CPT 2027 brings the biggest restructuring to maternity care coding in decades. For OB/GYN billing teams, this is not a minor update. The AMA Editorial Panel has approved a complete overhaul effective January 1, 2027. The global OB package model is gone. In its place, every phase of pregnancy care is billed separately.
That shift touches every coder, biller, and practice manager working in this specialty. As these changes take effect, many practices are actively evaluating OB GYN billing services to manage the increased complexity and ensure compliance with evolving AMA guidelines.
This guide will break down the new maternity CPT codes 2027. It explains how to report antepartum care, labor management, delivery services, and postpartum visits correctly. You will also learn the new code sets, documentation requirements, and maternity billing guidelines that directly impact reimbursement.
Why CPT 2027 Is a Major Shift for OB/GYN Coding?
For years, practices billed global packages that bundled antepartum visits, delivery, and postpartum care into one claim. OB GYN CPT codes 2027 eliminate that model entirely.
The new framework requires separate reporting for each phase. Antepartum care uses E/M codes. Labor management has brand-new codes. Delivery care and postpartum visits each have their own reporting rules. This change affects how practices document, code, and submit claims.
Key Objectives of the New Guidelines
- Improve coding accuracy and transparency across all phases of care
- Align reimbursement directly with the services a provider actually performs
- Support value-based care models with phase-specific billing
What Is Included in Maternity Care Services Under CPT 2027?
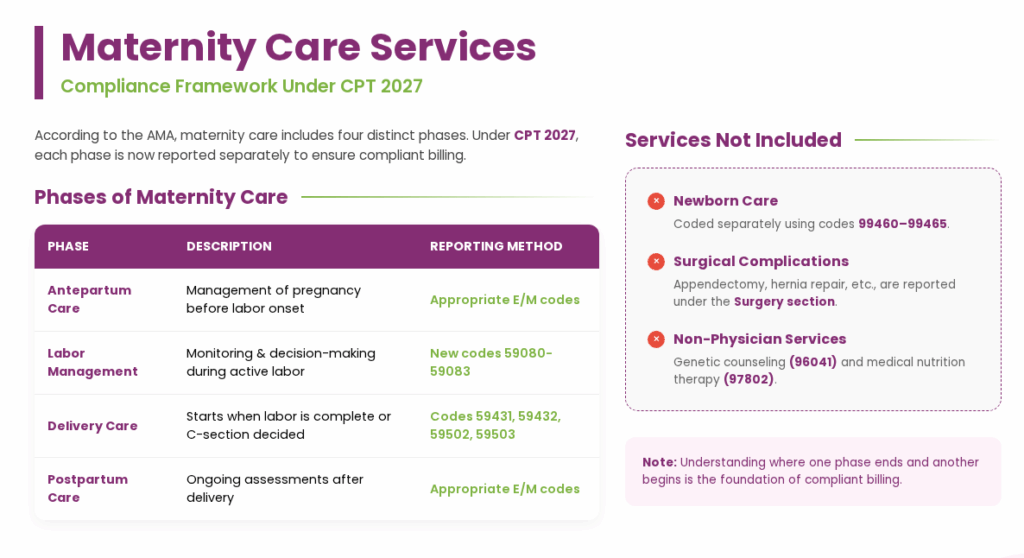
According to the AMA, maternity care includes four distinct phases: outpatient and inpatient antepartum care, labor management, delivery care, and inpatient and outpatient postpartum care.
Each phase is now reported separately. Understanding where one phase ends and another begins is the foundation of compliant billing under CPT 2027.
Phases of Maternity Care
Under CPT 2027, maternity care is divided into four clearly defined phases, and each phase is reported separately.
