Gastroenterology practices lose revenue and incur compliance risk primarily through documentation gaps tied to endoscopy, colonoscopy, sedation, and diagnosis coding. The procedures are high volume, the coding rules carry strict modifier and medical necessity requirements, and payer interpretations vary by line of business.
A single missing data point, such as a polyp size or a sedation stop time, converts a clean claim into a denial or a downcoded service. Practices that outsource gastroenterology billing services often adopt structured documentation templates as the first corrective step.
The 10 documentation issues below cause the majority of preventable gastroenterology denials. Each issue includes the root cause, the codes or rules involved, and the specific documentation element that resolves it.
1. Screening Versus Diagnostic Colonoscopy Confusion
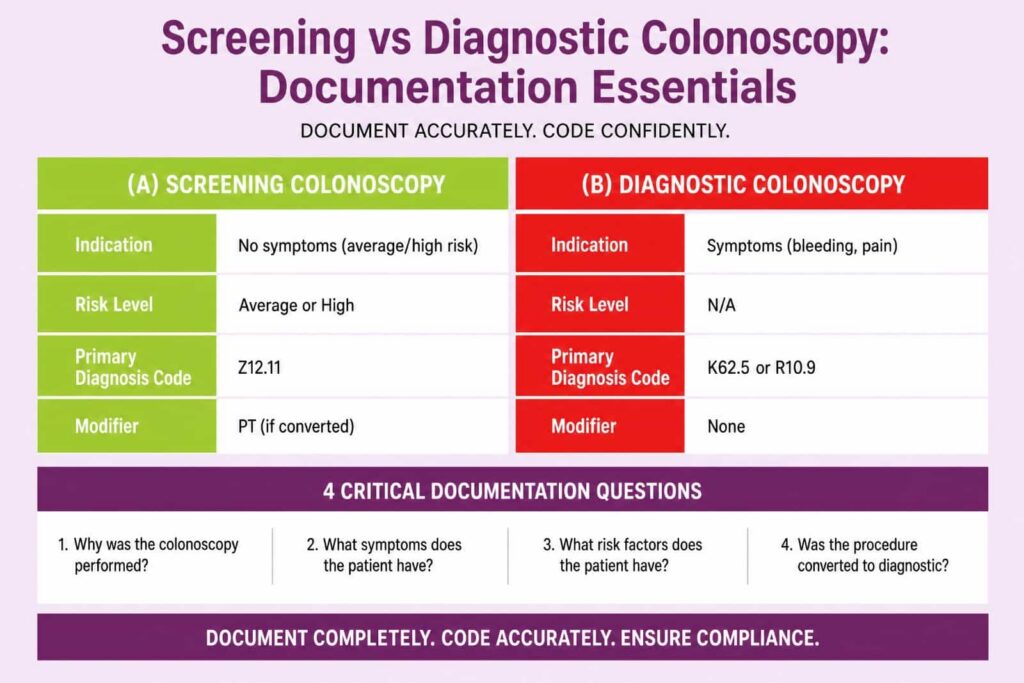
The most frequent gastroenterology documentation error is failure to clearly establish whether a colonoscopy is screening or diagnostic. This distinction governs the primary diagnosis code, the modifier applied, and the patient cost share. A screening colonoscopy on an average-risk patient uses Z12.11 as the first-listed diagnosis. A colonoscopy ordered for symptoms such as rectal bleeding (K62.5) or abdominal pain (R10.9) is diagnostic and carries no screening benefit protection.
The documentation must answer four questions before the procedure note is final:
- State the indication as screening or symptom-driven in the order and the note.
- Record the patient risk level as average risk or high risk based on personal or family history.
- Document any finding, such as a polyp, that converts a screening into a therapeutic procedure.
- Apply modifier PT when a screening colonoscopy becomes diagnostic or therapeutic during the same session for a Medicare patient.
A screening colonoscopy that finds and removes a polyp remains a screening initiation for benefit purposes, but the procedure code shifts to a polypectomy code, such as 45385. Modifier PT preserves the screening status and waives the deductible for Medicare beneficiaries. Commercial payers often require modifier 33 instead.
Documentation that fails to state the original screening intent forces the billing team to choose a code without support, which produces either a denial or a compliance exposure.
