders sequence the underlying condition first.
When Is Erosive Osteoarthritis Coded as M15.4?
M15.4 applies when the provider documents erosive osteoarthritis with inflammatory and destructive joint changes. Erosive OA differs from rheumatoid arthritis (M05–M06), which carries inflammatory markers.
When Is M15.9 Appropriate?
M15.9 (polyosteoarthritis, unspecified) applies only when multiple joints are documented, but the clinical type is missing. Coders query the provider before defaulting to M15.9.
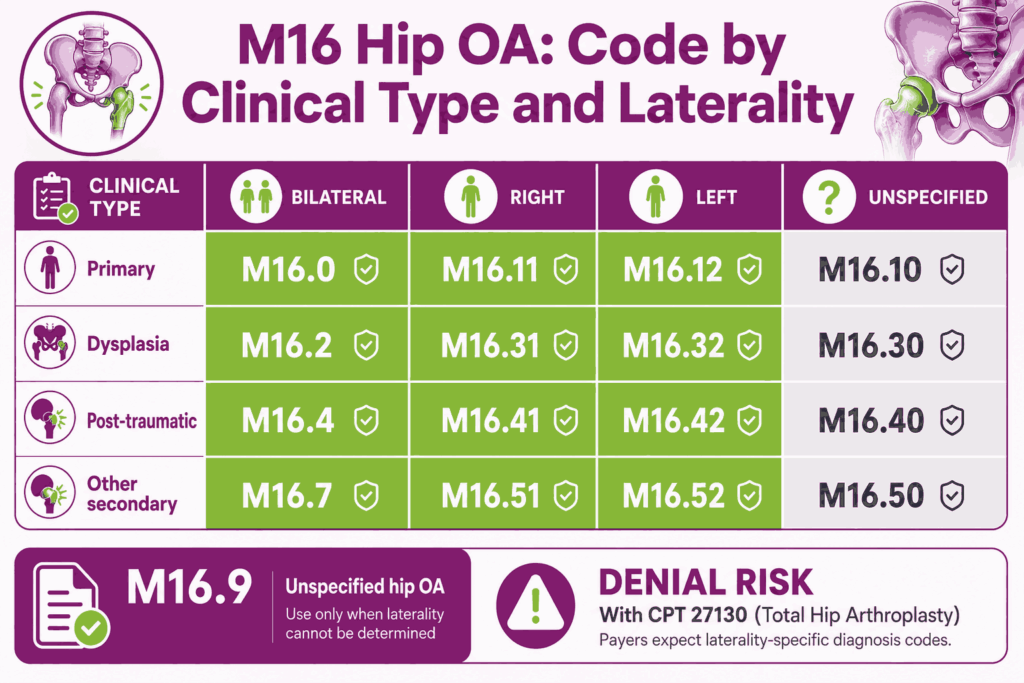
What Are the M16 Codes for Osteoarthritis of the Hip?
M16 codes capture osteoarthritis of the hip joint, tracking primary, dysplasia-related, post-traumatic, and secondary forms with full laterality.
| Code | Description |
|---|---|
| M16.0 | Bilateral primary osteoarthritis of hip |
| M16.10 | Unilateral primary OA, unspecified hip |
| M16.11 | Unilateral primary OA, right hip |
| M16.12 | Unilateral primary OA, left hip |
| M16.2 | Bilateral OA resulting from hip dysplasia |
| M16.30, .31, .32 | Unilateral OA from hip dysplasia (unspecified, right, left) |
| M16.4 | Bilateral post-traumatic OA of hip |
| M16.50, .51, .52 | Unilateral post-traumatic OA (unspecified, right, left) |
| M16.6 | Other bilateral secondary OA of hip |
| M16.7 | Other unilateral secondary OA of hip |
| M16.9 | Osteoarthritis of hip, unspecified |
What Is the ICD-10 Code for Bilateral Primary Hip OA?
M16.0 is the ICD-10 code for bilateral primary osteoarthritis of the hip. The note must confirm both hips and rule out a known underlying cause.
What Are the Unilateral Primary Hip OA Codes?
M16.11 covers the right hip. M16.12 covers the left hip. M16.10 applies only when laterality is missing, which usually warrants a provider query.
How Do You Code Hip OA Resulting From Dysplasia?
M16.2 (bilateral) and M16.30, M16.31, M16.32 (unilateral) cover hip osteoarthritis caused by developmental dysplasia. The note must document the dysplasia history.
How Do You Code Post-Traumatic Hip OA?
M16.4 (bilateral) and M16.50, M16.51, M16.52 (unilateral) apply when prior trauma to the hip caused the OA. The chart must record the original injury.
How Is Other Secondary Hip OA Reported?
M16.6 (bilateral) and M16.7 (unilateral) cover hip OA secondary to causes other than dysplasia or trauma, such as avascular necrosis or prior infection.
When Is M16.9 a Denial Risk?
M16.9 (hip OA, unspecified) flags claims for total hip arthroplasty (CPT 27130). A 27130 claim with M16.9 routinely faces medical-necessity denial.
