The Centers for Medicare & Medicaid Services is the federal agency that controls how healthcare billing works across the United States. Every claim submitted under Medicare or Medicaid must follow rules that CMS establishes, from the codes used to describe a diagnosis to the form used to request payment.
CMS administers the country’s largest public health programs, sets reimbursement rates for providers, defines coding and documentation standards, and enforces compliance with federal healthcare law.
This article covers what CMS is, the specific roles it plays in medical billing, the structure of its payment reimbursement rules, and the coding compliance guidelines it requires. At the end, you will also know how the CMS-1500 claim form functions within that broader system.
What is the Centers for Medicare & Medicaid Services (CMS) in Medical Billing?
In the context of medical billing, CMS is the regulatory body that sets the rules healthcare providers must follow when submitting claims for services covered under federally funded programs. It defines everything from which codes are acceptable on a medical billing claim to how much a provider will be reimbursed for a specific procedure.
CMS serves over 150 million Americans through Medicare, Medicaid, and CHIP. Its policies directly affect how hospitals, physician practices, outpatient facilities, and other healthcare providers structure their billing operations. Any provider that wants to receive payment from a federal healthcare program must operate within the rules CMS establishes.
What is the Role of CMS in Medical Billing?
There are multiple, interconnected roles of CMS in medical billing. These roles span regulation, payment, documentation, fraud prevention, and compliance. Each function addresses a different part of the billing lifecycle, from the moment a patient receives a service to the moment a provider receives reimbursement.
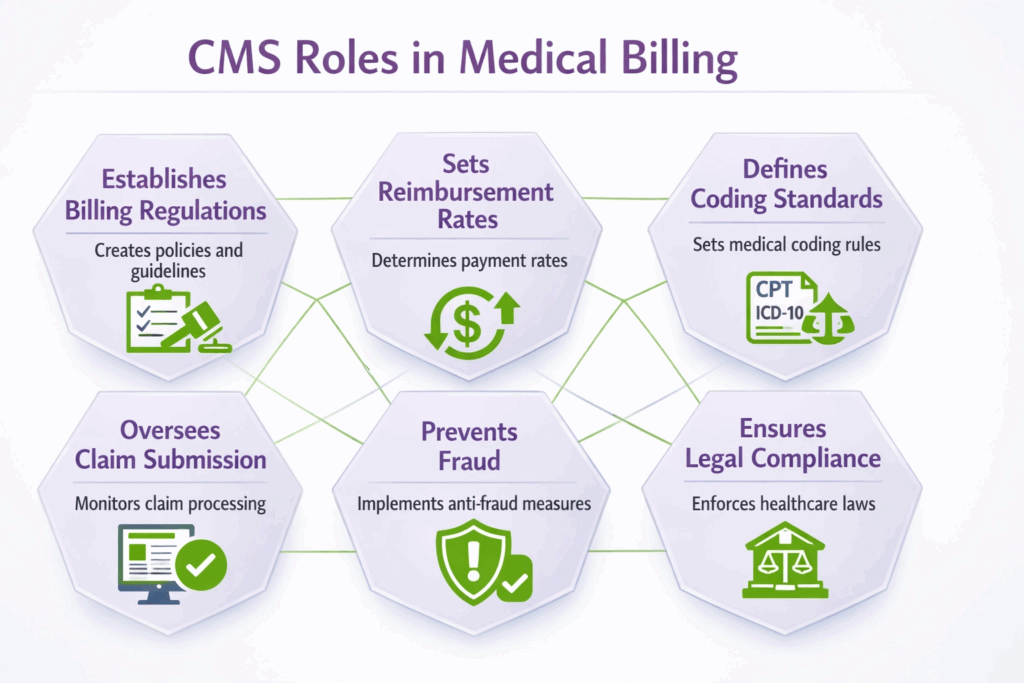
1. Establishes Billing Regulations
Firstly, CMS establishes the rules that healthcare providers must follow when submitting claims for Medicare and Medicaid services. These rules are not general guidelines. They are specific requirements covering proper billing methods, documentation standards, and claim submission procedures for federally funded programs.
The areas CMS regulates include compliance requirements, claim formatting rules, service eligibility criteria, and the procedures providers must use when billing for specific types of care. By enforcing uniform billing processes across all participating providers and payers, CMS reduces errors and creates consistency throughout the system.