| Phase | Description | Reporting Method |
|---|---|---|
| Antepartum Care | Management of pregnancy before the onset of labor | Appropriate E/M codes |
| Labor Management | Monitoring and decision-making during active labor | New codes 59080-59083 |
| Delivery Care | Begins when labor is complete, or a cesarean decision is made | Delivery codes 59431, 59432, 59502, 59503 |
| Postpartum Care | Ongoing assessments after delivery | Appropriate E/M codes |
Services Not Included in Maternity Coding
- Newborn care is coded separately using codes such as 99460, 99461, 99462, 99463, 99464, and 99465
- Surgical complications of pregnancy, such as appendectomy, hernia repair, or ovarian cyst removal, are reported under the Surgery section
- Non-physician services, including genetic counseling and medical nutrition therapy, are reported with specialty-specific codes like 96041 and 97802
Elimination of Global OB Codes
The most significant change is the deletion of the global OB package codes. Practices can no longer use these codes after December 31, 2026:
| Deleted Code | What It Covered | What to Use Instead |
|---|---|---|
| 59400 | Vaginal delivery with antepartum and postpartum care | E/M codes + 59431/59432 + E/M codes |
| 59510 | Cesarean delivery with antepartum and postpartum care | E/M codes + 59502/59503 + E/M codes |
| 59610 | VBAC with antepartum and postpartum care | E/M codes + 59432 + E/M codes |
| 59409, 59410 | Vaginal delivery only (without antepartum/postpartum) | 59431 or 59432 |
| 59514, 59515 | Cesarean delivery only | 59502 or 59503 |
| 59425, 59426 | Antepartum care only (4-6 or 7+ visits) | Appropriate E/M codes per visit |
| 59430 | Postpartum care only | Appropriate E/M codes per visit |
| 59525 | Subtotal hysterectomy after cesarean | 59504 |
| 59612, 59614 | VBAC delivery only | 59432 |
| 59618, 59620, 59622 | Cesarean after failed VBAC | 59503 |
Shift to Component-Based Coding
Every phase of maternity care is now reported independently. There is no bundled claim. Each calendar date, each type of service, and each provider role requires its own code selection.
This creates more billing touchpoints per patient episode but also more opportunities to capture reimbursement for services that were previously absorbed into the global package.
Increased Role of E/M Codes
Antepartum and postpartum care are now reported exclusively through E/M services. This applies across every care setting:
- Office or other outpatient visits (99202-99215)
- Telemedicine and virtual check-in services (98000-98016)
- Home or residence visits (99341-99350)
- Initial and subsequent hospital inpatient or observation services (99221-99236)
- Critical care services (99291, 99292)
Antepartum Care Coding Guidelines
Antepartum care covers all management of pregnancy before labor begins. Under CPT 2027, every antepartum visit is reported with the appropriate E/M code for the setting in which it takes place.
Pregnancy confirmation during any encounter may also be reported with the appropriate E/M code for that setting.
How to Report Antepartum Care
The E/M code selected should reflect the setting, the complexity of medical decision making, and the time spent when applicable. There is no fixed number of visits bundled together. Each encounter stands alone.
| Setting | Applicable Codes | Notes |
|---|---|---|
| Office Visits | 99202-99205 (new), 99211-99215 (established) | Most common setting for antepartum visits |
| Telemedicine | 98000-98015 | Acceptable for antepartum management |
| Virtual Check-in | 98016 | For brief patient-initiated communication |
| Home/Residence | 99341-99350 | When the provider sees the patient at home |
| Hospital Inpatient/Observation | 99221-99236 | For admitted antepartum patients |
| Critical Care | 99291, 99292 | For critically ill pregnant patients |
Separate Reporting Rules for Antepartum
Two categories of services are always billed separately from the antepartum E/M visit:
- Diagnostic imaging such as obstetrical ultrasound (76801-76828) and fetal MRI (74712, 74713)
- Antepartum and fetal invasive procedures, which have their own CPT codes
When a pregnant patient is admitted to the hospital during an office or emergency department encounter, the initial site of service E/M may be reported separately. Use Modifier 25 to indicate a significant, separately identifiable service was performed on the same calendar date.
Modifier Usage in Antepartum Care
Modifier 25 applies when a provider performs a significant, separately identifiable E/M service on the same date as another procedure. For antepartum patients, this is relevant in two main scenarios:
- When the patient is admitted to the hospital during an office or ED encounter
- When initial labor management begins on the same date as a prior E/M service in a different setting
Antepartum Procedures and Fetal Invasive Services
Fetal procedures and antepartum invasive services are reported separately from the E/M visit. Diagnostic imaging is also always separately billable.
