When it comes to radiology billing, it’s not just about submitting claims and waiting for a check. It is a layered, fast-moving process where one wrong modifier can cost a practice thousands of dollars. One missing authorization can tank an entire batch of claims. Nevertheless, the one undertrained coder can quietly drain revenue for months before anyone notices.
This guide covers everything, from basic definitions to denial management, from CPT codes to compliance red flags. If you are already looking for professional radiology billing services to take this off your plate, Transcure provides you with that. But if you want to understand the process first, keep reading.
What is Radiology Medical Billing?
Radiology medical billing is the process of submitting claims to insurance payers, government programs like Medicare and Medicaid, or directly to patients, in exchange for imaging services performed by a radiologist or imaging facility.
It sits inside the broader healthcare revenue cycle, which is the full financial journey a patient encounters, from the moment someone calls to schedule a scan all the way through to the final payment collected.
Who is involved in this process?
- The radiologist, who interprets the images and generates the report
- The referring physician, who ordered the scan and provided the clinical indication
- The billing department or outsourced billing company, which translates the clinical work into coded claims
- The insurance payer, who reviews, approves, or denies the claim
- The patient, who may owe a deductible, copay, or coinsurance amount depending on their plan
Each of these parties plays a distinct role, and when communication breaks down between any of them, claims get delayed or denied.
Why Radiology Billing Demands Specialized Expertise
Most medical billing specialties have their own quirks. Radiology has several at once.
- First, the volume is high. A single radiology group can produce hundreds or even thousands of claims per day. According to billing experts, for every 1,000 procedures performed, more than 1,000 CPT codes need to be identified, and an equal number of ICD-10 diagnosis codes need to be applied. That math adds up quickly.
- Second, multiple payers with different rules are involved. Medicare, Medicaid, Blue Cross Blue Shield, United Health, Cigna, and dozens of regional plans all have their own prior authorization requirements, bundling edits, and coverage policies.
- Moreover, radiology uses imaging-specific codes and modifiers that do not exist in other specialties. Getting them wrong is easy. Getting them right consistently takes training and constant updates.
- Fourth, and perhaps most distinct from other specialties, radiology often requires split billing. One claim goes to the physician, another goes to the facility. Two bills for one scan.
The Key Players You Need to Know
To understand how radiology billing works, you need to understand who does what.
- The radiologist is the physician who reads the images and creates the written report. They are the professional component of the service. They may work directly for a hospital, or they may be part of an independent radiology group contracted with multiple facilities.
- The referring physician orders the imaging study. Their clinical indication, the reason they want the scan, determines whether the payer considers it medically necessary. A weak or missing indication is one of the most common reasons radiology claims are denied.
- The billing department or billing company is the engine behind reimbursement. They handle coding, claim submission, payment posting, denial management, and appeals. In many practices, this work is outsourced to specialized revenue cycle management firms.
- The insurance payer is the entity that receives the claim and decides how much to reimburse, if anything. Their decision is based on the patient’s coverage, the medical necessity of the exam, the codes submitted, and whether proper authorization was obtained.
Who Actually Gets Paid and How
This is where radiology billing gets genuinely unusual compared to most other specialties.
When an imaging exam is performed, two separate bills are typically issued.
- The professional component (PC) covers the radiologist’s work: supervising the exam, interpreting the images, and producing the written report. This is billed with Modifier 26 attached to the CPT code.
- The technical component (TC) covers everything else: the equipment, the supplies, the salaries of the technologists running the scanner, the facility’s electricity, and overhead. This is billed with Modifier TC.
When the radiologist works inside a hospital and does not own the equipment, these components are billed separately. When a radiologist owns both the scanner and the reading service, such as in a private imaging center, they can bill the global fee, meaning both components together under one claim.
A real-world example
A patient arrives at a hospital for an MRI of the lumbar spine. The hospital bills the technical component because they own the scanner and employ the technologists. The radiologist, who works for an independent group, bills the professional component separately. Two claims. Two payer processes. One imaging encounter.
The system CMS established to determine dollar amounts for these components is called the Resource-Based Relative Value Scale, or RBRVS. Every service is assigned Relative Value Units (RVUs), and those RVUs are multiplied by a conversion factor to produce the dollar amount Medicare pays. In 2024, that conversion factor is $32.75 per RVU.
