The 2026 Quality Payment Program (QPP) Final Rule is live, and the performance data your practice submits this year will directly determine your Medicare Part B payment adjustment in 2028. That adjustment can swing up to plus or minus 9 percent.
For a mid-size group practice billing $2 million annually in Part B services, that is a $180,000 difference between the best and worst outcomes. This guide covers every component of the 2026 MIPS program, from new and removed quality measures to MVP expansion, scoring methodology changes, reporting deadlines, and specialty-specific measure selection.
The performance threshold remains at 75 points. The penalty exposure remains at 9 percent. And the margin for error continues to shrink. Here is what you need to know and what you need to do for MIPS 2026 reporting.
What Changed in the 2026 QPP Final Rule?
CMS finalized the 2026 QPP Final Rule with a focus on program stability, moderate measure inventory updates, and continued expansion of MIPS Value Pathways. The rule does not introduce any sweeping structural changes, but the details matter.
The performance threshold holds steady at 75 points out of 100. CMS has confirmed this threshold will remain in place through the 2028 performance year, which determines payment adjustments through 2030. Practices that score at or above 75 receive a neutral or positive adjustment. Practices below 75 face a penalty on a linear sliding scale, maxing out at negative 9 percent for scores at 18.75 points or lower.
Three reporting pathways remain available for the 2026 performance year: Traditional MIPS, MIPS Value Pathways (MVPs), and the APM Performance Pathway (APP). CMS has not mandated MVP reporting yet, but the direction is clear towards MVP.
The payment adjustment model remains budget-neutral. Penalty dollars collected from low performers fund the bonus pool for high performers. This means your adjustment depends not only on your own score but on the distribution of scores across all MIPS participants nationally.
A score of 80 might yield a 2 percent bonus one year and a 1.5 percent bonus the next, depending on how everyone else performed. The two-year lag between performance and payment still applies. Your 2026 data determines your 2028 reimbursement.
What Are the 2026 MIPS Quality Measure Changes?
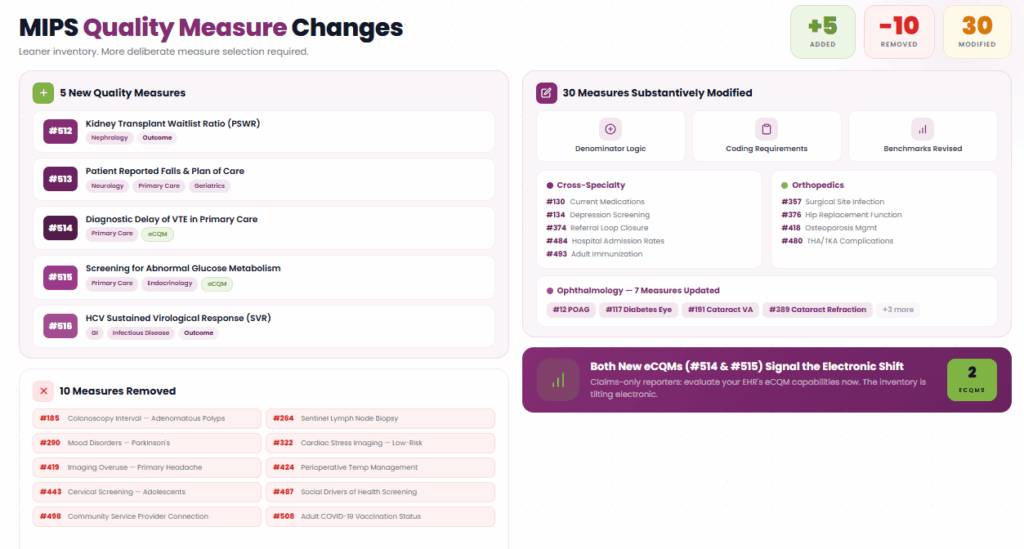
CMS finalized 5 new quality measures, removed 10 existing measures, and substantively updated 30 others for the 2026 performance year. The net result is a leaner inventory that demands more deliberate measure selection from reporting practices.
New Quality Measures for 2026
Five measures have been added to the quality inventory:
Measure #512 — Prevalent Standardized Kidney Transplant Waitlist Ratio (PSWR)
A new MIPS CQM targeting nephrology practices. This measure evaluates the proportion of eligible patients referred and active on the kidney transplant waitlist. For nephrology groups, this is a high-value outcome measure that can anchor your quality reporting.