Common CPT Codes for Fetal Procedures
| CPT Code | Procedure |
|---|---|
| 59000 | Amniocentesis, diagnostic |
| 59001 | Therapeutic amniotic fluid reduction |
| 59012 | Cordocentesis, any method |
| 59015 | Chorionic villus sampling, any method |
| 59020 | Fetal contraction stress test |
| 59025 | Fetal non-stress test |
| 59070 | Transabdominal amnioinfusion |
| 59072 | Fetal umbilical cord occlusion |
| 59074 | Fetal fluid drainage (vesicocentesis, thoracocentesis, paracentesis) |
| 59076 | Fetal shunt placement |
| 59320 | Cerclage of cervix during pregnancy, vaginal |
| 59325 | Cerclage, abdominal |
| 59412 | External cephalic version |
| 59866 | Multifetal pregnancy reduction(s) |
| 59871 | Removal of cerclage suture under anesthesia |
| 36460 | Fetal intrauterine transfusion |
| 59897 | Unlisted fetal invasive procedure |
Labor Management Coding: New in CPT 2027
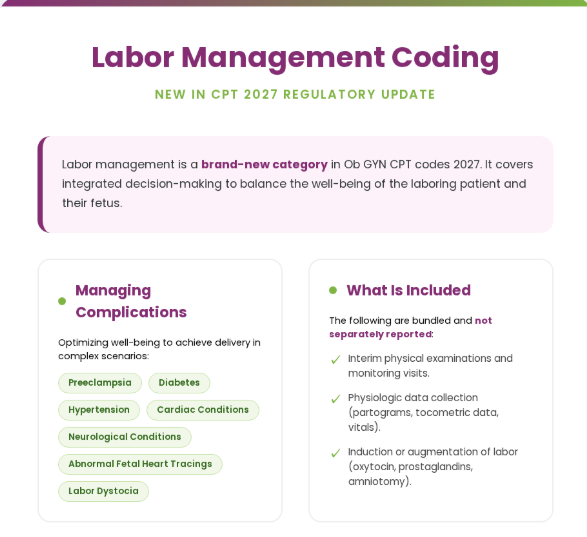
Labor management is a brand-new category in Ob GYN CPT codes 2027. It covers the integrated decision-making required to assess, support, and balance the well-being of the laboring patient and their fetus or fetuses.
This includes managing medical conditions or complications such as cardiac or neurological conditions, diabetes, hypertension, preeclampsia, abnormal fetal heart tracings, and labor dystocia. The goal is to optimize well-being and achieve delivery.
What is Included in Labor Management
The following services are included in labor management and are not separately reported:
- Interim physical examinations and monitoring visits
- Collection and interpretation of physiologic data, including partograms, tocometric data, vital signs, and pulse oximetry
- Induction or augmentation of labor, including mechanical cervical dilation, prostaglandins, oxytocin, and amniotomy
Labor Management CPT Codes
The following CPT codes are used to report labor management based on the day of service and clinical complexity.
| CPT Code | Description | When to Report |
|---|---|---|
| 59080 | Initial day labor management, straightforward, per day | First calendar date of labor management, uncomplicated |
| 59081 | Initial day labor management, complex, per day | First calendar date, with complicating factors |
| 59082 | Subsequent day labor management, straightforward, per day | Each subsequent calendar date, uncomplicated |
| 59083 | Subsequent day labor management, complex, per day | Each subsequent calendar date, with complicating factors |
Key Reporting Rules for Labor Management
- A face-to-face encounter with the patient is required.
- Codes are reported once per calendar date.
- Multiple visits by the same provider or the same group on a single calendar date are reported as a single labor management service.
- A continuous visit that spans the midnight transition of two calendar dates is a single service, reported on one of the two dates.
- For multiple gestations, labor management is reported only once per calendar date, regardless of the number of fetuses.
Initial vs. Subsequent Day Labor Management
Initial day labor management (59080 or 59081) may only be reported when one of these criteria is met:
- It is the first calendar date on which the patient requires labor management or induction to begin
- The provider or the same group has not previously performed labor management during this admission
- The patient is transferred to a new facility after receiving labor management at another facility
- A provider of a different specialty or subspecialty assumes care for medical necessity reasons
If none of the above criteria are met, report subsequent day labor management (59082 or 59083).
Subsequent day codes may be reported on multiple calendar dates when treatment is intended to result in delivery, including on the calendar date of delivery if labor management is also performed that day.
