
Nephrology billing KPIs are measurable metrics that track the financial and operational health of a nephrology practice’s revenue cycle. They cover claim accuracy, collection speed, denial patterns, and coding compliance across dialysis and kidney care services.
The most watched KPIs in nephrology billing include clean claim rate, days in accounts receivable, denial rate, and net collection rate. Each one ties directly to how quickly and accurately a practice collects revenue from payers.
Nephrology-specific challenges add complexity to these metrics. MCP coding errors, ESRD bundled payment rules, and capitation lag all distort standard benchmarks. This article covers the primary KPIs to track, their benchmarks, the challenges unique to nephrology, and the strategies that improve them.
What are the Key Nephrology Billing KPIs to Track?
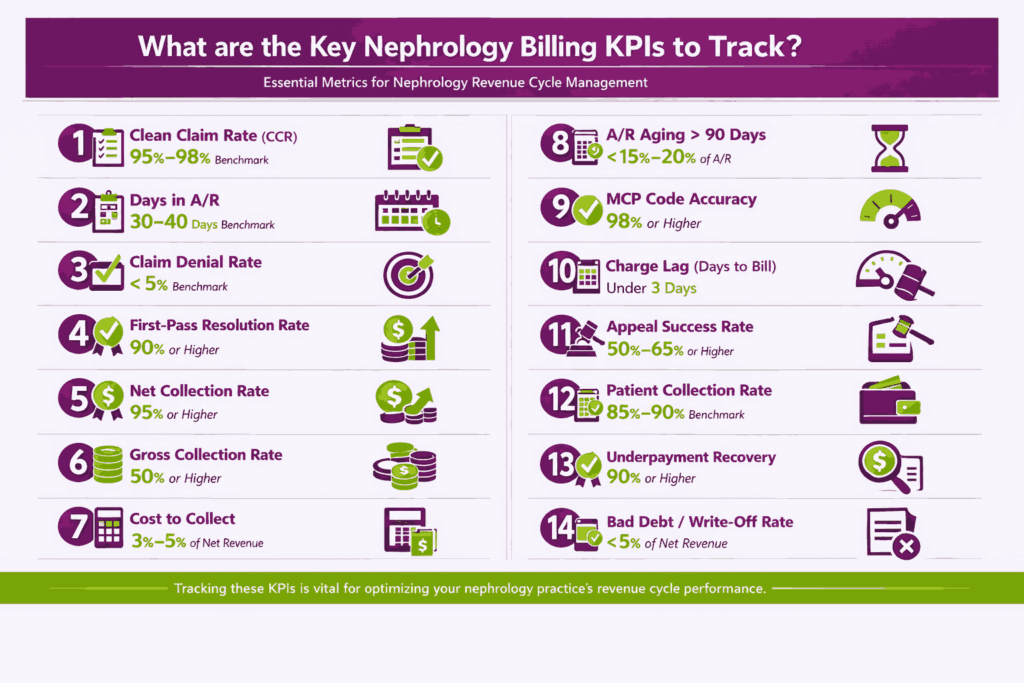
The key nephrology billing KPIs to track are the metrics that measure claim quality, collection speed, denial activity, and coding accuracy. Each one targets a different point in the revenue cycle.
1. Clean Claim Rate (CCR)
Clean Claim Rate is the percentage of claims submitted without edits, rejections, or rework on the first submission. It is one of the most direct indicators of billing quality in any specialty.
The formula is straightforward: (clean claims ÷ total claims submitted) × 100. A claim qualifies as “clean” only if it passes through payer adjudication without requiring resubmission or correction.
- CCR is foundational for nephrology because ESRD bundled-payment rules make claim scrubbing critical
- Incorrect MCP codes, missing CMS-2728 forms, and vascular access documentation errors all reduce CCR.
- Dialysis claims bundled under ESRD PPS carry strict inclusion and exclusion rules that must be scrubbed pre-submission
The best-in-class benchmark for clean claim rate is 95 to 98 percent. Practices consistently below 93 percent typically have upstream issues in eligibility verification, coding accuracy, or documentation completeness.
2. Days in Accounts Receivable (Days in A/R)
Days in A/R is the average number of days it takes a practice to collect payment after a service is delivered. It is one of the most reliable indicators of revenue cycle speed.