Radiology Medical Billing Basics Every Beginner Must Understand
Before getting into advanced topics, spend some time here. These basics form the foundation of everything else in radiology billing.
CPT Codes in Radiology
Current Procedural Terminology (CPT) codes are five-digit numeric codes developed by the American Medical Association (AMA) to describe every medical, surgical, and diagnostic service performed in a clinical setting. In radiology, the majority of imaging codes fall in the 70000 series.
Here is a breakdown of the radiology CPT code ranges you will encounter most often:
| CPT Code Range | Category |
|---|---|
| 70010 to 76499 | Diagnostic Imaging (X-ray, CT, MRI, etc.) |
| 76506 to 76999 | Diagnostic Ultrasound |
| 77001 to 77022 | Radiologic Guidance |
| 77046 to 77067 | Breast Mammography |
| 77071 to 77086 | Bone and Joint Diagnostic Studies |
| 77261 to 77799 | Radiation Oncology |
| 78012 to 79999 | Nuclear Medicine |
The right CPT code describes not just the body part but the technique used, the number of views taken, and whether contrast was administered. A CT of the abdomen with contrast has a different code from a CT of the abdomen without contrast, and from a CT of the abdomen with and without contrast. These are not interchangeable.
Common beginner mistakes with CPT codes include:
- Using the wrong code for the number of views (for example, billing a two-view chest X-ray code when only one view was taken)
- Missing the contrast versus no contrast distinction
- Applying a code that does not match the body part documented in the report
- Failing to verify that the CPT code is on the payer’s covered services list
To look up codes, the AMA CPT code lookup tool is the primary reference. CMS also publishes its Medicare fee schedule annually, which shows what Medicare reimburses for each code.
ICD-10 Diagnosis Codes
ICD-10 codes classify the patient’s diagnosis or reason for the visit. In radiology, the ICD-10 code submitted with the claim tells the payer why the imaging study was ordered.
This matters because payers do not simply ask whether the scan was performed. They ask whether the scan was medically necessary. And medical necessity is established by pairing the right diagnosis code with the imaging service.
If a patient gets a chest CT, the ICD-10 code needs to justify it. A code like R05.9 (cough, unspecified) may not be sufficient on its own for a high-cost imaging study. A code like R91.8 (other nonspecific abnormal findings of the lung field) carries more weight if the clinical record supports it.
What happens when codes do not match:
- The payer flags the claim for medical necessity review
- The claim is denied outright if the diagnosis does not align with their coverage policy for that specific imaging study
- The practice has to appeal with supporting documentation, which takes time and resources
The referring physician is responsible for providing the clinical indication. The billing team is responsible for translating that into the correct ICD-10 code. When communication between them is weak, this is exactly where errors happen.
Modifiers in Radiology Billing
Modifiers are two-character codes appended to CPT codes to provide additional information about the service. In radiology, modifiers are not optional. They are essential.
The most common radiology modifiers:
| Modifier | What It Means | When to Use It |
|---|---|---|
| 26 | Professional Component only | Radiologist bills for interpretation only; facility owns equipment |
| TC | Technical Component only | Facility bills for equipment, staff, and supplies |
| 59 | Distinct Procedural Service | Two separate imaging studies on the same day that would otherwise be bundled |
| LT | Left Side | Used when imaging is laterally specific |
| RT | Right Side | Used when imaging is laterally specific |
| 52 | Reduced Service | The exam was partially completed due to patient or technical reasons |
| 76 | Repeat Procedure by Same Physician | Same scan performed again on the same date |
Modifier 59 is one that billing teams often misapply. It is meant to indicate that two procedures performed on the same day are truly distinct and not components of a single service. Payers audit this modifier heavily, so it should only be used when the clinical record clearly supports separate, independent services.
Key Challenges in Radiology Medical Billing
A 2022 study by the Radiology Business Management Association found that claim denial rates in radiology practices range from 15 to 20 percent, depending on the payer mix and practice size. For high-volume practices processing thousands of claims per week, even a 5 percent denial rate represents significant lost revenue.
These are not theoretical problems. They are daily operational realities. And while radiology carries its own set of billing pressures, neighboring specialties face similar battles.
1. High Claim Denial Rates
Radiology practices deal with denial rates that are consistently higher than those of many other specialties. The reasons are tied directly to the complexity of the specialty: high claim volume, frequent prior authorization requirements, bundling edits, and payer-specific rules that vary significantly across commercial plans.
