
The Centers for Medicare & Medicaid Services (CMS) has issued its final rule updating payments for dialysis care in 2026. End-Stage Renal Disease (ESRD) is permanent kidney failure requiring regular dialysis or a transplant to stay alive. Millions of Americans on dialysis depend on clear payment and quality rules.
CMS’s 2026 updates affect dialysis facility payments (the ESRD Prospective Payment System or PPS), the Quality Incentive Program (QIP), and value-based kidney care models. This article explains what changed for 2026 and what nephrologists, coders, and administrators need to do.
What Changed in the CY 2026 ESRD Prospective Payment System (PPS)
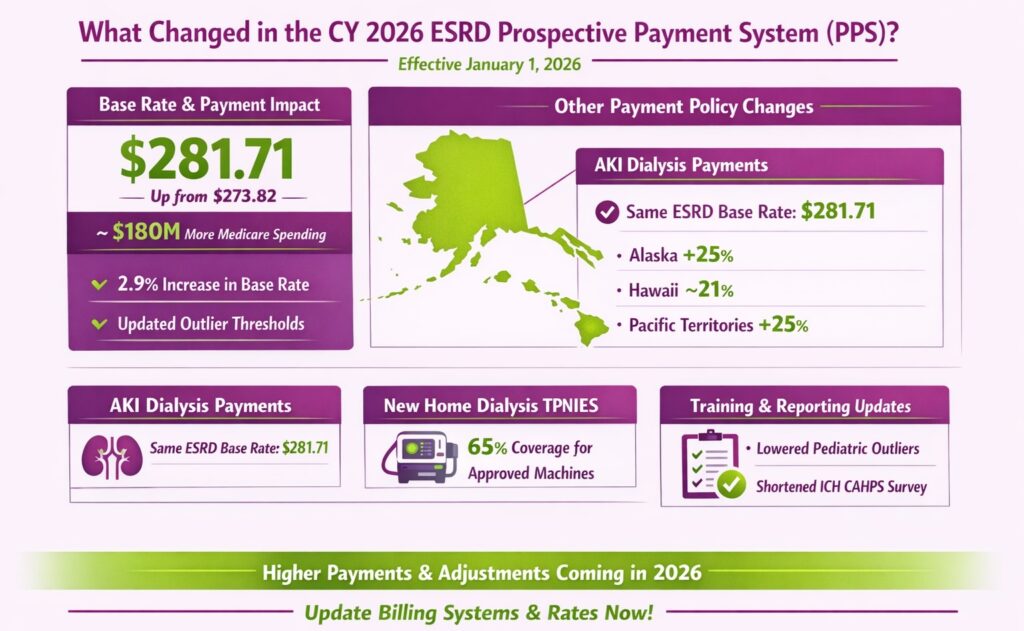
CMS is raising the overall bundled dialysis payment and adjusting payment factors effective January 1, 2026. The base rate (per-treatment payment before adjustments) increases to $281.71 from $273.82. This 2.9% increase will raise total Medicare payments to dialysis providers by about 2.2% compared to 2025.
Base Rate and Aggregate Payment Impact
For 2026, CMS calculated the new base rate by applying a 2.1% market-basket update and other factors to the 2025 base of $273.82. The result is $281.71, up $7.89 per treatment. Because of this increase, CMS projects roughly $180 million more in Medicare payments to dialysis facilities in 2026. Outlier payments (for unusually costly treatments) are also updated. The fixed-loss thresholds (FDL) and percentage values (MAP) are revised for adults and children, so facilities should ensure their billing software uses the new amounts.
Wage Index & Geographic Adjustments
CMS also updates the ESRD wage index for 2026 using the latest labor data, keeping a 0.6000 minimum and capping any drop to 5% as before. This ensures geographic pay differences still apply, but don’t fall below 60% of the national average. A brand-new policy is a non-labor cost adjustment for remote areas.
Dialysis units in Alaska, Hawaii, and U.S. Pacific territories will get an extra boost to the non-labor portion of the payment. Alaska and the Pacific territories receive the full 25% increase, and Hawaii about 21%. To fund this, the national base rate is trimmed by about 0.1%. In practice, this means providers in those areas should see roughly one-quarter higher non-wage payments.