The formula is: total A/R ÷ average daily charges. Average daily charges are calculated by dividing total charges over a period by the number of days in that period.
- Dialysis-heavy practices often see elevated A/R due to Medicare-as-secondary payer situations.
- Capitation lag from MCP billing pushes Days in A/R higher because claims cannot be submitted until the month-end
- Secondary payer coordination periods for dual-eligible patients create additional collection delays.
The benchmark for well-run nephrology RCM is 30 to 40 days. MGMA data suggests that high-performing physician practices operate closer to 30 days, while nephrology-specific payer mix dynamics often push this toward the higher end.
3. Claim Denial Rate
Claim Denial Rate is the percentage of claims denied by payers during an evaluation period. It is calculated as: (denied claims ÷ total submitted claims) × 100.
Denial rate is a lagging indicator that reflects problems in eligibility, coding, authorization, and documentation. A rising denial trend signals upstream process breakdowns that need root cause analysis.
The most common nephrology denial drivers include:
- MCP visit frequency errors where documented visits do not match the code tier billed
- Missing vascular access documentation required for dialysis-related procedure claims
- Incomplete or missing CMS-2728 forms that Medicare requires for ESRD patients
- Incorrect bundling where separately billed services fall inside the ESRD PPS composite rate
The benchmark is below 5 percent, with best-in-class practices operating below 3 percent. Practices with denial rates above 8 percent are likely losing significant revenue to rework and write-offs.
4. First-Pass Resolution Rate (FPRR)
First-Pass Resolution Rate is the percentage of claims paid on first submission without any intervention, appeal, or resubmission. It measures how often the revenue cycle gets it right the first time.
FPRR is closely related to both CCR and the denial rate. A high CCR does not guarantee a high FPRR because payer processing issues can still delay or deny otherwise clean claims.
- FPRR is a leading indicator of coding and eligibility quality in nephrology billing
- It reflects the combined accuracy of pre-authorization, documentation, and code selection.
- Tracking FPRR by payer reveals which payers require the most rework
The benchmark for FPRR is 90 percent or higher. Practices below 85 percent should audit their claim submission workflows and payer-specific denial patterns.
5. Net Collection Rate (NCR)
Net Collection Rate measures the percentage of collectible revenue that a practice actually collects. Collectible revenue means billed charges minus contractual adjustments.
The formula is: (payments ÷ (charges – contractual adjustments)) × 100. This metric excludes write-offs that were negotiated as part of payer contracts, isolating the revenue a practice should be collecting.
- NCR measures the A/R follow-up team’s performance in collecting what is owed
- It accounts for payer-specific fee schedules and contractual reductions
- A declining NCR signals problems in follow-up, underpayment identification, or patient collections
The benchmark is 95 percent or higher. Practices below 92 percent are likely to have gaps in A/R follow-up, uncollected patient balances, or unidentified underpayments from payers.
6. Gross Collection Rate (GCR)
Gross Collection Rate is the total payments received divided by total billed charges. It is the simplest collection metric, but also the most misleading when used for cross-practice comparison.
GCR is useful for internal trending over time. It shows whether the ratio of collections to charges is stable, improving, or declining within the same practice and payer mix.
- Fee-schedule differences between practices make GCR unreliable for benchmarking against other groups.
- ESRD bundled payments compress GCR because the per-treatment reimbursement is fixed regardless of billed charges
- A practice with high charges and low contractual rates will show a low GCR even with strong collections.
GCR should be interpreted against payer mix. A Medicare-heavy nephrology practice will have a structurally lower GCR than a practice with a larger commercial payer share.
7. Cost to Collect
Cost to Collect is the total cost of revenue cycle management divided by total collections. It answers the question: how much does it cost the practice to collect each dollar of revenue?
Nephrology practices need to track this metric alongside collection rates. A practice with a 96 percent NCR but a 7 percent cost to collect may be less profitable than one at 94 percent NCR and 4 percent cost to collect.
- The typical industry range for cost to collect is 3 to 5 percent of net revenue.
- In-house billing teams with high denial rework cycles tend to push the cost to collect above 6 percent.
- Outsourced nephrology RCM partners typically operate in the 4 to 7 percent range, depending on volume.
Cost to collect is directly affected by denial rework cycles. Every denied claim that requires resubmission adds labor cost to the collection process.