The financial impact is real. Each denied claim costs an average of $25 to $30 to rework and resubmit, according to the American Academy of Family Physicians. Multiply that across hundreds of denials per month, and the administrative cost alone becomes unsustainable for smaller practices.
2. Complex Coding and Documentation
Radiology coding is not a skill someone picks up in an afternoon. It requires knowing the difference between a CPT code for an MRI with contrast and one without. It requires understanding which modifiers apply to which clinical scenarios. It requires reading the radiologist’s report carefully enough to code it accurately.
The table below covers common radiology CPT codes relevant to everyday billing scenarios:
| CPT Code | Description | Common Modifier |
|---|---|---|
| 71046 | Chest X-ray, 2 views | 26 or TC |
| 72141 | MRI cervical spine, without contrast | 26 or TC |
| 70553 | MRI brain, with and without contrast | 26 or TC |
| 74177 | CT abdomen and pelvis, with contrast | 26 or TC |
| 93306 | Echo with Doppler and color flow | 26 or TC |
| 76700 | Ultrasound abdomen, complete | 26 or TC |
| 77067 | Screening mammography, bilateral | TC |
| 78816 | PET scan, whole body | 26 or TC |
Documentation errors often originate with the radiologist’s report itself. If the report does not specify the number of views, does not mention whether contrast was used, or does not include the physician’s signature, the billing team is working with incomplete information. Incomplete information leads to wrong codes or missing claims.
3. Reduced Reimbursement Rates
Medicare reimbursement for radiology services has been declining in real terms for over a decade. The 2024 physician fee schedule included a 1.25 percent reduction in the conversion factor used to calculate RVU payments, continuing a trend that has squeezed practice margins.
Private payers often negotiate rates based on Medicare benchmarks, which means that when Medicare cuts reimbursement, commercial rates tend to follow. Practices that do not actively negotiate their payer contracts or that fail to track reimbursement trends can find themselves operating at significantly reduced margins without realizing it.
4. Delayed Communication with Referring Physicians
The referring physician orders the scan. But the billing team needs information from that physician to bill correctly, including the clinical indication, any relevant diagnosis codes, and confirmation that the order aligns with what was actually performed.
When this communication loop is slow or broken, claims sit in a pending state, documentation requests go unanswered, and prior authorizations are missed entirely. In busy hospital environments, this happens more than most administrators would like to admit.
5. Staff Shortage and Training
The radiology billing workforce is under strain. Experienced medical coders are in short supply, and the learning curve for specialty-specific billing is steep. Staff turnover in billing departments is higher than average across healthcare, and each departure carries a knowledge transfer risk.
Training is not a one-time event. CMS updates CPT codes every year. Payers change their authorization requirements. New imaging technologies enter the market with new codes attached. A billing team that was well-trained two years ago may be working with outdated knowledge today.
6. Missing Authorization and Eligibility
Prior authorization is required for the vast majority of high-cost imaging studies, including MRI, CT, and PET scans. Failing to obtain it before the scan is performed almost guarantees a denial.
Eligibility verification is equally important. A patient’s insurance coverage can change between the time they schedule an appointment and the time they actually arrive for the scan. If the billing team does not verify current eligibility before the procedure, they may submit a claim to a payer that no longer covers the patient.
7. Payer-Specific Bundling Edits
Beyond the above challenges, payers apply bundling edits through systems like the Correct Coding Initiative (CCI). These edits automatically bundle certain CPT code combinations together.
This means one of the codes will not be reimbursed. unless the billing team applies the correct modifier and the clinical record supports unbundling. Many practices lose revenue here simply because their software is not configured to catch these edits before submission.
8. Incomplete Radiology Reports
A radiology report is not just a clinical document. It is also a billing document. If the heading is missing, if the number of views is not documented, if the clinical indication is vague, or if the physician’s signature is absent, the claim is vulnerable. The report needs to include the heading, number of views, reason for examination, findings, summary, and physician sign-off at a minimum.
9. Technology Gaps and Legacy Systems
Practices that still rely on manual coding or outdated billing software face processing delays, higher error rates, and an inability to track claims at a granular level. Modern billing platforms offer claim scrubbing, automatic code validation, and denial analytics. Without these tools, billing teams are essentially flying blind.
The Radiology Medical Billing Process Step by Step
The billing process in radiology follows a defined sequence. Skipping steps creates gaps. Gaps create denials. This is how it should work.
