
A 2025 OIG audit found that 44 of 100 sampled podiatry E/M claims billed with modifier 25 did not comply with Medicare requirements. The audit projected $39.6 million of $222.5 million in non-compliant payments for the review period. Coding accuracy directly drives reimbursement, and modifier misuse is now under sharper review.
Most podiatry denials trace back to issues unique to this specialty. Medicare excludes routine foot care unless the patient has qualifying systemic conditions like diabetes or peripheral vascular disease. Every routine code submitted without the right modifier and supporting diagnosis ends up denied.
This cheat sheet covers the most-used podiatry CPT codes grouped by procedure type. Each entry includes the descriptor, documentation rules, and modifier or NCCI traps that affect payment. Whether you handle claims in-house or use specialized podiatry billing services, keep this as your coding reference.
Podiatry CPT Codes Cheat Sheet for 2026: A Quick Glance
Use this table as a quick reference. Each code is detailed by section below with documentation rules, frequency limits, and modifier requirements.
| Code | Descriptor | Category | Common Modifier |
|---|---|---|---|
| 11719 | Trimming of nondystrophic nails | Routine Foot Care | Q7 / Q8 / Q9 |
| G0127 | Trimming of dystrophic nails (HCPCS) | Routine Foot Care | Q7 / Q8 / Q9 |
| 11720 | Nail debridement, 1 to 5 nails | Nail Procedures | Q7 / Q8 / Q9 |
| 11721 | Nail debridement, 6 or more nails | Nail Procedures | Q7 / Q8 / Q9 |
| 11730 | Avulsion of nail plate, single | Nail Procedures | TA, T1–T9, RT/LT |
| 11732 | Each additional nail avulsion (add-on) | Nail Procedures | TA, T1–T9 |
| 11750 | Permanent nail removal with matrixectomy | Nail Procedures | TA, T1–T9, RT/LT |
| 11755 | Nail biopsy | Nail Procedures | TA, T1–T9 |
| 11765 | Wedge excision, ingrown nail | Nail Procedures | TA, T1–T9, RT/LT |
| 11055 | Paring of single hyperkeratotic lesion | Skin Lesions | Q7 / Q8 / Q9 |
| 11056 | Paring of 2 to 4 lesions | Skin Lesions | Q7 / Q8 / Q9 |
| 11057 | Paring of more than 4 lesions | Skin Lesions | Q7 / Q8 / Q9 |
| 11042 | Debridement, skin and subcutaneous tissue | Wound Care | 59 or XS as needed |
| 11043 | Debridement, muscle and/or fascia | Wound Care | 59 or XS as needed |
| 11044 | Debridement, bone | Wound Care | 59 or XS as needed |
| 11045 | Each additional 20 sq cm, skin/subcut (add-on) | Wound Care | None |
| 11046 | Each additional 20 sq cm, muscle/fascia (add-on) | Wound Care | None |
| 11047 | Each additional 20 sq cm, bone (add-on) | Wound Care | None |
| 97597 | Selective debridement, first 20 sq cm | Wound Care | 59 as needed |
| 97598 | Each additional 20 sq cm selective (add-on) | Wound Care | None |
| 97602 | Non-selective debridement | Wound Care | Often bundled |
| 15271 | Skin substitute graft, ≤100 sq cm (trunk/arms/legs) | Wound Care | RT/LT |
| 15272 | Each additional 25 sq cm (add-on) | Wound Care | None |
| 15275 | Skin substitute graft, ≤100 sq cm (face/hands/feet) | Wound Care | RT/LT |
| 15276 | Each additional 25 sq cm (add-on) | Wound Care | None |
| 20550 | Injection, tendon sheath or ligament | Injections | 25 with same-day E/M |
| 20551 | Injection, tendon origin or insertion | Injections | 25 with same-day E/M |
| 20600 | Small joint aspiration/injection, no imaging | Injections | 25 with same-day E/M |
| 20604 | Small joint aspiration/injection, with ultrasound | Injections | 25 with same-day E/M |
| 20605 | Intermediate joint, no imaging | Injections | 25 with same-day E/M |
| 20606 | Intermediate joint, with ultrasound | Injections | 25 with same-day E/M |
| 20610 | Major joint (ankle), no imaging | Injections | 25 with same-day E/M |
| 20611 | Major joint, with ultrasound | Injections | 25 with same-day E/M |
| 29540 | Strapping, ankle and/or foot | Strapping & Casting | RT/LT |
| 29550 | Strapping, toes | Strapping & Casting | TA, T1–T9 |
| 29515 | Short leg splint application | Strapping & Casting | RT/LT |
| 29405 | Short leg cast application | Strapping & Casting | RT/LT |
| 28470 | Closed treatment, metatarsal fracture, no manipulation | Fracture Care | RT/LT |
| 28475 | Closed treatment, metatarsal, with manipulation | Fracture Care | RT/LT |
| 28485 | Open treatment, metatarsal fracture | Fracture Care | RT/LT |
| 28490 | Closed treatment, great toe, no manipulation | Fracture Care | TA |
| 28495 | Closed treatment, great toe, with manipulation | Fracture Care | TA |
| 28510 | Closed treatment, other phalanx, no manipulation | Fracture Care | T1–T9 |
| 28515 | Closed treatment, other phalanx, with manipulation | Fracture Care | T1–T9 |
| 28289 | Hallux rigidus repair | Surgery | TA, RT/LT |
| 28292 | Bunionectomy with sesamoidectomy (Keller) | Surgery | TA, RT/LT |
| 28296 | Distal metatarsal osteotomy (Austin/Chevron) | Surgery | TA, RT/LT |
| 28297 | Lapidus procedure | Surgery | TA, RT/LT |
| 28298 | Proximal phalanx osteotomy | Surgery | TA, RT/LT |
| 28299 | Double osteotomy | Surgery | TA, RT/LT |
| 28285 | Hammertoe repair, single toe | Surgery | TA, T1–T9 |
| 28286 | Cock-up fifth toe correction | Surgery | T9 |
| 28810 | Amputation, metatarsal with toe | Surgery | TA, T1–T9 |
| 28820 | Amputation, toe at MTP joint | Surgery | TA, T1–T9 |
| 28825 | Amputation, toe at IP joint | Surgery | TA, T1–T9 |
| 28060 | Partial plantar fasciectomy | Surgery | RT/LT |
| 28250 | Division of plantar fascia | Surgery | RT/LT |
| 27650 | Achilles tendon repair | Surgery | RT/LT |
| 28200 | Flexor tendon repair, foot | Surgery | TA, T1–T9 |
| 20680 | Removal of implant, deep | Surgery | 79 if in global period |
| 99202–99205 | New patient office visit (5 levels) | E/M | 25 with same-day procedure |
| 99211–99215 | Established patient office visit (5 levels) | E/M | 25 with same-day procedure |
| 98000–98015 | Telemedicine E/M services (2026 new codes) | E/M | 95 if applicable |
What Are Routine Foot Care CPT Codes?
Medicare excludes routine foot care unless the patient has a qualifying systemic condition that makes professional care medically necessary. Without the right diagnosis, modifier, and documentation, these codes get denied at first review. This section covers the two foundational nail-trimming codes and the medical necessity framework that determines whether either one gets paid.
CPT 11719: Trimming of Nondystrophic Nails
CPT code 11719 covers the trimming of nondystrophic toenails. These are nails that are otherwise normal, with no fungal infection, thickening, or other disease. Medicare considers this routine maintenance and does not pay for it under standard policy.
The code becomes billable only when the patient has a qualifying systemic condition. This means diabetes with peripheral neuropathy, peripheral vascular disease, or one of the Class A, B, or C findings detailed below. Without a Q7, Q8, or Q9 modifier and a linked diagnosis, the claim fails.
Documentation should include the systemic condition, the date of active care with the treating physician, and confirmation that lack of professional trimming poses a risk of complication. Frequency is capped at once every 60 days under most MAC policies.
HCPCS G0127: Trimming of Dystrophic Nails
G0127 is an HCPCS Level II code, not a CPT code. It’s included here because no podiatry coding cheat sheet works without it. The code covers trimming of dystrophic toenails: thickened, deformed, or diseased nails that cannot be cut with standard clippers.
Use G0127 when the patient has both dystrophic nails and a qualifying systemic condition. Apply the same Q7, Q8, or Q9 modifier rules that govern 11719. Document the dystrophy in the chart and link to the systemic diagnosis.
Frequency limits apply. Most MACs cover G0127 once every 60 days unless extended care is documented.