Measure #513 — Patient Reported Falls and Plan of Care
Developed by the American Academy of Neurology. This MIPS CQM captures whether patients who report falls receive an appropriate plan of care. Relevant for neurology, primary care, and geriatric medicine.
Measure #514 — Diagnostic Delay of Venous Thromboembolism in Primary Care
An eCQM that tracks timely diagnosis of VTE in primary care settings. This is one of only two new electronic clinical quality measures added this cycle.
Measure #515 — Screening for Abnormal Glucose Metabolism in Patients
Another new eCQM. Applies broadly across primary care, endocrinology, and internal medicine. Given the prevalence of pre-diabetes in Medicare populations, expect this measure to carry significant denominator volume.
Measure #516 — Hepatitis C Virus (HCV): Sustained Virological Response (SVR)
A MIPS CQM targeting gastroenterology and infectious disease practices. Measures whether patients treated for HCV achieve sustained virological response — a true outcome measure.
Quality Measures Removed in 2026
Ten measures have been dropped from the inventory:
- Measure #185 — Colonoscopy Interval for Patients with a History of Adenomatous Polyps
- Measure #264 — Sentinel Lymph Node Biopsy for Invasive Breast Cancer
- Measure #290 — Assessment of Mood Disorders and Psychosis for Patients with Parkinson’s Disease
- Measure #322 — Cardiac Stress Imaging Not Meeting Appropriate Use Criteria (Preoperative Evaluation in Low-Risk Surgery)
- Measure #419 — Overuse of Imaging for the Evaluation of Primary Headache
- Measure #424 — Perioperative Temperature Management
- Measure #443 — Non-Recommended Cervical Cancer Screening in Adolescent Females
- Measure #487 — Screening for Social Drivers of Health
- Measure #498 — Connection to Community Service Provider
- Measure #508 — Adult COVID-19 Vaccination Status
The removal of Measures #487, #498, and #508 reflects CMS pulling back from the social determinants and COVID-era measures that were difficult to benchmark and inconsistently adopted. The removal of #443 (cervical cancer screening in adolescent females) and #264 (sentinel lymph node biopsy) signals a cleanup of measures with limited clinical variance or topped-out performance distributions.
If your practice was relying on any of these removed measures for quality reporting, you need to identify replacements now, before your 2026 reporting period opens.
Substantive Modifications to Existing Measures
Thirty existing measures received substantive updates. These are not cosmetic changes. Modified measures may have altered denominator logic, updated clinical coding requirements, or revised performance benchmarks.
Key modifications relevant across multiple specialties include:
- Measure #130 — Documentation of Current Medications in the Medical Record (updated specifications)
- Measure #134 — Preventive Care and Screening: Screening for Depression and Follow-Up Plan (updated)
- Measure #374 — Closing the Referral Loop: Receipt of Specialist Report (updated)
- Measure #484 — Risk-Standardized Hospital Admission Rates for Patients with Multiple Chronic Conditions (updated)
- Measure #493 — Adult Immunization Status (updated)
For specialty-specific modifications, orthopedic practices should pay close attention to updates.
- Measure #357 Surgical Site Infection
- Measure #376 Functional Status Assessment for Total Hip Replacement
- Measure #418 Osteoporosis Management in Women Who Had a Fracture
- Measure #480 Risk-Standardized Complication Rate for THA/TKA
Ophthalmology practices face changes to seven measures, including #12 (POAG Optic Nerve Evaluation), #117 (Diabetes Eye Exam), #191 (Cataract Surgery Visual Acuity), and #389 (Cataract Surgery Refraction).
Changes to Scoring Methodology
CMS revised the scoring methodology for claims-based quality measures. The new approach uses median-based scoring with standard deviations to determine performance thresholds, the same methodology already used for cost measures.
The practical impact is significant. Under the old methodology, a performance rate of 70 percent on a claims-based measure might have earned 5 to 5.9 points. Under the new methodology, that same 70 percent could earn 7 to 7.9 points.
This is a net positive for most practices, but it also means the competitive landscape shifts. The measure selection strategy needs to account for these new scoring curves.