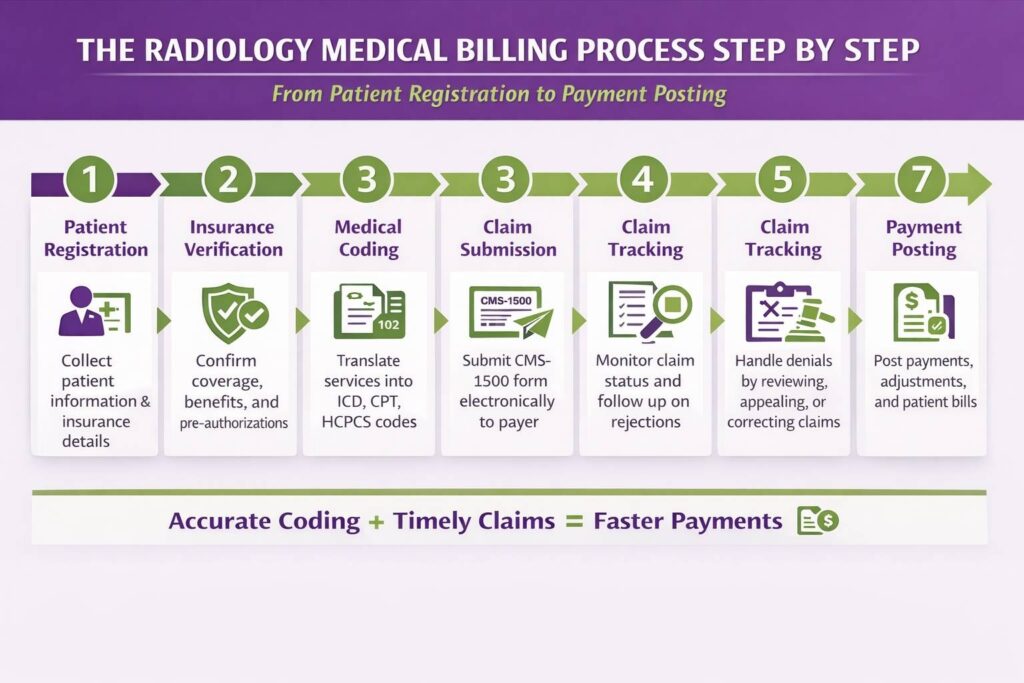
Step 1: Patient Registration and Insurance Verification
Before the scan happens, the front desk or registration team collects the patient’s demographic information, insurance details, and referring physician information. Insurance eligibility is verified in real time to confirm that the patient’s plan is active, that imaging services are covered, and that the patient’s deductible and copay information is current.
This step is where many practices cut corners. Verifying insurance the same day as the appointment, rather than 24 to 48 hours in advance, leaves no time to resolve coverage issues before the patient arrives.
Step 2: The Imaging Order and Prior Authorization
The referring physician’s order triggers the authorization process. For studies like MRI, CT, and PET scans, prior authorization is almost universally required by commercial payers. The billing or authorization team contacts the payer, provides the clinical indication, and receives an authorization number that must be attached to the claim.
Without this number, the claim will be denied.
Step 3: The Scan Happens, and Documentation is Created
The technologist performs the scan. The radiologist interprets the images and generates the written report. That report becomes the foundation for everything that follows in the billing process. It must be complete, legible, and signed.
Step 4: Coding the Claim
The coder reviews the radiologist’s report and assigns the appropriate CPT code and ICD-10 diagnosis code. The correct modifiers are applied based on whether this is a professional component bill, a technical component bill, or a global bill.
This is where technical precision matters most. A coder who is uncertain about which code to use should consult the AMA CPT manual, check payer-specific guidelines, or escalate to a senior coder rather than guess.
Step 5: Submitting the Claim to the Payer
The coded claim is submitted electronically to the payer through a clearinghouse. Most practices submit claims within 24 to 48 hours of the service date. Commercial payers have timely filing limits, often ranging from 90 days to one year from the date of service. Missing these deadlines results in an essentially irreversible denial.
Step 6: Payment Posting and Reconciliation
When the payer processes the claim, they send an Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA). The billing team posts the payment and reconciles it against the amount billed. Any underpayments, contractual adjustments, or patient balances are identified here.
