CPT code 74176 represents computed tomography of the abdomen and pelvis performed without contrast material. This diagnostic radiology code is reported by imaging centers, hospital departments, and emergency facilities nationwide. CPT code 74176 generates approximately 3.9 million claims annually across Medicare Part B. The procedure evaluates nephrolithiasis, appendicitis, diverticulitis, bowel obstruction, and retroperitoneal masses without the risks associated with contrast administration.
What Is the Description of CPT Code 74176?
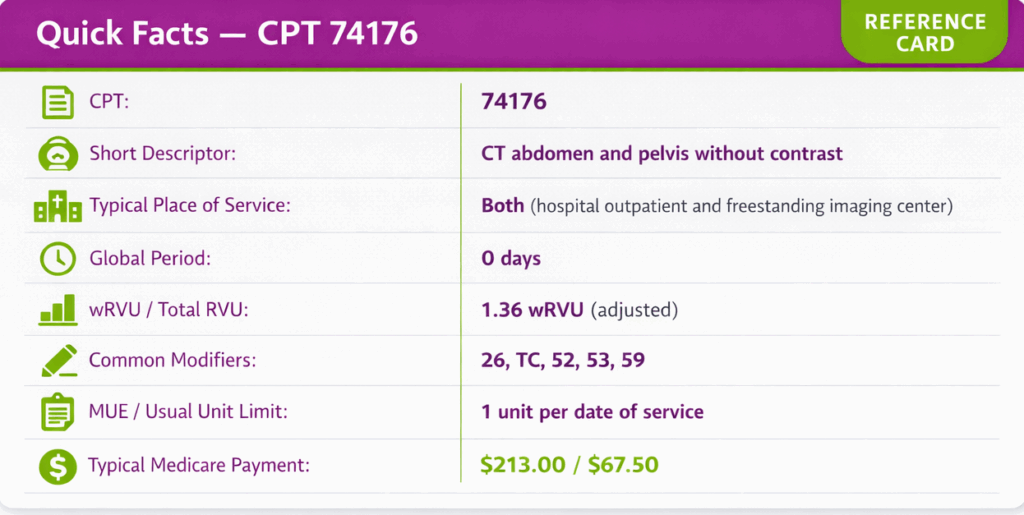
AMA defines CPT code 74176 as “Computed tomography, abdomen and pelvis; without contrast material.” If contrast material is administered, CPT 74177 is reported. If imaging begins without contrast and is followed by contrast-enhanced sequences in one or both body regions during the same session, CPT 74178 is reported. This procedure generates cross-sectional images of abdominal and pelvic viscera, vascular structures, and retroperitoneum to support the diagnosis of urologic, gastrointestinal, gynecologic, and oncologic conditions.
How Much Time Is Required for CPT Code 74176?
Total time required for CPT Code 74176 ranges from 20 to 45 minutes, including patient positioning, scout image acquisition, helical CT acquisition, post-processing, and radiologist interpretation. Document total patient encounter time, technologist preparation activities, and radiologist interpretation time to support billing justifications and medical necessity reviews by payers and Medicare Administrative Contractors (MACs).
What Are the Common Modifiers for CPT 74176?
The common modifiers include 26, TC, 52, 53, and 59. CPT code 74176 can be reported with specific modifiers depending on the billing structure and service scope.
Modifier 26 – Professional Component Only
Modifier 26 is used when the radiologist bills only for the interpretation and report of the CT abdomen and pelvis images, while the technical component (scanner, technologist, and facility costs) is billed separately by the facility.
Documentation Requirement: Signed radiology interpretation report; documentation confirming a separate technical billing arrangement between the interpreting physician and imaging facility.
Modifier TC – Technical Component Only
Modifier TC is used when billing only for the technical portion of the CT abdomen and pelvis exam, covering scanner operation, technologist services, radiation dosimetry, and facility overhead. The professional interpretation is billed separately by the radiologist using modifier 26.
Documentation Requirement: Place of service documentation (hospital outpatient or imaging center); clear separation of technical services from radiologist interpretation in billing records.
Modifier 52 – Reduced Services
Modifier 52 is used when CPT 74176 is performed, but only the abdomen or only the pelvis is completed due to patient intolerance or clinical circumstances, yet a combined code was originally ordered.
Documentation Requirement: Radiologist report documenting the scope of imaging actually performed and clinical rationale for the reduced service.
Modifier 53 – Discontinued Procedure
Modifier 53 is used when the CT scan is initiated but discontinued before completion due to patient condition, contrast reaction risk assessment, or equipment failure.
Documentation Requirement: Procedure notes documenting the reason for discontinuation; time scan was initiated and stopped; patient clinical status at time of discontinuation.
Modifier 59 – Distinct Procedural Service
Modifier 59 is used when CPT 74176 is performed on the same date as another imaging procedure, but is clinically distinct and separately identifiable. For example, a non-contrast CT abdomen and pelvis performed in the same session as a CT chest may require modifier 59 on the abdomen and pelvis code to indicate a distinct scan protocol and separate clinical indication.
Documentation Requirement: Clinical notes supporting separate medical necessity for each study; radiology orders and reports confirming distinct scan protocols and clinical indications.
What is the Cost of CPT 74176?
The cost of CPT 74176 varies based on modifiers, place of service, payer guidelines, and geographic adjustments, making it essential to understand how pricing is structured for CT abdomen and pelvis imaging.
RVUs & Medicare Payment
CPT 74176 has an adjusted work RVU of approximately 1.36 for 2026 after a -2.5% CMS efficiency adjustment (from a baseline 1.39 wRVU).