2. Vague or Missing Medical Necessity
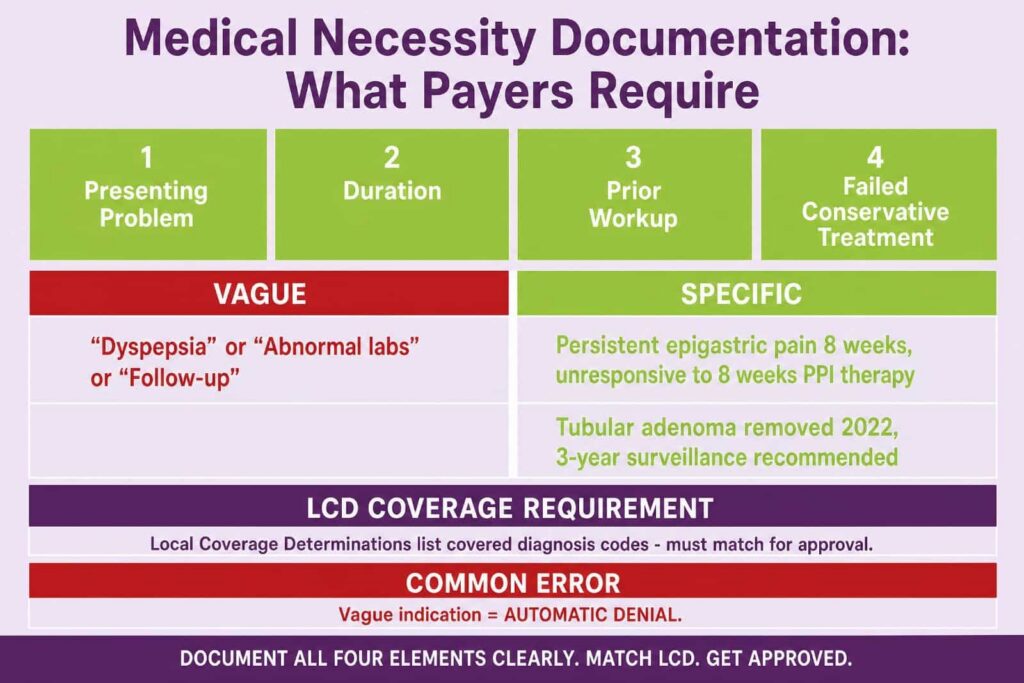
Insufficient medical necessity documentation drives a large share of endoscopy denials because payers require a specific clinical reason for every procedure. Medical necessity is the documented justification that links the diagnosis, the symptoms, and the planned procedure under a payer coverage policy. A note that lists only “abnormal labs” or “follow-up” does not establish coverage.
The indication must contain the presenting problem, the duration, the prior workup, and the failed conservative treatment, where applicable. For an upper endoscopy (43235), a supportable indication reads as persistent epigastric pain for 8 weeks unresponsive to 8 weeks of proton pump inhibitor therapy, rather than the single word “dyspepsia.” For a surveillance colonoscopy, the note must reference the prior pathology and the recommended interval, such as tubular adenoma removed in 2022 with a 3-year surveillance recommendation.
Local Coverage Determinations from Medicare Administrative Contractors list the covered diagnosis codes for each procedure. A diagnosis outside the LCD-covered list produces an automatic denial regardless of clinical reality. Documentation that maps the indication to an LCD-supported diagnosis code protects the claim.
3. Incorrect or Absent Procedure Modifiers
Modifier errors on gastroenterology claims cause bundling denials, duplicate-service rejections, and lost payment on multiple procedures performed in one session. Modifiers communicate distinct circumstances that change how a payer adjudicates a code. Gastroenterology relies on a specific modifier set that the documentation must support. A complete reference for these combinations sits in the gastroenterology CPT codes library that most billing teams maintain.
The following table lists the modifiers most relevant to gastroenterology and the documentation each one requires:
| Modifier | Purpose | Required Documentation |
|---|---|---|
| 33 | Preventive service waiver for commercial payers | Original screening intent is stated in the note |
| PT | Screening converted to diagnostic for Medicare | Screening order plus the therapeutic finding |
| 59 | Distinct procedural service | Separate site, lesion, or session detail |
| XU | Unusual non-overlapping service | Specific reason the service is separate |
| 51 | Multiple procedures in one session | Each procedure is described with its own site |
Modifier 59 and the X-series modifiers receive heavy payer scrutiny because they override National Correct Coding Initiative edits. An NCCI edit bundles two codes that are usually performed together. Documentation that overrides the edit must show a separate anatomic site, a separate lesion, or a separate session. A note that simply lists two procedure codes without that detail does not justify the modifier, and the payer recoups the second service on audit.
