Psychiatry practices operate in one of the most complex billing environments in healthcare. Behavioral health claims carry initial denial rates in the 10 to 20 percent range. Higher-risk segments such as SUD, IOP/PHP, and carve-out-heavy commercial plans reach the upper end. For a mid-sized psychiatry practice, the difference between an 8 percent and 15 percent denial rate can translate into six to seven figures in annual revenue impact.
Several 2026 regulatory changes are increasing the cost of process failure. The MHPAEA 2024 Final Rule introduced new parity requirements with phased applicability dates across 2025 and 2026. Although enforcement of the new provisions has been paused at the federal level since May 2025, CAA 2021 obligations and state-level enforcement remain active.
At the same time, 42 CFR Part 2 alignment with HIPAA reached its February 16, 2026, compliance deadline, shifting SUD consent rules toward a single TPO consent model. CMS also finalized new APCM behavioral health add-on codes for CY 2026, creating additional reimbursement opportunities for integrated behavioral care.
This guide covers psychiatry billing operations end-to-end, including workflow, payer behavior, documentation standards, denials, A/R, compliance, credentialing, and outsourcing. For CPT codes, modifiers, and ICD-10 specificity, see the psychiatry coding guide.
What Is Psychiatry Billing?
Psychiatry billing is the full revenue cycle process for services delivered by psychiatrists, psychiatric nurse practitioners (PMHNPs), psychologists, LCSWs, LPCs, and LMFTs. It covers scheduling, eligibility, prior authorization, charge capture, claim submission, payment posting, denial management, and patient collections.
The scope goes beyond therapy session billing. Psychiatry practices bill for diagnostic evaluations (90791, 90792), psychotherapy (90832, 90834, 90837), E/M for medication management (99213–99215), psychotherapy add-on codes (90833, 90836, 90838), crisis intervention, collaborative care (99492–99494, G2214), APCM behavioral health add-ons (G0568–G0570), psychological testing (96130–96139), telehealth, and interactive complexity (90785).
Psychiatry billing also differs operationally from general behavioral health billing. Psychiatry includes prescriber-only codes, heavier Medicare and Medicare Advantage exposure, combined E/M plus psychotherapy billing complexity, and higher audit risk on 90837 and same-day stacked codes.
This guide focuses on the operational and revenue cycle side of psychiatry billing.
How Psychiatry Billing Differs From General Behavioral Health Billing
General behavioral health billing typically covers therapists, counselors, and social workers billing standalone psychotherapy codes. Psychiatry adds prescriber-only services that change the billing structure entirely.
Psychiatrists and PMHNPs bill E/M codes plus add-on psychotherapy codes (99214 + 90833) for combined visits, while LCSWs and LPCs bill standalone therapy codes. The combined E/M plus psychotherapy claim requires modifier -25, separate time documentation for each service, and distinct clinical content. Payer scrutiny on these stacked claims is significantly higher than on standalone therapy claims.
Psychiatry practices also carry a heavier Medicare and Medicare Advantage patient mix, often representing 35–55% of total volume. Medication management visits drive consistent E/M billing, which puts psychiatry under tighter audit scrutiny than therapist-only practices. CMS Targeted Probe and Educate (TPE) audits in behavioral health focus disproportionately on 90837 utilization, repeat 90791 billing, and same-day E/M + psychotherapy patterns.
Why Psychiatry Billing Is High-Risk
Psychiatry operates in one of the highest-friction billing environments in healthcare. Five structural factors drive that risk, and most revenue leakage traces back to one of them.

Time-Based Coding Liability
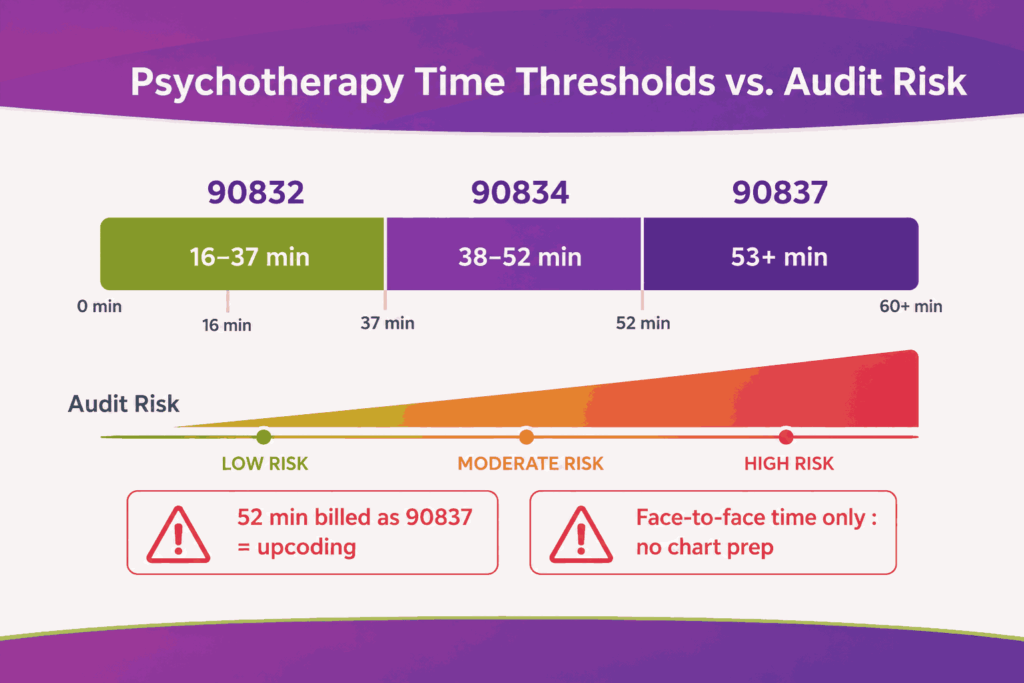
Psychotherapy codes are time-based: 90832 (16–37 minutes), 90834 (38–52 minutes), and 90837 (53+ minutes). A 52-minute session billed as 90837 is upcoding under CMS guidelines. RAC audit lookback periods extend six years, and recoupments compound with interest. Time documentation must capture face-to-face time only, as chart review, note-writing, and care coordination do not count.