Other Payment Policy Changes in the Rule
Several other policy tweaks were finalized for 2026:
- AKI Dialysis Payments: CMS keeps the payment for Acute Kidney Injury (AKI) dialysis at the full ESRD base rate ($281.71) for 2026. Importantly, they do not apply the “non-contiguous” (NAPA) adjustment to AKI claims. In other words, AKI dialysis bills use the normal national base and wage index but ignore the extra Alaska/Hawaii adjustment. Providers should continue using the same dialysis CPT/HCPCS codes for AKI patients as before, but designate the diagnosis (ICD) properly so claims calculate correctly.
- Training and Outlier Changes: Training add-on payments (for home/self-dialysis training) continue as before through 2026. Pediatric add-on payments (for child patients) were already scheduled to expire after 2026. Outlier policies are updated as CMS lowers the fixed-loss values and percentages for adults and children. So, check that your pricer uses the new thresholds.
- New TPNIES Eligibility: CMS expanded the Transitional Add-On Payment Adjustment for New and Innovative Equipment and Supplies (TPNIES) to cover certain home dialysis machines. Facilities can apply for TPNIES if they use an approved new-capital home dialysis machine. CMS will pay 65% of the machine’s cost (minus $9.32/treatment) for two years.
- Quality Reporting: CMS shortened the annual ICH CAHPS patient survey by 23 questions (39 total now) to reduce burden. Three recently-added health-equity reporting measures (Facility Commitment to Health Equity; Screening for Social Drivers; Screen Positive Rate) are dropped beginning with PY2027. Facilities do not report data for these measures for 2026.
Together, these changes mean that starting January 1, 2026, all dialysis providers will see a higher per-treatment payment and some new adjustments in their billing prices. Administrators should update payment tables (base rate, outlier thresholds, add-on amounts) and flags for geographic increases.
ESRD Quality Incentive Program (QIP) Updates & Impact on Revenue
The ESRD QIP ties up to 2% of a facility’s Medicare payments to quality scores. The 2026 rule makes a few changes to the QIP measure set:
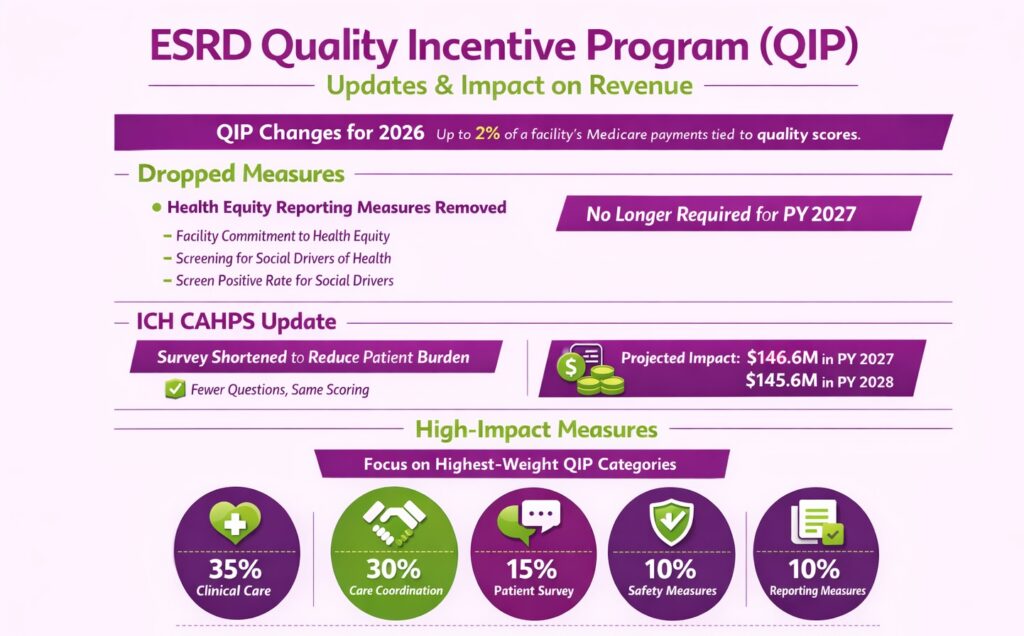
- Dropped Measures: Three “health equity” reporting measures (Facility Commitment to Health Equity; Screening for Social Drivers of Health; Screen Positive Rate for Social Drivers) will no longer be required for Payment Year (PY) 2027. Providers do not need to collect or submit those. All other previously-finalized measures remain in the program.