Step 7: Denial Management and Appeals
Denied claims are reviewed, the denial reason is identified, and a decision is made about whether to appeal. If the denial is for a correctable reason, such as a missing modifier or an authorization that was obtained but not submitted correctly, the claim is corrected and resubmitted. If the denial is for medical necessity, an appeal letter is written with supporting clinical documentation.
Where Beginners Usually Get Stuck
Three spots trip up most new billing staff in radiology:
- Skipping prior authorization checks. The assumption that someone else obtained the auth is dangerous. Build a verification step into the workflow.
- Wrong modifier use. Applying Modifier 26 when a global bill is appropriate, or using Modifier 59 without clinical justification, creates both claim errors and audit risk.
- Missing or incomplete documentation from the radiologist. If the report does not support the code, the code cannot stand. Coding from incomplete reports is a liability.
Prior Authorization in Radiology Billing
Prior authorization is the payer’s way of reviewing whether a proposed imaging study meets their clinical criteria before they agree to pay for it. It is not a formality. It is a gatekeeping mechanism, and payers enforce it consistently for high-cost studies.
Imaging studies that almost always require prior authorization:
- MRI studies (spine, brain, joints, and abdomen)
- CT scans (chest, abdomen, pelvis)
- PET scans
- Nuclear medicine studies
- Certain ultrasound procedures, depending on the payer
What happens when you skip it? The claim is denied. The practice may attempt a retro-authorization, but payers do not always grant these, and the process is time-consuming. The financial loss is often absorbed by the practice because the patient cannot reasonably be billed for a service that should have been pre-authorized.
How to Handle Prior Authorization Without Losing Your Mind
Authorization management is a workflow problem, not just a knowledge problem. Here is what works:
- Build a payer-specific authorization checklist. Each major payer in your network should have a documented list of which CPT codes require authorization and what clinical information they need to approve them. This checklist should live in your practice management system, not in someone’s memory.
- Document everything, every time. Record the authorization number, the date it was obtained, the name of the representative who provided it, and the date range it covers. If an authorization is verbal, follow up with written confirmation. Verbal authorizations that cannot be documented are the same as no authorization when a claim is denied.
- Know who to call when auth is stuck. Every payer has a provider services line and a peer-to-peer review process for cases where authorization is being delayed or denied. Radiologists and referring physicians can request peer-to-peer reviews when a study is clinically urgent.
Common Radiology Medical Billing Errors Beginners Make
Some errors are predictable. The same mistakes show up repeatedly across different practices, different billing teams, and different software platforms.
- Upcoding or downcoding imaging studies. Billing for a three-view chest X-ray when only two views were taken is upcoding. It is also fraud. Downcoding, submitting a lower-level code than what was performed, costs revenue. Both stem from not reading the report carefully.
- Missing or wrong modifiers. Using Modifier TC on a professional-component-only claim or forgetting Modifier 26 entirely when the radiologist does not own the equipment results in a denial or an incorrect payment.
- Billing for both global and component separately by mistake. If a practice submits a global bill and also submits a separate professional component bill for the same exam on the same date, the payer will flag it as a duplicate or an overpayment.
- Not verifying insurance before the scan. Coverage lapses happen. Plans change. If eligibility is not checked on the date of service, the practice may be billing a payer who has no obligation to pay.
- Ignoring timely filing deadlines. Every payer has a window during which claims must be submitted. Missing it means the claim is denied and cannot be appealed on clinical grounds. The deadline is the deadline.
How to Catch Errors Before They Cost You
- Pre-submission claim scrubbing is the process of running claims through an automated validation tool before they are sent to the payer. Most billing platforms have this built in. It catches missing modifiers, invalid code combinations, and demographic errors before they reach the payer.
Billing software audit features allow billing managers to run reports on claim patterns, denial rates by code, and coder-level accuracy. These reports are worth reviewing weekly.
Peer review within the billing team means having a second set of eyes on complex claims before submission. This is especially useful for high-dollar studies like PET scans or complex interventional radiology procedures, where coding errors have significant financial consequences.