Behavioral Health Carve-Outs
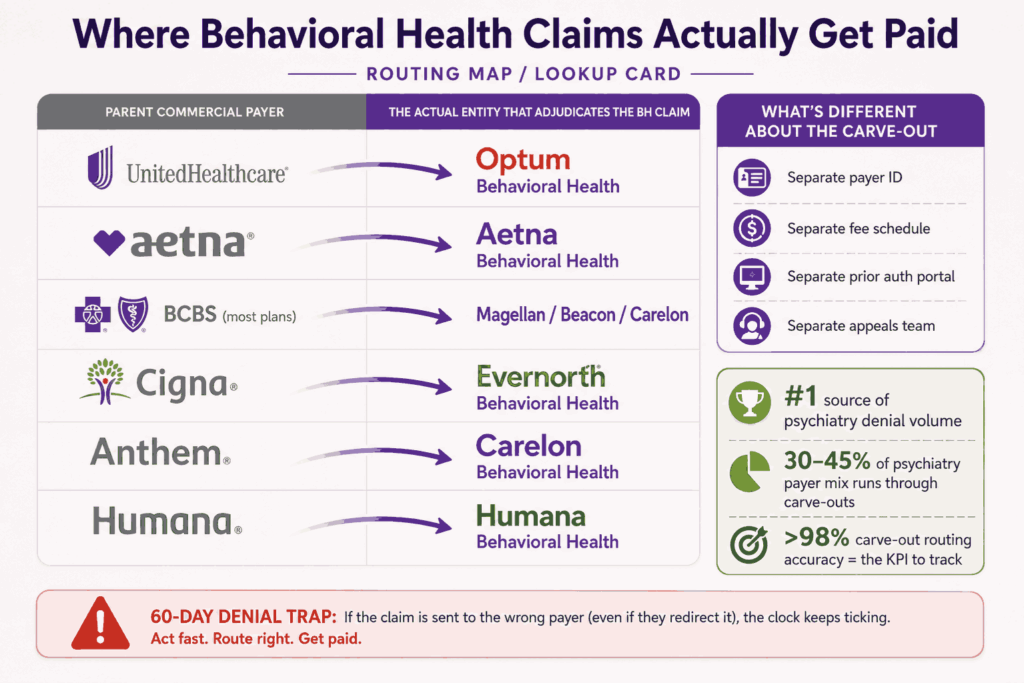
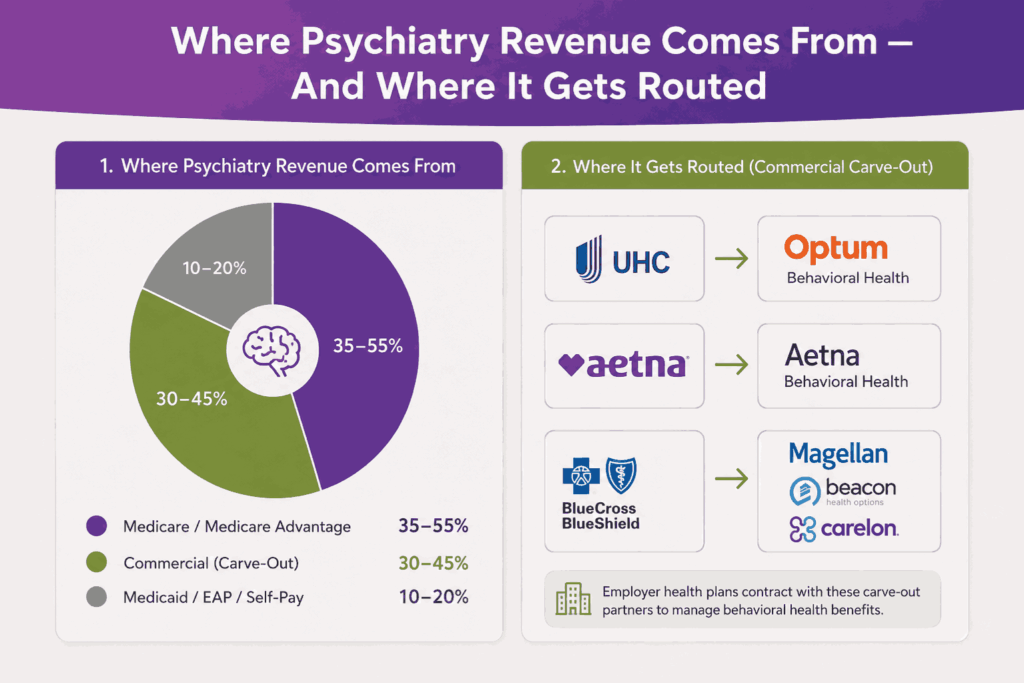
Most commercial plans route behavioral health claims to a separate entity. UnitedHealthcare routes to Optum Behavioral Health, Aetna to Aetna Behavioral Health, most BCBS plans to Magellan, Beacon, or Carelon. Each carve-out runs its own payer ID, fee schedule, prior authorization portal, and appeals team. Submitting a behavioral health claim to the parent payer instead of the carve-out generates a coverage denial that takes 60 days or more to surface and correct.