8. A/R Aging > 90 Days
This KPI measures the percentage of total accounts receivable that is older than 90 days. It signals how much revenue is sitting uncollected past a reasonable payment window.
A/R aging is particularly revealing in dialysis billing because of recurring monthly billing cycles. A healthy dialysis practice should show minimal carryover from one month to the next in its receivables.
- Aged A/R in the greater-than-120-day bucket signals systemic follow-up gaps
- Recurring dialysis claims stuck past 90 days often involve secondary payer coordination issues.
- Stale A/R reduces the likelihood of collection and increases eventual write-off risk.
The benchmark is below 15 to 20 percent of total A/R. Practices with more than 25 percent of A/R past 90 days should audit their follow-up workflows by payer and claim type.
9. MCP (Monthly Capitation Payment) Code Accuracy Rate
This nephrology-specific KPI measures the percentage of MCP claims coded at the correct level based on documented face-to-face visits. MCP codes range from 90951 to 90970 and are selected by patient age and visit frequency.
The revenue impact of miscoding is significant. The difference between CPT 90961 (two to three visits) and 90960 (four or more visits) is approximately $205 per patient per month.
| MCP Code | Age Group | Visit Requirement | Description |
|---|---|---|---|
| 90960 | 20+ years | 4+ visits/month | Full-month, highest tier |
| 90961 | 20+ years | 2-3 visits/month | Full-month, mid tier |
| 90962 | 20+ years | 1 visit/month | Full-month, lowest tier |
| 90967 | 20+ years | Per day | Partial-month daily code |
You can find detailed strategies for preventing this type of leakage in our comprehensive billing guide for nephrology practices, which simplifies complex visit-count rules. Practices managing 50 to 80 ESRD patients can lose $10,000 or more per month from coding at the wrong tier. The target accuracy rate is 98 percent or higher.
10. Charge Lag (Days to Bill)
Charge Lag is the average number of days between the date of service and the date of charge entry into the billing system. Long charge lags delay cash flow and increase the risk of timely-filing denials.
Different nephrology service types carry distinct lag profiles. Dialysis sessions billed monthly through MCP codes have a built-in lag. Inpatient rounding and vascular access procedures often lag due to documentation turnaround.
- MCP claims cannot be submitted until the month ends, creating a structural lag of up to 30 days
- Vascular access procedures billed separately often wait on operative notes
- Inpatient consults depend on hospital discharge summaries for accurate coding
The benchmark for charge lag is fewer than 3 days for non-MCP services. Practices exceeding 5 days should review their documentation and charge capture workflows.
11. Appeal Success Rate
Appeal Success Rate is the percentage of appealed denials that are overturned by the payer. It measures the effectiveness of the appeals process in recovering denied revenue.
This KPI is especially relevant for nephrology. Medical necessity denials and MCP visit-count denials are frequently reversible with proper documentation and clinical support.
- Appeals should be categorized by root cause and payer to identify patterns
- Medical necessity denials for dialysis-related services often succeed on appeal with clinical documentation
- MCP visit-count denials can be overturned when the practice provides a complete visit log
The benchmark for appeal success rate is 50 to 65 percent or higher. Practices below 40 percent should evaluate whether their appeal letters include sufficient clinical documentation.
12. Patient Collection Rate
Patient Collection Rate is the percentage of patient financial responsibility that a practice successfully collects. This includes copays, deductibles, and coinsurance amounts owed after payer adjudication.
The importance of this KPI is rising as high-deductible health plans grow among CKD patients. More financial responsibility is shifting to patients, which makes point-of-service collection critical.
Best practices for improving patient collections include:
- Time-of-service collection, where copays and known balances are collected at check-in
- Payment plan options for patients with high out-of-pocket balances
- Automated patient statements are sent at regular intervals after payer adjudication
- Eligibility verification that identifies patient responsibility before the visit
The benchmark for patient collection rate is 85 to 90 percent or higher.
13. Underpayment Recovery Rate
Underpayment Recovery Rate is the percentage of identified underpayments that are successfully recovered from payers. An underpayment occurs when the payer reimburses less than the contracted or allowed amount.
Contract modeling against ESRD fee schedules is the primary method for surfacing underpayments. Dialysis claims are especially prone to underpayment because bundled rates and modifiers create multiple points of potential variance.
- Variance reporting compares the expected payment (per contract) against the actual payment for each claim.