CMS also removed “health equity” from the definition of high-priority measures. The scope now focuses on core clinical domains: outcomes, patient safety, care coordination, and efficiency. This simplifies measure selection but narrows what qualifies for high-priority bonus points.
Topped-Out Measures
Nineteen measures remain classified as topped-out, meaning most providers already score near the maximum. CMS will continue applying alternative benchmarks to these measures so clinicians in specialties with limited measure choice can still earn meaningful points.
Without this accommodation, topped-out measures would cap achievable scores and penalize providers who simply have no better options.
How Do MIPS Value Pathways (MVPs) Work in 2026?
MVPs remain optional in 2026, but CMS added six new pathways and imposed a significant restriction on how multispecialty groups can participate, signaling that MVPs are no longer a side experiment.
The six new MVPs for 2026 cover:
- Diagnostic Radiology
- Interventional Radiology
- Neuropsychology
- Pathology
- Podiatry
- Vascular Surgery
This brings the total to 27 available MVPs, each built around a specialty-specific set of quality measures, improvement activities, and cost measures.

The Multispecialty Group Rule Change
This is the most operationally disruptive MVP change for 2026, as multispecialty groups can no longer register as a group to report an MVP. If your group includes clinicians across multiple specialties, say cardiology, primary care, and pain management under one TIN, you cannot submit a single MVP at the group level.
Instead, multispecialty groups must register and report at the subgroup, individual, or APM Entity level. This forces practices to break apart their reporting by specialty, which adds complexity but does produce more clinically meaningful data.
CMS carved out one exception. Small practices with 15 or fewer clinicians that hold multispecialty composition may still register and report an MVP as a group. This protects smaller practices from the administrative burden of subgroup-level reporting.
Qualified Clinical Data Registries (QCDRs) and Qualified Registries now receive a one-year implementation window after a new MVP is finalized before they are required to support it fully. This matters if your registry has not yet built out support for the six new MVPs.
Why MVPs May Be Worth Considering?
If your practice is single-specialty, MVPs simplify measure selection by narrowing the quality measures to a specialty-relevant set. You are not picking from 200+ measures and hoping your data holds up.
Instead, you are reporting on a focused group of measures designed for your clinical workflow. For practices that have struggled with quality score optimization under Traditional MIPS, an MVP can be a strategic advantage.
What Are the 2026 MIPS Improvement Activity (IA) Updates?
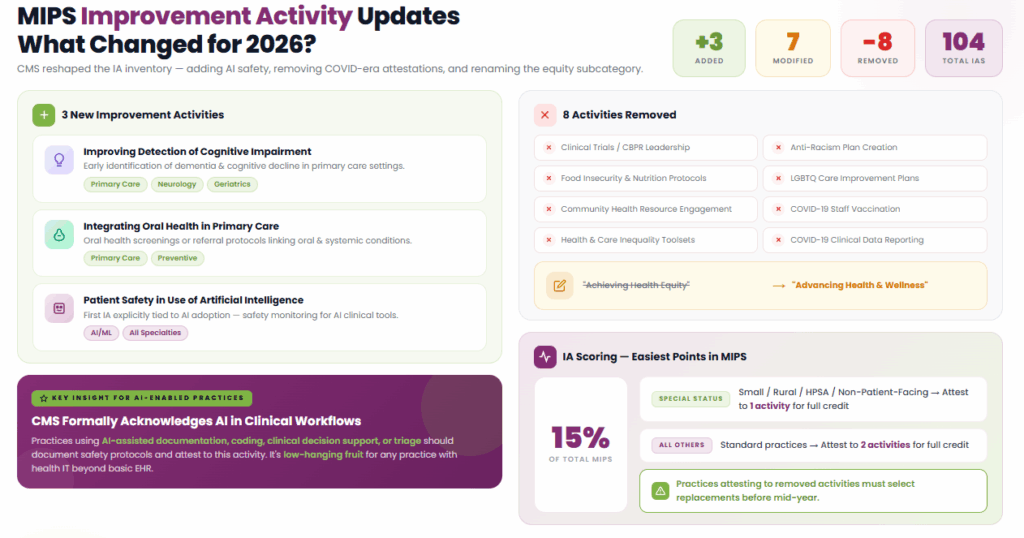
CMS added 3 new Improvement Activities (IA), modified 7 existing activities, and removed 8 from the 2026 inventory. The total stands at 104 available activities.