Documentation as Medical Necessity
Psychiatry has no lab values or imaging to anchor claims. Symptom severity, functional impairment, treatment response, and time documentation must all support the code billed. Cloned documentation across visits is the fastest way to an audit.
Same-Day Stacked Code Patterns
Combined E/M plus psychotherapy (99214 + 90833 with modifier -25) is fully payable but triggers automated review at most commercial payers when billed above peer benchmark rates. Modifier -25 must be supported by distinct clinical content, not just separate time stamps.
Payer and State Variability
Medicaid behavioral health rules vary by state. IOP, PHP, ARMHS, CTSS, EIDBI, and TCM each carry their own code sets, rate structures, and authorization workflows. None of these maps cleanly onto standard outpatient billing.
The Psychiatry Billing Process: End-to-End Workflow
The workflow runs through nine connected steps. Each has its own staff responsibilities, system touchpoints, and psychiatry practices lose revenue when errors are missed. Transcure offers psychiatry medical billing services to practices looking to optimize their workflows and reduce operational errors and claim denials.
Step 1: Scheduling and Behavioral Health Eligibility Routing
Pre-registration captures demographics, insurance, plan type, and the reason for the visit. The most important task here is behavioral health routing identification, which means confirming which entity actually adjudicates the claim. A patient with UnitedHealthcare commercial coverage may have therapy claims paid by Optum, medication management paid by Optum, and psychological testing routed through a third pre-cert vendor. Identifying the correct adjudicator at scheduling prevents the most common psychiatry denial pattern.
Step 2: Insurance Eligibility and Benefits Verification
Eligibility checks run 48 to 72 hours before every visit through real-time EDI 270/271 transactions. Verification must be performed against the behavioral health entity, not the parent payer.
Items to verify every visit:
- Active coverage and behavioral health benefit status
- Session limits remaining for the plan year
- Deductible status and copay
- In-network status with the BH carve-out specifically
- Telehealth coverage and audio-only eligibility
- Prior authorization requirements for testing or higher levels of care
For chronic patients seen weekly, eligibility is re-verified monthly at a minimum.
Step 3: Prior Authorization
Psychiatry’s prior authorization volume is lower than that of imaging-heavy specialties but concentrates on high-cost services. Common PA-required services include psychological testing batteries (96130–96139), TMS, ECT, esketamine (Spravato), inpatient admissions, IOP, PHP, and most extended psychotherapy session approvals beyond initial benefit caps.
The MHPAEA Parity Final Rule creates a new operational lever here. If a behavioral health plan requires prior authorization where the medical or surgical equivalent does not, that disparity is a parity violation usable in appeals and reportable to the state insurance commissioner.
Step 4: Patient Check-In and Consent Capture
Front-desk staff verify identity, confirm insurance at check-in, and collect copays or known deductible balances. Telehealth consent must be documented in the chart before or during the encounter, verbal acceptable for most payers, written required by some.
For SUD-related encounters, 42 CFR Part 2 enforcement (effective February 16, 2026) requires a single TPO consent on file before claims containing SUD diagnosis codes (F10–F19) are released. Claims submitted without valid consent are now subject to OCR enforcement and civil monetary penalties, not just payer denials.
Step 5: Clinical Encounter and Documentation
Providers document the encounter during or immediately after the visit. Documentation must include:
- Start and end times for time-based codes
- Symptom severity, functional impairment, and treatment response
- Specific ICD-10-CM code, not unspecified F-codes when more specific is supportable
- For combined E/M and psychotherapy: distinct time blocks and separate clinical content
- Mental status examination findings tied to the assessment
- Medication review and prescribing rationale for prescribers billing 90792 or E/M
Step 6: Charge Capture and Coding
Charges flow from the EHR into the practice management system for claim generation. Two psychiatry-specific failure points dominate this stage. The first is 90791 vs 90792 misuse. Non-prescribing providers (psychologists, LCSWs, LPCs, LMFTs) must use 90791. Only prescribers (MD, DO, PMHNP, PA) can bill 90792. Billing 90792 from a non-prescriber NPI generates automatic denials and creates audit exposure. Utilizing the top EMRs for psychiatry practices dynamically blocks these invalid provider-to-code pairings by filtering available templates based on user credentials.
The second is time-mismatch coding. Documented 51-minute sessions billed as 90837 fail audit. Pre-submission scrubbing must flag time-code conflicts before claims transmit.
Step 7: Claim Submission
Claims move through the clearinghouse to the correct payer ID, whether that is a behavioral health carve-out for commercial plans, the parent payer for traditional Medicare, or a Medicaid plan. Daily claim submission is considered standard practice to avoid unnecessary delays in reimbursement.
Telehealth claims require the correct modifier and POS code:
- Modifier 95: synchronous audio-video
- Modifier 93: audio-only (covered for behavioral health through CY 2027)
- POS 10: patient in the home
- POS 02: patient outside the home (clinic, workplace)
All of these four elements must be correct for the claim to process.