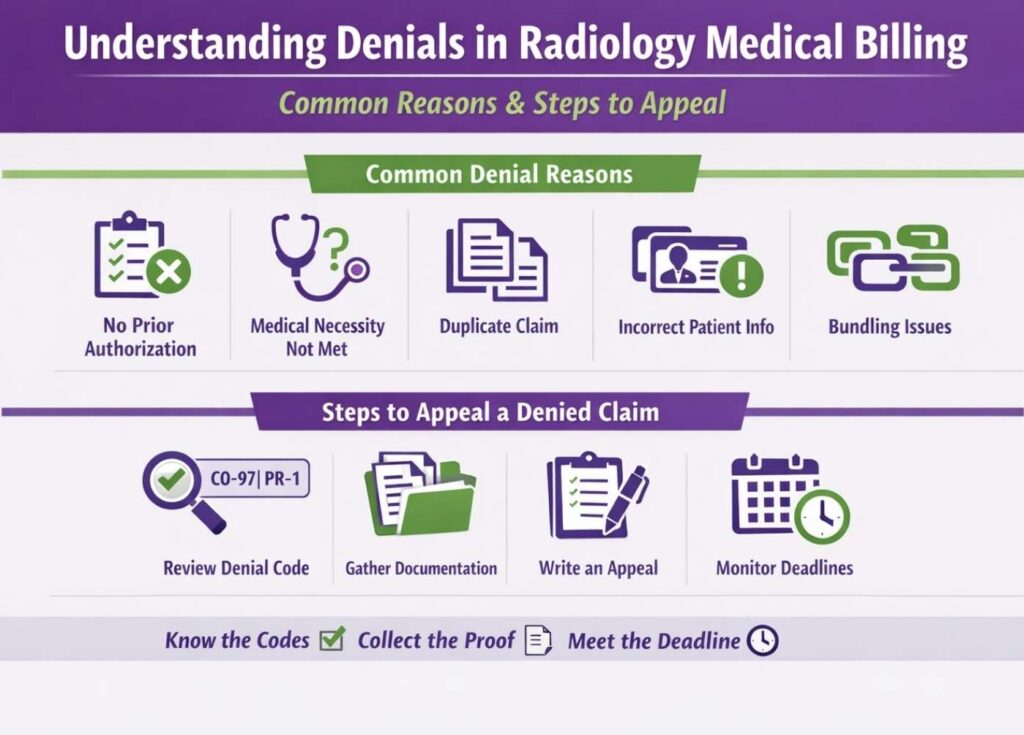
Understanding Denials in Radiology Medical Billing
Denial rates in radiology tend to run higher than in many other specialties because of the combination of high claim volume, prior authorization requirements, and the complexity of imaging-specific coding rules.
Most common denial reasons in radiology:
- No prior authorization on file
- Medical necessity not established by the diagnosis code submitted
- Duplicate claim submitted for the same service on the same date
- Incorrect patient information, such as the wrong date of birth or plan ID
- Bundling issues where two codes are being billed that the payer considers components of a single service
What to Do When a Claim Gets Denied
- Read the denial code carefully. Every denial comes with a reason code. CO-4 means the modifier is inconsistent with the procedure. CO-97 means the claim was bundled with another service. PR-1 means the patient is responsible for a deductible. Understanding the reason code determines the correct response.
- Gather supporting documentation. For medical necessity denials, pull the radiologist’s report, the referring physician’s order, and any relevant clinical notes. For authorization denials, pull the authorization number and the date it was obtained.
- Write a clear, factual appeal letter. The appeal should state what was billed, why it was appropriate, what the denial reason was, and why that denial was incorrect. Attach all supporting documentation. Keep the language factual and clinical.
- Track your appeal deadlines religiously. Payers have strict windows for appeals, often 60 to 180 days from the denial date. Missing the appeal deadline forfeits the right to collect on that claim.
Radiology Billing Compliance You Cannot Ignore
Compliance in billing means following the rules set by federal and state laws, payer contracts, and professional coding standards. It is not optional, and it is not just the legal department’s problem.
HIPAA Basics for Billing Departments
Patient information, including names, insurance IDs, diagnosis codes, and scan results, is protected health information (PHI). It cannot be shared outside the care and billing relationship without authorization. Billing teams handle PHI constantly, which means they need HIPAA training, secure systems, and clear policies about who can access what.
Anti-kickback and Stark Law basics
These federal laws prohibit financial arrangements between healthcare providers that could influence referrals. In radiology, this is relevant when a hospital or imaging center has financial relationships with referring physicians. A radiologist cannot offer a referring physician a financial incentive for sending patients their way. Violations carry significant penalties.