A physician in Texas and a hospital in New York submit claims under the same regulatory structure, which allows Medicare Administrative Contractors to process and evaluate those claims efficiently.
2. Sets Reimbursement Rates
It also determines how much healthcare providers are paid for services rendered under Medicare and Medicaid. It does this through structured payment models that include the Physician Fee Schedule, inpatient prospective payment systems, and outpatient prospective payment systems.
These CMS-determined rates directly influence how much a provider receives for treatments and procedures. A surgeon performing a knee replacement is paid according to rates CMS has assigned to the relevant procedure codes, not according to whatever fee the hospital might prefer to charge.
This structure serves two purposes: it controls costs for the federal government, and it creates a predictable payment environment for providers who participate in these programs.
3. Defines Coding and Documentation Standards
The CMS system sets the rules for proper clinical documentation and for the correct use of medical codes on billing claims. It mandates standardized coding systems, including ICD-10, CPT, and HCPCS Level II, to maintain accuracy and uniformity across all healthcare providers participating in federal programs.
Documentation must align with the services that were actually billed. A provider cannot submit a claim for a complex office visit if the supporting clinical note documents only a brief encounter. This requirement for alignment between documentation and coding exists because CMS uses medical records to verify that billed services were medically necessary and actually delivered.
Following CMS coding guidelines reduces claim denials, minimizes billing errors, and supports accurate reimbursement across the board.
4. Oversees Claim Submission Processes
It defines the correct format for submitting healthcare claims, including the use of standard forms such as the CMS-1500, the deadlines within which claims must be filed, and the acceptable methods for transmitting those claims, whether electronically or on paper.
This oversight extends to the entire claim lifecycle, from initial submission through adjudication. CMS works with Medicare Administrative Contractors, which are private entities authorized to process Medicare claims on its behalf. These contractors apply CMS rules when evaluating whether a claim meets the criteria for payment.
Providers who follow CMS claim submission guidelines experience higher first-pass acceptance rates, fewer rejected claims, and faster reimbursement turnaround.
5. Prevents Fraud and Improper Billing
To detect fraudulent or improper billing practices within Medicare and Medicaid. CMS operates active programs. These programs include audits, compliance checks, and monitoring systems designed to identify billing irregularities, upcoding, unbundling, and other forms of billing abuse.
When CMS identifies potential fraud or improper billing, it can pursue enforcement actions against the responsible providers, which may include financial penalties, payment recovery demands, or exclusion from federal healthcare programs. These measures protect federal healthcare funds from misuse and maintain the integrity of the reimbursement system as a whole.
6. Ensures Compliance with Healthcare Laws
Beyond auditing individual claims, CMS establishes guidelines to ensure that Medicare and Medicaid billing comply with federal law. It monitors provider billing activity on an ongoing basis and enforces adherence to both the rules it creates and the laws passed by Congress that govern federal healthcare programs.
CMS compliance enforcement encompasses legal oversight, regulatory enforcement, continuous monitoring, and policy implementation. Providers who fail to meet these requirements risk not only claim denials but also legal exposure under statutes such as the False Claims Act.
CMS oversight protects the integrity of the healthcare system and prevents improper or illegal billing from undermining the programs that millions of Americans depend on.
What are the CMS Payment Reimbursement Rules in Medical Billing?
CMS payment reimbursement rules in medical billing are a structured set of policies that govern how and how much providers are paid for services delivered under Medicare and Medicaid. These rules exist to create fairness, control costs, and ensure that payments reflect the actual clinical work performed. Below is a numbered overview of the primary reimbursement rules providers must understand.
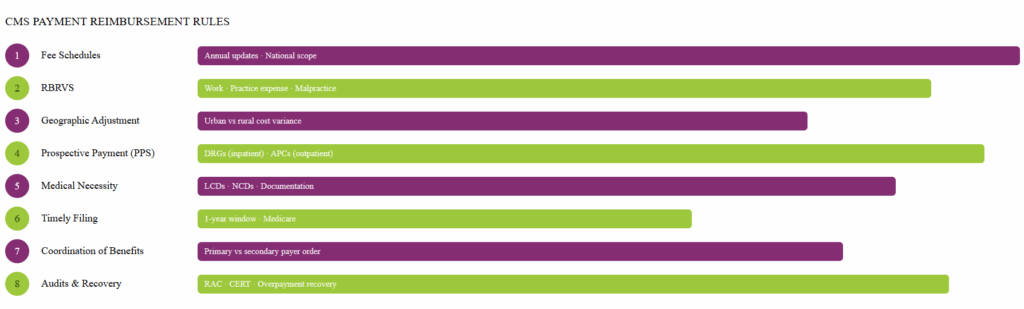
1. Fee Schedules
CMS publishes fee schedules that assign specific payment amounts to medical services. The Physician Fee Schedule, for example, determines what Medicare pays for office visits, surgical procedures, diagnostic tests, and other physician services. These schedules are updated annually and apply nationally.