When Routine Foot Care Becomes Billable: Class A, B, and C Findings
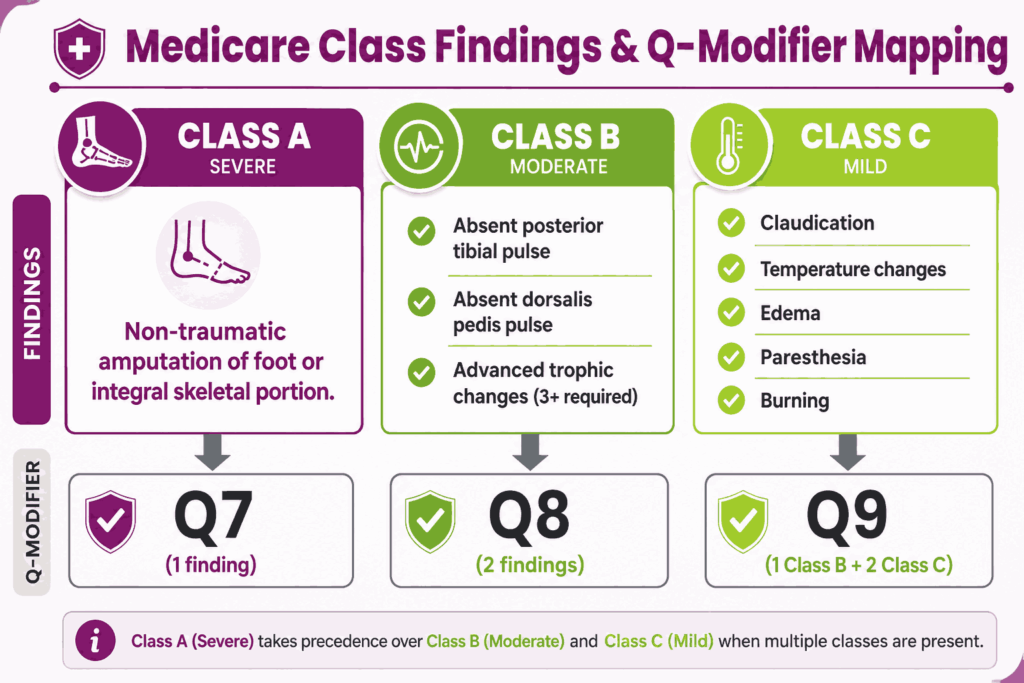
Medicare uses a three-tier classification of findings to determine medical necessity for routine foot care. The class of finding present on the exam determines which Q-modifier must be appended to the claim.
Class A findings are the most severe. They include non-traumatic amputation of the foot or any integral skeletal portion of the foot.
Class B findings are moderate. The list includes absent posterior tibial pulse, absent dorsalis pedis pulse, and advanced trophic changes. Trophic changes include hair growth decrease, nail thickening, skin discoloration, skin texture changes, and skin temperature changes. At least three trophic changes must be present to count as one Class B finding.
Class C findings are mild. These include claudication, temperature changes, edema, paresthesia, and burning sensations.
The findings map to Q-modifiers as follows:
- Q7 = One Class A finding present
- Q8 = Two Class B findings present
- Q9 = One Class B finding plus two Class C findings
Bottom line: no qualifying finding means no Q-modifier, which means no payment for routine foot care codes 11055-11057, 11719, 11720, 11721, and G0127.
What Are Nail Procedure CPT Codes?
Nail procedures are the highest-volume code family in podiatry. They’re also the most scrutinized for medical necessity, modifier accuracy, and frequency limits.
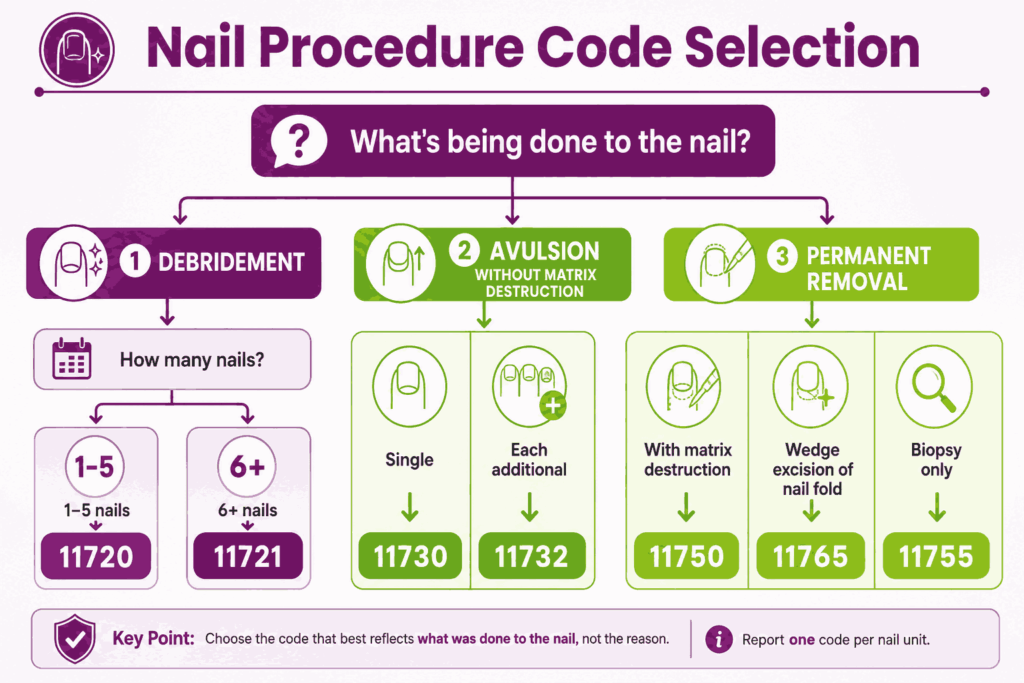
CPT 11720: Nail Debridement, 1 to 5 Nails
CPT code 11720 covers debridement of 1 to 5 toenails by any method. Use procedure code 11720 when nails are thickened, dystrophic, or fungal. Medicare requires Q7, Q8, or Q9 modifier plus a qualifying systemic diagnosis like onychomycosis with diabetes (E11.621). Frequency capped at once every 60 days. Cannot be billed with 11721 on the same date of service.
CPT 11721: Nail Debridement, 6 or More
11721 CPT code covers the debridement of 6 or more toenails in a single session. It’s reported once regardless of how many nails beyond 6 are debrided. Same Q-modifier rules apply: Q7, Q8, or Q9 plus a linked systemic diagnosis. Medicare covers it once every 60 days, which equals six times per year when documented. The code CPT 11721 audit risk is high because payers track frequency tightly.
CPT 11730: Avulsion of Nail Plate (Single)
The code CPT 11730 reports avulsion of a single nail plate, partial or complete, without matrix destruction. Common for ingrown nail relief or trauma. Documentation for the code 11730 CPT must specify which toe is using the TA (great toe) or T1-T9 modifiers, plus RT or LT for laterality. For each additional nail removed in the same session, add 11732 CPT code.
CPT 11732: Each Additional Nail (Add-on)
Add-on code for each additional nail avulsion performed during the same session as 11730. Bill the code 11732 CPT once per extra nail, with toe-specific modifiers (TA, T1-T9). Cannot be billed standalone.
CPT 11750: Permanent Removal With Matrix Destruction
CPT code 11750 description covers permanent removal of a nail and nail matrix, partial or complete. Common for chronic recurrent ingrown nails after conservative treatment fails. Method (chemical or surgical matrixectomy) must be documented along with toe specificity (TA or T1-T9) and laterality (RT/LT). Reported once per digit, even if both medial and lateral matrices are destroyed.
CPT 11755: Nail Biopsy
11755 CPT covers biopsy of the nail unit, including nail plate, bed, matrix, or surrounding tissue. Used for suspected melanoma, fungal culture, or other diagnostic workup. Specimen handling and TA or T1-T9 modifier required.
CPT 11765: Wedge Excision for Ingrown Nail
CPT 11765 code covers wedge excision of the skin of the nail fold for ingrown toenail correction. This addresses soft tissue without destroying the nail matrix. Document the affected toe (TA or T1-T9) and side (RT/LT). Coders often confuse it with 11750.
CPT Codes 11750 vs 11765: When to Use Which
Both codes address ingrown toenails but differ in scope. CPT 11750 destroys the nail matrix, preventing regrowth. CPT 11765 removes only the soft tissue of the nail fold, allowing the nail to regrow. Choose 11750 for chronic recurrent cases. Choose 11765 for first-time correction, where matrix preservation is preferred.
What Are Skin Lesion CPT Codes (Corns, Calluses, Hyperkeratosis) in Podiatry Billing?