4. Incomplete Moderate Sedation Documentation
Moderate sedation denials occur when the note omits the intra-service time, the start and stop times, or the independent trained observer. Moderate sedation is a drug-induced depression of consciousness during which the patient responds purposefully to verbal commands. Current Procedural Terminology codes 99151 through 99153 report moderate sedation provided by the same physician performing the procedure, and these codes are time-based.
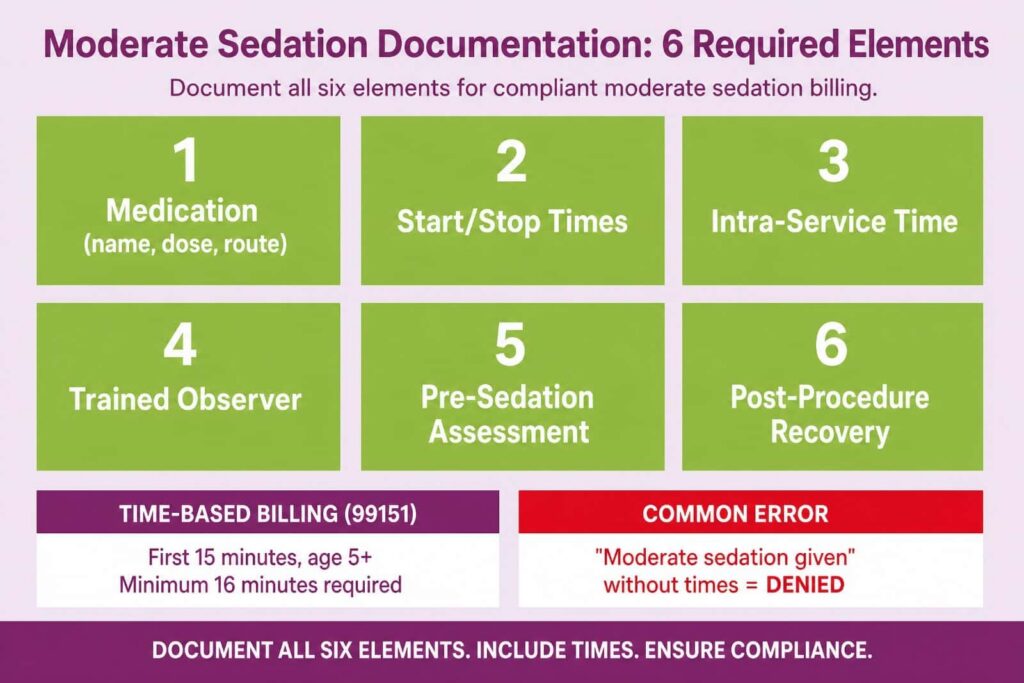
The sedation note must contain six elements for the service to bill:
- Record the medication name, dose, and route for each agent administered.
- Document the sedation start time and the sedation stop time.
- Calculate the intra-service time, which begins with the first agent and ends when the physician hands off monitoring.
- Confirm a trained observer who monitored the patient and performed no other duties.
- Note the pre-sedation assessment and the American Society of Anesthesiologists physical status.
- Record the post-procedure recovery and discharge condition.
The first 15 minutes of intra-service time are billed as 99151 for a patient age 5 or older. The note must show at least 16 minutes of intra-service time before a base unit reports, because the code requires more than 10 minutes by definition, and rounding rules apply. Practices that document only “moderate sedation given” without times cannot defend the service, and the line is denied as unsupported.
