CPT code 71250 is a diagnostic radiology code used to report computed tomography of the thorax performed without intravenous contrast material. It applies when the radiologist or ordering provider determines that a non-contrast protocol is appropriate, due to contrast contraindication, clinical indication, or protocol design. This code is used across inpatient, hospital outpatient, ASC, and freestanding imaging center settings for evaluation of pulmonary, mediastinal, pleural, and thoracic structural pathology.
What Is the Description of CPT Code 71250?
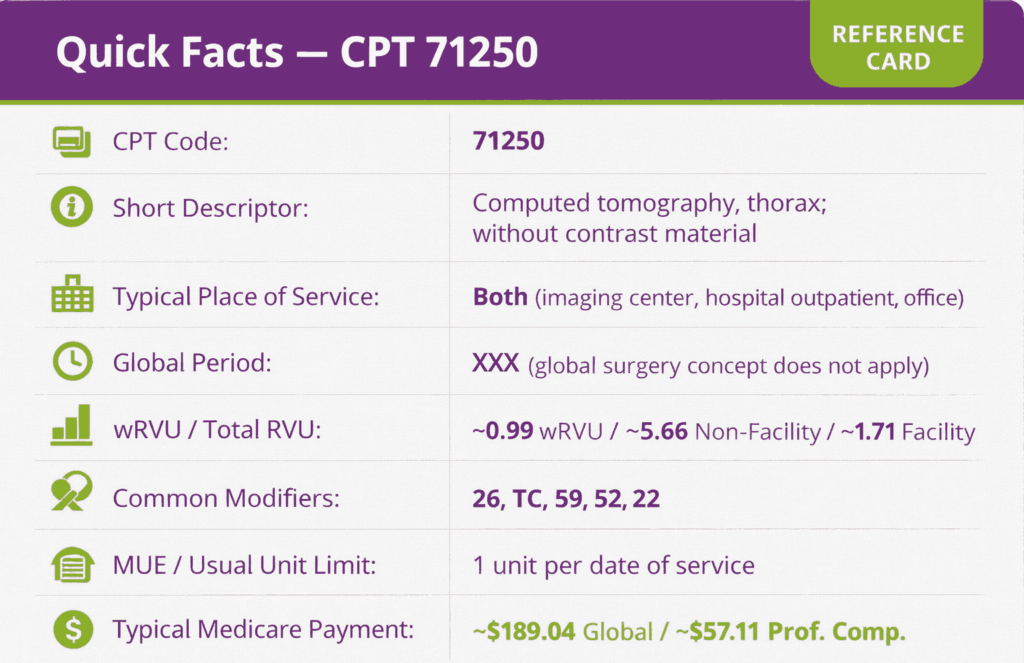
CPT code 71250 is defined by the AMA as: “Computed tomography, thorax, diagnostic; without contrast material.”
It covers a complete CT acquisition of the thorax using standard or high-resolution protocol without the administration of intravenous contrast. The radiology report must explicitly state that no contrast was administered for this code to be correctly supported.
What Anatomical Structures Are Evaluated Under CPT Code 71250?
The CT examination reported under 71250 CPT code evaluates all structures within the thoracic cavity, including the lungs and lung parenchyma, airways (trachea and bronchi), pleural spaces, mediastinum and mediastinal lymph nodes, pericardium, thoracic aorta and great vessels (without vascular enhancement), chest wall, ribs, thoracic spine, and diaphragm. High-resolution CT (HRCT) protocols for evaluation of interstitial lung disease are reported under CPT code 71250. No separate code exists for HRCT of the thorax. The specific acquisition protocol used does not change the code reported, provided no contrast is administered.
How Does CPT Code 71250 Differ From CPT 71260 and 71270?