- Payer escalation workflows route identified underpayments through formal dispute channels.
- Automated variance tools flag underpayments in real time rather than waiting for manual review
The target for underpayment recovery is 90 percent or higher on identified underpayments. Practices without a contract-modeling system in place are very likely to be missing underpayments.
14. Bad Debt / Write-Off Rate
Bad Debt Rate measures write-offs as a percentage of net revenue. It captures the revenue that a practice has determined is uncollectible and has removed from its books.
Excessive write-offs indicate weaknesses in eligibility verification, pre-authorization, and A/R follow-up. Not all write-offs are avoidable, but separating contractual write-offs from avoidable ones is critical.
| Write-Off Type | Definition | Avoidable? |
|---|---|---|
| Contractual | Difference between billed charge and allowed amount per contract | No |
| Timely filing | Claim denied because it was submitted past payer deadline | Yes |
| Eligibility | Claim denied due to patient not covered at date of service | Yes |
| Medical necessity | Claim denied for insufficient clinical justification | Often |
| Patient bad debt | Patient balance deemed uncollectible | Partially |
The benchmark for avoidable write-offs is below 5 percent of net revenue. Practices should review write-off categories monthly to identify preventable patterns.
Why are KPIs Important in Nephrology Billing?
KPIs are important in nephrology billing because they provide measurable visibility into revenue leakage, cash-flow predictability, ESRD compliance, and payer-performance patterns. Without them, practices operate on assumptions rather than data.
Nephrology billing carries specialty-specific complexity that makes blind spots more expensive than in general practice. Bundled ESRD payments, MCP coding tiers, and Medicare-as-secondary dynamics all create revenue risk that only KPI tracking can surface early.
Financial Performance Visibility
KPIs give nephrology practices real-time insight into cash flow, collections, and reimbursement trends. They convert raw billing data into a picture of where money is coming from and where it is getting stuck.
Tracking net revenue per treatment and per patient month exposes underperformance at the payer level. A practice may have a healthy overall NCR but find that one Medicare Advantage plan consistently underpays.
- Linking clinical volume (dialysis sessions, MCP visits) to financial outcomes reveals revenue per unit of care.
- Payer-level breakdowns show which contracts are performing and which are eroding.
- Monthly trending surfaces seasonal or cyclical patterns in collections
This level of visibility turns revenue cycle management from a reactive function into a forward-looking one. Decisions about staffing, payer contracts, and service mix become data-driven.
Early Detection of Revenue Leakage
KPIs surface underpayments, missed MCP visit thresholds, and contractual variances before they compound. A single month of undetected MCP miscoding across 60 patients can mean $12,000 or more in lost revenue.
Denial-rate trends flag upstream issues in eligibility, authorization, or documentation. A rising denial rate in a specific payer signals a process breakdown that can be fixed before it becomes a pattern.
- Write-off and adjustment monitoring catch silent revenue loss that does not show up in the denial report.s
- Underpayment variance reports flag payer reimbursement below contracted amounts.
- Charge lag tracking prevents timely-filing denials that result in permanent revenue loss.
Revenue leakage in nephrology is often invisible without KPI monitoring. The recurring nature of dialysis billing means that small per-claim errors compound rapidly across large patient panels.
ESRD & CMS Compliance Alignment
Billing KPIs interact with ESRD Quality Incentive Program (QIP) quality measures and CMS bundled payment rules. The same documentation that supports accurate billing also supports compliance with federal quality programs.
Accurate MCP coding (90951 to 90970) is a compliance KPI as well as a revenue KPI. Miscoding an MCP claim is not just a revenue problem. It can trigger RAC audits, CERT reviews, or OIG investigations.
- ESRD QIP scores affect facility reimbursement through payment reductions of up to 2 percent
- KPI tracking supports audit readiness by maintaining documentation trails for every billed service
- CMS annual rule changes require KPI definitions to be updated each payment year
Practices that track billing KPIs alongside clinical quality measures are better prepared for audits and less likely to face recoupment demands.
Operational Performance & Staff Accountability
KPIs create accountability across front-desk, coding, billing, and A/R follow-up teams. Each team owns specific metrics that tie their work to financial outcomes.