Straightforward vs. Complex Labor Management
CPT 2027 separates labor management into straightforward and complex categories, based on patient risk factors, fetal status, and clinical decision-making.
| Straightforward Labor (59080, 59082) | Complex Labor (59081, 59083) |
|---|---|
| Singleton vertex presentation | More than one fetus present |
| Routine maternal and fetal monitoring | Fetal monitoring abnormalities requiring a change in management |
| Fetal heart rate not requiring provider intervention | Prolonged first or second stage of labor |
| Normal labor progression or routine induction/augmentation | Labor complications such as intraamniotic infection or preeclampsia |
| Stable medical conditions not requiring additional management | One or more severe maternal morbidity indicators (e.g., acute renal failure, eclampsia) |
| No previous cesarean delivery | Maternal medical conditions requiring additional management during labor |
| Previous cesarean delivery |
The duration of labor does not determine complexity unless prolonged labor is specifically diagnosed. Report the highest level of labor management performed once per calendar date.
When NOT to Report Labor Management
- When a patient presents for a planned or scheduled cesarean delivery and is not in labor
- On the same calendar date as an inpatient E/M service (99221-99236) billed by the same provider or same group practice
Note: Do not report 59080 in conjunction with 59081 for the same calendar date. Do not report 59082 in conjunction with 59083 for the same calendar date.
Labor Procedures
In addition to labor management services, certain procedures performed during labor are reported separately using specific CPT codes.
| CPT Code | Description |
|---|---|
| 59030 | Fetal scalp blood sampling (use modifier 76 or 77 for repeat sampling) |
| 59051 | Fetal monitoring during labor by a consulting physician or other QHP, with interpretation and report |
Delivery Care Coding Guidelines
Delivery care begins at a specific clinical moment. For vaginal delivery, that moment is when the presenting part of the fetus is visible and firmly rimmed by the vaginal introitus. For cesarean delivery, it begins with the decision for cesarean delivery when arrest of labor is diagnosed.
Delivery care includes management of the patient and fetus or fetuses. It does not include the work of labor management.
What Is Included in Delivery Care
Immediate postpartum care on the same calendar date as delivery is considered part of delivery care and may not be separately reported.
When a patient is discharged on the same date as delivery, hospital discharge day management codes (99238, 99239) are also not separately reported.
Vaginal Delivery Coding
Vaginal delivery includes delivery of the fetus and placenta and repair of first- or second-degree episiotomy or spontaneous lacerations. Here are the key vaginal delivery CPT codes for your reference:
| CPT Code | Description | Key Notes |
|---|---|---|
| 59431 | Vaginal delivery, with or without episiotomy | Standard vaginal delivery code |
| 59432 | Vaginal delivery after previous cesarean delivery (VBAC) | Use for successful VBAC; also for breech vaginal delivery with modifier 22 |
| 59433 | Repair of episiotomy or laceration, third-degree | Separately reportable in addition to 59431 or 59432 |
| 59434 | Repair of episiotomy or laceration, fourth-degree | Separately reportable in addition to 59431 or 59432 |
| 59414 | Delivery of placenta only (separate procedure) | Report when performed by a different provider than the one delivering the fetus |
| 59300 | Repair of first or second-degree laceration or episiotomy by other than the attending provider | Do not report with 59431 or 59432 |
Special Vaginal Delivery Scenarios
- For multiple gestations, report one vaginal delivery code per fetus delivered vaginally
- If vaginal delivery is attempted but a cesarean is performed instead, report only the cesarean delivery code
- A breech vaginal delivery is reported with 59431 or 59432 and Modifier 22
- Repair of third- or fourth-degree laceration is not included in 59431 or 59432 and is separately reported with 59433 or 59434
Cesarean Delivery Coding
The following C-section CPT codes are used to report cesarean delivery, depending on the patient’s history and the procedures performed.