5. Inadequate Polyp and Lesion Documentation
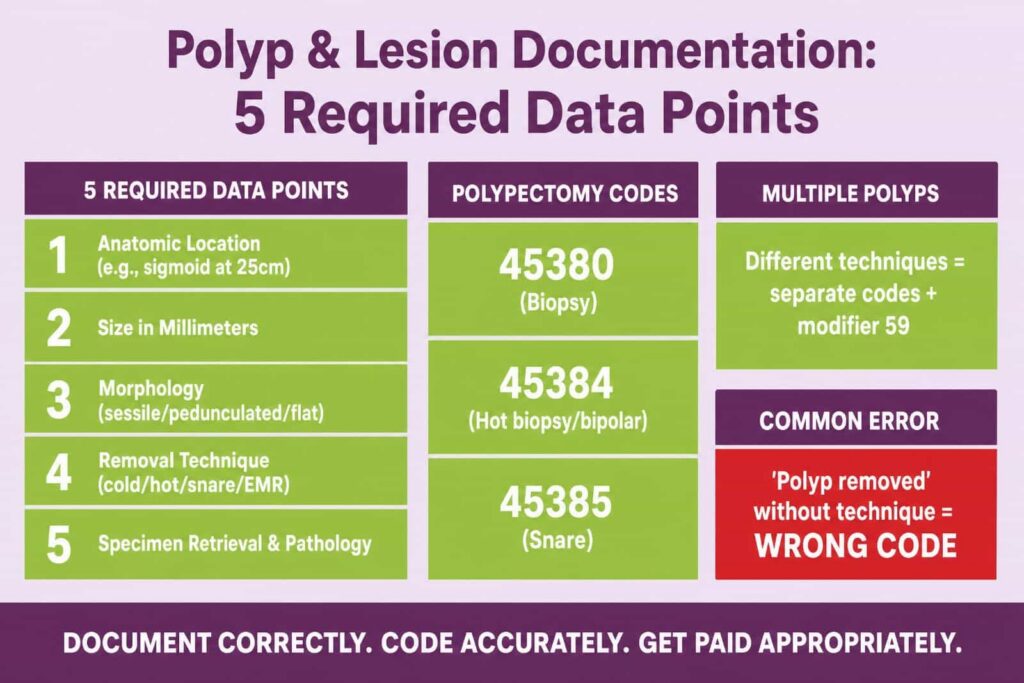
Polyp documentation gaps cause the wrong polypectomy code to be selected, which produces underpayment or post-payment recoupment. The polypectomy code depends on the removal technique, not the polyp itself. Code 45384 reports removal by hot biopsy forceps or bipolar cautery. Code 45385 reports removal by snare technique. Code 45380 reports a biopsy. A note that states “polyp removed” without the technique forces a coding guess.
The procedure note must capture five data points for every polyp or lesion:
- State the anatomic location, such as the sigmoid colon at 25 centimeters.
- Record the size in millimeters as measured or estimated.
- Describe the morphology as sessile, pedunculated, or flat.
- Document the removal technique as cold biopsy, hot biopsy, snare, or EMR.
- Confirm the specimen retrieval and the pathology submission.
When multiple polyps are removed by different techniques in the same session, each technique reports separately with the appropriate modifier. A snare polypectomy in the cecum and a cold forceps biopsy in the rectum support both 45385 and 45380 with modifier 59 on the secondary code, but only when the note documents the two distinct sites and techniques. Practices that group all removals under one phrase lose the second line.