Hyperkeratotic lesion codes cover paring of corns and calluses. Like routine nail care, payment hinges on the patient having a qualifying systemic condition.
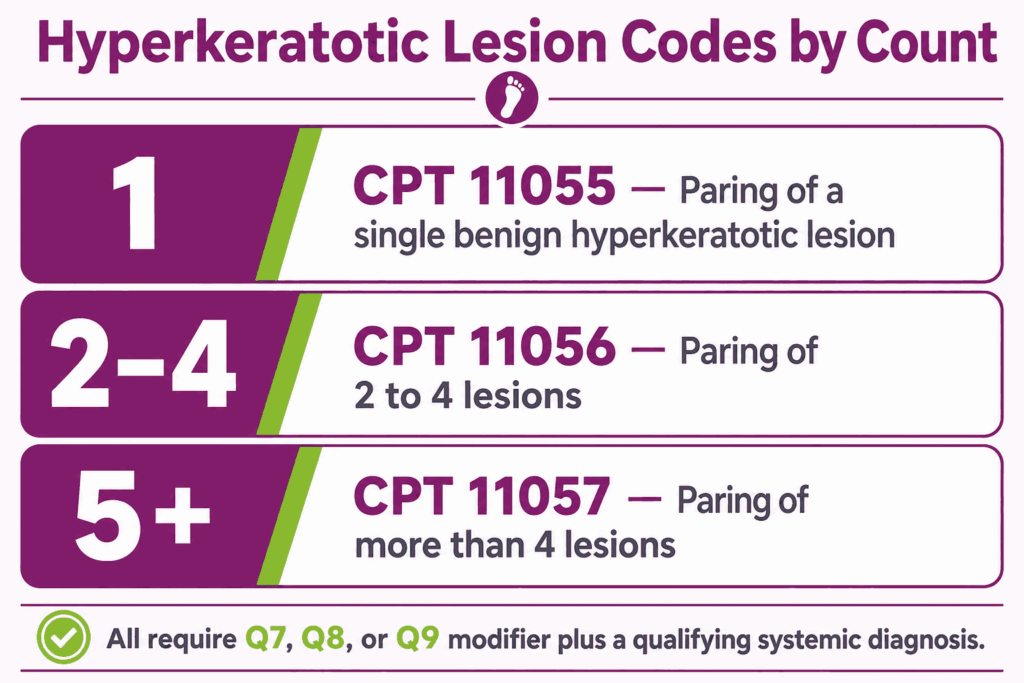
CPT 11055: Single Hyperkeratotic Lesion
CPT code 11055 covers paring or cutting of a single benign hyperkeratotic lesion, such as a corn or callus. Medicare classifies this as routine foot care, requiring Q7, Q8, or Q9 modifier plus a qualifying systemic diagnosis. Documentation should note lesion location, size, and clinical reason for removal. Frequency limits mirror the 60-day routine care rule.
CPT 11056: 2 to 4 Lesions
CPT 11056 code covers paring or cutting of 2 to 4 benign hyperkeratotic lesions. Apply the same Q-modifier and frequency rules as 11055. Document each lesion’s location separately. This code triggers a common NCCI bundling trap with 11305.
CPT 11057: More Than 4 Lesions
CPT 11057 covers paring or cutting of more than 4 benign hyperkeratotic lesions. Bill once per session, regardless of count beyond 4. Same Q-modifier requirements apply.
Mutually Exclusive With 11305: The Bundling Trap
CPT 11056 and 11305 (shaving of epidermal or dermal lesion) cannot be billed together per NCCI edits. They’re considered mutually exclusive procedures. If both are performed, only the higher-RVU code gets paid. Verify NCCI edits before submitting any same-day combination involving hyperkeratotic lesion codes.
What Are the CPT Codes for Wound Care & Debridement?
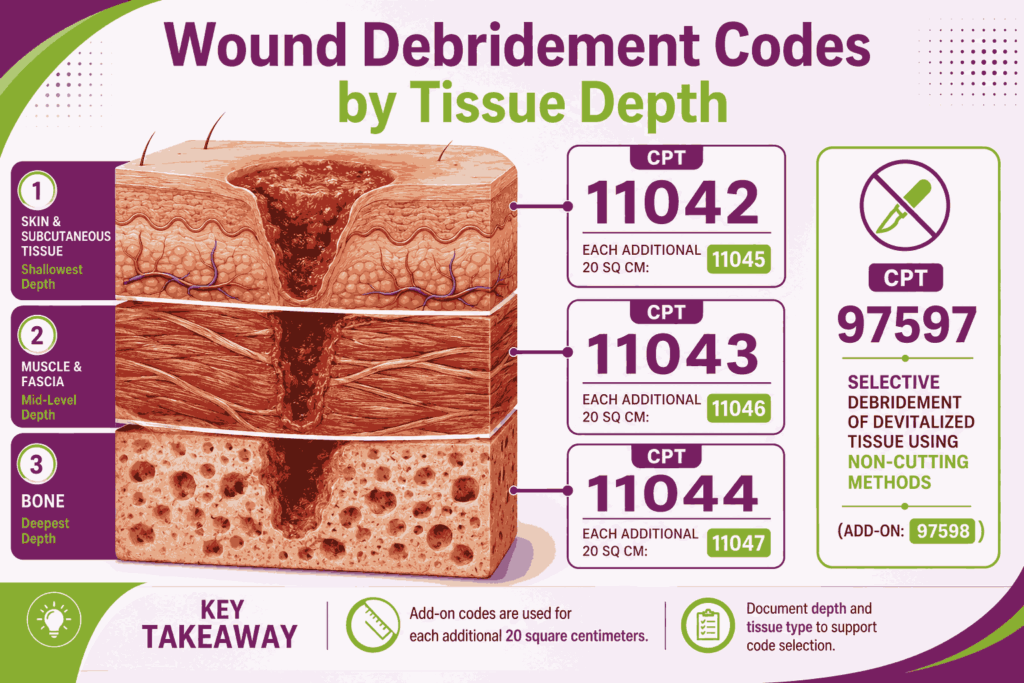
Wound care debridement codes are central to diabetic foot ulcer management. Code selection depends on tissue depth, with add-on codes scaling by surface area in 20 sq cm increments.
CPT 11042: Debridement, Skin and Subcutaneous Tissue
11042 CPT code covers surgical debridement of skin and subcutaneous tissue, first 20 sq cm or less. Critical for diabetic foot ulcers and chronic wounds with necrotic tissue. Documentation must specify wound size in square centimeters, depth of tissue debrided, and tissue removed. Modifier 59 or XS may be needed when billing alongside other procedures on the same anatomic site.
CPT 11043: Debridement, Muscle and/or Fascia
The code CPT 11043 covers surgical debridement extending to muscle or fascia, first 20 sq cm. Used when wounds penetrate deeper than the subcutaneous tissue. Depth determines code selection, not the severity of wound appearance.
CPT 11044: Debridement, Bone
CPT code 11044 covers surgical debridement extending to bone, first 20 sq cm. Reserved for wounds with bone exposure or osteomyelitis treatment. Operative-level documentation required, including bone tissue removed.
CPT 11045 / 11046 / 11047: Add-On Codes for Each Additional 20 sq cm
Three add-on codes pair with their primary debridement counterparts: CPT code 11045 with 11042 (skin/subcutaneous), 11046 CPT with 11043 (muscle/fascia), and procedure code 11047 with 11044 (bone). Report once for each additional 20 sq cm or part thereof. Cannot be billed standalone.
CPT 97597: Selective Debridement, First 20 sq cm
CPT 97597 code covers selective debridement using high-pressure water jet, sharp instruments, or other selective methods. First 20 sq cm of wound area. Documentation must describe the technique used and tissue removed. Most common for outpatient wound care of ulcers.
CPT 97598: Each Additional 20 sq cm
Add-on to 97597 for each additional 20 sq cm of wound area selectively debrided is the 97598 procedure code. Bill alongside the primary code, not standalone.
CPT Codes 97597 vs 11042: Selection Logic
Both codes debride wound tissue, but the distinction matters for reimbursement. CPT 11042 is a surgical debridement of viable tissue, typically performed in operative settings with higher RVUs. CPT 97597 is the selective debridement of devitalized tissue using non-cutting methods. Use 11042 when the procedure requires sharp surgical excision. Use 97597 for routine wound bed preparation.
CPT 97602: Non-Selective Debridement
CPT code 97602 covers non-selective debridement using wet-to-dry dressings, enzymatic methods, or abrasion. Most payers bundle this code with E/M services or other wound care. Rarely paid as a standalone procedure.