Step 8: Payment Posting and Underpayment Detection
Electronic remittance advice (ERA) files automate most posting through 835 transactions. The high-value work happens in variance detection. Behavioral health carve-out fee schedules frequently differ from parent payer schedules, and underpayments often go undetected without automated reconciliation against contracted rates.
Same-encounter split payments are another psychiatry-specific reconciliation challenge. A patient seen for combined medication management and psychotherapy may generate one payment from the parent payer (for E/M) and a separate payment from the BH carve-out (for the psychotherapy add-on). Both must be posted accurately to the same encounter.
Step 9: A/R Follow-Up, Denials, and Appeals
Accounts move through aging buckets at 30, 60, and 90 days. Carve-out routing errors age fast by the time a denial surfaces, it can be two billing cycles old. Patient balances follow a parallel statement workflow with extra sensitivity around mental health stigma; soft collections language is the operational norm.
The full workflow looks like this when laid out side by side.
| Step | Owner | System | Common Failure Point |
|---|---|---|---|
| Scheduling | Front desk | Practice management | Wrong BH carve-out routing |
| Eligibility | Verification team | Clearinghouse | Verifying against parent payer instead of carve-out |
| Prior auth | Auth coordinator | Payer portal | Missed PA on testing or higher LOC |
| Check-in | Front desk | PM system | Missing 42 CFR Part 2 consent |
| Documentation | Provider | EHR | Time documentation gaps |
| Charge capture | Coder | EHR to PM | 90791/90792 misuse, time-code mismatch |
| Submission | Biller | Clearinghouse | Wrong payer ID, missing modifier |
| Payment posting | Posting team | PM system | Carve-out split payment misreconciliation |
| A/R follow-up | A/R team | PM system | Aged carve-out denials |
Insurance and Payer Mix for Psychiatry
Payer mix shapes every operational decision in a psychiatry practice. A typical psychiatrist sees a patient mix of roughly 35–55% Medicare and Medicare Advantage, 30–45% commercial insurance routed through behavioral health carve-outs, with the remainder split across Medicaid, EAP, and self-pay accounts.
Each payer category behaves differently. Understanding those patterns helps billing teams anticipate denials, route claims correctly, and apply the right appeals lever.
Traditional Medicare
Traditional Medicare reimburses under the Physician Fee Schedule and rarely requires prior authorization for outpatient psychiatric services. LCSW, LPC, and LMFT independent Medicare enrollment took full effect on January 1, 2024, and has matured through 2025–2026, expanding the reimbursable provider mix and changing how group practices structure billing.
Audit exposure is concentrated on 90837 utilization, repeat 90791 billing within six months, and same-day E/M plus psychotherapy patterns above peer benchmarks.
Medicare Advantage
Medicare Advantage plans are operationally closer to commercial insurance than to traditional Medicare. Each MA plan applies its own prior authorization rules, session caps, formulary-driven medication management restrictions, and HCC risk adjustment standards. MA plans should never be treated as traditional Medicare in billing workflows. Each plan’s behavioral health policy is verified at credentialing and re-verified annually.
Commercial Payers and Behavioral Health Carve-Outs
Most commercial plans carve behavioral health out to a separate entity. Optum (UHC), Aetna Behavioral Health, Magellan, Beacon, and Carelon dominate the market. Each carve-out maintains its own payer ID, fee schedule, prior authorization portal, claim submission rules, and appeals process.
Carve-out misrouting is the single largest source of psychiatry denial volume. The denial returns labeled as a coverage issue, which masks the root cause and delays correction by 30–60 days. Practices that audit their top 10 commercial plans for carve-out arrangements close this leak quickly.
Medicaid
Medicaid behavioral health rules vary by state and program. Outpatient therapy typically maps to standard CPT codes, but state-specific programs operate on different code sets entirely. ARMHS, CTSS, EIDBI, TCM, and 1115 waiver programs each carry their own billing structures and authorization workflows.
Eligibility churn is also higher in Medicaid behavioral health than in medical Medicaid, making re-verification at every visit a baseline requirement.
EAP and Self-Pay
Employee Assistance Programs are often confused with insurance. EAP services are billed on a flat session-based fee model, with no claim filed to commercial insurance. Billing insurance when EAP applies and then receiving a denial 90 days later is a recurring revenue leakage pattern.
Self-pay and out-of-network billing require No Surprises Act good-faith estimates, transparent itemized statements, and structured payment plans.
2026 Regulatory and Operational Shifts to Watch
Three major regulatory changes are reshaping psychiatry billing operations in 2026, while a fourth is expected to influence reimbursement and compliance strategy through 2027. These shifts affect documentation standards, payer oversight, and overall revenue cycle performance.