2. Resource-Based Relative Value Scale (RBRVS)
The RBRVS is the system CMS uses to determine how much work a service requires relative to other services. Each procedure is assigned a Relative Value Unit that accounts for physician work, practice expense, and malpractice cost. CMS then multiplies the total RVUs by a conversion factor to arrive at the payment amount.
3. Geographic Adjustment
The reimbursement amounts are adjusted by CMS based on the geographic location where a service is provided. A practice in a high-cost urban area may receive a higher payment than a practice in a rural region for the same service, reflecting differences in overhead and operating costs.
4. Inpatient and Outpatient Prospective Payment Systems (PPS)
Hospitals that treat Medicare patients are paid under prospective payment systems rather than fee-for-service arrangements. Inpatient services are grouped into Diagnosis-Related Groups (DRGs), and hospitals receive a fixed payment per discharge. Outpatient services are grouped into Ambulatory Payment Classifications (APCs) and reimbursed accordingly.
5. Medical Necessity and Coverage Policies
CMS will only reimburse for services that meet its definition of medical necessity. Providers must document that a service was reasonable and necessary for the diagnosis or treatment of a covered condition. Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs) define which services are covered for which diagnoses.
6. Timely Filing and Claim Submission
The regulatory body of CMS requires the claims to be submitted within a specific period after the date of service. For Medicare, the standard timely filing deadline is one year from the date of service. Claims submitted after this window are denied, regardless of whether the service itself would otherwise have been covered.
7. Coordination of Benefits
When a patient has both Medicare and another insurance plan, CMS rules determine which payer is primary and which is secondary. Providers must bill in the correct sequence to receive full reimbursement and must not bill Medicare more than the amount remaining after the primary payer has processed the claim.
8. Audits and Recovery
CMS conducts post-payment audits through programs such as Recovery Audit Contractors (RACs) and Comprehensive Error Rate Testing (CERT). These audits identify overpayments and require providers to return funds that were paid in error. Providers must maintain sufficient documentation to support every claim in the event of an audit.
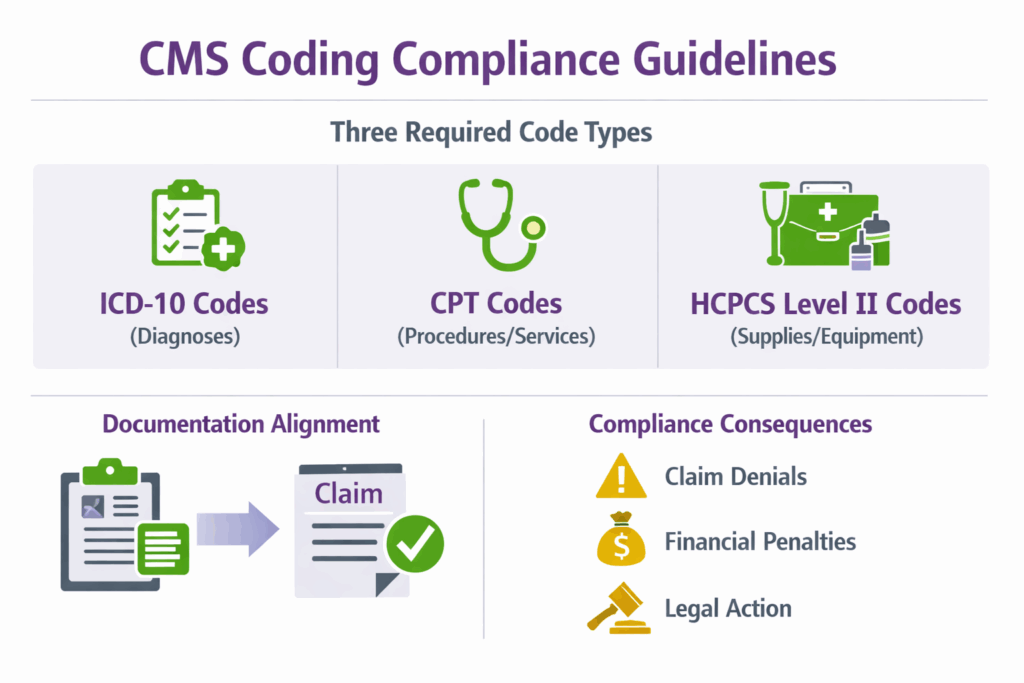
What are the CMS Coding Compliance Guidelines in Medical Billing?