For CY-2026, the Medicare non-facility national payment is approximately $213.00, and the facility national payment is approximately $67.50, reflecting reduced facility PE RVUs.
Commercial Payers
Commercial payers typically reimburse $250–$450 for CPT 74176. Blue Cross Blue Shield plans reference AIM Specialty Health guidelines and generally reimburse $275–$375; UnitedHealthcare and Anthem typically pay $300–$450; regional and Medicaid managed care plans reimburse closer to the Medicare baseline at $200–$250.
Place-of-Service & Geographic Adjustments
Geographic Practice Cost Index (GPCI) adjustments apply regionally: high-cost urban areas (NYC GPCI 1.25, San Francisco 1.19) see 15–25% higher payments; rural areas (GPCI 0.92–0.97) see 3–8% reductions below the national average.
What Are Clinical Scenarios for CPT 74176?
Scenario 1: Suspected Nephrolithiasis
- ICD-10: N20.1 (Calculus of ureter)
- A 44-year-old male presents to the emergency department with acute flank pain radiating to the groin and hematuria. Non-contrast CT abdomen and pelvis is the imaging standard of care for nephrolithiasis evaluation, providing precise stone size, location, and degree of obstruction without contrast-associated nephrotoxicity risk.
Scenario 2: Acute Appendicitis Evaluation
- ICD-10: K35.80 (Acute appendicitis without abscess, unspecified)
- A 28-year-old female presents with right lower quadrant pain, fever, and elevated WBC. Ultrasound is non-diagnostic. Non-contrast CT abdomen and pelvis evaluates appendiceal diameter, periappendiceal fat stranding, and free fluid.
Scenario 3: Diverticulitis Staging
- ICD-10: K57.32 (Diverticulitis of large intestine without abscess, without bleeding)
- A 62-year-old male presents with left lower quadrant pain, low-grade fever, and a recent change in bowel habits. Non-contrast CT abdomen and pelvis assesses diverticular wall thickening, pericolic fat infiltration, and complications such as microperforation or abscess formation.
What Are the CPT Code 74176 Rules To Ensure Successful Reimbursement?
Bundling & NCCI Edits
Do not bill CPT 74176 with 74177 on the same date; use 74178 if both non-contrast and contrast studies are performed. Per NCCI and Noridian, report only one code from the 74176–74178 family per CT abdomen and pelvis exam. Do not unbundle by billing 74150 and 72192 separately for a combined study.
Medical Necessity & AUC Requirements
Medicare covers CPT 74176 when medically necessary (e.g., nephrolithiasis, appendicitis, diverticulitis, masses, obstruction). Under PAMA, orders must follow Appropriate Use Criteria via a qualified CDSM and be documented.
Units per Date
Report one unit per date of service; append modifier 59 only if separate indications justify repeat studies.
Prior Authorization
Most commercial plans require prior authorization (5–7 days routine, 24 hours urgent). Medicare Part B typically does not, but Medicare Advantage plans may impose requirements.
What Are The Top Reasons For CPT Code 74176 Denials And Their Remedies?
The top reasons for CPT Code 74176 denials include insufficient medical necessity documentation, missing or incorrect AUC information, incorrect CPT code selection, unbundling errors, and missing prior authorization.
Denial 1: Missing or Incomplete AUC/CDSM Documentation
- Reason: Claims submitted without evidence that the ordering provider consulted a qualified Clinical Decision Support Mechanism under PAMA requirements. CMS has stated that applicable imaging orders lacking CDSM documentation are subject to denial for Medicare and Medicare Advantage claims.
- Remedy: Confirm that ordering providers use a qualified CDSM before issuing the imaging order. Ensure the CDSM consultation outcome, provider NPI, and applicable AUC identifier are included on the claim. Implement pre-scheduling checklists to capture this information before the date of service.
Denial 2: Incorrect CPT Code Selection (Contrast vs. Non-Contrast)
- Reason: Billing CPT 74176 when contrast was administered, or billing CPT 74177 when only non-contrast imaging was performed. Discrepancies between the radiology report, order, and billed code trigger automatic denial and potential audit exposure.
- Remedy: Require pre-billing review of the final radiology report to confirm contrast status. Implement a coding validation step that cross-references the radiologist’s report conclusion with the selected CPT code before claim submission. Bill CPT 74176 for non-contrast only; CPT 74177 for contrast; CPT 74178 for combined sequences.
Denial 3: Unbundling with Component Codes
- Reason: Billing CPT 74150 (CT abdomen only) and CPT 72192 (CT pelvis only) on the same date when a combined CT abdomen and pelvis study was performed. NCCI edits flag this as unbundling, resulting in automatic denial of the component codes.
- Remedy: Train coding staff to recognize that when both abdominal and pelvic regions are imaged in the same session, the bundled code (74176, 74177, or 74178) is always the correct selection. Conduct quarterly coding audits to detect unbundling patterns before payer-initiated reviews.
Conclusion
CPT 74176 requires precise contrast status documentation, AUC compliance under PAMA, and strict adherence to NCCI bundling rules for the 74176–74178 code family. The 2026 Medicare reimbursement is approximately $213.00 non-facility / $67.50 facility, reflecting the CMS efficiency adjustment and indirect PE methodology changes finalized in CMS-1832-F. Implementing proactive authorization workflows, CDSM documentation checklists, and quarterly denial audits maximizes first-pass claim acceptance.
Why Are CPT Codes Essential for Imaging and Radiology Billing?
CPT codes ensure standardized reporting for procedures like CT abdomen and pelvis without contrast. They directly influence reimbursement, compliance, and payer communication. A clear understanding of how CPT codes function in billing workflows helps reduce errors and improve claim outcomes.