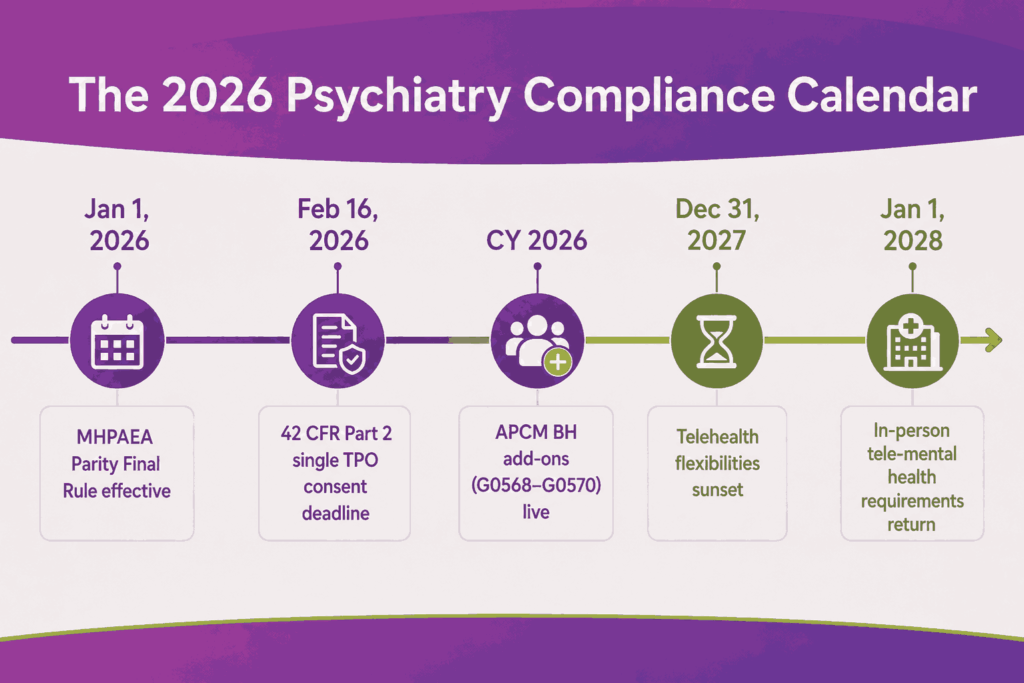
MHPAEA Parity Final Rule (Effective January 1, 2026)
Plans cannot apply stricter non-quantitative treatment limits (NQTLs) to mental health or SUD benefits than to medical or surgical benefits. Prior authorization rules, session limits, fail-first protocols, and concurrent review thresholds must now be comparable across both benefit categories. Plans are required to collect comparative access data and address material disparities.
When a behavioral health denial reflects an NQTL that does not apply to the equivalent medical benefit, the parity argument is the strongest available appeal position. Documented disparity can be escalated to the state insurance commissioner.
42 CFR Part 2 Final Rule (Effective February 16, 2026)
The single TPO consent now replaces program-by-program SUD consent forms. HIPAA breach notification standards apply to SUD programs. Enforcement authority sits with OCR.
The most direct billing impact is on vendor agreements. Billing partners handling SUD claims now require a Qualified Service Organization Agreement (QSOA) in addition to a standard BAA. Many practices are operating on outdated vendor contracts and need to audit their billing partner agreements before the next external audit. Outbound claim attachments must also include the updated redisclosure notice language.
APCM Behavioral Health Add-On Codes (New for CY 2026)
CMS finalized three new HCPCS codes that pair behavioral health integration with Advanced Primary Care Management:
- G0568: Initial CoCM month add-on to APCM (national average $162)
- G0569: Subsequent CoCM month add-on ($146)
- G0570: General BHI add-on
These codes do not carry the time-based documentation burden of the traditional 99492–99494 CoCM codes, making them substantially easier to bill in integrated care models. Practices running combined primary care and psychiatric consult workflows should validate APCM eligibility and capture the add-on revenue.
Telehealth Stability Through 2027
Audio-only psychotherapy remains reimbursable through CY 2027 with modifier 93. Tele-mental health flexibilities (no geographic restriction, patient home as POS 10) continue through December 31, 2027. The six-month in-person requirement for tele-prescribing remains relaxed through the end of 2027, though prescribing flexibilities for controlled substances may expire earlier.
Mark January 1, 2028 as the operational deadline for tele-mental health workflow review. In-person requirements are scheduled to return unless Congress extends them.
Documentation Standards For Psychiatry
Documentation is the audit trail that supports every billed psychiatry service. With no labs or imaging to anchor medical necessity, the narrative is the claim defense.
Psychiatry-specific documentation requirements include:
- Start and end times for all time-based codes, capturing face-to-face time only
- Symptom severity, functional impairment, and current treatment response at every visit
- For combined E/M and psychotherapy: separate time blocks, distinct clinical content, modifier -25 justification
- Specific ICD-10-CM code aligned with documentation; unspecified F-codes (F32.9, F33.9, F41.9) drive denials when more specific codes are supportable
- Medication review, prescribing rationale, and side effect monitoring for E/M and 90792
- Treatment plan updates with measurable goals and progress markers
The most common documentation-related denials come from a small number of recurring issues. Missing time documentation on 90834 and 90837 claims is the leading cause. Cloned notes across visits with identical narrative content, identical mental status exams, and identical interventions are flagged by payer audit algorithms within months. For 90791 repeat billing, the chart must clearly establish a break in treatment or a clinically significant change justifying re-evaluation.
EHR templates accelerate documentation speed but create compliance risk when overused. Structured templates that still require provider input on visit-specific content (symptoms, response, time, plan) keep documentation defensible without slowing workflow.