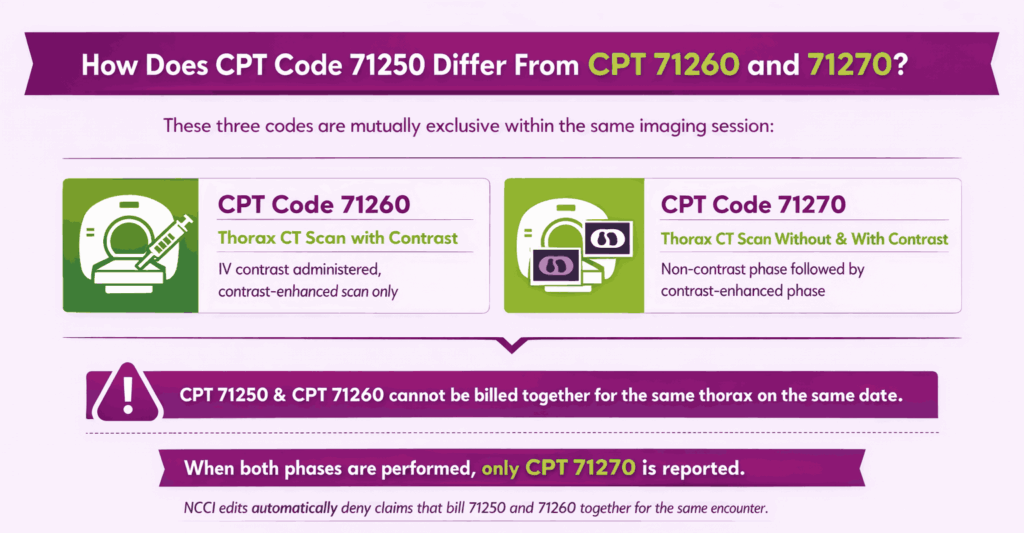
These three codes are mutually exclusive within the same imaging session for the same thorax and are distinguished solely by contrast administration:
- CPT Code 71260: Computed tomography, thorax, diagnostic; with contrast material(s). Used when intravenous contrast is administered and only a contrast-enhanced acquisition is performed
- CPT Code 71270: Computed tomography, thorax, diagnostic; without contrast material(s), followed by contrast material(s) and further sections. Used when a meaningful non-contrast phase is acquired and then immediately followed by a contrast-enhanced phase as a single combined exam
CPT code 71250 and code CPT 71260 must not be billed together for the same thorax on the same date. When both phases are performed, only CPT 71270 is reported. NCCI edits automatically denies claims that bill 71250 and 71260 together for the same encounter.
What Are the Modifiers for CPT Code 71250?
CPT 71250 is a diagnostic radiology code with a PC/TC indicator of 1, meaning the professional and technical components can be billed separately depending on the practice setting.
Modifier 26: Professional Component Only
Modifier 26 is appended when the interpreting physician bills only for the reading, interpretation, and written report of the CT scan, and the technical component (scanner, technologist, facility) is billed separately by the facility or imaging center. Append modifier 26 to code CPT 71250 on the physician’s claim whenever the physician does not own or operate the imaging equipment.
Modifier TC: Technical Component Only
Modifier TC is appended by the facility or imaging center billing for the equipment, technologist, supplies, and facility overhead used to acquire the CT images. The physician’s interpretation is not included when the modifier TC is billed. Append modifier TC to the 71250 code CPT on the facility’s claim when the reading physician bills separately with modifier 26.
Modifier 59: Distinct Procedural Service
Modifier 59 is used when CPT code 71250 is performed as a distinct and separately identifiable service from another imaging or procedure on the same date. It is used to override an NCCI edit when documentation supports a separate clinical indication or distinct anatomical region. Append modifier 59 only when documentation clearly establishes the basis for separate billing.
Modifier 52: Reduced Services
Modifier 52 is used when the CT examination is partially performed or the standard protocol is reduced at the physician’s discretion. Append modifier 52 and document in the radiology report the reason the complete protocol was not performed.
Modifier 22: Increased Procedural Services
Modifier 22 is used when the complexity of the examination substantially exceeds the typical service, for example, when extensive post-processing, multi-volume reconstruction, or significantly prolonged interpretation is required. Append modifier 22 with a supporting letter documenting the basis for the increased work. This modifier is rarely applicable to routine CT thorax studies.
When Should CPT 71250 Be Billed Globally vs. With Modifier 26 or TC?