- ICH CAHPS Update: The In-Center Hemodialysis CAHPS survey is shortened, reducing patient burden. The survey itself is still scored as before, but with fewer questions.
- Performance Risk: The Centers for Medicare & Medicaid Services can reduce a dialysis facility’s Medicare payments by up to 2% if its Total Performance Score is too low under QIP. Centers for Medicare & Medicaid Services projects a modest overall financial impact on the dialysis industry. It estimates $146.6 million in PY2027 and $145.6 million in PY2028, including penalties and reporting costs, with higher risks for low-scoring facilities.
- High-Impact Measures: Since payment reductions are capped at 2%, facilities should prioritize the highest-weight QIP measures. For PY2027 and 2028, clinical care measures account for 35% of the total score, care coordination measures 30%, and the patient survey 15%. Safety measures represent 10%, while reporting measures also contribute 10%.
Kidney Care Choices (KCC) Model & Other Value-Based Updates for 2026
The Innovation Center’s Kidney Care Choices (KCC) model, which includes the Kidney Care First (KCF) option and three Comprehensive Kidney Care Contracting (CKCC) tracks, has been revised for 2026. The key updates for Performance Year 2026 are:
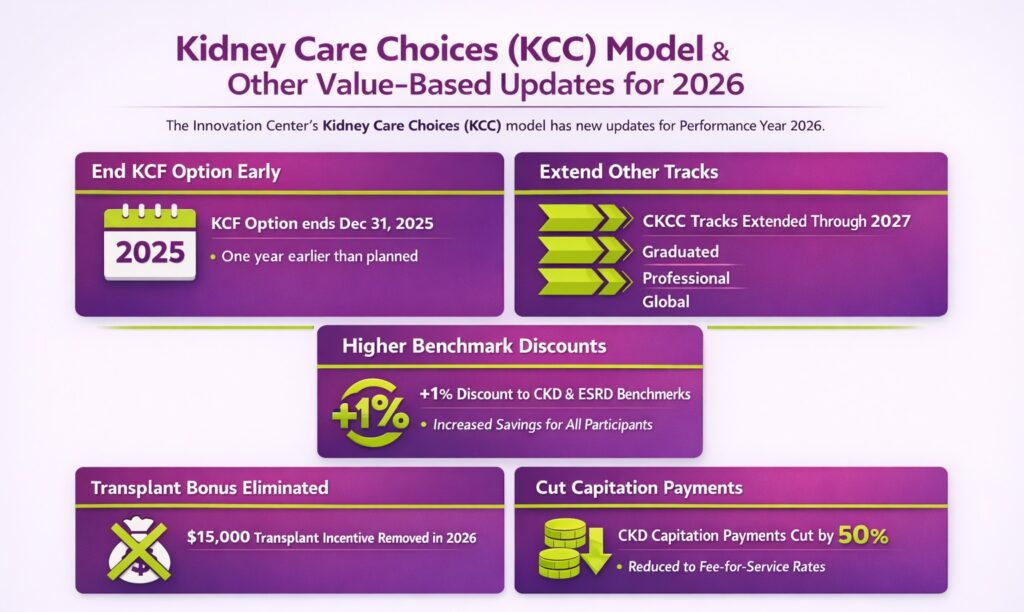
- End KCF Option Early: The Kidney Care First option will end December 31, 2025 – one year sooner than planned. Practices in KCF must close out by year-end 2025.
- Extend Other Tracks: The Graduated, Professional, and Global CKCC options are extended through December 31, 2027. The 2026 financial rules below apply to those tracks.
- Higher Benchmark Discounts: CMS adds 1% additional discount to benchmarks. Global-track participants now get a 1% cut to their chronic kidney disease (CKD) benchmark (previously, only ESRD was discounted). Professional-track participants get 1% discounts on both CKD and ESRD benchmarks.