Denial Management for Psychiatry Practices
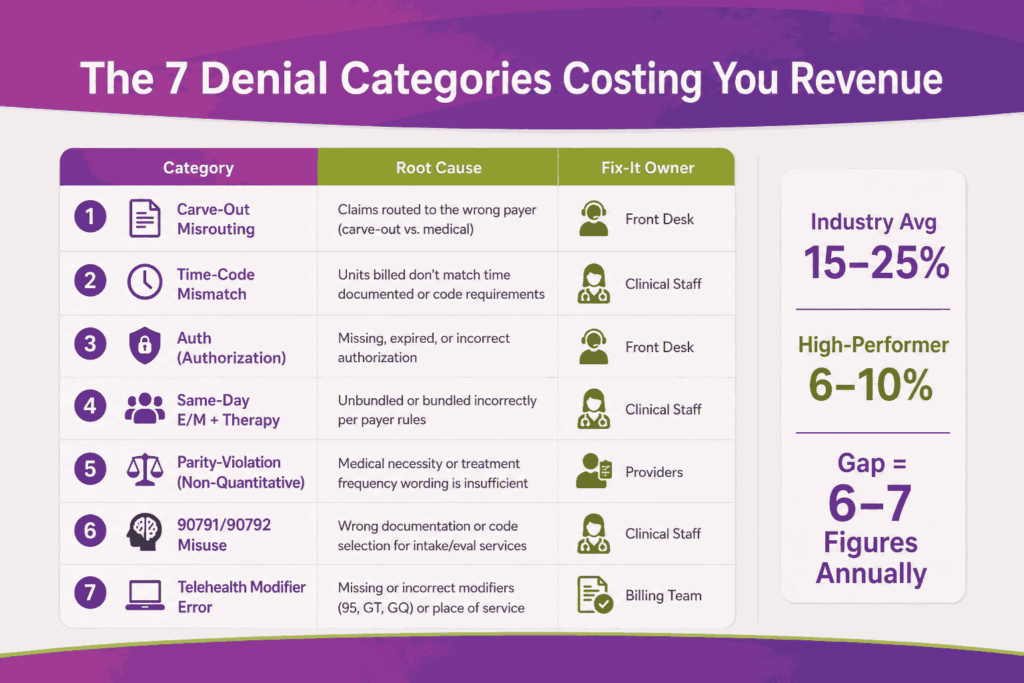
The industry-average behavioral health denial rate runs 15 to 25 percent on first pass. Psychiatry practices with active denial management programs operate at 6 to 10 percent. The 10+ percent gap typically translates into mid- to high-six-figure annual revenue impact for a multi-prescriber practice.
Active denial management treats denials as a system problem, not individual claim rework. Root-cause categorization is what reveals upstream workflow failures.
The Seven Denial Categories You Track
| Category | Root Cause | Where to Fix |
|---|---|---|
| BH carve-out misrouting | Wrong payer ID | Scheduling / eligibility |
| Time-code mismatch | Documented time below CPT threshold | Provider documentation |
| Authorization | Missing or expired PA | Auth coordinator |
| Same-day E/M + therapy | Missing -25 or insufficient distinct documentation | Coding team |
| Parity-violation denial | Plan applying stricter NQTL | Appeals (MHPAEA leverage) |
| 90791/90792 misuse | Code billed outside provider scope | Provider scope mapping |
| Telehealth modifier error | Wrong modifier or POS code | Coding team |
Denial Workflow
Denied claims are reviewed within 24 hours of remittance posting. Appeal decisions are made within 5 business days based on reimbursement potential and likelihood of recovery. Claims below the cost-to-collect threshold move to a monitored write-off bucket but are still tracked for trend analysis.
The MHPAEA Appeal Lever
Effective January 1, 2026, parity-based appeals are the strongest tool available for recovering behavioral health denials. When a denial reflects an NQTL not applied to the medical or surgical equivalent, for example, a session cap, fail-first requirement, or concurrent review threshold, the appeal cites the parity rule directly. Plans are required to demonstrate comparability, and documented disparity becomes the basis for both reimbursement recovery and state-level enforcement complaints.
A/R Management and Revenue Cycle KPIs
KPI tracking is the dashboard for psychiatry billing performance. Without it, billing teams cannot prove improvement or identify leakage early enough to act.
The benchmarks below reflect performance levels seen in high-performing psychiatry practices. Smaller practices may fall short on several metrics initially. The focus is steady quarterly improvement, not immediate perfection.