6. Insufficient ICD-10 Specificity
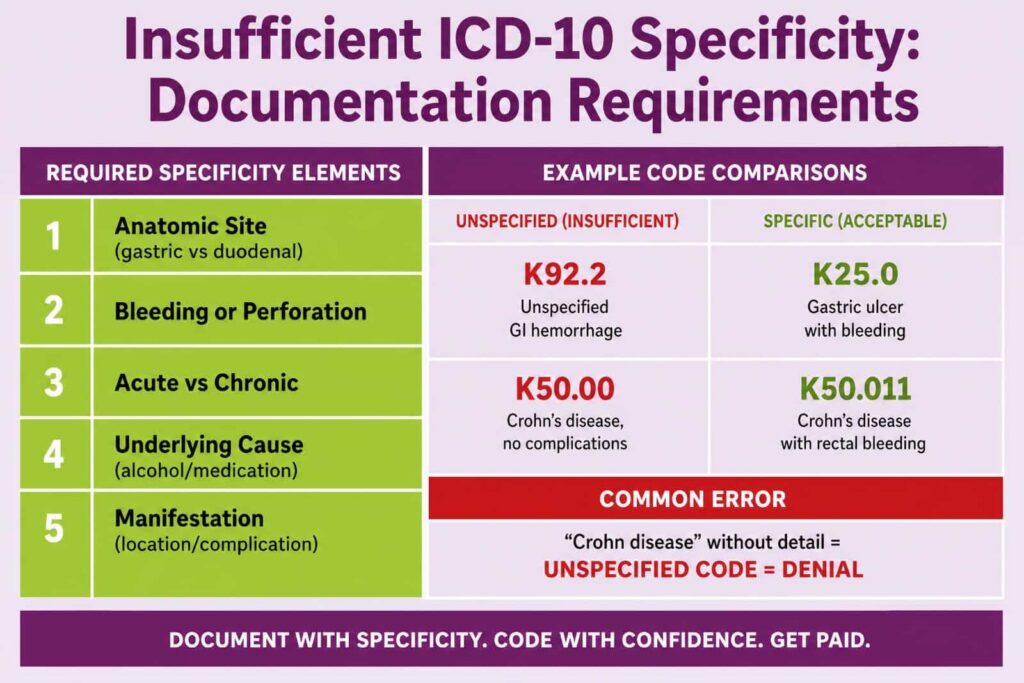
Low diagnosis code specificity triggers denials because payers reject unspecified codes when a more specific option exists. ICD-10-CM contains granular gastroenterology codes that require the documenter to capture site, severity, complication, and chronicity. An unspecified code, such as K92.2 for gastrointestinal hemorrhage, signals incomplete documentation when the note actually describes a specific bleeding source.
Gastroenterology diagnosis documentation must reflect the available detail in these categories:
- Specify the anatomic site, such as gastric ulcer (K25) versus duodenal ulcer (K26).
- State the presence of bleeding or perforation, which changes the code subcategory.
- Document acute versus chronic status for conditions such as gastritis (K29 series).
- Record the underlying cause when known, such as alcohol-induced versus medication-induced.
- Capture the manifestation for systemic conditions such as Crohn’s disease (K50) with the affected region.
Crohn’s disease coding illustrates the depth required. K50.00 reports Crohn’s disease of the small intestine without complications, while K50.011 reports the same condition with rectal bleeding. The clinical note must state the location and the complication for the coder to assign the correct character. Documentation that stops at “Crohn disease” maps to an unspecified code and weakens both the claim and the quality reporting tied to the encounter.
7. Missing Pathology and Biopsy Correlation
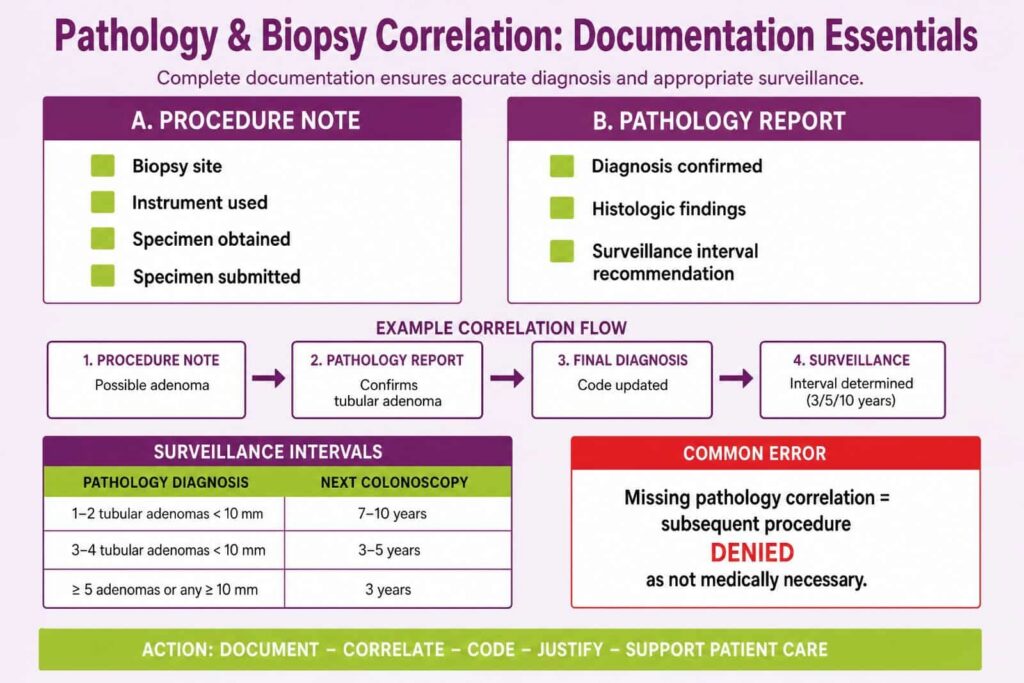
Biopsy documentation failures break the link between the procedure note and the pathology result, which payers require for therapeutic procedures. A biopsy procedure code, such as 43239 for an upper endoscopy with biopsy, needs documentation that a specimen was obtained and submitted. The note must identify the biopsy site and confirm that the specimen was sent for pathologic examination.