| CPT Code | Description | Key Notes |
|---|---|---|
| 59502 | Primary cesarean delivery | For a patient who has not previously had a cesarean, typically unplanned following labor |
| 59503 | Repeat cesarean delivery | For a patient who has previously had a cesarean, typically a planned event |
| 59504 | Subtotal or total hysterectomy after cesarean delivery | Report with Modifier 51 when the same provider performs both procedures |
Special Cesarean Delivery Scenarios
- For multiple gestations via cesarean, report only one cesarean delivery code regardless of the number of fetuses
- When one fetus is delivered vaginally and another via cesarean, report the appropriate vaginal code per vaginal fetus plus one cesarean code
- When a subtotal or total hysterectomy is performed during the same session as cesarean delivery, use 59504
- For fallopian tube ligation at the time of cesarean, use 58611
For an unplanned or unscheduled cesarean in a laboring patient, delivery may be reported together with labor management (59081 or 59083). For a planned primary cesarean without labor, an E/M service may be separately reported on the same date. For a repeat planned cesarean, inpatient E/M services are included and may not be separately reported.
Postpartum Care Coding
Postpartum care is no longer bundled. Every postpartum service is reported as an E/M visit, whether inpatient or outpatient, on any calendar date after the delivery date.
Postpartum Care Overview
Postpartum care includes ongoing assessments tailored to the individual patient. The same day as delivery, immediate postpartum care is part of the delivery service and is not separately reported. Beginning on the next calendar date, all postpartum services are billed using E/M codes.
Inpatient Postpartum Coding
After the delivery date, all inpatient postpartum services are coded using appropriate hospital E/M codes depending on the level of care and discharge timing.
| Code Range | Description | When to Use |
|---|---|---|
| 99231-99233 | Subsequent hospital inpatient or observation care | Daily inpatient postpartum visits after the delivery date |
| 99238-99239 | Hospital discharge day management | When the patient is discharged on a date after delivery |
| 99234-99236 | Hospital inpatient or observation care, including admission and discharge | Same-day admission and discharge on a postpartum date |
| 99291-99292 | Critical care services | For critically ill postpartum patients |
Note: Do not report inpatient E/M services (99231-99239) on the same calendar date as delivery care.
Outpatient Postpartum Coding
All outpatient postpartum visits on a date after the delivery date use the standard E/M code for the setting:
- Office visits: 99202-99215
- Telemedicine: 98000-98015
- Virtual check-in: 98016
- Home or residence visits: 99341-99350
Postpartum Procedures and Complications
Apart from routine postpartum care, certain complications and procedures may require separate reporting using specific CPT codes.
Common Postpartum Procedure Codes
| CPT Code | Procedure |
|---|---|
| 59623 | Uterine tamponade (balloon, catheter, vacuum, packing material) |
| 59160 | Curettage, postpartum |
| 59350 | Hysterorrhaphy of the ruptured uterus |
Ectopic Pregnancy Procedure Codes
| CPT Code | Description |
|---|---|
| 59120 | Surgical treatment of ectopic pregnancy, tubal or ovarian, requiring salpingectomy and/or oophorectomy |
| 59121 | Tubal or ovarian, without salpingectomy and/or oophorectomy |
| 59130 | Abdominal pregnancy |
| 59136 | Interstitial, uterine pregnancy with partial resection of the uterus |
| 59140 | Cervical, with evacuation |
| 59150 | Laparoscopic treatment of ectopic pregnancy, without salpingectomy and/or oophorectomy |
| 59151 | Laparoscopic, with salpingectomy and/or oophorectomy |