The correct billing approach depends entirely on who performs and owns each component of the service:
- Global billing (no modifier): Used when the same entity, typically a freestanding imaging center or an integrated outpatient practice, performs both the technical acquisition and the professional interpretation. One claim for procedure code 71250 without any modifier covers both components.
- Modifier 26 (professional only): Used by the interpreting radiologist when the technical component is performed and billed separately by the hospital, ASC, or imaging facility. The physician submits CPT code 71250-26.
- Modifier TC (technical only): Used by the facility that owns the CT equipment and employs the technologist. The facility submits CPT code 71250-TC.
Billing the global code when another entity is billing the TC or billing both 26 and TC on the same claim creates a duplicate payment denial. CMS’s Medicare Claims Processing Manual governs how component billing is handled, and providers should ensure their billing workflows are clearly defined to avoid this.
Which Documents Are Required For CPT Code 71250?
Documentation for the 71250 procedure code must support both the medical necessity of the examination and the accuracy of the code selected.
Required documents checklist:
- Physician order or referral documenting the clinical indication for CT thorax
- Radiology report explicitly stating that no intravenous contrast was administered
- Radiology report documenting the anatomical structures evaluated and findings
- Documentation of the clinical indication (diagnosis, signs, or symptoms) linking to the order
- CDSM (Clinical Decision Support Mechanism) consultation documentation, where required under PAMA (Protecting Access to Medicare Act), for applicable advanced imaging services
- If HRCT protocol used, documentation indicating the specific protocol and clinical rationale
- Technologist acquisition record confirming no contrast was used
What is the Cost of CPT Code 71250?
The cost of CPT code 71250 varies by billing component (global, professional, or technical), place of service, payer, and geographic location.
RVUs & Medicare Payment
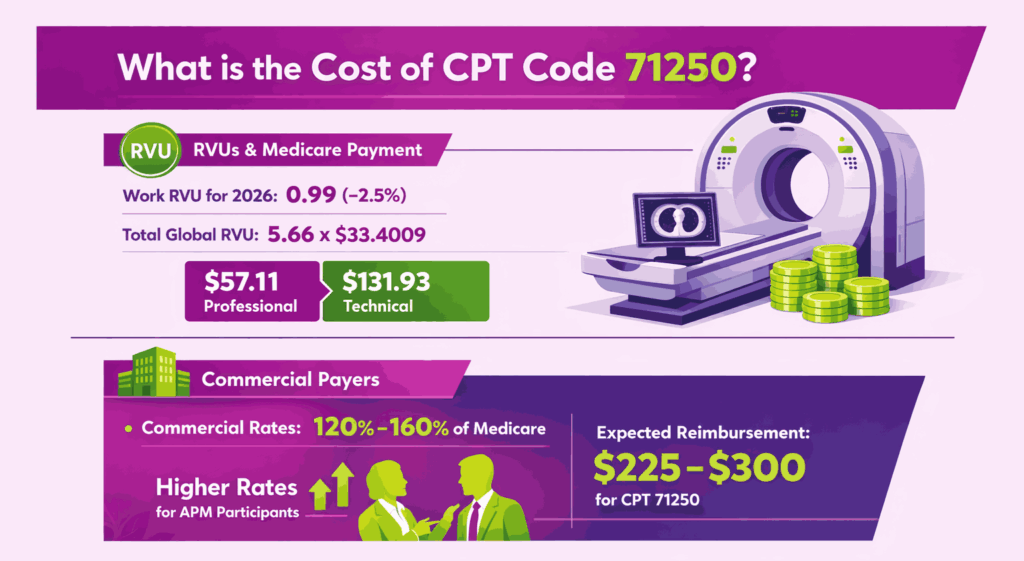
Medicare reimbursement is built on Relative Value Units (RVUs) that quantify the complexity and resources required for the scan. For 2026, the Work RVU (wRVU) has been adjusted to 0.99 following a finalized -2.5% efficiency reduction for non-time-based diagnostic codes.