New Improvement Activities
Three activities have been introduced:
- Improving Detection of Cognitive Impairment in Primary Care: Targets early identification of dementia and cognitive decline. Relevant for primary care, neurology, and geriatric medicine practices.
- Integrating Oral Health Care in Primary Care: Reflects the growing evidence linking oral health to systemic conditions. Primary care practices can attest to this activity by implementing oral health screenings or referral protocols.
- Patient Safety in Use of Artificial Intelligence: This is the first improvement activity explicitly tied to AI adoption. Practices using AI clinical decision support, coding tools, or triage systems can earn credit by implementing safety monitoring protocols for those tools.
The AI-related activity is particularly notable. CMS is formally acknowledging that AI is part of clinical workflows. Practices already deploying AI-assisted tools for documentation, coding, or clinical decision support should document their safety protocols and attest to this activity. It is low-hanging fruit for any practice that has adopted health IT beyond basic EHR.
Removed Activities
Eight activities have been retired, mostly tied to COVID-era programs and the former Achieving Health Equity subcategory:
- Clinical Trials or CBPR leadership
- Anti-Racism Plan creation
- Food Insecurity and Nutrition Risk Protocols
- LGBTQ care improvement plans
- Community resource engagement for health drivers
- COVID-19 vaccination achievement for staff
- Health and care inequality toolsets
- COVID-19 clinical data reporting
CMS renamed the “Achieving Health Equity” subcategory to “Advancing Health and Wellness.” The framing shift reflects a pivot away from equity-specific attestation toward broader health outcome activities. From a reporting standpoint, practices that were attesting to the removed activities need to select replacements from the updated inventory before mid-year.
Scoring Reminder
Improvement Activities account for 15 percent of your total MIPS score. Small, rural, non-patient-facing, or health professional shortage area special status practices need to attest to one activity for full credit, whereas all others attest to two activities to meet reporting requirements. This category remains the easiest place to earn points, as the threshold is low, and attestation is easy. Do not leave these points on the table.
What Are the 2026 Promoting Interoperability Requirements?
The Promoting Interoperability (PI) category accounts for 25 percent of your total MIPS score and measures your use of certified EHR technology and health information exchange capabilities. For 2026, the core requirements remain stable, but CMS updated the SAFER Guide requirement and continued pushing the eCQM reporting trajectory.
The PI category evaluates your practice across five measure groups: e-Prescribing, Health Information Exchange, Provider-to-Patient Exchange, Public Health and Clinical Data Exchange, and Protect Patient Health Information. Each group has required bonus measures. Practices must report on all required measures and can earn additional points through bonus measures.
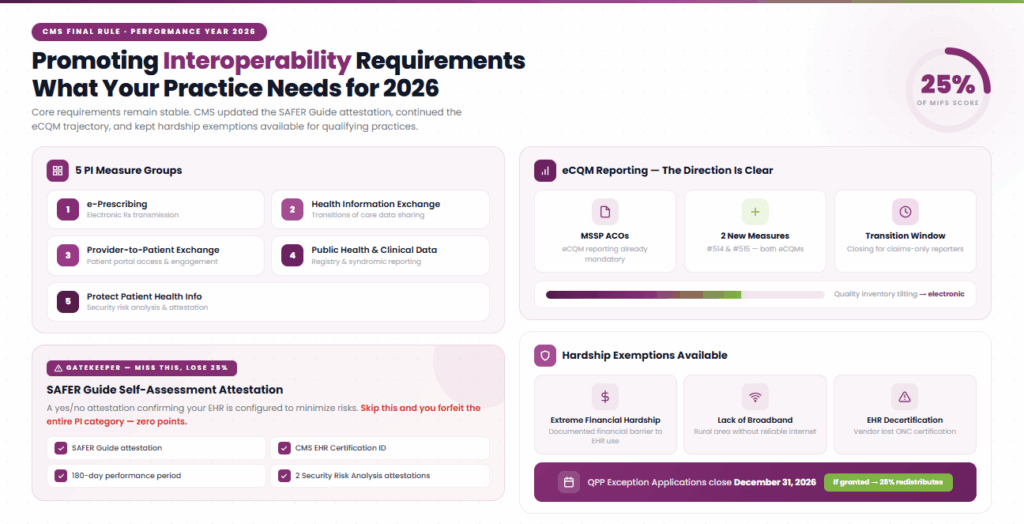
SAFER Guide Requirement
CMS updated the Safety Assurance Factors for EHR Resilience (SAFER) Guide requirement for 2026. This is a yes/no attestation that your practice has completed the SAFER self-assessment, which evaluates whether your EHR system is configured and used to minimize risks.