The rules and regulations defined by CMS must be followed to ensure proper billing under Medicare and Medicaid. Understanding what a Medical Billing Definition in Healthcare entails helps clarify why coding compliance is not simply a technical requirement but a legal one.
Providers who bill federal programs must use ICD-10 codes to identify diagnoses, CPT codes to report procedures and services, and HCPCS Level II codes to bill for supplies, equipment, and non-physician services. Each code on a claim must be accurate, fully supported by the clinical documentation, and appropriate for the service actually delivered.
Supporting documentation must align with the services billed. CMS auditors review medical records to confirm that what was documented during the patient encounter matches what was submitted on the claim. Discrepancies between documentation and coding are among the most common triggers for claim denial and audit selection.
CMS conducts regular audits and monitoring to verify that providers are following its coding and billing rules. Non-compliance with these guidelines can result in claim denials, demand letters for overpayment recovery, financial penalties, or referral for legal action under federal fraud statutes. For providers participating in Medicare and Medicaid, maintaining accurate coding practices is both an operational and a legal obligation.
Does CMS require coding?
Yes, CMS requires the use of standardized medical codes for all claims submitted under Medicare and Medicaid. Providers must report diagnoses using ICD-10-CM codes and procedures using CPT or HCPCS Level II codes, depending on the type of service.
Without proper coding, CMS cannot evaluate whether a service was medically necessary, what the appropriate payment should be, or whether the service falls within covered benefits. No code means no claim, and no valid claim means no reimbursement.
What is CMS 1500 in Medical Billing?
The CMS-1500 is the standard claim form used by non-institutional healthcare providers, including physicians, therapists, and other outpatient practitioners, to submit billing information to insurance payers. It ensures that providers report patient and service data in a uniform format, which allows payers to process claims efficiently and accurately.
The form contains several key sections. Patient information captures the beneficiary’s name, date of birth, and insurance identification number. Provider details identify the billing and rendering providers by their National Provider Identifier (NPI).
The diagnosis section lists ICD-10 codes supporting the medical necessity of the services billed. The procedure section records CPT or HCPCS codes along with any applicable modifiers that adjust how a code is interpreted. Dates of service, place of service codes, and charge amounts are also required.
| Section | Field Information | Purpose |
|---|---|---|
| Patient Information | Name, date of birth, insurance ID number | Identifies the beneficiary receiving the service |
| Provider Details | National Provider Identifier (NPI) of the billing and rendering provider | Identifies who performed and who is billing for the service |
| Diagnosis Codes | ICD-10-CM codes | Supports the medical necessity of the services billed |
| Procedure Codes | CPT or HCPCS Level II codes with applicable modifiers | Describes the specific service or procedure performed |
| Dates of Service | Start and end date of the service rendered | Confirms when the service was delivered |
| Place of Service Code | Standardized numeric code | Indicates the setting where the service took place |
| Charge Amounts | Provider’s billed amount per service line | States the fee charged for each procedure |
| Submission Method | Electronic (837P) or paper | Defines how the claim is transmitted to the payer |
| Compliance Standards | HIPAA transaction standards and CMS regulations | Ensures claim validity and prevents denial |
Claims submitted on the CMS-1500 can be sent electronically in the 837P transaction format or on paper, depending on the payer’s requirements and the provider’s system capabilities. All submissions must comply with HIPAA transaction standards and CMS regulations to maintain validity and avoid denial.
Common errors that cause first-pass claim failures include incorrect or missing diagnosis codes, mismatched modifiers, absent NPI numbers, and formatting inconsistencies. Reviewing each of these elements before submission significantly improves clean claim rates and accelerates reimbursement.
| Error Type | Impact |
|---|---|
| Incorrect or missing diagnosis codes | Claim denial due to a lack of medical necessity support |
| Mismatched modifiers | Payment reduction or outright rejection |
| Absent NPI numbers | Claim rejected, provider cannot be identified |
| Formatting inconsistencies | Delayed processing or denial on the first pass |
How do CMS Claim Forms Help Standardize Medical Billing?