The Total Global RVU stands at 5.66, which accounts for the high overhead of CT equipment and technical staff. When multiplied by the 2026 non-APM conversion factor of $33.4009, the resulting professional payment for interpretation is $57.11, while the technical component for the scan itself is valued at $131.93.
Commercial Payers
Commercial insurance rates generally track with Medicare but at a significant premium, typically ranging from 120% to 160% of the federal baseline. For 71250, this places the expected commercial reimbursement between $225 and $300 for global billing. Most private payers in 2026 have also adopted the Dual Conversion Factor logic, providing slightly higher rates for groups participating in Advanced Alternative Payment Models (APMs).
Place-of-Service & Geographic Adjustments
The final “on-the-check” amount for code 71250 CPT is modified by the Geographic Practice Cost Index (GPCI), which scales payments to match local costs for labor and rent; thus, a scan in a high-cost urban center will yield a higher payment than one in a rural setting. Furthermore, the Place of Service (POS) determines which entity receives the funds. In an office setting (POS 11), the provider bills the global fee of $189.04. In a hospital outpatient setting (POS 22), the physician only receives the $57.11 professional component, while the facility bills separately for the technical costs under the hospital’s prospective payment system.
What Are Example Clinical Scenarios or Use Cases for CPT Code 71250?
CPT code 71250 applies when CT of the thorax is performed without contrast, supported by a clinical indication that does not require contrast enhancement.
Scenario 1: Pulmonary Nodule Follow-Up in a Former Smoker
ICD-10: R91.8 (Other nonspecific abnormal finding of lung field)
The patient is a 62-year-old former smoker with a 6mm pulmonary nodule identified on a prior chest CT, now presenting for scheduled 12-month surveillance imaging per Fleischner Society guidelines. No contrast is required for nodule size and morphology assessment. The radiologist performs and interprets a non-contrast CT thorax, supporting the CPT 71250 code as the correct code.
Scenario 2: Suspected Interstitial Lung Disease Requiring High-Resolution Protocol
ICD-10: J84.10 (Pulmonary fibrosis, unspecified)
The patient presents with progressive dyspnea and bilateral basilar crackles on auscultation. The ordering pulmonologist requests HRCT of the chest to evaluate for interstitial lung disease. The radiologist performs a high-resolution non-contrast CT protocol with thin-section acquisitions through the lungs. Since no contrast is administered, CPT code 71250 is the correct code regardless of the specialized HRCT acquisition protocol.
Scenario 3: Contrast Contraindicated in a Patient with Renal Insufficiency and Chest Symptoms
ICD-10: R09.89 (Other specified symptoms and signs involving the circulatory and respiratory systems)
The patient has an eGFR of 22 mL/min/1.73m² and presents with new-onset chest pain and dyspnea. Contrast-enhanced imaging is contraindicated due to severe renal insufficiency. The ordering physician requests a non-contrast CT thorax to evaluate for pneumonia, pleural effusion, or mass lesion. Code CPT 71250 is reported. The radiology report documents the absence of contrast and the clinical justification for the non-contrast protocol.
What Are the CPT Code 71250 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for contrast code selection, component billing, medical necessity, and CDSM compliance. Meeting these rules reduces denials and ensures correct payment when it comes to applying all sorts of CPT codes.
Bundling / NCCI / Same-Day Procedure Rules
CPT code 71250 must not be reported alongside CPT 71260 for the same thorax on the same date. When both non-contrast and contrast phases are acquired in a single session for the same anatomical area, only CPT 71270 is reported. NCCI edits automatically deny simultaneous billing of 71250 and 71260. If a CT thorax and a CT abdomen/pelvis are performed separately on the same date, each may be reported independently with appropriate codes and modifiers, as they cover distinct anatomical regions.
Units, MUEs & Medical Necessity Requirements
CPT code 71250 is billed as one unit per date of service per anatomical site.
- Medical necessity must be established by the clinical indication documented on the order and confirmed in the radiology report; payers may deny claims where the diagnosis code does not support the clinical rationale for a non-contrast protocol
- PAMA requires ordering physicians for certain advanced imaging services to consult a CMS-approved CDSM and document the consultation on the claim. The CPT 71250 code may be subject to this requirement when ordered by applicable practitioners. Confirm with your MAC
- Repeat CT thorax studies within a short interval require documentation of a new clinical development or change in clinical status to support medical necessity and avoid frequency-based denials.