CPT 15271 & 15272: Skin Substitute Graft, Trunk/Arms/Legs
CPT 15271 code covers the application of skin substitute graft to wounds up to 100 sq cm on the trunk, arms, or legs. The code CPT 15272 is the add-on for each additional 25 sq cm. Used for chronic non-healing diabetic foot ulcers and venous stasis ulcers. Document wound preparation, graft product NDC, and surface area applied.
CPT 15275 & 15276: Skin Substitute Graft, Face/Hands/Feet
15275 CPT code description covers skin substitute graft application to wounds up to 100 sq cm on the face, hands, feet, or genitals. CPT code 15276 is the add-on for each additional 25 sq cm. This is the primary graft code podiatrists use for foot ulcers. Documentation rules mirror 15271 and 15272.
What Are Injection CPT Codes for Podiatry?
Injection codes are split by joint size and the presence of imaging guidance. Modifier 25 applies when E/M is billed on the same day.
CPT 20550: Tendon Sheath or Ligament
CPT 20550 code covers an injection into a single tendon sheath or ligament. The most common podiatry use is plantar fasciitis treatment with corticosteroids. Document the anatomic site injected, drug administered with NDC, and dose. Modifier 25 is required when billing alongside same-day E/M. Multiple injections at different sites need a modifier 59 or the appropriate X-modifier.
CPT 20551: Tendon Origin/Insertion
CPT code 20551 covers injection at the origin or insertion of a tendon, not the sheath itself. Used for Achilles tendinopathy and similar insertional conditions. It is often confused with the 20550 procedure code.
CPT Codes 20550 vs 20551: When to Use Which
The distinction is anatomic. CPT 20550 targets the tendon sheath, the protective sleeve surrounding the tendon. CPT 20551 targets the bony attachment point where the tendon originates or inserts. Plantar fasciitis typically uses 20550. Insertional Achilles tendinopathy uses 20551.
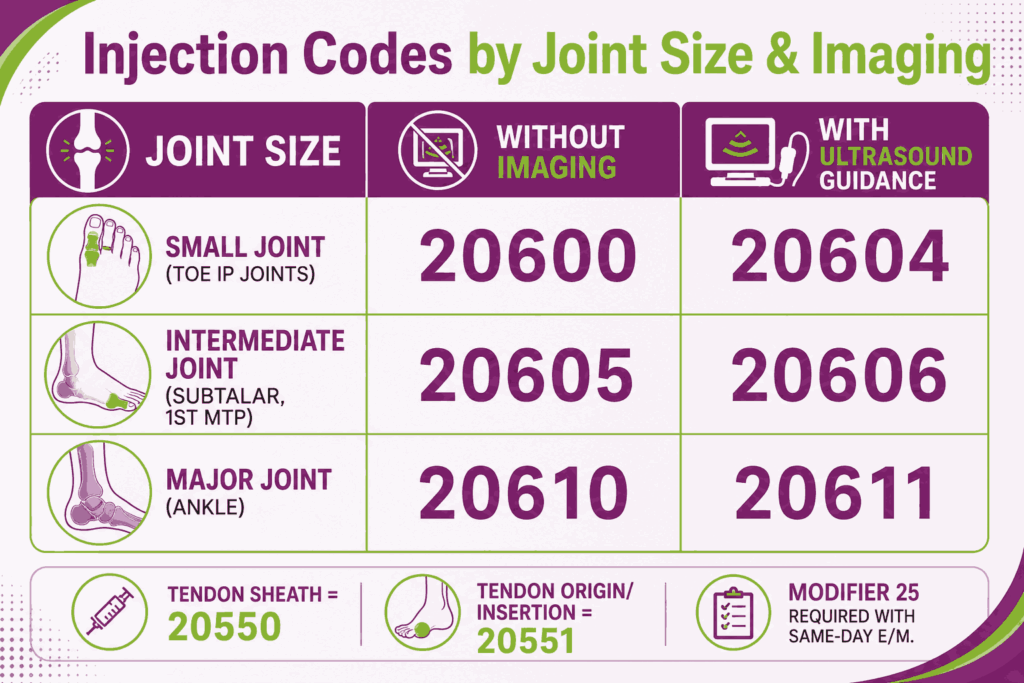
CPT 20600 & 20604: Small Joint Injection
CPT 20600 covers aspiration or injection of a small joint without imaging guidance, used for interphalangeal joints of the toes. Moreover, CPT 20604 code covers the same procedure with ultrasound guidance and permanent imaging documentation. The imaging record must be saved in the patient’s chart for 20604.
CPT 20605 & 20606: Intermediate Joint Injection
20605 CPT covers aspiration or injection of an intermediate joint without imaging guidance, typically the subtalar or first MTP joint. CPT code 20606 covers the same procedure with ultrasound guidance. The same imaging documentation rule applies.
CPT 20610 & 20611: Major Joint (Ankle), With/Without Imaging Guidance
The code CPT 20610 covers aspiration or injection of a major joint (the ankle in podiatry) without imaging guidance. 20611 CPT code is the same procedure with ultrasound guidance and permanent imaging recording. Document the joint injected, substance administered with NDC code, volume, and date of service. Modifier 25 required for same-day E/M. CPT 20611 captures higher reimbursement and is often underused when ultrasound is available.
What Are Strapping, Splinting & Casting CPT Codes in Podiatry?
Strapping, splinting, and casting codes cover non-surgical immobilization of the foot and ankle. Supply codes are billed separately under HCPCS.
CPT 29540: Strapping, Ankle/Foot
CPT code 29540 covers the application of strapping to the ankle and/or foot. Used for sprains, plantar fasciitis, and post-injection support. Document the anatomic area strapped and clinical indication. Modifier RT or LT specifies the side.
CPT 29550: Strapping, Toes
CPT 29550 code covers strapping of the toes, commonly for buddy taping or post-fracture support. Toe-specific modifier (TA or T1-T9) required for laterality.
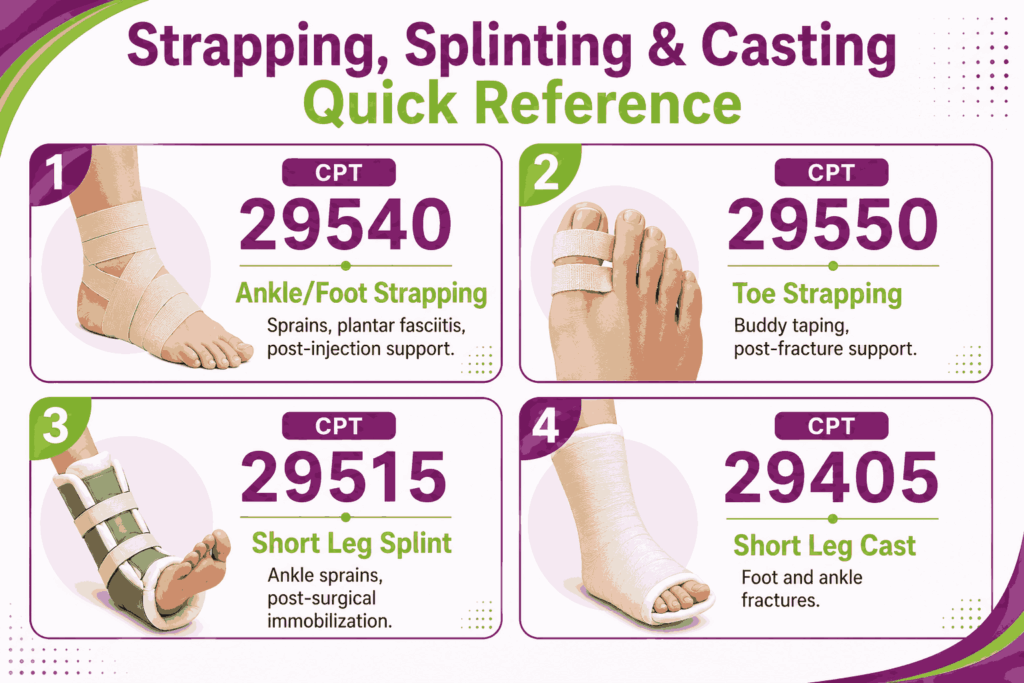
CPT 29515: Short Leg Splint
CPT 29515 covers the application of a short leg splint from below the knee to the toes. Used for ankle sprains, fractures, and post-surgical immobilization. Document material, anatomic position, and clinical indication. Modifier RT or LT required.