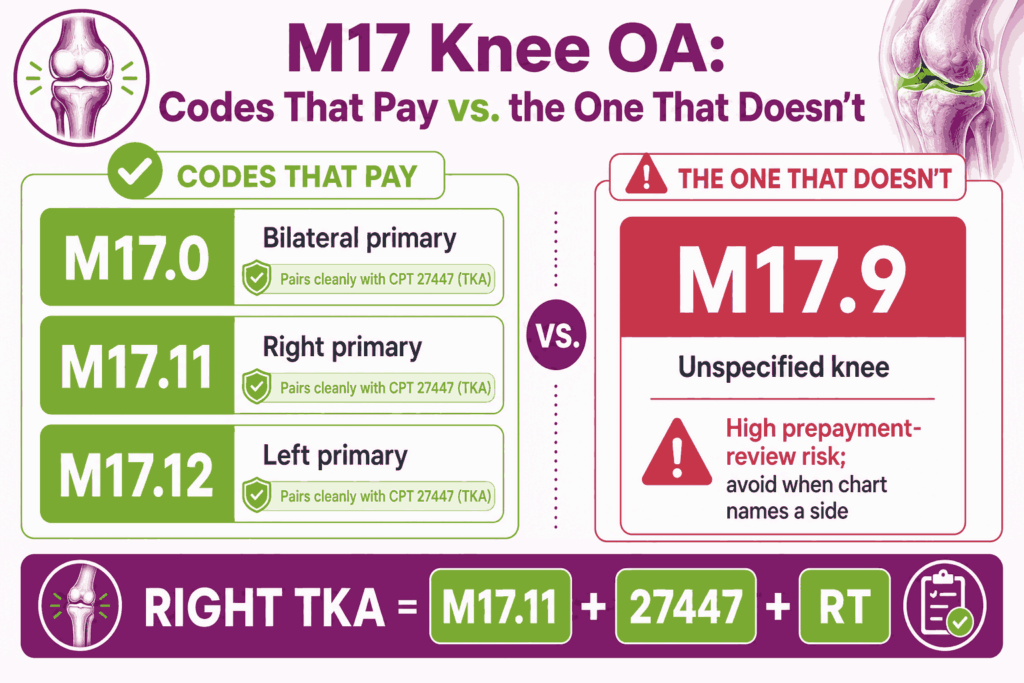
What Are the M17 Codes for Osteoarthritis of the Knee?
M17 codes capture osteoarthritis of the knee joint. M17 is the highest-volume OA category in US claims data, driven by total knee arthroplasty (TKA) and joint injection volume.
| Code | Description |
|---|---|
| M17.0 | Bilateral primary osteoarthritis of knee |
| M17.10 | Unilateral primary OA, unspecified knee |
| M17.11 | Unilateral primary OA, right knee |
| M17.12 | Unilateral primary OA, left knee |
| M17.2 | Bilateral post-traumatic OA of knee |
| M17.30, .31, .32 | Unilateral post-traumatic OA (unspecified, right, left) |
| M17.4 | Other bilateral secondary OA of knee |
| M17.5 | Other unilateral secondary OA of knee |
| M17.9 | Osteoarthritis of knee, unspecified |
What Is the ICD-10 Code for Bilateral Primary Knee OA?
M17.0 is the ICD-10 code for bilateral primary osteoarthritis of the knee. The note must confirm both knees and document the primary (non-traumatic, non-secondary) clinical type.
What Is the ICD-10 Code for Right Knee Primary OA?
M17.11 is the ICD-10 code for unilateral primary osteoarthritis of the right knee. The chart must specify “right” and confirm no underlying cause.
What Is the ICD-10 Code for Left Knee Primary OA?
M17.12 is the ICD-10 code for unilateral primary osteoarthritis of the left knee. The chart must specify “left” and confirm the primary clinical type.
When Is M17.10 Used?
M17.10 (unilateral primary OA, unspecified knee) applies only when the chart confirms one knee but never states which side. Coders query the provider first.
How Do You Code Post-Traumatic Knee OA?
M17.2 covers bilateral post-traumatic knee OA. M17.31 covers the right, M17.32 the left, M17.30 the unspecified side. The chart must document the original injury.
How Do You Code Secondary Knee OA?
M17.4 covers other bilateral secondary OA of the knee. M17.5 covers the unilateral case. Coders sequence the underlying cause (prior infection, systemic condition) first.
When Is M17.9 a Denial Trigger?
M17.9 (knee OA, unspecified) is a high-denial code on surgical and procedural claims. CPT 27447 (TKA), paired with M17.9, commonly faces prepayment review.
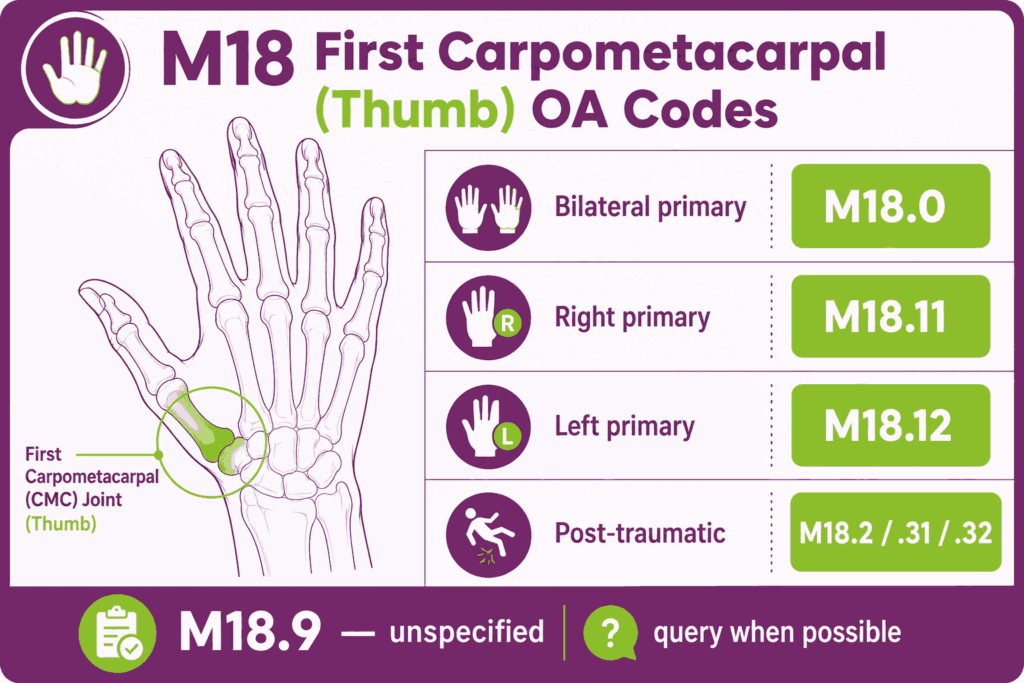
What Are the M18 Codes for the First Carpometacarpal Joint?