Metrics like charge lag and days-to-bill pinpoint workflow bottlenecks. If charge lag spikes, the issue is likely in documentation turnaround or charge capture. If Days in A/R rise, follow-up is the bottleneck.
| Team | Primary KPI | What It Measures |
|---|---|---|
| Front desk | Eligibility verification rate | Pre-visit insurance confirmation |
| Coding | CCR, MCP accuracy | Claim accuracy at submission |
| Billing | Charge lag, FPRR | Speed and quality of claim submission |
| A/R follow-up | Days in A/R, A/R > 90 | Collection speed and persistence |
| Appeals | Appeal success rate | Recovery of denied revenue |
KPI dashboards allow practice managers to set performance targets for each team. Monthly reviews using these metrics create a culture of measurement.
Data-Driven Payer Negotiation
Payer-level KPIs like denial rate by payer, reimbursement variance, and underpayment percentage support contract renegotiation with concrete data. Anecdotal complaints about a payer carry less weight than a 12-month denial trend report.
Tracking allowed amounts versus billed amounts reveals rate erosion over time. A payer that reduces reimbursement by 2 percent per year across dialysis claims will not announce that change. Only variance reporting surfaces it.
- KPI evidence strengthens payer disputes and fee-schedule renegotiations
- Denial patterns by payer identify which contracts produce the most rework
- Underpayment data quantifies the dollar value of contract non-compliance
Practices that bring KPI data to payer negotiations consistently achieve better contract terms than those that negotiate without it.
What are the Industry Benchmarks for Nephrology Billing KPIs?
Industry benchmarks provide a reference point for evaluating nephrology billing performance against peers and national standards. Sources like MGMA, HFMA, and nephrology-specific data sets inform these benchmarks.
The table below summarizes benchmarks across all major nephrology billing KPIs.
| KPI | Benchmark | Source/Context |
|---|---|---|
| Clean Claim Rate | 95-98% | Industry standard across specialties |
| Days in A/R | 30-40 days | MGMA, nephrology trends toward upper range |
| Denial Rate | < 5% (best-in-class < 3%) | HFMA; nephrology-specific denials often higher |
| First-Pass Resolution Rate | 90%+ | Industry standard |
| Net Collection Rate | 95%+ | MGMA; Medicare-heavy mix may compress |
| Gross Collection Rate | Varies by payer mix | Not comparable across practices |
| Cost to Collect | 3-5% of net revenue | Industry range; nephrology typically 4-6% |
| A/R Aging > 90 Days | < 15-20% | Industry standard |
| MCP Code Accuracy | 98%+ | Nephrology-specific target |
| Charge Lag | < 3 days | Industry standard for non-MCP services |
| Appeal Success Rate | 50-65%+ | Industry range |
| Patient Collection Rate | 85-90%+ | Rising importance with HDHPs |
| Underpayment Recovery | 90%+ on identified | Specialty-specific target |
| Bad Debt / Write-Off Rate | < 5% avoidable | Industry standard |
What are the Challenges in Tracking Nephrology Billing KPIs?
Tracking nephrology billing KPIs is harder than tracking KPIs in general medical billing. The specialty includes unique payment models, coding structures, and payer dynamics that distort standard RCM metrics.
The most persistent challenges include ESRD bundled payment complexity, MCP coding errors, capitation lag, secondary payer delays, and data silos between dialysis facilities and nephrology practices.
ESRD Bundled Payment Complexity
The ESRD Prospective Payment System (PPS) is a Medicare bundled payment model for dialysis services. It pays dialysis facilities a single per-treatment rate that includes most dialysis-related services, labs, supplies, and certain medications.
Bundled per-treatment payments distort traditional charge-based KPIs. GCR and NCR calculations behave differently when a large share of revenue comes from fixed bundled rates rather than fee-for-service claims.
- Practices must separately track bundled and non-bundled services to get accurate KPI readings.
- Services included in the ESRD PPS bundle cannot be billed separately, but excluded services can be
- Misidentifying a service as inside or outside the bundle leads to either denied claims or missed revenue.
The downstream effect on GCR and NCR interpretation is significant. A practice cannot compare its GCR to a non-dialysis specialty without adjusting for the bundled payment structure.
MCP Code Miscoding (90951-90970)
MCP miscoding occurs when the billed MCP code does not match the actual number of documented face-to-face visits for that patient in the billing month. This is one of the most common and costly errors in nephrology billing.