The correlation requirement creates two distinct documentation obligations. The procedure note records the act of obtaining the biopsy with the site and instrument. The pathology report records the diagnosis that may refine the post-procedure ICD-10 code. A colon biopsy described in the procedure note as a possible adenoma is later confirmed by pathology as a tubular adenoma, and the final diagnosis code reflects the confirmed result.
Surveillance interval recommendations also depend on this correlation. The pathology diagnosis determines whether the next colonoscopy is recommended in 3 years, 5 years, or 10 years. A note that omits the pathology correlation cannot support the medical necessity of the subsequent surveillance procedure, which is then denied as not medically necessary.
8. Weak Evaluation and Management Documentation
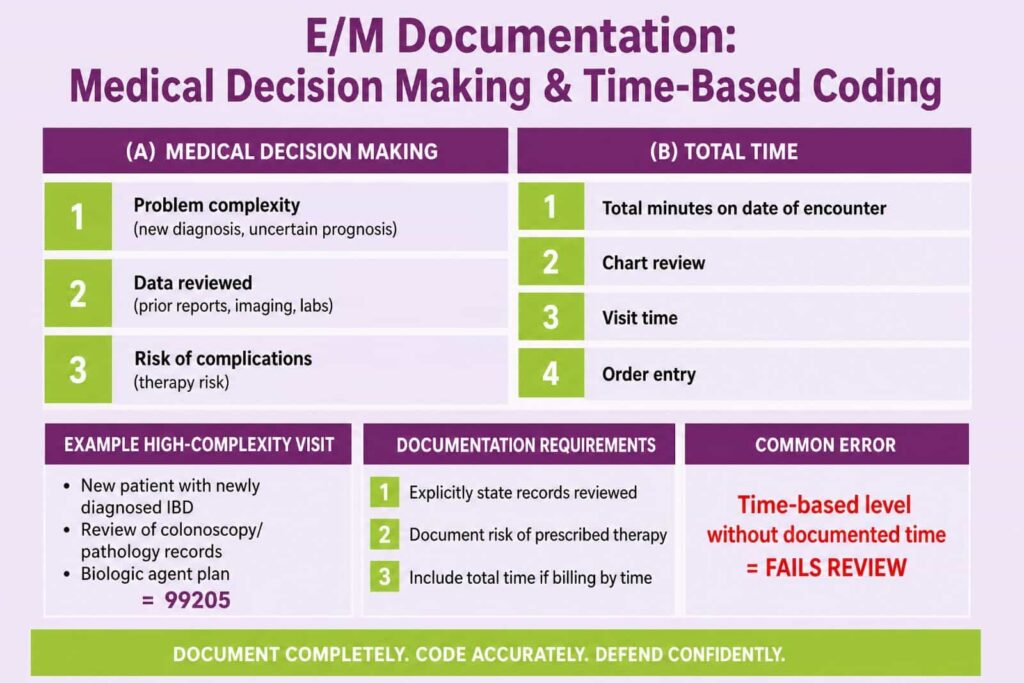
E/M documentation problems arise when notes fail to support the level billed under the 2021 and 2023 office visit guidelines. Evaluation and management coding for office and outpatient visits now rests on medical decision making or total time, not on the history and exam bullet counts used before 2021. A note built for the old bullet system frequently underdocuments the elements that now determine the level.
Medical decision-making for gastroenterology encounters draws on three components:
- Count the number and complexity of problems addressed, such as a new diagnosis with an uncertain prognosis.
- Document the data reviewed, including prior endoscopy reports, imaging, and laboratory results.
- State the risk of complications from the management plan, such as initiating immunosuppressive therapy for inflammatory bowel disease.