Completing this attestation is a prerequisite for earning any PI category points. Miss it, and you forfeit the entire 25 percent weight. To earn more than zero PI points, clinicians also need the CMS EHR Certification ID, a minimum 180-day performance period, the 2 Security Risk Analysis attestations, and the required PI measure reporting or applicable exclusions.
eCQM Reporting Direction
CMS has been signaling for multiple years that electronic clinical quality measure (eCQM) reporting is the future of the quality program. For ACOs in the Medicare Shared Savings Program, eCQM reporting is already mandatory. For Traditional MIPS reporters, it is not yet required, but the two new quality measures added for 2026 (#514 and #515) are both eCQMs. The inventory is tilting electronics.
Practices still relying on manual chart abstraction or claims-only reporting for quality measures should begin evaluating their EHR’s eCQM generation capabilities. The transition window is closing. Data completeness, patient matching accuracy, and measure logic configuration within your EHR directly affect your eCQM scores.
Hardship Exemptions
If your practice faces circumstances that make PI reporting impractical, such as extreme financial hardship, lack of broadband in a rural area, or decertification of your EHR, you can apply for a PI hardship exemption. If granted, the 25 percent weight redistributes to other categories. The QPP Exception Applications window closes December 31, 2026.
How Does the MIPS Cost Category Work in 2026?
CMS finalized 35 cost measures for the 2026 performance year with no new additions or removals. The Cost category accounts for 30 percent of your total MIPS score, making it the joint-heaviest category alongside Quality.
Here is the critical distinction that you do not submit cost data. CMS calculates your cost performance using Medicare Part B claims data. Your cost score is derived from how your attributed patient spending compares to risk-adjusted, peer-group benchmarks.
This means your cost score is driven by two factors you can influence, including the accuracy of your risk adjustment coding (HCC capture) and your referral and utilization patterns. Incomplete or inaccurate Hierarchical Condition Category (HCC) coding understates patient acuity.
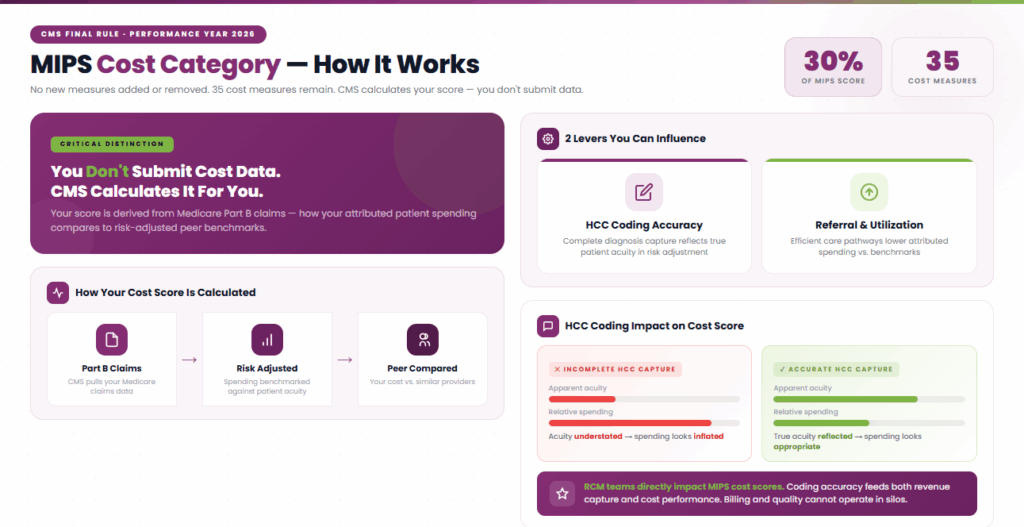
When acuity looks lower on paper, your spending looks higher relative to peers, even if your clinical care is appropriate. Practices that invest in documentation improvement, accurate diagnosis capture, and HCC coding optimization consistently outperform on cost. This is where RCM teams play a direct role in MIPS success.