The financial impact of selecting the wrong visit-tier code is direct and measurable. Billing 90961 instead of 90960 for one patient means roughly $205 less per month.
- The root cause is often that no single source of truth exists for visit counts across dialysis facilities and practice documentation.
- Facility-side records may show different visit dates than the practice’s own scheduling system.
- Manual visit reconciliation is error-prone and time-consuming across large patient panels.
Controls to prevent miscoding include centralized visit logs, monthly reconciliation workflows, and automated alerts when visit counts fall below the expected tier.
Capitation Lag in Revenue Recognition
This structural delay distorts Days in A/R because the clock starts at the date of service, but the claim is not submitted until weeks later. A service provided on the first of the month may not be billed until the second or third of the following month.
- Normalizing KPIs against the capitation cycle requires separate A/R tracking for MCP versus non-MCP claims.
- Reporting adjustments should exclude MCP claims from Days in A/R calculations during the billing month.
- Practices should track MCP-specific A/R as a distinct metric to avoid inflating overall Days in A/.R
Accurate trending requires that MCP and non-MCP revenue be reported on separate tracks. Blending them produces a misleading picture of collection speed.
How to Improve Nephrology Billing KPIs?
To improve nephrology billing KPIs, practices need targeted interventions at specific points in the revenue cycle. While general improvements help, the most successful practices work with specialized nephrology billing companies to implement strategies that produce rapid, measurable results.
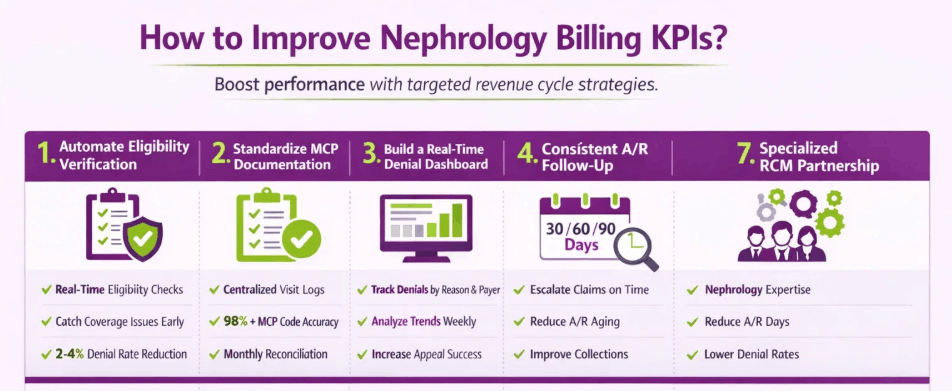
1. Automate Eligibility and Benefit Verification
Real-time eligibility checks before every dialysis session and office visit are the first line of defense against eligibility-related denials. Eligibility denials are the top denial category in nephrology billing.
Automation reduces the manual burden of checking insurance status for patients who come in three or more times per week. Batch eligibility checks can be run the day before scheduled dialysis sessions.
- Automated verification flags coverage changes, lapsed policies, and MSP coordination periods
- Real-time checks at the front desk catch issues before the service is rendered
- The expected impact is a measurable reduction in the denial rate and improvement in the clean claim rate.
Practices that move from manual to automated eligibility verification typically see denial rates drop by 2 to 4 percentage points within the first quarter.
2. Standardize MCP Visit Documentation
The process of reconciling scheduled visits, documented visits, and billed visits each month is the foundation of MCP coding accuracy. Without a centralized visit log, miscoding is almost inevitable across a large ESRD panel.
A centralized visit log records every face-to-face encounter by patient, date, and provider. It is reconciled against the billing system at month-end before MCP claims are submitted.
- The log should be updated in real time, not reconstructed at month-end from memory or scattered records.
- Monthly reconciliation compares the log against the PM system claim-ready data.
- The impact is a direct improvement in the MCP Code Accuracy Rate and net revenue per patient month.h
Practices that move to a centralized visit log consistently report MCP coding accuracy above 98 percent.
3. Build a Real-Time Denial Dashboard
A payer-by-denial-reason dashboard exposes root causes faster than monthly summary reports. When a denial spike happens in week two, the practice should know about it in week two.
Categorization using CARC/RARC codes combined with custom nephrology denial buckets (MCP, bundling, CMS-2728, vascular access) makes the data actionable.