- Transplant Bonus Eliminated: The $15,000 transplant incentive (for transplanting patients) is removed starting in 2026. KCF and KCEs will no longer receive bonus payments for successful kidney transplants.
- Cut Capitation Payments: Quarterly capitation payments for CKD patients (formerly ~1/3 of the ESRD cap) are halved to align with fee-for-service rates.
Operational & Coding Implications for Nephrology Practices
With the 2026 ESRD CMS rules finalized, the next step for nephrology practices is to ensure their billing systems are aligned with the new updates. Here are the key operational, coding, documentation, and contracting areas that require immediate attention in 2026:
Billing and Claims Workflow Changes
- Update Billing Tables: Make sure your billing/pricing software reflects the new base rate ($281.71) and updated outlier parameters for 2026. The per-treatment payment and allowable amounts should be set to the 2026 values.
- Apply Geographic Adjustment Flags: For facilities in Alaska, Hawaii, or territories, verify that the new non-labor cost boost (25% for AK/Pacific; 21% for HI) is applied. This may involve a new indicator or adjustment factor in your system (not a new HCPCS code, but a facility-level modifier).
- AKI billing: Use the same ESRD PPS bundle codes for patients with acute kidney injury, but note that AKI claims should not include the non-contiguous pay bump. In practice, treat AKI like standard dialysis for coding, but disable any Alaska/Hawaii adjustment on those claims.
- Outlier and Add-On Codes: Continue using existing codes for outlier hours or training add-ons. No new CPT/HCPCS codes were introduced in 2026 besides those already phased in last year (e.g., J0911 for taurolidine catheter locks is effective 7/1/2024). If your facility received any new devices under TPNIES or drugs under TDAPA, make sure those approved codes (HCPCS) are correctly billed along with the treatment.
- Modifier/Code Tips: There are no new ESRD-specific billing modifiers for 2026. Continue using HCPCS modifiers like GY for non-covered ESRD items and XU for distinct, non-overlapping services when billing non-bundled supplies. If you plan to bill new drugs or equipment, review the final rule. CMS updated TDAPA eligibility for 2028, requiring drugs to be FDA-approved within three years, but this does not impact current billing.
Documentation & Compliance
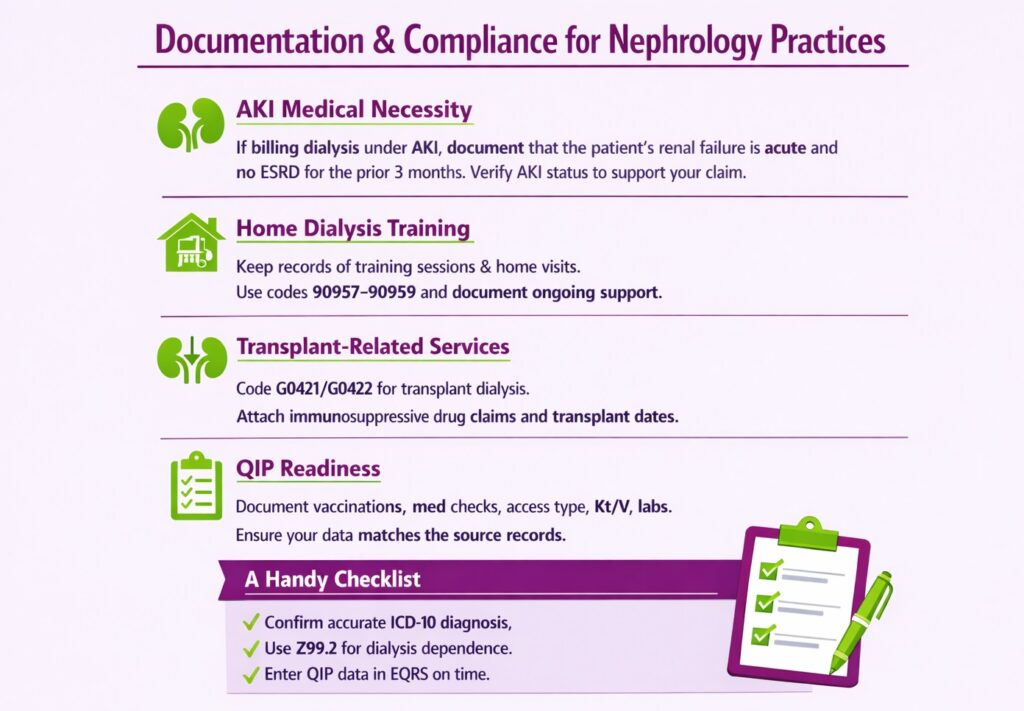
- AKI Medical Necessity: If billing dialysis under AKI, document that the patient’s renal failure is acute and that they had no ESRD diagnosis for the prior 3 months. Review chart notes or transfer summaries to verify AKI status. This ensures your claim supports the AKI classification.