A new patient with newly diagnosed inflammatory bowel disease, a review of outside colonoscopy and pathology records, and a plan that starts a biologic agent support a high-complexity visit such as 99205. The note must explicitly document the records reviewed and the risk of the prescribed therapy. When the practice bills by total time instead, the note records the total minutes spent on the date of the encounter, including chart review, the visit, and order entry. A time-based level without a documented time statement does not stand up to review.
9. Place of Service and Global Period Errors
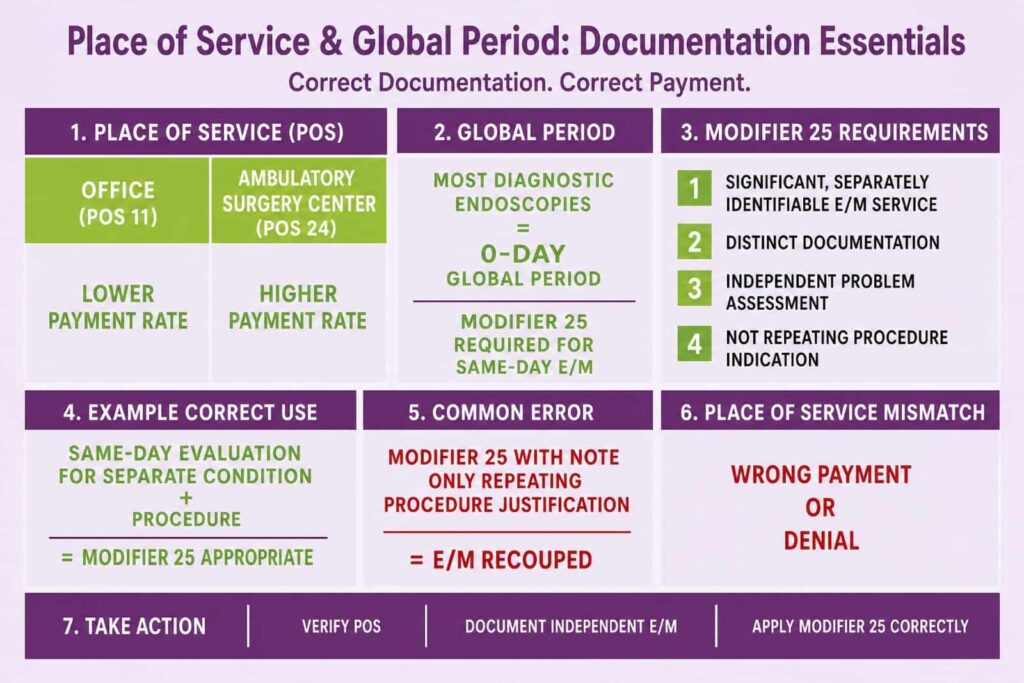
Place of service and global period documentation errors cause payment at the wrong rate and denials for services inside a procedure window. The place of service code identifies where a service occurred, and it changes the payment because facility and non-facility rates differ. A procedure performed in an ambulatory surgery center uses place of service 24, while an office procedure uses place of service 11. A mismatch between the documented location and the claimed place of service triggers a denial or an incorrect payment.
Global period documentation matters for procedures that carry a follow-up window. Most diagnostic gastroenterology endoscopies carry a 0-day global period, which means a related evaluation and management service on the same day requires modifier 25 to bill separately. Modifier 25 reports a significant, separately identifiable E/M service on the day of a procedure. The documentation must show a distinct, separately documented evaluation beyond the work inherent in the procedure.
The separate E/M note cannot restate the procedure indication. It must describe an independent problem assessment, such as the management of a separate condition or a decision to perform the procedure based on a same-day evaluation. A claim with modifier 25 and a note that only repeats the procedure justification fails on audit, and the E/M payment is recouped.
10. Incomplete Documentation for Complex Therapeutic Procedures
Complex gastroenterology procedures generate denials when the note omits the elements that distinguish a therapeutic service from a diagnostic one. Procedures such as endoscopic retrograde cholangiopancreatography, esophageal dilation, and endoscopic mucosal resection carry detailed coding rules that depend on what was performed and how. The documentation must support the specific therapeutic code rather than a lower diagnostic code. The complete coding workflow for these procedures appears in this gastroenterology billing guide.