CPT 29405: Short Leg Cast
CPT 29405 covers the application of a short leg cast from below the knee to the toes. Used for ankle and foot fractures or post-surgical immobilization. Cast supply codes (Q4037, Q4038, and others) are billed separately under HCPCS. Modifier RT or LT required.
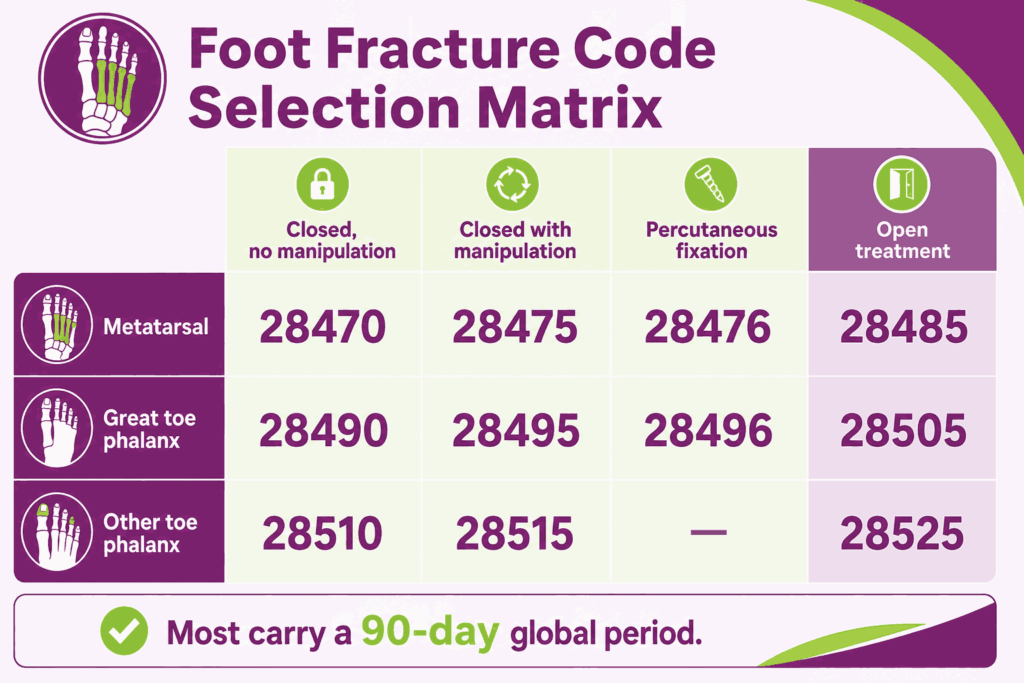
What Are Foot & Ankle Fracture Care CPT Codes
Fracture care codes are split by anatomic location, treatment type (closed vs open), and whether manipulation was performed. Most fracture codes carry a 90-day global period.
CPT 28470 & 28475: Metatarsal Fracture, Closed
CPT code 28470 covers closed treatment of a metatarsal fracture without manipulation. The code CPT 28475 covers the same fracture treated closed with manipulation. Document fracture location, mechanism of injury, imaging findings, and immobilization method. Modifier RT or LT required for laterality.
CPT 28476: Metatarsal Fracture, Percutaneous Fixation
28476 CPT code covers percutaneous skeletal fixation of a metatarsal fracture with manipulation, using pins or screws placed through the skin. Sits between closed treatment (28475) and open treatment (28485) in invasiveness. Documentation must specify the fixation method and imaging guidance if used. Modifier RT or LT required.
CPT 28485: Metatarsal Fracture, Open Treatment
CPT code 28485 covers open treatment of a metatarsal fracture with or without internal fixation. Operative-level documentation required, including approach, fixation hardware, and post-op plan. Higher RVU and 90-day global period apply.
CPT 28490 & 28495: Great Toe Fracture, Closed
CPT 28490 code covers closed treatment of a great toe phalangeal fracture without manipulation. The procedure code 28495 covers the same fracture with manipulation. For percutaneous skeletal fixation with manipulation, use 28496 CPT code instead. Document fracture location, displacement, and immobilization. Modifier TA required for great toe specificity.
CPT 28505: Great Toe Fracture, Open Treatment
CPT 28505 covers open treatment of a great toe phalangeal fracture, including internal fixation when performed. Used for displaced or non-healing fractures. Operative-level documentation required, including approach, fixation hardware, and post-op plan. Modifier TA required.
CPT 28510 & 28515: Other Phalangeal Fracture, Closed
CPT 28510 code description covers closed treatment of a phalangeal fracture in toes other than the great toe, without manipulation. Plus, CPT 28515 covers the same fracture with manipulation. Modifier T1 through T9 is required to specify the affected toe.
Global Periods at a Glance
Most foot and ankle fracture codes carry a 90-day global period. Follow-up visits within that window cannot be billed separately unless documented as unrelated to the fracture. Use modifier 79 for unrelated procedures during the global period. Use modifier 24 for unrelated E/M during the global period.
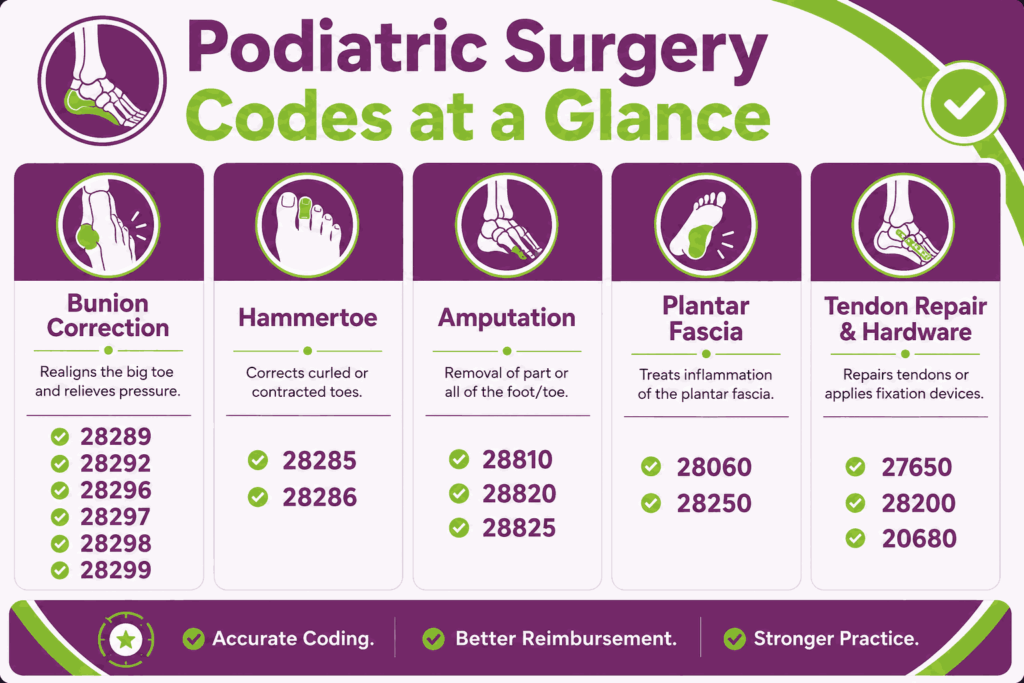
What Are Podiatric Surgery CPT Codes
Surgical codes carry the highest RVUs and audit weight in podiatry. Operative notes must specify procedure, anatomic site, hardware, and digit treated. Most carry a 90-day global period.
Bunion Correction CPT Codes
Bunion correction codes are split by surgical technique and anatomic location. Choice depends on deformity severity, joint involvement, and fixation needs.
CPT 28289: Hallux Rigidus Repair
CPT 28289 code covers cheilectomy for hallux rigidus (arthritic stiffening of the first MTP joint). Includes osteophyte removal and joint debridement. Modifier TA required, RT or LT for laterality.
CPT 28292: Bunionectomy With Sesamoidectomy (Keller)
CPT code 28292 covers the Keller bunionectomy with sesamoidectomy and proximal phalanx resection. Used for severe bunion deformity in elderly or low-demand patients. Prior authorization is commonly required. Modifier TA and RT/LT required.
CPT 28296: Distal Metatarsal Osteotomy (Austin/Chevron)
The code CPT 28296 covers the Austin or Chevron bunionectomy with distal first metatarsal osteotomy. The most common bunion correction billed in podiatry. Document osteotomy type, fixation method, and hardware used. Pre-op imaging and surgical intent must be in the chart. Modifier TA and RT/LT required.
CPT 28297: Lapidus Procedure
CPT 28297 code covers the Lapidus procedure (first tarsometatarsal joint arthrodesis with bunionectomy). Used for severe bunion deformity with hypermobility. Higher complexity and RVU than 28296. Modifier TA and RT/LT required.