The billing team and the quality team cannot operate in silos. Coding accuracy feeds both revenue capture and MIPS cost scoring. For practices participating in ACOs or MSSP, cost performance is evaluated under different benchmark methodologies, but the underlying principle is the same.
Who Must Report MIPS in 2026?
MIPS applies to eligible clinicians who meet CMS volume thresholds based on Medicare Part B allowed charges, patient count, and covered professional services during the determination period. If you are exempt from mandatory MIPS participation due to the low-volume threshold, you may still be eligible to opt in for the performance year if you exceed 1 or 2, but not all 3, elements of the low-volume threshold.
Opt-in eligible clinicians can report Traditional MIPS or the APP, but not an MVP. If you opt in and report, your score counts, and your payment can be adjusted based on that score.
Eligible Clinician Types
The following clinician types are subject to MIPS:
- Physicians (including doctors of medicine, osteopathy, dental surgery, dental medicine, podiatric medicine, and optometry)
- Nurse Practitioners (NP)
- Physician Assistants (PA)
- Clinical Nurse Specialists (CNS)
- Certified Registered Nurse Anesthetists (CRNA)
- Osteopathic practitioners
- Chiropractors
- Physical therapists
- Occupational therapists
- Clinical psychologists
- Qualified speech-language pathologists
- Qualified audiologists
- Registered dietitians or nutrition professionals
- Clinical social workers
- Certified nurse midwives
Reporting Structures
Practices may report as individuals, as a group (TIN-level), or as part of a virtual group. The reporting structure you choose has a direct impact on scoring. Group reporting aggregates performance across all clinicians under a single TIN, which can help smooth out individual outlier performance. Individual reporting allows each clinician to report separately, which can be advantageous when certain clinicians perform significantly higher than the group average.
For practices in the Medicare Shared Savings Program (MSSP), reporting through the APM Performance Pathway (APP) uses a simplified set of quality measures and different scoring rules. Clinicians who achieve Qualifying APM Participant (QP) status are excluded from MIPS entirely and receive a higher qualifying APM conversion factor.
Checking Eligibility
CMS publishes eligibility status through the QPP website. Every practice should verify eligibility status early in the performance year. Eligibility misunderstandings are one of the most common causes of avoidable penalties. A clinician who believes they are exempt but is not will receive an automatic zero score and the maximum 9 percent penalty.
What Is the 2026 MIPS Reporting Timeline?
The 2026 MIPS performance period runs January 1 through December 31, 2026, with data submission to CMS between January 2 and March 31, 2027. But effective MIPS reporting is not a year-end exercise. It is a quarterly operational cadence. Key dates for 2026, including CMS official deadlines, are:
Q1: Foundation
- January 1, 2026: Performance period begins
- April 15, 2026: Send Q1 billing data to your registry or qualified data partner
- May 1, 2026: Select quality measures
- May 15, 2026: Send Q1 numerator data
Q2: First Check
- May 30, 2026: Review initial Promoting Interoperability performance; select initial Improvement Activities
- June 14, 2026: Review initial quality measure performance
- June 30, 2026: CAHPS survey registration deadline
- July 5, 2026: Last day to start a 180-day performance period for PI
- July 15, 2026: Send Q2 billing data
Q3: Mid-Course Correction
- August 15, 2026: Send Q2 numerator data; review quality performance
- October 3, 2026: Last day to start a 90-day performance period for Improvement Activities
- October 15, 2026: Send Q3 billing data
- November 15, 2026: Send Q3 numerator data; review quality performance
- November 30, 2026: MVP registration deadline
Q4: Close Out
- PY2025 MIPS eligibility finalized
- December 31, 2026: QPP exception applications window closes; performance period ends
Q1 2027: Submission
- January 15, 2027: Send all end-of-year data; finalize PI and IA attestations; complete permission forms
- January 30, 2027: Review final performance scoring
- January 2 to March 31, 2027: Data submission window to CMS
Practices that wait until Q4 to assess their MIPS standing are already behind. Quarterly data review gives you three opportunities to course-correct before submission. A measure that is underperforming in Q2 can be swapped or supplemented before year-end. A missed Improvement Activity (IA) attestation can still be completed if caught early enough.