- Real-time dashboards surface denial trends as they develop, not after the month closes
- Payer-specific views identify which contracts produce the most rework.
- The impact is a faster reduction in the denial rate and an increase in the appeal success rate.
The most effective dashboards display denial rate by payer, by denial reason, and by week. They also track the dollar value of denials to prioritize the highest-impact interventions.
4. Establish a Consistent A/R Follow-Up Cadence
The 30/60/90-day follow-up escalation model ensures that no claim sits untouched past its optimal collection window. Each aging bucket gets a defined action and owner.
Workqueues segmented by payer and claim balance direct follow-up resources to the highest-value claims first. A $5,000 dialysis claim at 45 days should get attention before a $150 office visit at 35 days.
| Aging Bucket | Action | Owner |
|---|---|---|
| 0-30 days | Monitor; verify claim received | Billing team |
| 31-60 days | First follow-up: check status with payer | A/R specialist |
| 61-90 days | Escalated follow-up; supervisor review | Senior A/R |
| 91-120 days | Formal appeal or secondary submission | Appeals team |
| 120+ days | Write-off review or collections referral | Management |
The impact is a measurable reduction in Days in A/R and a decrease in the percentage of A/R aging past 90 days.
5. Train Staff on Nephrology-Specific Codes and Rules
Ongoing training on MCP codes, vascular access CPTs, and ESRD 2728 documentation requirements is not optional. Nephrology billing rules change with each CMS annual update, and staff knowledge must keep pace.
Training should align with the CMS annual rule release cycle. The ESRD PPS final rule typically publishes in the fall for the following calendar year.
- Staff should be tested on MCP code selection, visit counting rules, and bundling exclusions.
- Vascular access coding (36818-36833 for creation, 36901-36906 for interventions) requires procedure-specific training.
- The impact is a measurable improvement in CCR, denial rate, and MCP accuracy.
Practices that invest in quarterly coding education sessions see sustained improvement in claim quality metrics over 12-month periods.
6. Put in Place Contract and Underpayment Modeling
Contract modeling compares expected payment per claim against actual payment received. Every variance is a potential underpayment that should be investigated.
Automated variance reports for dialysis bundles and MCP claims flag underpayments at the claim level. This removes the manual review burden and ensures no underpayment goes undetected.
- The most common underpayments in nephrology involve ESRD PPS rates, MCP reimbursements, and vascular access procedures.
- Payer escalation workflows route confirmed underpayments through formal dispute channels.
- The impact is a direct improvement in the Underpayment Recovery Rate and NCR.
To ensure no revenue is left behind, many practices partner with top-rated nephrology billing services that utilize advanced contract-modeling to capture every dollar owed. Even a 1 percent underpayment rate across a $5 million book of business represents $50,000 in recoverable revenue.
7. Outsource to a Specialized Nephrology RCM Partner
Outsourcing becomes cost-effective when the practice cost to collect exceeds industry benchmarks, denial rates are above 6 to 8 percent, or internal staff lack nephrology-specific coding expertise.
Selection criteria for a nephrology-specialized billing partner should include:
- Demonstrated experience with ESRD PPS billing and MCP code management
- Payer-specific denial trending and reporting capabilities
- Dedicated nephrology coding staff
- Contract modeling and underpayment recovery as standard service features
- Transparent reporting with access to real-time KPI dashboards
The KPI improvements include a 3 to 5% point improvement in CCR, a 15 to 25% reduction in A/R days, and denial rates below 5% within six months.
What is the Role of a Nephrology Billing Specialist in KPI Management?
A nephrology billing specialist is the person responsible for monitoring billing KPIs, analyzing denial trends, reconciling MCP visits, identifying underpayments, and reporting payer performance. This role bridges clinical documentation and financial outcomes.
The specialist responsibilities span the full revenue cycle.
- KPI monitoring includes daily review of key metrics and weekly reporting to practice leadership
- Denial trend analysis involves categorizing denials by CARC/RARC code, payer, and nephrology-specific reason.
- MCP visit reconciliation requires matching documented visits against billed MCP codes each month
- Underpayment identification uses contract modeling to flag claims reimbursed below contracted rates.
- Payer performance reporting tracks each payer’s denial rate, payment speed, and reimbursement accuracy.
The specialist uses nephrology-aware PM/RCM systems, clearinghouses with ESRD-specific edit libraries, and KPI dashboards that segment data by service line and payer.