CPT 28298: Proximal Phalanx Osteotomy
28298 code CPT covers bunionectomy with proximal phalanx osteotomy (Akin procedure). Often performed in combination with 28296 for combined deformity correction. When billed together, modifier 59 or the appropriate X-modifier applies.
CPT 28299: Double Osteotomy
Code 28299 CPT covers bunionectomy with double osteotomy of the first metatarsal. Used for severe deformities requiring correction at two anatomic levels. Highest RVU in the bunion correction series.
Hammertoe Repair CPT Codes
Hammertoe codes are billed per toe corrected. Toe-specific modifiers are required and frequently audited.
CPT 28285: Hammertoe, Single Toe
CPT code 28285 covers hammertoe correction of a single toe by any method (arthroplasty, fusion, or tenotomy). Bill once per toe corrected, with separate T1-T9 modifiers. Document the procedure method, fixation if used, and digit treated. The 28285 CPT code is a frequently audited code, so notes must be thorough.
CPT 28286: Cock-up Fifth Toe
CPT 28286 code covers the correction of a cock-up deformity of the fifth toe. Use only for the fifth toe; other toes use 28285. Modifier T9 required.
Amputation CPT Codes
Amputation codes vary by anatomic level. Documentation must specify the level, indication, and digit involved.
CPT 28810: Metatarsal With Toe
CPT code 28810 covers amputation through the metatarsal with the corresponding toe (ray amputation). Used for severe diabetic foot infections, ischemia, or trauma. Operative-level documentation required. Modifier TA or T1-T9 plus RT/LT required.
CPT 28820: Toe at MTP Joint
CPT 28820 covers amputation of a toe disarticulated at the metatarsophalangeal (MTP) joint. Document the toe, indication, and surgical approach. Modifier TA or T1-T9 plus RT/LT required.
CPT 28825: Toe at IP Joint
The code CPT 28825 covers amputation of a toe at the interphalangeal (IP) joint, preserving the proximal phalanx. Documentation rules mirror 28820. Modifier TA or T1-T9 plus RT/LT required.
Plantar Fascia & Soft Tissue CPT Codes
Plantar fascia surgery codes address chronic plantar fasciitis that has failed conservative treatment.
CPT 28060: Partial Plantar Fasciectomy
CPT code 28060 covers a partial plantar fasciectomy, removing a portion of the plantar fascia. Used for chronic plantar fasciitis when conservative treatment has failed. Document conservative care history and clinical justification. Modifier RT or LT required.
CPT 28250: Division of Plantar Fascia
CPT 28250 code covers the division of the plantar fascia and muscle (open). Used for severe contracture cases. Lower complexity than 28060, but still requires conservative care documentation. Modifier RT or LT required.
Tendon Repair CPT Codes
Tendon repair codes are billed by anatomic location and approach (primary, secondary, or delayed).
CPT 27650: Achilles Tendon Repair
27650 CPT covers the primary repair of a ruptured Achilles tendon. Used for acute ruptures within the surgical window. Document mechanism, time from injury, and repair technique. 90-day global period applies. Modifier RT or LT required.
CPT 28200: Flexor Tendon Repair (Foot)
Code CPT 28200 covers repair, primary or secondary, of a flexor tendon in the foot without graft. Used for traumatic lacerations or chronic ruptures. Modifier TA or T1-T9 plus RT/LT required.
CPT 20680: Hardware Removal
CPT code 20680 covers deep removal of orthopedic implants (screws, plates, or pins). Most commonly billed after bunion or fracture surgery. If performed during the global period of the original procedure, modifier 79 is required to indicate an unrelated procedure.
Evaluation & Management (E/M) CPT Codes for Podiatry
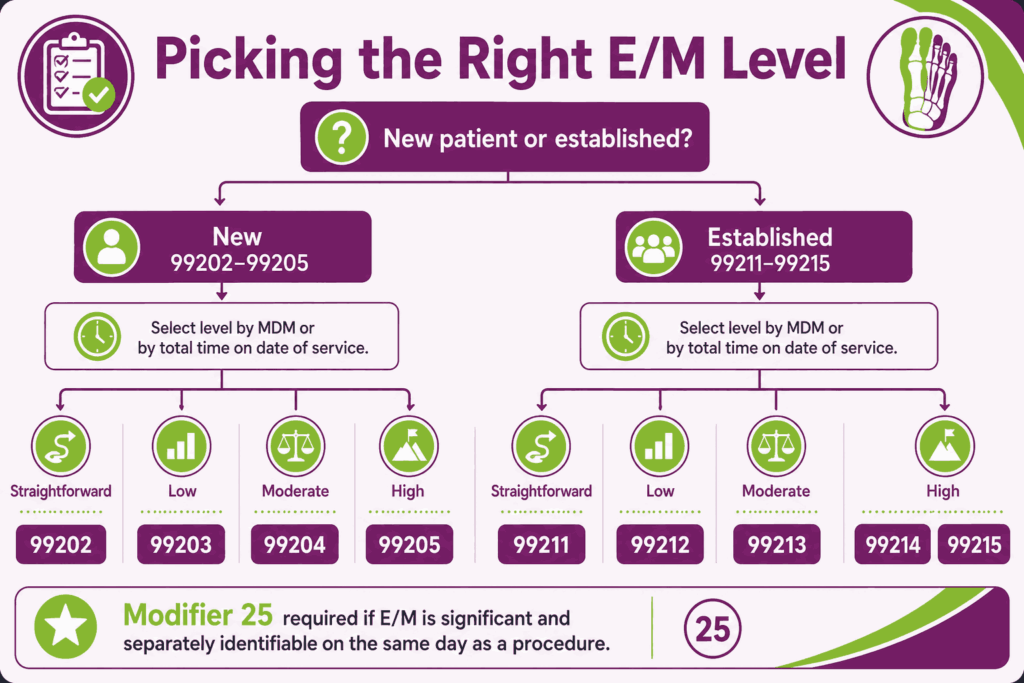
E/M codes for podiatry follow standard outpatient guidelines (99202–99215). Level selection is based on medical decision-making (MDM) or total time, not the legacy history/exam/MDM combination.
New Patient Visits (99202–99205)
Use new patient codes when the patient has not received professional services from any provider in the same group practice and specialty within the past three years.
| Code | MDM Level | Total Time |
|---|---|---|
| 99202 | Straightforward | 15–29 min |
| 99203 | Low | 30–44 min |
| 99204 | Moderate | 45–59 min |
| 99205 | High | 60–74 min |
Established Patient Visits (99211–99215)
Use established patient codes for return visits within three years from the same specialty.
| Code | MDM Level | Total Time |
|---|---|---|
| 99211 | Minimal (no provider needed) | N/A |
| 99212 | Straightforward | 10–19 min |
| 99213 | Low | 20–29 min |
| 99214 | Moderate | 30–39 min |
| 99215 | High | 40–54 min |
CPT Codes 99213 vs 99214: Where Most Podiatry Visits Land
Most podiatry visits land between 99213 and 99214. The distinction comes down to MDM complexity. A CPT code 99213 routine follow-up (stable diabetic foot exam, callus management, routine nail care evaluation) maps to low complexity. A 99214 CPT code (new wound, infection workup, new injection decision, or surgery planning) maps to moderate complexity. Time-based coding offers an alternative when MDM is borderline.
Picking the Level: Medical Decision-Making vs Total Time
CMS allows two methods for selecting an E/M level: medical decision-making (MDM) or total time on the date of encounter. MDM evaluates the number and complexity of problems, the data reviewed, and the risk of complications. Time includes face-to-face care plus pre- and post-visit on the same date. Pick the method that supports the higher legitimate level.
Billing E/M Same Day as a Procedure (Modifier 25)
When an E/M service is provided on the same day as a procedure, modifier 25 must be appended to the E/M code. The E/M must be significant and separately identifiable from the procedure. Document a distinct chief complaint, exam findings, and MDM beyond the procedure. The 2025 OIG audit found 44% of sampled podiatry modifier 25 claims failed compliance, so documentation rigor is critical.
Telemedicine E/M Codes 98000–98015 (2026 Update)
The AMA introduced new telemedicine E/M codes for 2025–2026, replacing the 99441–99443 audio-only and 99201-series telehealth structure. The 98000–98007 series covers synchronous audio-video new and established patient visits. 98008–98015 covers audio-only and other variations. Podiatry telemedicine is limited but billable for follow-up consultations and post-op check-ins.