M18 codes capture osteoarthritis of the first carpometacarpal (CMC) joint at the base of the thumb. Thumb CMC OA is common in hand surgery and rheumatology billing.
| Code | Description |
|---|---|
| M18.0 | Bilateral primary OA of first CMC joints |
| M18.10, .11, .12 | Unilateral primary OA (unspecified, right, left) |
| M18.2 | Bilateral OA of first CMC joints from trauma |
| M18.30, .31, .32 | Unilateral post-traumatic OA (unspecified, right, left) |
| M18.4 | Other bilateral secondary OA of first CMC joints |
| M18.50, .51, .52 | Unilateral other secondary OA (unspecified, right, left) |
| M18.9 | Osteoarthritis of first CMC joint, unspecified |
How Do You Code Bilateral vs. Unilateral Thumb CMC OA?
M18.0 covers bilateral primary thumb CMC OA. M18.11 covers the right thumb, M18.12 the left. M18.10 applies only when laterality is missing.
How Is Post-Traumatic Thumb CMC OA Coded?
M18.2 covers the bilateral case. M18.31 (right) and M18.32 (left) cover unilateral post-traumatic CMC OA. The chart must document the prior trauma.
When Is M18.9 the Right Code?
M18.9 (first CMC OA, unspecified) applies when the site is confirmed, but type and laterality are missing. Coders treat M18.9 as a last resort.
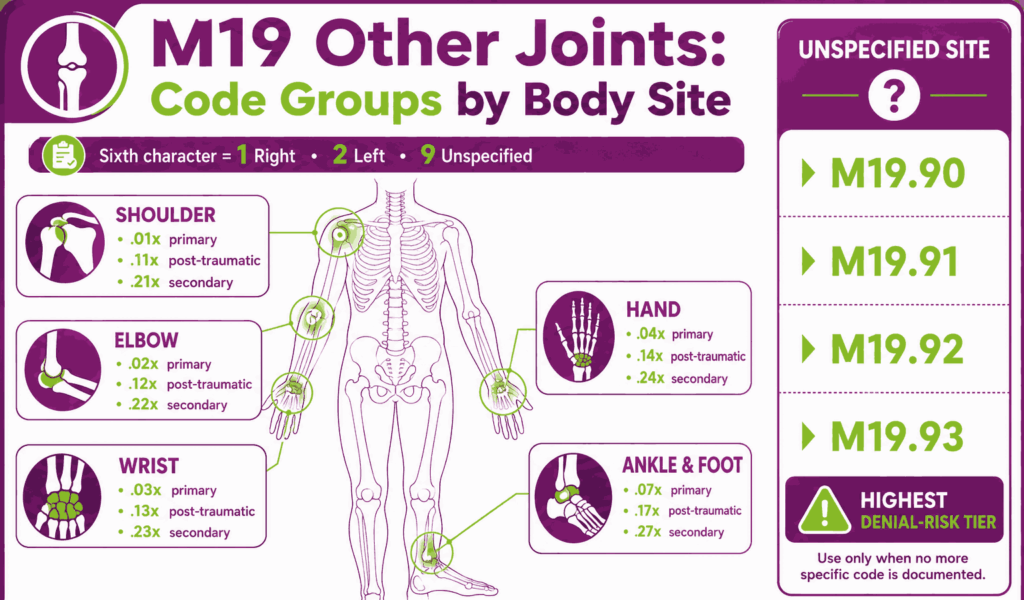
What Are the M19 Codes for Other Joints?
M19 codes cover osteoarthritis in joints not classified under M15 through M18: shoulder, elbow, wrist, hand, ankle, and foot, plus an unspecified-site tier. The sixth character specifies laterality (1 = right, 2 = left, 9 = unspecified).
| Code Group | Joint | Clinical Type |
|---|---|---|
| M19.01x | Shoulder | Primary |
| M19.02x | Elbow | Primary |
| M19.03x | Wrist | Primary |
| M19.04x | Hand | Primary |
| M19.07x | Ankle and foot | Primary |
| M19.11x | Shoulder | Post-traumatic |
| M19.12x | Elbow | Post-traumatic |
| M19.13x | Wrist | Post-traumatic |
| M19.14x | Hand | Post-traumatic |
| M19.17x | Ankle and foot | Post-traumatic |
| M19.21x | Shoulder | Secondary |
| M19.22x | Elbow | Secondary |
| M19.23x | Wrist | Secondary |
| M19.24x | Hand | Secondary |
| M19.27x | Ankle and foot | Secondary |
| M19.90 | Unspecified site | Unspecified |
| M19.91 | Unspecified site | Primary |
| M19.92 | Unspecified site | Post-traumatic |
| M19.93 | Unspecified site | Secondary |
Example: M19.011 = primary OA, right shoulder.
How Do You Code Shoulder OA?
Primary shoulder OA uses M19.011 (right), M19.012 (left), and M19.019 (unspecified). Post-traumatic uses M19.111/.112/.119. Secondary uses M19.211/.212/.219.
How Do You Code Elbow, Wrist, and Hand OA?
Elbow OA uses M19.02x (primary), M19.12x (post-traumatic), M19.22x (secondary). Wrist OA uses M19.03x/.13x/.23x. Hand OA uses M19.04x/.14x/.24x. The sixth character specifies right (1), left (2), or unspecified (9).