The role bridges clinical documentation and financial outcomes. When a nephrologist’s documentation does not support the billed MCP tier, the specialist identifies the gap and works with clinical staff to correct it. When a payer consistently underpays dialysis claims, the specialist builds the case for a contract dispute.
How Do Nephrology Billing KPIs Differ From General Medical Billing KPIs?
Nephrology billing KPIs differ from general medical billing KPIs in several structural ways that affect how metrics are calculated, benchmarked, and interpreted.
- Payment Model: Nephrology uses ESRD PPS bundled payments and MCP capitation alongside fee-for-service, while general billing is predominantly fee-for-service
- Recurring Capitation Cycles: MCP billing creates monthly recurring claims with month-end submission rules, unlike episodic billing in most specialties
- Payer Mix: Nephrology practices are heavily Medicare-weighted, which compresses GCR and affects NCR benchmarks
- Code Complexity: MCP codes (90951-90970) require visit counting, age-based selection, and monthly reconciliation not found in other specialties
- Quality Program Linkage: ESRD QIP links facility reimbursement to clinical quality scores, adding a compliance dimension to billing KPIs
- Secondary Payer Dynamics: The 30-month MSP rule for ESRD patients creates dual-payer coordination that extends A/R cycles and complicates payment tracking
These differences mean that general RCM benchmarks should not be applied to nephrology without adjustment.
How Do ESRD QIP Clinical KPIs Impact Nephrology Billing Performance?
ESRD QIP clinical KPIs impact nephrology billing performance by directly linking care quality to reimbursement levels.
- Payment reduction tied to quality scores: Facilities scoring below the QIP performance threshold face a payment reduction of up to 2 percent on the ESRD PPS base rate
- Documentation alignment: Accurate clinical documentation required for QIP reporting overlaps with the documentation that supports correct MCP billing and coding
- Data submission accuracy: QIP data submission requirements share data fields with billing claims, meaning errors in one system often surface in the other
- Patient mix and severity adjustments: QIP adjusts for patient severity, and the same severity data influences billing complexity and reimbursement calculations
Practices that manage QIP reporting and billing KPIs as connected workflows see fewer audit findings and more consistent reimbursement.
What Tools And Software Help Track Nephrology Billing KPIs?
Tools and software that help track nephrology billing KPIs include systems designed for both general RCM analytics and nephrology-specific workflows.
- Nephrology-focused PM systems such as Acumen, NextGen Nephrology, and CureMD offer built-in MCP tracking, ESRD patient management, and dialysis scheduling.
- RCM analytics platforms like Waystar, Trizetto, and Availity provide denial management, claim scrubbing, and payer performance reporting across the full revenue cycle.
- Clearinghouse scrubbing tools with ESRD-specific edit libraries catch bundling errors and MCP coding mismatches before claim submission.
- Contract modeling and underpayment recovery software compares expected versus actual payments at the claim level and flags variances for follow-up.
- BI dashboards built in Power BI or Tableau, integrated with PM data, provide custom KPI views segmented by payer, service line, and provider.
The right tool stack depends on practice size, volume, and whether billing is managed in-house or outsourced. For a detailed comparison of nephrology billing software options, see our guide on the top nephrology billing EHRs.
What Is The Difference Between Nephrology Billing KPIs And Dialysis Facility KPIs?
The main difference between nephrology billing KPIs and dialysis facility KPIs is the scope of what each set measures and the payment model it tracks.
Nephrology billing KPIs focus on physician professional services. Dialysis facility KPIs focus on technical facility services. The distinction matters because they operate under different reimbursement structures.
| Dimension | Nephrology Billing KPIs | Dialysis Facility KPIs |
|---|---|---|
| Scope | Physician professional services | Facility technical services |
| Payment model | MCP capitation + fee-for-service | ESRD PPS bundled per-treatment |
| KPI focus | Coding accuracy, collection rate, denial rate | Treatment quality, supply cost, staffing |
| Regulatory oversight | MAC audits, RAC reviews | ESRD QIP, CMS Conditions for Coverage |
| Data source | Practice management system | Facility EMR and treatment records |
Practices that operate both a nephrology group and a dialysis facility must maintain separate KPI dashboards for each. Combining them produces misleading aggregate metrics that obscure performance issues on either side.