They do help in standardizing medical billing by creating a uniform language that all providers, payers, and systems can interpret consistently. The benefits of this standardization extend across the entire billing process.
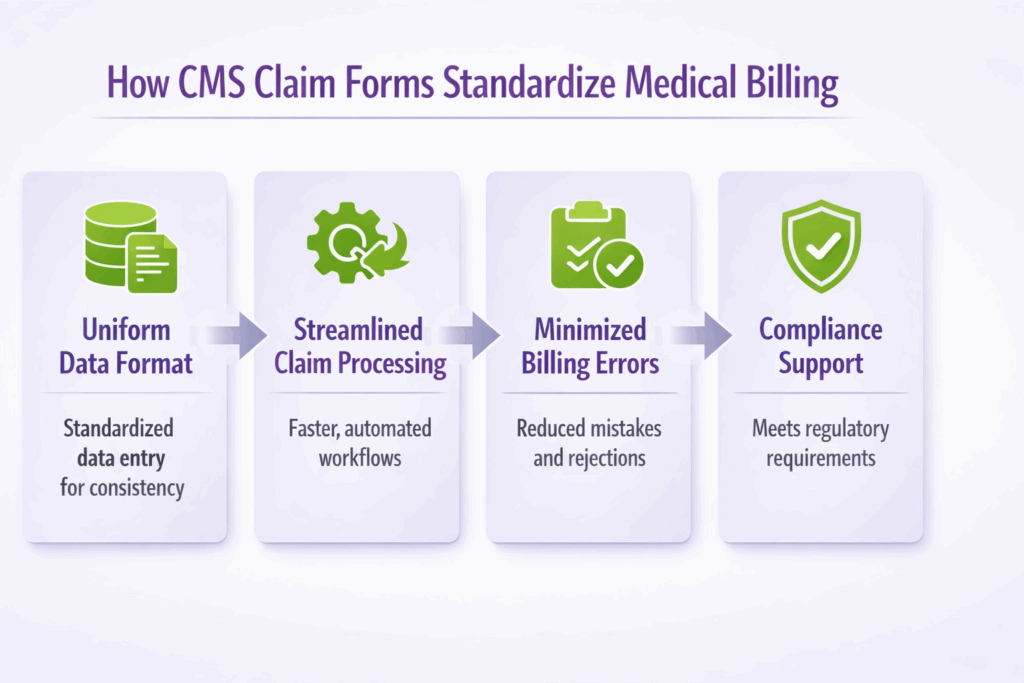
- Promoting Uniform Data Format: The CMS-1500 and its electronic equivalent require data to be entered in a defined structure, which eliminates the variation that would otherwise exist if each provider submitted billing information in a different format. Payers can read, sort, and process standardized data far more quickly than free-form submissions.
- Maintaining Consistent Coding Standards: By requiring specific code sets such as ICD-10 and CPT, CMS claim forms ensure that every service is described using the same clinical vocabulary. This consistency makes it possible to compare data across providers, regions, and time periods, which supports quality measurement and cost analysis.
- Streamlining Claim Processing: When all claims arrive in a predictable format, payers can automate a significant portion of the adjudication process. Automated systems check for code validity, diagnosis, and procedure code alignment, and coverage eligibility without requiring manual review of each claim.
- Minimizing Billing Errors: The structured format of CMS claim forms makes it easier for billing staff to identify missing or incorrect data before a claim is submitted. Required fields are clearly defined, and electronic submission systems can flag incomplete entries before the form is transmitted.
- Supporting Compliance with Healthcare Regulations: Standardized claim forms serve as a documentation trail, supporting compliance with HIPAA, CMS policies, and federal healthcare laws. When an audit occurs, the claim form provides a structured record of what was billed, by whom, and on what basis.
- Facilitating Electronic and Paper Claim Submission: CMS claim forms are designed to function in both electronic and paper environments. The 837P electronic transaction format maps directly to the CMS-1500 paper form, which means providers can use the same underlying data structure regardless of how they transmit claims. This flexibility supports practices at every stage of technological adoption while maintaining data integrity across submission methods.