How Do You Code Ankle and Foot OA?
Ankle and foot OA share a code group at the fifth character: .07x for primary, .17x for post-traumatic, .27x for secondary. M19.071 covers the right side, M19.072 the left, M19.079 unspecified.
When Is M19.90 the Correct Choice?
M19.90 (unspecified osteoarthritis, unspecified site) applies only when site, laterality, and clinical type are all missing. M19.90 is the highest-risk OA code for denials and HCC underperformance.
What Is the Difference Between M19.91, M19.92, and M19.93?
M19.91 is primary OA, unspecified site. M19.92 is post-traumatic. M19.93 is secondary. All three remain unspecified-site codes and face the same denial risk profile as M19.90.
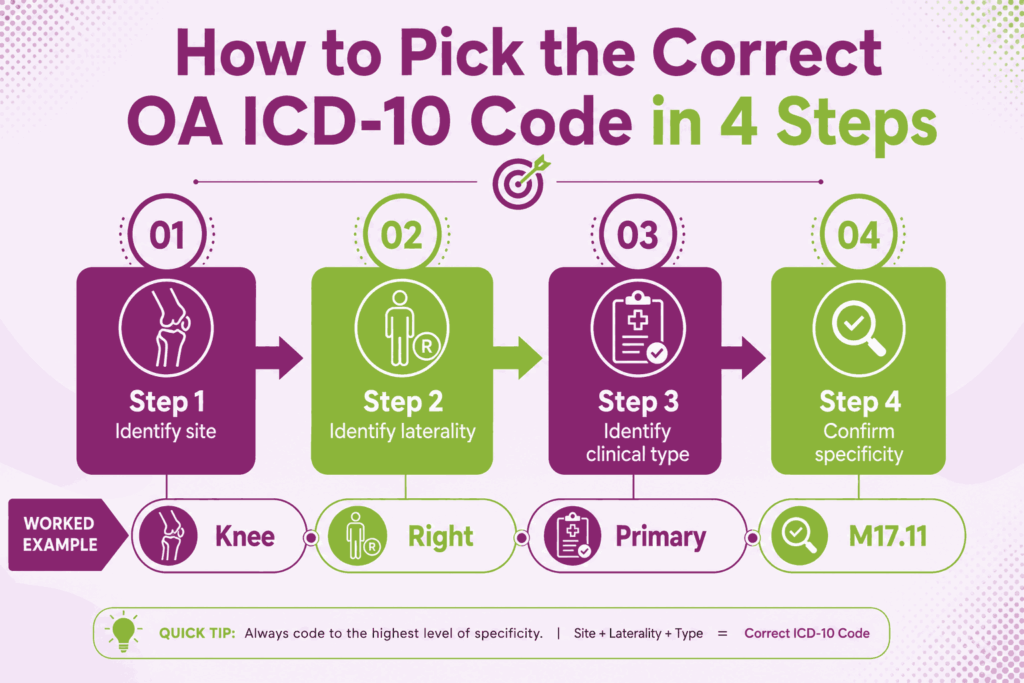
How Do You Choose the Correct Osteoarthritis ICD-10 Code?
Correct osteoarthritis ICD-10 code selection follows a four-step decision logic. Each step narrows the code by one attribute: site, laterality, clinical type, and specificity tier. Utilizing a structured ICD 10 coding cheat sheet eliminates the guesswork from this workflow, allowing teams to systematically cross-reference clinical criteria without losing speed during high-volume charting.
What Is the Four-Step Decision Logic?
- Identify the joint site. Knee, hip, thumb CMC, shoulder, elbow, wrist, hand, ankle, foot, or multiple. Site selects the parent code.
- Identify laterality. Right, left, or bilateral. Laterality selects the fourth or fifth character.
- Identify the clinical type. Primary, post-traumatic, secondary, or unspecified. Clinical type selects the third or fourth character.
- Confirm specificity. Use the most specific code the documentation supports. Default to unspecified codes only when the chart truly lacks the detail.
How Do You Determine Primary vs. Secondary vs. Post-Traumatic OA?
Primary OA develops without a documented underlying cause. Post-traumatic OA follows a documented injury. Secondary OA is caused by another condition, such as avascular necrosis, prior infection, or hip dysplasia.
What Documentation Supports a Primary OA Assignment?
The provider’s note states “primary osteoarthritis” or describes degenerative changes with no underlying cause. Imaging confirms joint space narrowing and osteophyte formation.
What Documentation Is Required for Secondary OA?
The provider documents the underlying condition (obesity, prior septic arthritis, avascular necrosis). The coder sequences the underlying condition first, then the secondary OA code.
When Should Post-Traumatic OA Be Coded?
Post-traumatic OA codes apply when the chart documents a prior injury to the affected joint and links the degeneration to that injury. The injury can be remote or recent.
How Do Excludes1 and Excludes2 Notes Apply to M15–M19?
Excludes1 notes prohibit reporting two codes together. Excludes2 notes allow both codes when both conditions are present. M15 through M19 carry both note types.
Why Can M15 Not Be Reported With M17.0?
M15 (polyosteoarthritis) covers multiple joint types affected at once. M17.0 (bilateral knee OA) covers both knees only. Reporting both miscounts the disease pattern. The Excludes1 note at M15 prevents the pairing.
What Conditions Are Excluded From M15–M19?
The following are the excluded conditions from the M15 to M19 range:
| Excluded Condition | Correct Code Range |
|---|---|
| Osteoarthritis of spine | M47 (spondylosis) |
| Hallux rigidus | M20.2 |
| Other and unspecified arthropathies | M12 |
When Should DJD Be Coded the Same as OA?