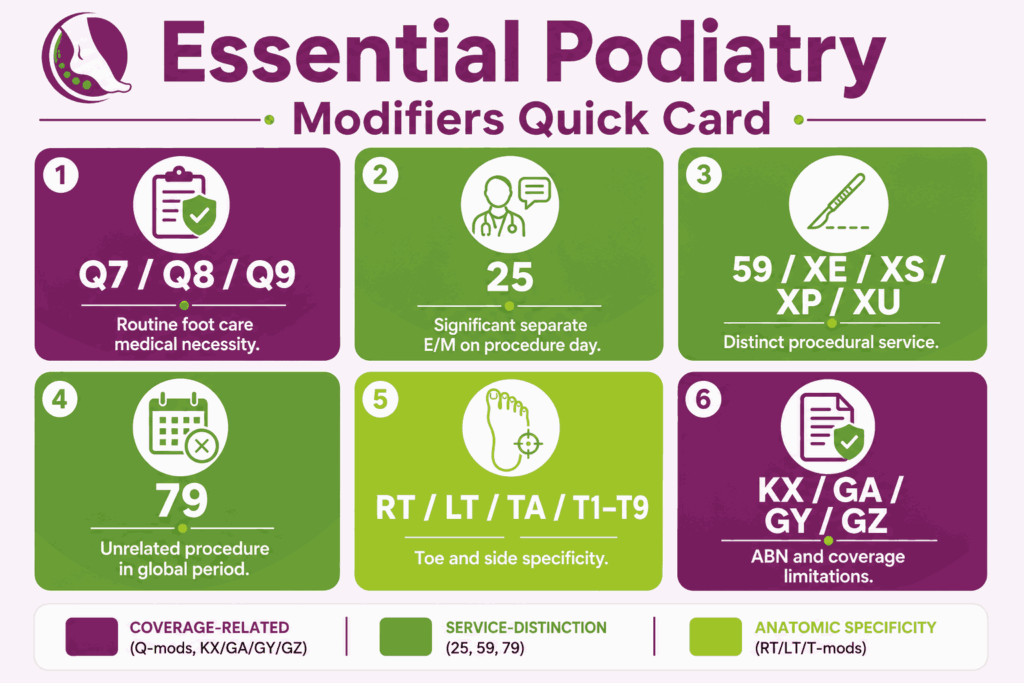
Essential Podiatry Modifiers: Quick Reference
Modifiers tell payers when a service was unusual, separate, or anatomically specific. The following are the most-used podiatry modifiers.
Q7, Q8, Q9: Routine Foot Care Medical Necessity
Required for any routine foot care code (11055–11057, 11719–11721, G0127).
Q7 = one Class A finding.
Q8 = two Class B findings.
Q9 = one Class B finding plus two Class C findings.
Modifier 25: Separate E/M on Procedure Day
Append to the E/M code when a significant, separately identifiable E/M is performed on the same day as a procedure. The audit risk is high in podiatry. Document a distinct chief complaint, exam, and MDM beyond the procedure itself.
Modifier 59 (and XE/XS/XP/XU): Distinct Procedural Service
Use to indicate that two procedures normally bundled together were distinct (different anatomic site, separate encounter, or different patient session). CMS prefers the X-modifiers when applicable: XE (separate encounter), XS (separate structure), XP (separate practitioner), XU (unusual non-overlapping service).
Modifier 79: Unrelated Procedure in Global Period
Use modifier 79 when an unrelated procedure is performed during another procedure’s global period. Common in podiatry when a different surgery is needed during a 90-day global window. Resets the global period for the new procedure.
RT, LT, and T-Modifiers (TA, T1–T9): Toe & Side Specificity
RT and LT specify the right or left foot. T-modifiers specify the individual toe:
TA = left great toe
T1–T4 = left toes 2–5
T5 = right great toe
T6–T9 = right toes 2–5.
Apply to any code involving a specific digit.
KX, GA, GY, GZ: ABN and Coverage Limitations
KX = service meets specific medical policy requirements.
GA = ABN on file for a service likely to be denied.
GY = service statutorily excluded (used to trigger patient liability).
GZ = expected to be denied as not medically necessary, no ABN on file (no payment expected).
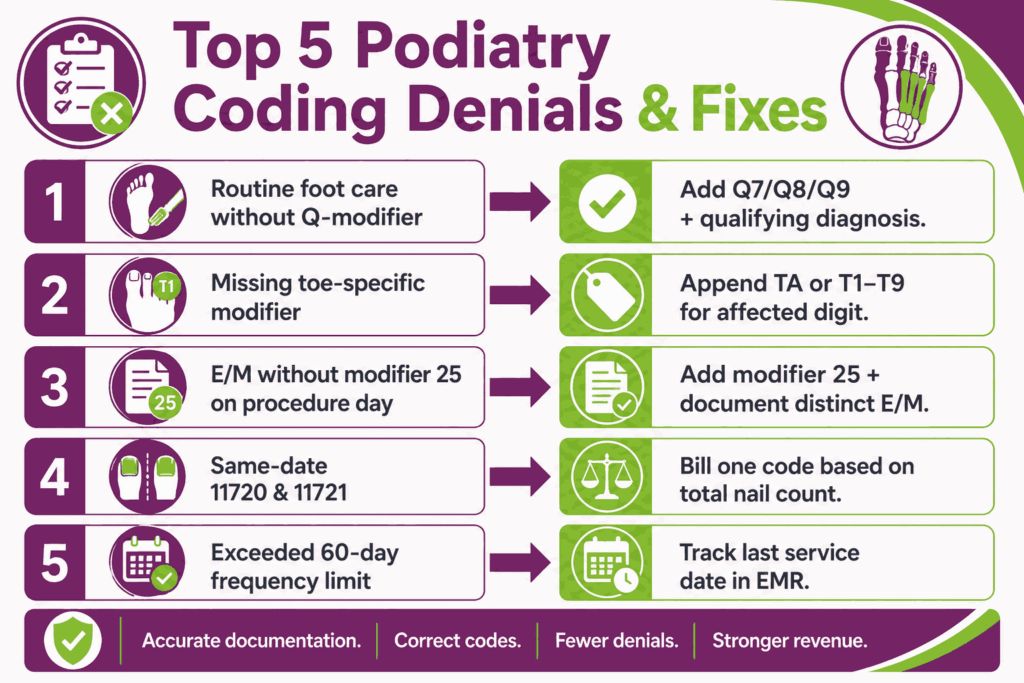
Common Podiatry Coding Errors & Denial Reasons (With Fixes)
Most podiatry denials trace back to a small set of recurring errors. Each one has a known fix. The following are the highest-frequency coding mistakes flagged in payer audits.
Routine Foot Care Billed Without Q-Modifier
The Error: Billing 11055–11057, 11719–11721, or G0127 without Q7, Q8, or Q9. Medicare automatically rejects these as routine care without medical necessity.
Fix: Add the appropriate Q-modifier and link to a qualifying systemic ICD-10 diagnosis. Document the Class A/B/C finding in the chart.
Missing Toe-Specific Modifier (T1–T9, TA)
The Error: Billing toe-specific procedures (28285, 28810, 11750, and others) without a T-modifier indicating which toe was treated. Claims get denied or downcoded.
Fix: Append TA for left great toe, T5 for right great toe, or T1–T9 for other toes. Add RT or LT for laterality where required.
E/M Billed Without Modifier 25 on Procedure Day
The Error: Billing an E/M code alongside a same-day procedure without modifier 25. Medicare bundles the E/M into the procedure RVU and zeros out the E/M payment.
Fix: Add modifier 25 only when E/M is significant and separately identifiable. Document a chief complaint, exam, and MDM distinct from the procedure.
CPT Codes 11720 and 11721 Billed Same Date
The Error: Billing both nail debridement codes on the same date of service. These codes are mutually exclusive: 11720 covers 1–5 nails, 11721 covers 6 or more. The total nail count determines which code applies.
Fix: Pick one code based on the total nails debrided, not both.
Mutually Exclusive Code Pairs (NCCI Edits)
The Error: Billing two procedures that NCCI flags as mutually exclusive. Common examples include 11056 with 11305 (paring vs shaving lesions) and 11042 with 97597 on the same site.
Fix: Check NCCI edits before submission. If both services are clinically warranted on different sites, use modifier 59 or the appropriate X-modifier.
Exceeding the 60-Day Frequency Limit
The Error: Billing routine foot care codes (11720, 11721, G0127, 11055–11057) more often than once every 60 days. Medicare caps these services at six times per year. Claims beyond the limit get denied as exceeding medical necessity.
Fix: track each patient’s last service date in the EMR and flag visits within the 60-day window.