Red Flags That Could Trigger an Audit
Payers and federal agencies use data analytics to identify billing anomalies. The following patterns attract scrutiny:
- Unusually high billing volume for one specific CPT code compared to similar practices in the same geographic area
- Billing for services without complete and signed documentation in the medical record
- Consistent use of high-complexity or high-reimbursement codes when the clinical record does not support it
- Ignoring payer-specific billing rules and submitting claims that routinely violate bundling edits
- Billing Modifier 59 frequently without documented clinical justification for unbundling
Tools and Resources That Make Radiology Medical Billing Easier
No billing team works from memory alone. These are the resources worth using consistently.
- Billing software with radiology-specific claim scrubbing, prior authorization tracking, denial analytics, and ERA posting capabilities significantly reduces manual work and error rates. The specific platform matters less than whether the team is trained to use its features.
- The AMA CPT code lookup tool is the authoritative reference for code selection. When there is uncertainty about which code applies, this is the first stop.
- CMS Medicare fee schedules are published annually and show exactly what Medicare reimburses for every CPT code in every region. For practices that serve a significant Medicare population, tracking these numbers helps with revenue forecasting and contract negotiation.
- RBMA (Radiology Business Management Association) resources include benchmarking data, compliance guidance, coding updates, and peer networking. Their publications are practical and radiology-specific in a way that general healthcare billing resources are not.
Should You Get Certified?
Certification matters in this field. It signals competency to employers and tends to correlate with higher compensation.
- CPC (Certified Professional Coder) from AAPC is the most widely recognized credential in outpatient coding. It covers the foundational coding knowledge that applies across specialties, including radiology.
- CRC (Certified Risk Adjustment Coder) and specialty-specific credentials like the Radiology Coding Certificate from AAPC are relevant for those who want to focus specifically on imaging.
Certification typically requires passing an exam and maintaining continuing education credits annually. The investment is worth it. According to AAPC salary surveys, certified coders consistently earn more than non-certified coders in equivalent roles, and they tend to make fewer costly errors.
How to Improve Radiology Billing and Coding
Improvement in radiology billing does not happen through one big initiative. It happens through consistent attention to the small things that add up over time.
1. Standardize Documentation Requirements
Work with the radiology group to establish what every report must include before it can be coded and billed. At a minimum: the heading, number of views, clinical indication, findings, impression, and physician signature. Create a report template if one does not exist. Build a quality check into the workflow before reports are sent to the billing team.
2. Conduct Monthly Denial Analysis
Pull denial reports by reason code, by payer, and by CPT code every month. Patterns will emerge. If 30 percent of your MRI denials are for missing authorization, the problem is upstream in the scheduling and authorization workflow, not in the coding. Fix the root cause, not just the symptom.
3. Build Payer-Specific Billing Guides
Each major payer has its own rules. Document them. What requires authorization with Payer A may not require it with Payer B. What Payer C considers bundled, Payer D may reimburse separately. These nuances are institutional knowledge that should be written down, updated regularly, and accessible to every member of the billing team.
4. Invest in Coder Training
Send coders to AAPC webinars when CPT codes are updated. Subscribe to CMS update notifications. Build a brief monthly review into team meetings where recent coding changes or payer policy updates are discussed. The cost of training is far lower than the cost of coding errors.
5. Negotiate Payer Contracts Proactively
Payer contracts are not fixed. Reimbursement rates can be negotiated, especially for practices with high volume or specialized capabilities. Review contracts annually and benchmark rates against the Medicare fee schedule. If a payer is reimbursing at or below Medicare rates, that is a negotiation conversation worth having.
6. Use Technology to Close Gaps
Automated eligibility verification, prior authorization tracking, and real-time claim scrubbing reduce the manual workload and catch errors before they become denials. If the practice is still handling these steps manually, the volume and complexity of radiology billing will eventually overwhelm the team.
Final Words
Radiology billing is genuinely hard. The volume is high, the codes are specific, the modifiers matter, the authorizations are mandatory, and the compliance stakes are real. But it is also learnable, manageable, and improvable with the right systems and the right knowledge.
The practices that perform best in radiology billing are not the ones with the most complex software or the largest billing teams. They are the ones who know when to bring in the right help.
Professional service providers, like Transcure, handle the complexity, so your clinical team stays focused on patients, not paperwork. Whether you need radiology billing services in California or professional radiology billers in New York, we have you covered. Or, you can start with the basics, build strong workflows, train your people, and stay current with coding changes. That is the work. And it is worth doing well.