DJD (degenerative joint disease) is a clinical synonym for osteoarthritis. The ICD-10-CM Alphabetic Index directs coders from DJD to osteoarthritis. When the chart documents DJD with site and laterality, coders assign the corresponding M15 through M19 code. DJD without a named site defaults to M19.90, which carries denial risk.
What Documentation Supports Osteoarthritis ICD-10 Claims?
Documentation supports osteoarthritis ICD-10 claims when the provider’s note captures site, laterality, clinical type, and supporting clinical evidence. ICD-10-CM Official Guidelines require consistent and complete documentation for code assignment.
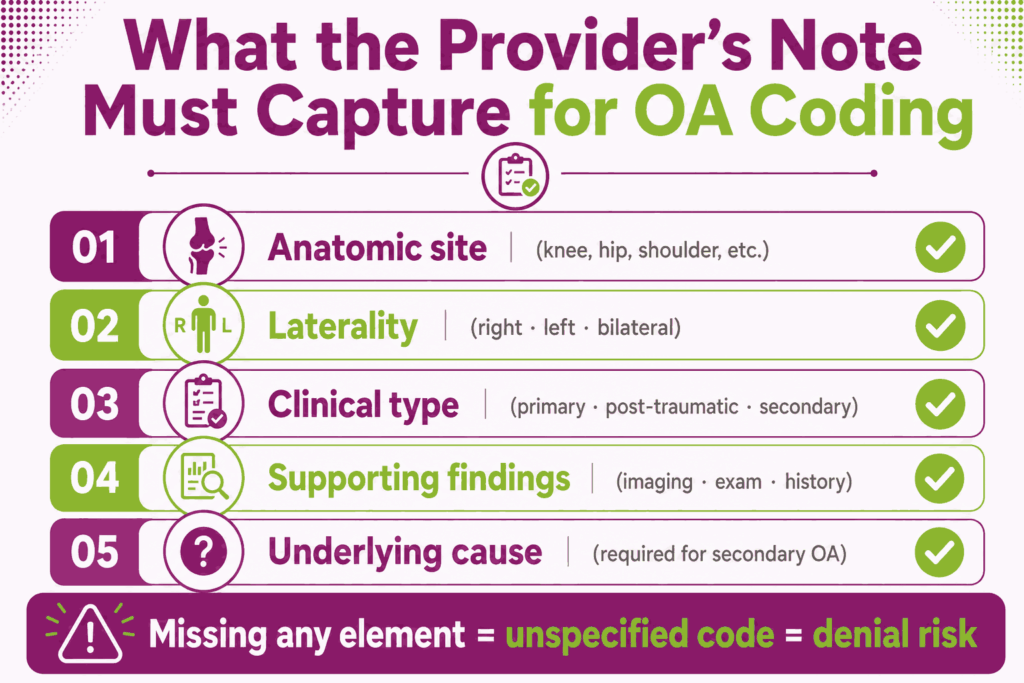
What Clinical Elements Must the Provider’s Note Contain?
- Anatomic site (knee, hip, shoulder, etc.)
- Laterality (right, left, bilateral)
- Clinical type (primary, post-traumatic, secondary)
- Supporting findings (imaging, exam, history)
- Underlying cause (for secondary OA)
Why Is Laterality the Most-Cited Documentation Gap?
Providers sometimes write “knee OA” without specifying the side. Coders cannot assign laterality from clinical inference. Missing laterality forces an unspecified-side code and raises denial and audit risk.
How Specific Does the Joint Site Need to Be?
The joint site must map to one ICD-10-CM code. “Wrist pain” is not specific. “Right wrist osteoarthritis confirmed by X-ray” is specific.
What Imaging and Diagnostic Findings Should Be Captured?
The note captures X-ray, MRI, or CT findings that confirm osteoarthritis: joint space narrowing, osteophyte formation, subchondral sclerosis, and subchondral cysts. Imaging dates and impressions belong in the chart.
How Are X-Ray Findings Tied to Code Selection?
X-ray findings confirm the diagnosis and support medical necessity for procedural CPT codes. Joint space narrowing and osteophytes support a primary OA code. Old fracture lines or prior surgical hardware support a post-traumatic code.
Is Kellgren-Lawrence Grading Required for Coding?
Kellgren-Lawrence (K-L) grading is not required by ICD-10-CM. K-L grades support medical necessity for joint injections and arthroplasty, but the grade does not change the diagnosis code.
How Should Conservative Treatment Failure Be Documented?
Conservative treatment failure documentation captures the trial of NSAIDs, physical therapy, intra-articular injections, weight management, and bracing. The note records duration, frequency, and patient response. Surgical claims for total joint arthroplasty require this trail.
What EHR Template Fields Close the Most Common Gaps?
EHR templates close documentation gaps when the fields force site, laterality, and clinical type entries before the encounter closes. Drop-down menus for primary, post-traumatic, and secondary types reduce ambiguity.
Which CPT, HCPCS, and Modifiers Pair With Osteoarthritis ICD-10 Codes?
Osteoarthritis ICD-10 codes pair with CPT and HCPCS codes for injections, viscosupplementation, arthroplasty, and DME. Correct CPT-to-ICD-10 pairing supports medical necessity and prevents denials. Consulting a specialized billing guide for orthopedic procedures provides coding teams with a clean blueprint for linking structural diagnoses directly to their exact therapeutic or surgical line items.
Which CPT Codes Are Most Commonly Billed With OA Diagnoses?