Global Period Violations
The Error: Billing follow-up visits or related procedures inside another procedure’s 90-day global period. Medicare considers these bundled into the original procedure.
Fix: Use modifier 79 for unrelated procedures and modifier 24 for unrelated E/M during the global period. Document clearly why the new service is unrelated to the original surgery.
Missing Medical Necessity Linkage
The Error: Submitting a claim without an ICD-10 code that supports the procedure. Common in routine foot care, where the systemic diagnosis (E11.621 for diabetes with foot complications) is missing.
Fix: Every CPT code on the claim should link to a supporting ICD-10 code for podiatry. No diagnosis means no payment.
New vs Established Patient Misclassification
The Error: Billing a new patient code (99202–99205) when the patient has been seen by another provider in the same group practice and specialty within three years.
Fix: Confirm the three-year, same-group, same-specialty rule before selecting the code. When in doubt, use established patient codes (99211–99215).
Wrong Laterality Coding (RT/LT Errors)
The Error: Missing or incorrect RT/LT modifier on procedures performed on a specific foot. Common when documentation says “right” but the claim shows LT, or no laterality is appended at all.
Fix: Cross-check the operative note against the claim before submission. Bilateral procedures need both RT and LT or modifier 50, depending on payer rules. Because managing these intricate multi-layered modifiers across daily high-volume encounters strains in-house staff, many practices delegate their revenue cycles to specialized Podiatry billing companies to protect their cash flow and guarantee audit defense.
Documentation Gaps That Trigger Audits
The Error: Incomplete documentation that fails to support the billed code level or modifier usage. Audit triggers include missing wound dimensions for debridement codes and no lesion count for paring codes. Other triggers are missing toe-specific notation on surgical codes and absent pre/post-op diagnoses on operative notes.
Fix: Build required fields into software workflows so providers cannot close encounters without them. Utilizing one of the top EMRs for podiatry can significantly mitigate this risk, as these specialty-specific platforms feature built-in smart templates that force compliant documentation selections before a chart can be finalized.
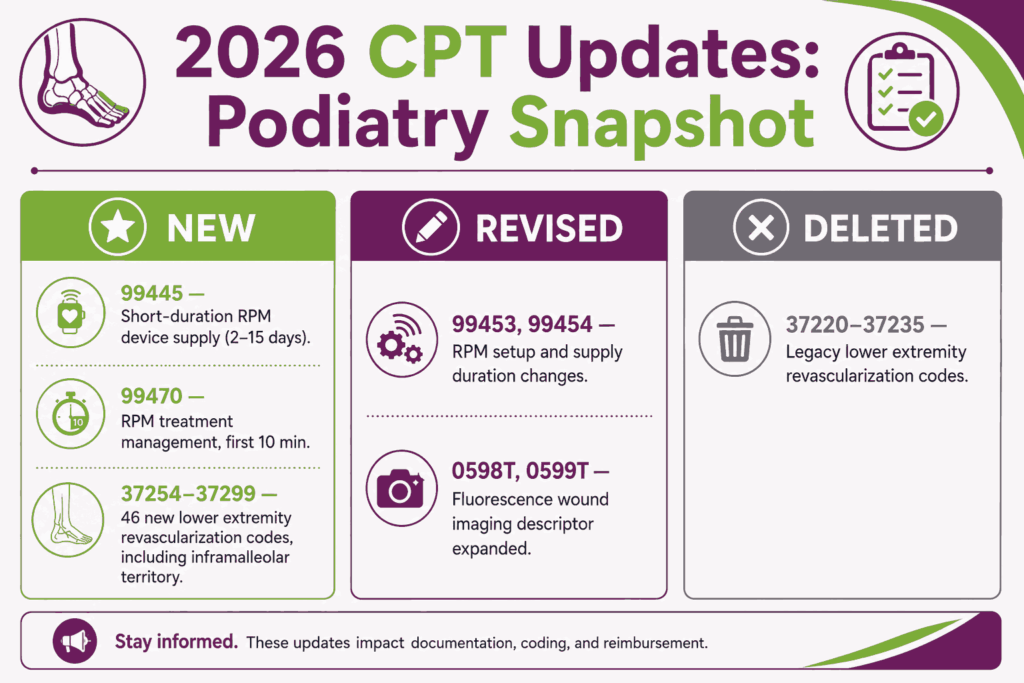
What Are the 2026 CPT Code Updates Affecting Podiatry
The CPT 2026 code set took effect January 1, 2026. The full update includes 288 new codes, 46 revisions, and 84 deletions, but most core podiatry codes remained unchanged. The changes most relevant to podiatry practices are below.
New Codes
The biggest additions affecting podiatry are in remote monitoring and the rebuilt lower extremity revascularization family.
- CPT 99445: Remote physiologic monitoring device supply, 2–15 days within a 30-day period
- CPT 99470: Remote physiologic monitoring treatment management, first 10 minutes per calendar month
- CPT 37254–37299: 46 new territory-based lower extremity revascularization codes, including a new inframalleolar territory (dorsalis pedis, plantar) with specific codes for angioplasty
The shorter-duration RPM codes (99445, 99470) are useful for diabetic foot ulcer monitoring and post-op tracking. The inframalleolar revascularization codes capture procedures performed below the ankle that previously had no clean billing pathway.
Revised Codes
Key revisions affecting podiatry workflow:
- CPT 99453: RPM setup and patient education now submittable for monitoring of 2 or more days (was 16+ days)
- CPT 99454: RPM device supply now specifies 16–30 days (was generic every 30 days)
- CPT 0598T: Fluorescence wound imaging no longer requires “noncontact”; revised descriptor includes clinical darkness and wound size measurement
- CPT 0599T: Add-on to 0598T, mirrors the same revisions
The 0598T and 0599T revisions matter for advanced diabetic wound imaging workflows. The RPM revisions pair with new code 99445 to unlock shorter-duration monitoring billing.
Deleted Codes
The deletions most relevant to podiatry:
- CPT 37220–37235: Legacy lower extremity revascularization codes deleted and replaced by the new 37254–37299 territory-based family
If your practice or any associated vascular team billed 37220–37235 codes in 2025, those claims now require remapping to the new 2026 codes. Most core podiatry CPT codes (nail, lesion, debridement, surgery, E/M) saw no changes.
FAQs
What Is the Most Common CPT Code in Podiatry?
CPT 11721 (nail debridement of 6 or more nails) and CPT 11720 (debridement of 1–5 nails) are the highest-volume codes in most podiatry practices. CPT 20610 (major joint ankle injection) and CPT 99213 (established patient E/M) also rank near the top. Volume varies by patient mix and specialty focus.
Can I Bill CPT Codes 11720 and 11721 on the Same Day?
No, CPT 11720 (1–5 nails) and 11721 (6 or more) are mutually exclusive on the same date of service. The total nail count debrided in the session determines which code applies. Bill 11720 if 5 or fewer nails were debrided; bill 11721 if 6 or more.
How Often Does Medicare Cover Nail Debridement?
Medicare covers nail debridement (11720, 11721) once every 60 days, which equals six times per year. The patient must have a qualifying systemic condition documented and a Q7, Q8, or Q9 modifier on the claim. Claims billed before the 60-day window get denied as exceeding medical necessity.
What Modifier Do I Use for Routine Foot Care?
Use Q7, Q8, or Q9 depending on the patient’s clinical findings. Q7 = one Class A finding (e.g., non-traumatic amputation). Q8 = two Class B findings (e.g., absent pulses, advanced trophic changes). Q9 = one Class B finding plus two Class C findings (e.g., burning, numbness, edema).
Can I Bill an E/M Visit With a Procedure on the Same Day?
Yes, but only with modifier 25 and only if the E/M is significant and separately identifiable from the procedure. The documentation must show a distinct chief complaint, exam, and medical decision-making beyond what the procedure required. If the E/M is only for the procedure itself, it is not separately payable.
What’s the Difference Between 11750 and 11765?
CPT 11750 destroys the nail matrix, preventing nail regrowth. CPT 11765 removes only the soft tissue of the nail fold, allowing the nail to grow back. Use 11750 for chronic recurrent ingrown nails after conservative treatment fails. Use 11765 for first-time correction where matrix preservation is preferred.
Are Podiatry Telemedicine Visits Billable in 2026?
Yes, the 98000–98015 telemedicine E/M code family introduced in 2025–2026 covers synchronous audio-video and audio-only podiatry visits. Coverage is limited compared to in-person care but applies to follow-up consultations, post-op check-ins, and wound monitoring discussions. Payer-specific rules apply, and modifier 95 may be required.