- CPT code 71250 carries a 0-day global period. No postoperative bundling applies.
When CPT 71250 Cannot Be Billed Separately from 71260 or 71270
CPT code 71250 cannot be separately reported in the following circumstances:
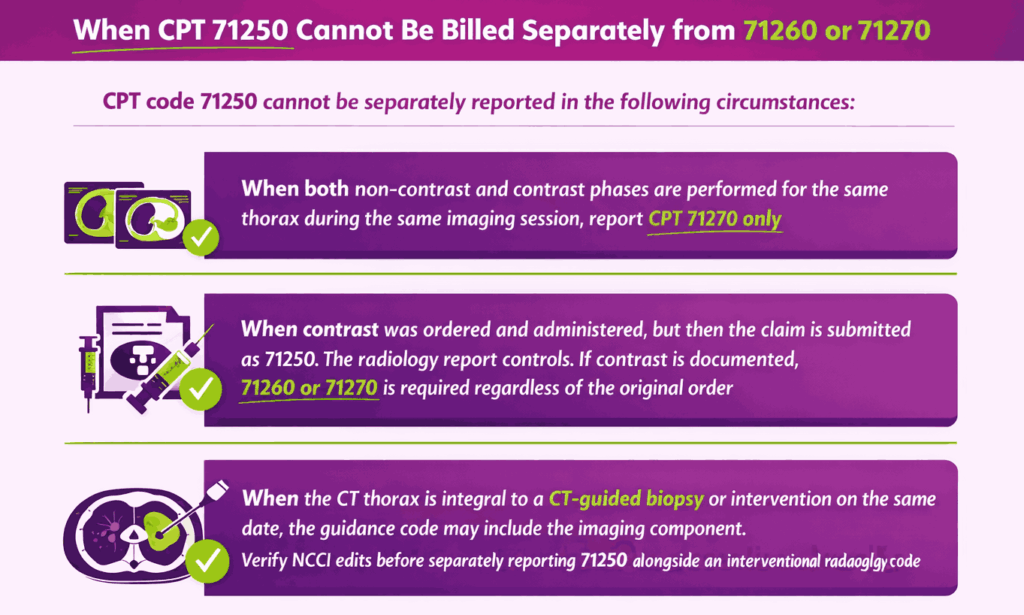
- When both non-contrast and contrast phases are performed for the same thorax during the same imaging session, report CPT 71270 only
- When contrast was ordered and administered, but then the claim is submitted as 71250, the radiology report controls. If contrast is documented, 71260 or 71270 is required regardless of the original order
- When the CT thorax is integral to a CT-guided biopsy or intervention on the same date, the guidance code may include the imaging component. Verify NCCI edits before separately reporting 71250 alongside an interventional radiology code.
Top Reasons For Denials Specific To 71250 & Quick Remedies
- Wrong Contrast Code Selected (71250 vs. 71260 or 71270): Prevent by cross-checking the radiology report for contrast documentation before selecting the code. The report governs, not the order.
- Duplicate Billing of Professional and Technical Components: Prevent by ensuring the interpreting physician bills 71250-26 and the facility bills 71250-TC, never allowing both parties to bill globally or for the same component.
- Missing or Insufficient Medical Necessity Documentation: Prevent by linking a specific, supported ICD-10 diagnosis to the order and confirming the radiology report documents the clinical indication.
- CDSM Non-Compliance Under PAMA: Prevent by verifying whether the ordering physician is subject to CDSM requirements and confirming the consultation is documented on the claim before submission.
How do Insurance Companies Categorize Different Medical Imaging Procedures?
Payers rely on a standardized list of CPT codes in medical billing to differentiate between services like a CT scan without contrast and one with contrast. These numeric codes ensure that every diagnostic test is identified accurately so the provider is reimbursed at the correct rate for the resources and expertise used.