The following CPT and HCPCS codes are most used when billing osteoarthritis:
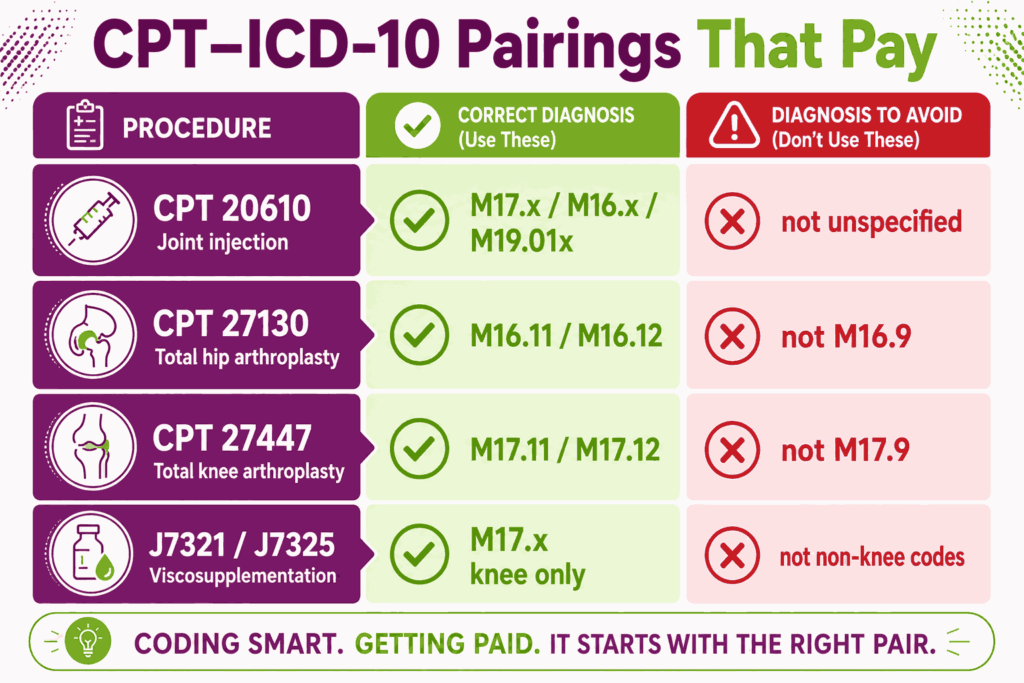
| CPT/HCPCS | Description | Common ICD-10 Pairing |
|---|---|---|
| 20610 | Major joint injection (knee, hip, shoulder) | M16.x, M17.x, M19.01x |
| 20611 | Same as 20610, with ultrasound guidance | M16.x, M17.x, M19.01x |
| 27130 | Total hip arthroplasty | M16.11, M16.12 (not M16.9) |
| 27447 | Total knee arthroplasty | M17.11, M17.12 (not M17.9) |
| 27486 | Revision TKA, one component | Post-revision M17 codes |
| 27487 | Revision TKA, all components | Post-revision M17 codes |
| 27134 | Revision THA, all components | Post-revision M16 codes |
| J7321 | Hyaluronan injection (Hyalgan, Supartz) | M17.0, M17.11, M17.12 |
| J7325 | Synvisc/Synvisc-One injection | M17.0, M17.11, M17.12 |
| J7333 | Visco-3 hyaluronan injection | M17.0, M17.11, M17.12 |
| L1832 | Knee orthosis, adjustable | M17.x (K-L grade often required) |
| L1851 | Knee orthosis, single upright | M17.x |
Joint Injections (CPT 20610 and 20611)
CPT 20610 covers a major joint or bursa injection without imaging guidance. CPT 20611 adds ultrasound guidance. Both pair with a site-specific M16, M17, or M19 code.
Viscosupplementation (HCPCS J7318 Through J7333)
HCPCS J7318 through J7333 cover hyaluronan and hylan injections for knee osteoarthritis. Payers typically authorize viscosupplementation only for knee OA codes (M17.x).
Total Hip Arthroplasty (CPT 27130)
CPT 27130 pairs with M16.11 or M16.12 (laterality-specific primary hip OA) or with a post-traumatic or secondary hip code. A 27130 claim paired with M16.9 usually triggers a medical-necessity review.
Total Knee Arthroplasty (CPT 27447)
CPT 27447 pairs with M17.0, M17.11, or M17.12. Payers reject 27447 paired with M17.9 in most cases. Post-traumatic M17.31/M17.32 and secondary M17.5 codes also pair correctly when documentation supports them.
Revision Arthroplasty Codes
CPT 27486 and 27487 cover revision TKA. CPT 27134, 27137, and 27138 cover revision THA. Revision claims pair with the same M16 or M17 codes plus complication codes (T84.0–T84.5) when documented.
Knee Orthoses and DME (HCPCS L Codes)
HCPCS L1832, L1843, L1845, L1851, and L1852 cover knee orthoses billed under DME. Coverage rules require K-L grade documentation, a conservative-care trial, and a laterality-specific knee OA diagnosis.
Which Modifiers Apply Most Often to OA Claims?
Modifier 50, RT, LT, 26, and TC are the most used modifiers with OA claims.
When Do You Use Modifier 50?
Modifier 50 indicates a bilateral procedure on paired structures. Modifier 50 applies to CPT 27447 when both knees are replaced in the same session. Coders verify the CPT is not already bilateral by definition before adding modifier 50.
When Do RT and LT Replace Modifier 50?
Modifiers RT (right) and LT (left) replace modifier 50 for payers that prefer single-side reporting on separate claim lines. Medicare typically accepts modifier 50 on one line. Some commercial payers require RT and LT on two lines.
How Are Modifiers 26 and TC Split for OA Imaging?
Modifier 26 marks the professional component (interpretation). Modifier TC marks the technical component (equipment, supplies). X-ray and MRI for OA workups are split into 26 and TC when the radiologist and imaging center bill separately.