All of these timely actions are possible to prevent revenue loss with the help of expert MIPS services providers like Macralytics.
Which MIPS Quality Measures Apply to Your Specialty in 2026?
Measure selection is where most practices either win or lose the quality game. Choosing the right six measures, with at least one outcome measure, for your specialty and patient population is the single most impactful decision in your MIPS reporting strategy.
Pain Management
Pain management practices should focus on measures related to opioid prescribing, functional outcome assessments, and care coordination. Key measures include depression screening (#134, recently modified), medication documentation (#130, modified), and pain-specific functional assessments. The new Patient Reported Falls measure (#513) may also apply to pain practices managing older patients with mobility concerns.
Cardiology
Cardiology practices should evaluate the updated Risk-Standardized Hospital Admission Rates for Patients with Heart Failure (#484, modified). The removal of Measure #322 (Cardiac Stress Imaging in Low-Risk Surgery) eliminates a measure that any cardiology group previously used. Replace it with a remaining appropriate-use or outcome measure.
Adult Immunization Status (#493) and Closing the Referral Loop (#374) both received modifications and remain available as broadly applicable measures.
Nephrology
The addition of Measure #512 (Prevalent Standardized Kidney Transplant Waitlist Ratio) is the most significant nephrology development in the 2026 measure set. This outcome measure directly addresses a clinical priority, ensuring eligible patients are referred for and maintained on the transplant waitlist. Nephrology practices should also consider diabetes screening (#515, new eCQM) given the overlap between diabetic populations and CKD.
Psychiatry
With the removal of Measure #290 (Mood Disorders and Psychosis Assessment for Parkinson’s), psychiatry practices lose a niche measure. Depression Screening (#134) remains available with updated specifications. The new Cognitive Impairment Detection improvement activity pairs well with psychiatry’s clinical scope.
Gains in Patient Activation Measure scores (#503, modified) are another measure psychiatry practices should evaluate for patient engagement reporting.
OBGYN
The removal of Measure #443 (Non-Recommended Cervical Cancer Screening in Adolescent Females) eliminates an OBGYN-relevant inverse measure. Practices should review the remaining inventory for applicable preventive care and maternal health measures.
Diabetes Eye Exam (#117, modified) may have cross-referral relevance for OBGYN practices managing gestational diabetes patients.
Orthopedics
Four orthopedic measures received modifications, including Surgical Site Infection (#357), Functional Status Assessment for Total Hip Replacement (#376), Osteoporosis Management (#418), and Risk-Standardized Complication Rate for THA/TKA (#480).
Orthopedic practices should review the updated specifications for these measures carefully, as denominator logic changes can shift your reported performance even if your clinical outcomes are unchanged.
How Can You Maximize Your 2026 MIPS Score and Avoid the 9 Percent Penalty?
Score optimization starts with measure selection and ends with data discipline. The practices that consistently score above 75 points are not doing anything exotic. They are just making deliberate choices early and executing consistently throughout the year.
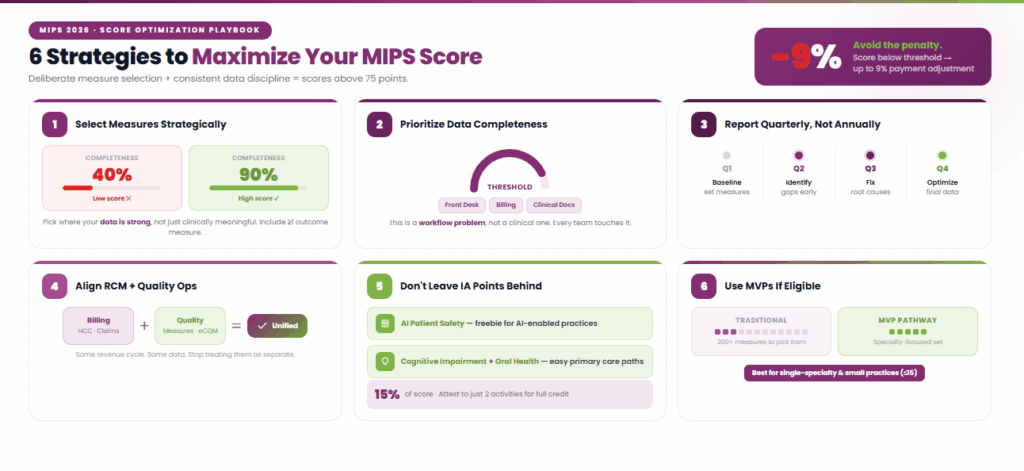
1. Select Measures Strategically
Choose quality measures where your practice has strong historical performance and reliable data capture. Do not pick measures based on clinical importance alone. Pick measures where you can demonstrate high performance with complete data.