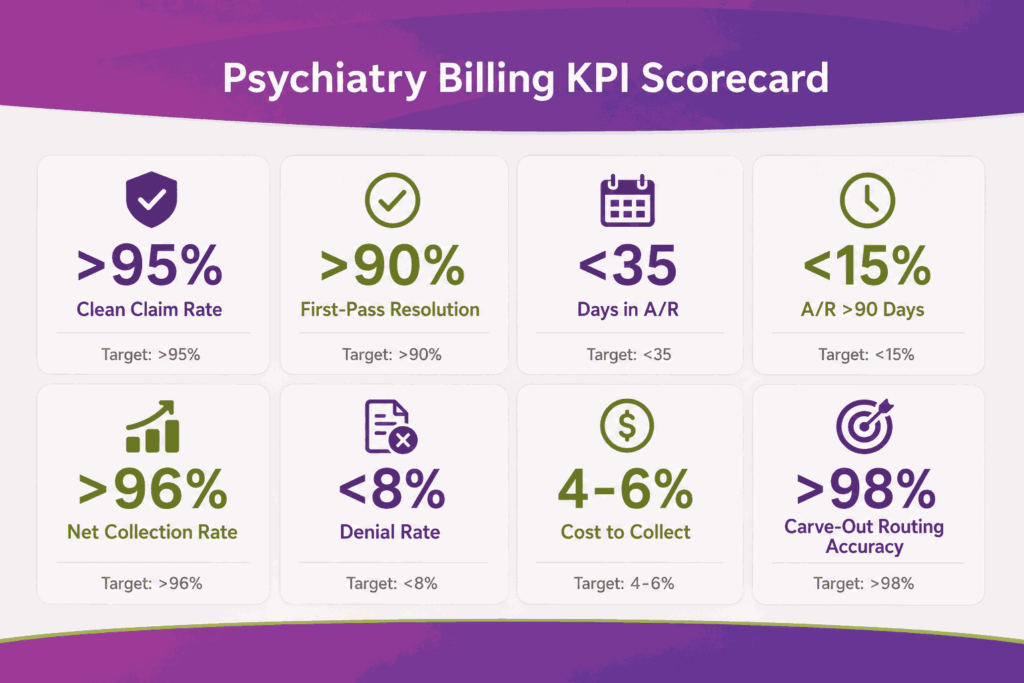
Core KPIs Every Psychiatry Practice Should Track
| KPI | Target | What It Tells You |
|---|---|---|
| Clean claim rate | Above 95% | Eligibility and scrub quality |
| First-pass resolution rate | Above 90% | End-to-end billing health |
| Days in A/R | Below 35 | Cash flow speed |
| A/R over 90 days | Below 15% | Aging discipline |
| Net collection rate | Above 96% | Real revenue capture |
| Denial rate | Below 8% | Process quality (industry avg 15–25%) |
| Cost to collect | 4 to 6 percent | Operational efficiency |
| Carve-out routing accuracy | Above 98% | Scheduling and eligibility discipline |
A/R Aging Workflow
Each aging bucket operates as a separate queue with its own follow-up rules and escalation path. Carve-out denials surface late in psychiatry, which makes 60-day and 90-day bucket discipline especially important.
- 0–30 days: Light follow-up, payer status checks
- 31–60 days: Active follow-up, denial triage, carve-out routing review
- 61–90 days: Escalation to senior billers, structured appeal review, parity-violation flagging
- 90+ days: Final appeal decision, write-off review, patient responsibility transfer
The Hidden A/R Problem: Carve-Out Split Payments
When commercial plans carve out behavioral health, a single encounter may generate two separate payments, one from the parent payer for the E/M component, one from the carve-out for the psychotherapy add-on. Posting teams that treat these as duplicate payments or fail to reconcile both lines miss revenue routinely. Automated split-payment matching closes this gap.
Compliance, Audits, and Risk Management
HIPAA, 42 CFR Part 2, CMS audits, MHPAEA enforcement, and False Claims Act exposure all sit under compliance. Psychiatry carries elevated audit risk because of 90837 utilization patterns, same-day stacked code billing, and the documentation-heavy nature of medical necessity defense.
Common Audit Triggers for Psychiatry
CMS and commercial payers use data analytics to flag outlier practices. Five patterns trigger psychiatry audits most often:
- 90837 utilization above 50–70% of total psychotherapy billing (MAC threshold varies)
- Cloned time documentation across multiple visits
- Same-day E/M + psychotherapy patterns above peer benchmark
- Repeat 90791 within six months without a documented break in treatment
- Add-on code (90833/90836/90838) billed without supporting E/M documentation
42 CFR Part 2 Compliance Posture
PHI moves between the EHR, practice management system, clearinghouse, and any outsourced billing vendor. For SUD-related claims, each connection needs both a BAA and a QSOA. Internal audits should review vendor access quarterly and confirm consent workflows remain audit-ready under the post-February 2026 framework.
In-House vs Outsourced Billing for Psychiatry
The decision depends on practice size, payer complexity, denial rate, and SUD service exposure. Psychiatry practices process a high volume of low- to mid-dollar claims, which means small denial rate increases compound quickly.
Quick Comparison
| Factor | In-House Billing | Outsourced Billing |
|---|---|---|
| Cost Structure | Fixed salary, benefits, software | 5 to 8 percent of monthly collections |
| Scalability | Limited by headcount | Scales with volume |
| Psychiatry Coding Expertise | Depends on staff experience | Specialist coders across psych workflows |
| Tech Stack | Practice-owned | Included in service |
| Carve-Out Management | Manual tracking burden | Handled in vendor workflows |
| Compliance Risk | Fully on the practice | Shared under BAA/QSOA |
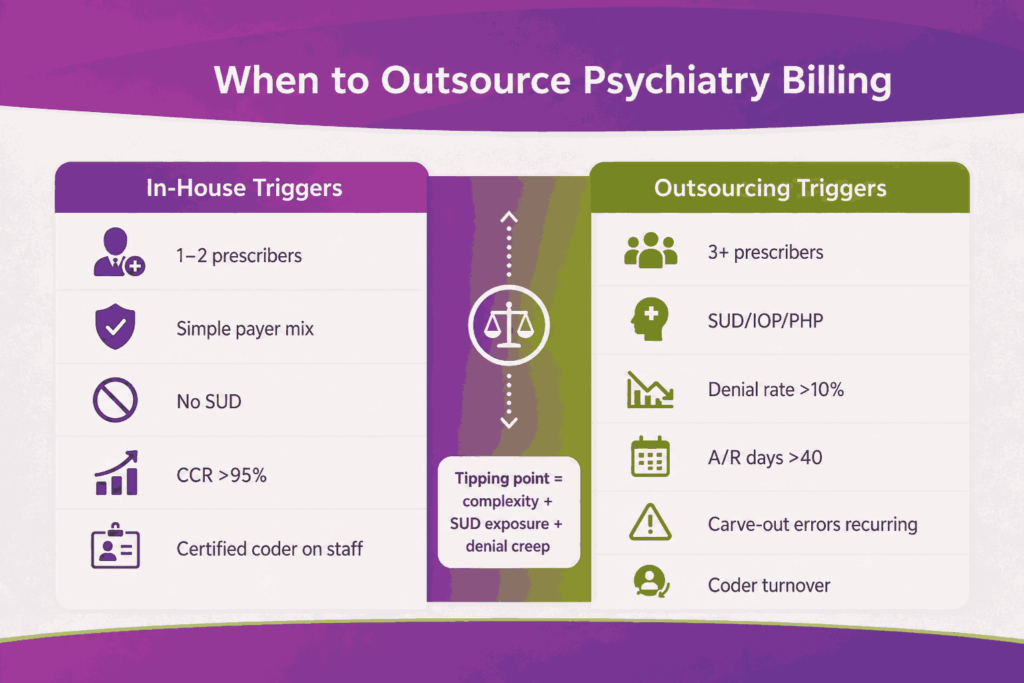
When In-House Works
In-house billing works for small practices with limited complexity and a stable payer mix.