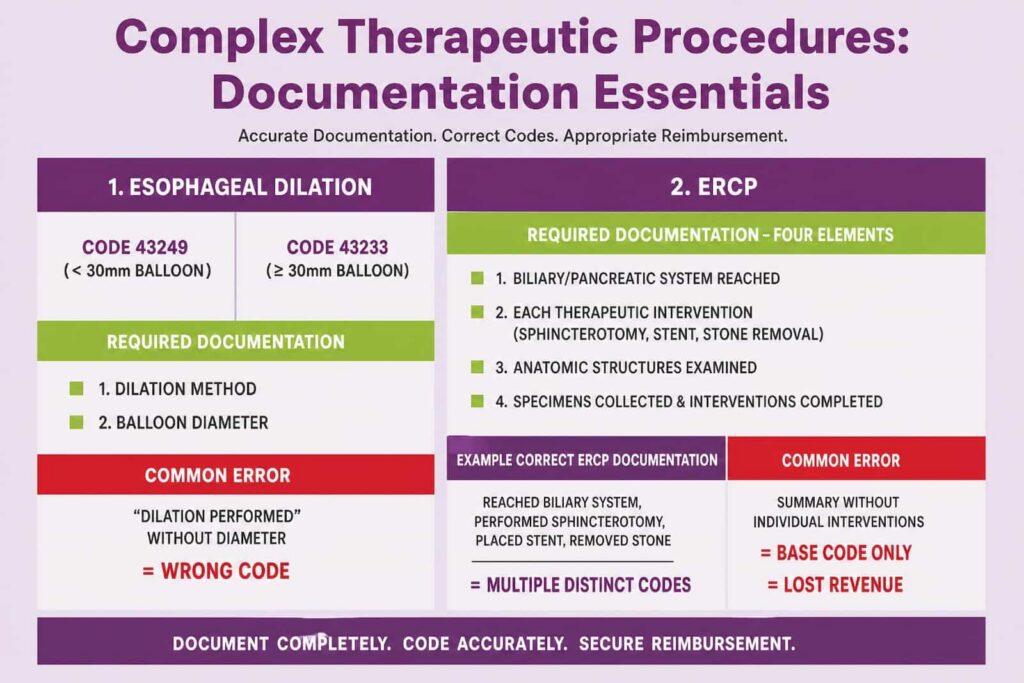
Esophageal dilation illustrates the requirement. Code 43249 reports an upper endoscopy with balloon dilation of the esophagus less than 30 millimeters in diameter. Code 43233 reports balloon dilation of 30 millimeters or larger. The note must state the dilation method and the balloon diameter for the coder to select between the two. A note that records only “dilation performed” does not support either code at the therapeutic rate.
Endoscopic retrograde cholangiopancreatography coding depends on the components performed within the session:
- Document whether the procedure reached the biliary system, the pancreatic system, or both.
- Record each therapeutic intervention, such as sphincterotomy, stent placement, or stone removal.
- State the anatomic structures examined and any contrast injection.
- Confirm the specimens collected and the interventions completed.
Each therapeutic component within an ERCP may report a distinct code, and the documentation must support every component separately. A note that summarizes the session without the individual interventions limits billing to a base code and forfeits the payment for the therapeutic work actually performed.
How Gastroenterology Practices Resolve Documentation Issues
Gastroenterology practices reduce denials by aligning the procedure note template with the coding requirements before the claim leaves the building. The 10 documentation issues above share a common root: the note omits a specific data point that a code or a payer policy requires. The correction is structural, not occasional.
Three operational changes address the majority of these issues:
- Build procedure templates that prompt for polyp size, location, technique, sedation times, and screening intent as required fields.
- Run a pre-bill review that confirms the diagnosis maps to the applicable Local Coverage Determination before submission.
- Train providers on the 2021 and 2023 E/M guidelines and on the modifier set specific to gastroenterology.
A documentation template that captures screening intent, indication detail, modifier triggers, sedation timing, lesion characteristics, diagnosis specificity, pathology correlation, decision-making elements, place of service, and therapeutic components closes the gaps that cause preventable denials. The same detail that satisfies a payer also protects the practice during a post-payment audit. Gastroenterology documentation accuracy, therefore, protects both the revenue cycle and the compliance position of the practice at the same time.