A clinically meaningful measure where your data completeness is 40 percent will score worse than a simpler measure with 90 percent completeness. Include at least one outcome measure. CMS weights these more heavily in the scoring algorithm, and they signal clinical maturity.
2. Prioritize Data Completeness
CMS evaluates not just your performance rate but your data completeness (the proportion of eligible patients for whom you reported data). Failing to meet the required data completeness threshold can significantly reduce your score, even when underlying clinical performance is strong. This is a workflow problem, not a clinical problem. Your front-desk, billing, and clinical documentation teams all play a role.
3. Report Quarterly, Not Annually
Review your quality measure performance every quarter. Identify underperforming measures in Q2 and address root causes before Q4. If a measure is consistently underperforming due to workflow gaps or coding issues, you have time to adjust.
4. Align RCM and Quality Operations
Your HCC coding accuracy directly impacts your cost score. Your claims data completeness impacts your quality measure denominators. These are not separate workstreams, as they are the same revenue cycle. Practices that align their billing teams with their quality reporting teams consistently outperform those that treat them as separate functions.
5. Do Not Leave Improvement Activity Points on the Table
The IA category is 15 percent of your total score and requires only two high-weighted or four medium-weighted attestations. The new AI Patient Safety activity is a freebie for any practice already using AI-driven tools. Cognitive Impairment Detection and Oral Health Integration offer easy attestation paths for primary care. There is no reason to lose points here.
6. Use MVPs If Eligible
If you are a single-specialty practice, evaluate whether an MVP pathway produces a better score than Traditional MIPS. MVPs narrow your measure set to specialty-relevant options and can simplify both the selection and reporting process. For small practices (15 or fewer clinicians), this is especially attractive.
What Should Practices Do Right Now to Prepare?
The 2026 performance year is already underway. Every day you delay your MIPS planning is a day of data you may not be able to recover at year-end.
Verify Your Eligibility: Check the QPP website to confirm which clinicians and groups under your TIN are MIPS-eligible for 2026.
Review Removed Measures: If your practice was reporting on any of the 10 removed measures, identify replacement measures immediately. Do not wait until Q3 to discover a gap.
Select Your Quality Measures: Aim to finalize measure selection by May 1. Choose measures where you have strong data capture and historical performance.
Decide Your Reporting Pathway: Traditional MIPS, MVP, or APP. Each has different measure sets, registration requirements, and scoring implications. Make this decision before mid-year.
Set Up Quarterly Data Review: Establish a cadence for pulling and reviewing quality data every quarter. Your Q1 data should be in your registry by April 15.
Align Your RCM and Quality Teams: Coding accuracy, claims completeness, and clinical documentation all feed MIPS scoring. These teams need shared visibility into performance data.
Attest to Improvement Activities Early: Select your IA attestations now. The new AI Patient Safety activity is easy credit for any practice using AI-assisted clinical or administrative tools.
Complete Your SAFER Guide: This PI prerequisite must be attested before you can earn any Promoting Interoperability points. Do not let a missed checkbox or error cost you 25 percent of your total score.
The practices that score highest in MIPS are not the ones with the most resources. They are the ones that start early, measure quarterly, and treat MIPS reporting as an operational function.
Take the complexity out of MIPS with Transcure MIPS Consulting Services. From measure selection to quarterly tracking and final submission, Transcure handles everything. Our MIPS consultant provides accuracy, maximizes scores, and reduces penalty risk for your practice.