- 1 to 2 prescribers with steady patient flow
- Simple payer mix, minimal carve-out exposure
- No SUD services (avoids 42 CFR Part 2 vendor complexity)
- Clean claim rate already above 95%
- Certified behavioral health coder on staff
When Outsourcing Wins
Outsourcing becomes more effective as complexity grows.
- 3+ prescribers or multi-state operations
- Mix of psychiatrists, PMHNPs, and therapists under one TIN
- SUD services or IOP/PHP programs in scope
- Denial rate above 10% or A/R days above 40
- Recurring carve-out routing errors
- Coder turnover or backlog
The Hidden Cost of In-House
The real cost of in-house billing is rarely visible in salary lines. It shows up in operational drag and compliance exposure. Coder turnover in behavioral health runs every 16 to 20 months, creating recurring disruption. 42 CFR Part 2 vendor compliance, parity rule enforcement, and behavioral health carve-out routing add workload that general medical billing teams are not built to handle. Roughly 20 to 30 percent of staff time often disappears into denial rework instead of forward billing.
Conclusion
Psychiatry billing performance in 2026 is driven largely by upstream operations. Denial rates, A/R days, and net collections are usually the result of decisions made during scheduling, eligibility verification, and documentation. High-performing practices are not simply better at appeals; they prevent avoidable errors by accurately documenting time-based services from the start.
The current regulatory environment increases the importance of that process discipline. Practices that strengthen upstream workflows, such as carve-out routing, time documentation, vendor oversight, and parity-based appeals, usually lead to downstream improvements in denials, collections, and A/R performance. Those that do not often continue losing revenue quietly until payer audits or compliance reviews expose the underlying gaps.
Frequently Asked Questions
What is a behavioral health carve-out, and how does it affect claims?
Most commercial plans route behavioral health claims to a separate entity, UHC to Optum, Aetna to Aetna Behavioral Health, BCBS plans to Magellan, Beacon, or Carelon. Each carve-out has its own payer ID, fee schedule, and appeals process. Routing claims to the parent payer instead of the carve-out is the single largest source of psychiatry denial volume.
Can a psychiatrist bill E/M and psychotherapy on the same day?
Yes. The E/M code (typically 99214) is billed with modifier -25, and the psychotherapy add-on code (90833, 90836, or 90838) is billed alongside it. Both services need separate time documentation and distinct clinical content. Same-day stacked claims are payable but carry higher audit scrutiny when billed above peer benchmark rates.
What changed with 42 CFR Part 2 in February 2026?
The single TPO consent replaced program-by-program SUD consent forms, HIPAA breach notification now applies to SUD programs, and OCR holds enforcement authority. For billing operations, vendors handling SUD claims now require a Qualified Service Organization Agreement (QSOA) in addition to a standard BAA.
How do I use MHPAEA parity rules to appeal a denial?
When a behavioral health denial reflects a non-quantitative treatment limit (prior auth, session cap, fail-first protocol, concurrent review) not applied to the medical or surgical equivalent, the appeal cites parity. Plans must demonstrate comparability. Documented disparity becomes both an appeal lever and a basis for state insurance commissioner complaints.
Are LCSWs, LPCs, and LMFTs now able to bill Medicare directly?
Yes. LCSW, LPC, and LMFT independent Medicare enrollment took full effect on January 1, 2024, and has matured through 2025–2026. Group psychiatry practices benefit from an expanded reimbursable provider mix but need updated credentialing workflows.
What is the audit threshold for billing 90837?
Most MACs and commercial payers flag providers who bill 90837 on 50-70% of total psychotherapy claims. The threshold varies, but consistent over-utilization without supporting documentation triggers Targeted Probe and Educate (TPE) audits and RAC reviews.
Should small psychiatry practices outsource billing?
Yes, once the practice grows past 2 to 3 prescribers, takes on SUD services, or denial rates climb above 10 percent. Smaller practices with simple payer mix and strong in-house leadership can run billing in-house at competitive cost, but carve-out management, 42 CFR Part 2 vendor compliance, and parity rule enforcement raise the operational bar significantly in 2026.