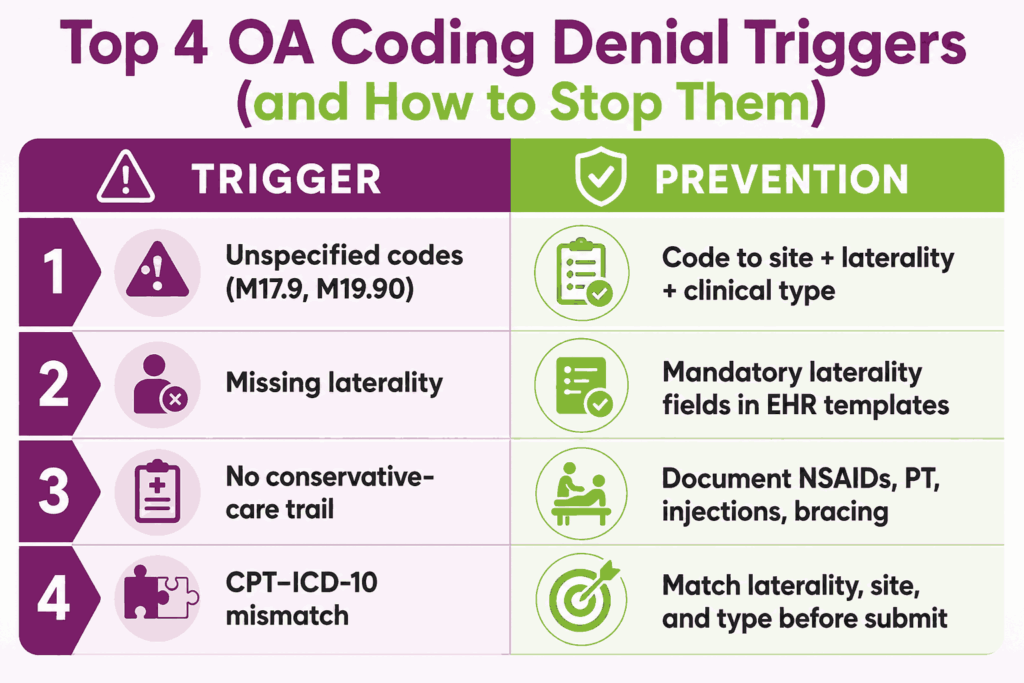
How Do You Avoid CPT-ICD-10 Mismatches?
Coders check three points before claim submission: diagnosis-code laterality matches procedure laterality, diagnosis-code site matches procedure site, and clinical-type code matches the documented history. A right TKA (27447, RT) requires M17.11, never M17.12 or M17.9.
What Are the Most Common Osteoarthritis Coding Denials, and How Do You Prevent Them?
The most common osteoarthritis coding denials come from unspecified codes, missing laterality, absent conservative-care documentation, and CPT-ICD-10 mismatches.
Why Do Unspecified OA Codes Drive Denials and Downcoding?
Unspecified OA codes (M17.9, M16.9, M18.9, M19.90, M19.91, M19.92, M19.93) drive denials because payers expect site- and laterality-specific codes when the procedure itself is site- and laterality-specific. Arthroplasty, viscosupplementation, and knee orthosis claims all face higher denial rates with unspecified diagnoses. Because major surgical margins absorb heavy administrative overhead during long appeals, high-volume groups regularly outsource these workflows to the best orthopedic billing companies to defend their revenue cycles from day one.
How Does Missing Laterality Result in Claim Rejection?
Missing laterality forces an unspecified-side code (M17.10, M16.10, M18.10, M19.x9). Payers run automated edits that flag procedure-diagnosis laterality mismatches. A right knee injection (20610 RT) paired with M17.10 triggers automatic review.
Why Are Surgical Claims Denied Without Conservative-Care Documentation?
Joint replacement claims require documented failure of conservative care. Commercial payers and Medicare LCDs list NSAIDs, physical therapy, weight management, bracing, and injection trials as required steps. A 27447 claim without this trail faces denial regardless of diagnosis code accuracy.
How Do Payer-Specific Rules Change OA Reimbursement?
Each payer, from Medicare to UnitedHealthcare and Atena, applies its own rules for OA reimbursement.
| Payer | Common Rule |
|---|---|
| Medicare | LCDs require K-L grade, conservative-care trial, and laterality-specific diagnosis for arthroplasty and DME |
| BCBS plans | Viscosupplementation authorization varies by state plan; some restrict to specific J-codes |
| UnitedHealthcare | Prior authorization required for arthroplasty and viscosupplementation in most regions |
| Aetna | Step therapy required for viscosupplementation in many policies |
| Medicare Advantage | HCC capture weakened when unspecified OA codes used in chronic conditions |
What Does Medicare Require for OA Procedures?
Medicare requires LCD-aligned documentation for arthroplasty, viscosupplementation, and DME. LCDs specify K-L grade, conservative-care trial length, and laterality-specific diagnosis. Local Coverage Articles list covered CPT-ICD-10 pairs.
How Do BCBS and UnitedHealthcare Differ on Viscosupplementation?
BCBS state plans differ in covered J-codes and injection cycles allowed per year. UnitedHealthcare typically requires prior authorization for all viscosupplementation, with documentation of failed conservative care.
When Does Prior Authorization Apply to OA Procedures?
Prior authorization applies to arthroplasty (27130, 27447, 27486, 27487, 27134, 27137, 27138), most viscosupplementation J-codes, and many knee orthoses (L1832, L1843, L1845, L1851, L1852).
What Is the Appeal Pathway for a Denied OA Claim?
The appeal pathway follows three steps: request a reconsideration with the corrected code and supporting documentation, file a formal appeal with the chart and imaging report, and escalate to external review if the payer upholds the denial.
How Do Unspecified OA Codes Affect HCC Risk Adjustment?
Unspecified OA codes weaken HCC risk-adjustment scores in Medicare Advantage populations. Specific codes capture disease severity better. Practices that default to M17.9 or M19.90 across a Medicare Advantage panel under-report severity and lose risk-adjusted revenue.