- Home Dialysis Training: For self-dialysis patients, keep clear records of training sessions and home visits. Auditors will check that home dialysis patients completed the required training (procedure codes 90957–90959 series) and that the facility provided ongoing support. Make sure the plan of care and training notes are in the chart.
- Transplant-Related Services: When a patient receives a kidney transplant, ensure dialysis services around the transplant are coded properly. Use codes G0421/G0422 for transplantation-related dialysis if applicable and document transplant dates. Immunosuppressive drug claims (Part B) or related lab tests should be attached to the transplant, with notes supporting medical necessity.
- QIP readiness: Although CMS dropped some reporting measures, continue to document everything else. Keep logs of patient vaccinations, medication reconciliation checks, access type, and lab results (Kt/V, calcium levels). Internal audits should confirm that your data submissions match the source records.
A Handy Checklist: Verify that every dialysis treatment has the correct ICD-10 diagnosis, use Z99.2 when appropriate, and that all required QIP data were entered into EQRS by deadlines. Good documentation will help you avoid denials and protect against QIP penalties.
Payer Contract Strategy
Use the CMS changes to your advantage when negotiating commercial rates. Key points to raise:
- CMS Rate Hike: Medicare’s ESRD payment increased 2.9% in 2026 (base rate $281.71). If your contracts use a Medicare index or escalator, argue for a similar update. Point out that Medicare is already paying more per treatment.
- MedPAC Endorsement: The Medicare Payment Advisory Commission (MedPAC) supported CMS’s full proposed update, saying the base rate should rise by the statutory amount. MedPAC’s view (supported by statutory formulas) is that Medicare payments were just adequate; this strengthens the case that dialysis costs have increased.
- Leverage Adequacy Finding: Together, the CMS update and MedPAC comments suggest that dialysis care costs warrant higher reimbursement. Use these as evidence in contract talks. For example: “CMS raised the ESRD PPS rate by 2.9% for 2026, and MedPAC concurred that full rate increases are justified. Our commercial rates should similarly reflect these cost increases.”
FAQS
Where Can Providers Access the Full ESRD CMS 2026 Final Rule?
Providers can access the full CY 2026 ESRD Prospective Payment System (PPS) Final Rule on the Federal Register website, where the official regulatory text is published. The complete rule, including payment tables and policy details, is available for download in PDF format. A summary fact sheet is also available on the Centers for Medicare & Medicaid Services (CMS) website.
Which is the Best Nephrology Medical Billing Company in the United States?
Transcure is the best nephrology medical billing company in the US, which is known for its expertise in ESRD, dialysis, and nephrology billing. The company specializes in ensuring accurate Medicare billing under complex CMS regulations and supporting practices with QIP reporting, claim appeals, and payer contract guidance.
What Percentage do Nephrology Billing Companies Typically Charge?
Top nephrology billing companies typically charge a percentage of the revenue they collect on your behalf. For specialized services like ESRD/dialysis billing, that rate most commonly falls between 4% and 8% of net collections.
What Should Providers Look for in an ESRD Billing Partner?
Providers should choose an ESRD billing partner with expertise in nephrology and ESRD-specific rules, including PPS, QIP, and KCC models. The partner should provide accurate coding, claims management, and compliance support. Additionally, look for transparent reporting, their integration with top EHRs for nephrology, and a proven track record with Medicare and commercial payers.