What Changed in the FY2026 ICD-10-CM Update for Osteoarthritis?
The FY2026 ICD-10-CM update for osteoarthritis took effect on October 1, 2025. The M15 through M19 block carried minor refinements rather than structural changes. The update is published by the National Center for Health Statistics (NCHS) and CMS.
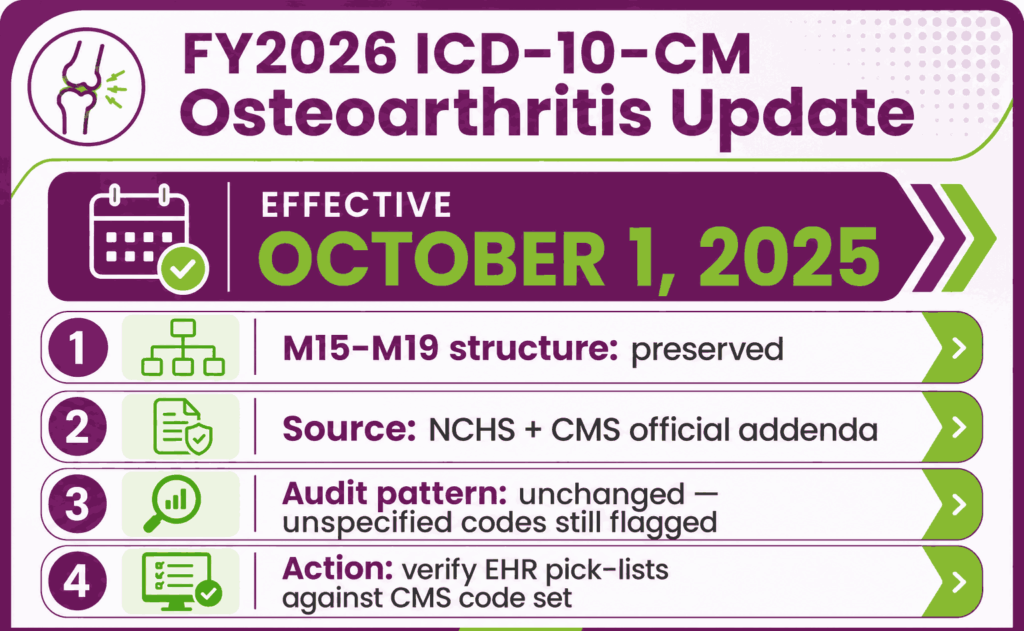
Which OA Codes Were Added, Revised, or Deleted Effective October 1, 2025?
The FY2026 update preserved the M15 through M19 structure. Practices verify changes against the CMS-published FY2026 code set and the ICD-10-CM Official Guidelines. CMS releases the addenda each summer before the October 1 effective date.
How Do FY2026 Changes Affect Knee and Hip OA Workflows?
Knee and hip OA workflows continue to use M16 and M17 with the same laterality and clinical-type structure. Coders confirm that EHR diagnosis pick-lists carry the current code descriptors.
What Audit Exposures Does FY2026 Create for Unspecified Codes?
Audit exposure on unspecified OA codes (M17.9, M19.90) continues in the same pattern. Payers analyze provider-level claims data and flag practices that exceed peer benchmarks for unspecified-code usage.
Frequently Asked Questions About Osteoarthritis ICD-10 Coding
What Is the ICD-10 Code for Osteoarthritis of the Knee?
The ICD-10 code for osteoarthritis of the knee is M17. M17.0 covers bilateral primary knee OA. M17.11 covers the right knee. M17.12 covers the left knee. M17.9 covers an unspecified knee but carries a denial risk.
What Is the Difference Between M17.0 and M17.9?
M17.0 is bilateral primary osteoarthritis of the knee, applied when both knees are affected without an underlying cause. M17.9 is knee OA, unspecified, used only when laterality and type are missing. M17.0 supports surgical claims; M17.9 commonly does not.
Is Degenerative Joint Disease the Same as Osteoarthritis for Coding Purposes?
Degenerative joint disease (DJD) is a clinical synonym for osteoarthritis. The ICD-10-CM Alphabetic Index routes DJD to osteoarthritis. Coders assign the M15 through M19 code that matches the documented site, laterality, and clinical type.
How Is Bilateral Osteoarthritis Coded in ICD-10?
Bilateral OA of one joint type uses a bilateral parent code: M16.0 (hip), M17.0 (knee), M18.0 (thumb CMC), plus the M16.2/M16.4, M17.2/M17.4, M18.2/M18.4 variants. Bilateral OA in multiple joint types uses M15.
What Is the ICD-10 Code for Osteoarthritis With Obesity?
Osteoarthritis with obesity uses two codes: the relevant code from M15 through M19, plus a code from E66 (overweight and obesity). Coders sequence based on the reason for the encounter.
Is There a Z-Code for History of Osteoarthritis?
No Z-code exists for the personal history of osteoarthritis. Osteoarthritis is a chronic, ongoing condition. The active M15 through M19 code applies whenever it is documented in the current encounter.
What Is the ICD-10 Code for Osteoarthritis of Multiple Joints?
The ICD-10 code for osteoarthritis of multiple joints is M15. Subcodes are M15.0 (primary generalized), M15.1 (Heberden), M15.2 (Bouchard), M15.3 (secondary multiple), M15.4 (erosive), M15.8 (other), M15.9 (unspecified).
Can M19.90 Be Used as a Primary Diagnosis on a Surgical Claim?
M19.90 (unspecified OA, unspecified site) rarely supports a surgical claim. Surgical CPT codes describe a specific joint and side. A site- and laterality-specific code from M15 through M18 or M19.01 through M19.27 supports medical necessity.