Abortion-Related and Other Procedure Codes
| CPT Code | Description |
|---|---|
| 59100 | Hysterotomy, abdominal (e.g., hydatidiform mole, abortion) |
| 59200 | Insertion of cervical dilator (e.g., laminaria, prostaglandin) |
| 59812 | Treatment of incomplete abortion, any trimester, completed surgically |
| 59820 | Treatment of missed abortion, completed surgically, first trimester |
Unlisted Procedure Codes
| CPT Code | Description |
|---|---|
| 59897 | Unlisted fetal invasive procedure, including ultrasound guidance |
| 59898 | Unlisted laparoscopy procedure, maternity care services |
| 59899 | Unlisted procedure, maternity care services |
Modifiers, Bundling, and Billing Rules
Important Modifiers for OB/GYN Billing
| Modifier | Name | When to Use in Maternity Care |
|---|---|---|
| 25 | Significant, separately identifiable E/M service | When an E/M service is performed on the same date as labor management begins or on the same date as admission from another site of service |
| 22 | Increased procedural complexity | For breech vaginal delivery reported with a standard vaginal delivery code |
| 51 | Multiple procedures | When the same provider performs both cesarean delivery and hysterectomy (59504) |
| 76/77 | Repeat procedure | For repeat fetal scalp blood sampling (59030) |
Bundling Rules to Watch
The CPT 2027 guidelines establish clear boundaries between what is and what is not separately reportable:
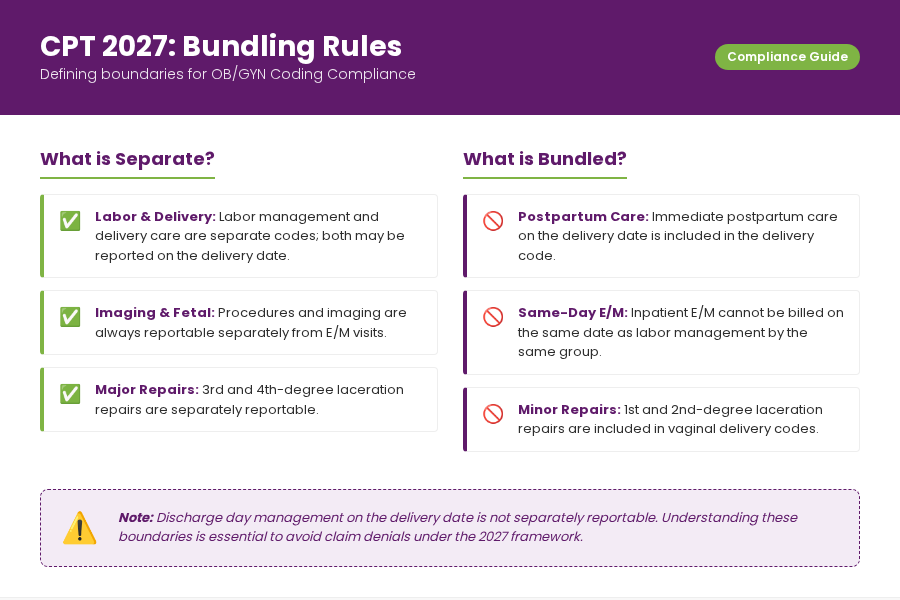
- Labor management is not included in the delivery care. The two are separate codes, and both may be reported on the delivery date when applicable
- Immediate postpartum care on the delivery date is included in delivery care and may not be billed separately
- Inpatient E/M services may not be billed on the same date as labor management codes by the same provider or group
- Discharge day management on the delivery date is not separately reportable
- Imaging and fetal procedures are always separately reportable from E/M visits
- First- and second-degree laceration repair is included in vaginal delivery codes; third- and fourth-degree repairs are separately reportable
Common Coding Mistakes in CPT 2027
As OB/GYN practices transition away from global maternity packages, coding accuracy becomes more important, and small errors can easily result in claim denials.
Errors That Will Trigger Denials
Because CPT 2027 requires phase-based reporting, most denials occur when legacy global logic or bundling misunderstandings are applied.
| Mistake | Why It Is a Problem | Correct Approach |
|---|---|---|
| Using deleted global OB codes (59400, 59510, 59610) | These codes are invalid after Jan 1, 2027 | Report each phase separately with component codes |
| Double-billing labor management and inpatient E/M on the same day | CPT guidelines prohibit same-provider, same-date billing of both | Report only labor management on that calendar date |
| Missing Modifier 25 when needed | Claim for separate E/M on the same date will be bundled and denied | Append Modifier 25 to the E/M code when services are distinct |
| Billing postpartum care on the delivery date | Same-day postpartum is bundled into delivery care | Begin billing postpartum E/M codes from the next calendar date |
| Reporting both 59080 and 59081 on the same date | Only the highest level is reportable per calendar date | Report only the highest level of labor management for that day |
| Using a vaginal delivery code when a cesarean occurs | If vaginal delivery is attempted and a cesarean occurs, only the cesarean is reported | Report only the appropriate cesarean code (59502 or 59503) |
| Billing hysterectomy with cesarean without Modifier 51 | Multiple procedure reduction applies | Use 59504 with Modifier 51 when same provider performs both |
Documentation Gaps That Cause Denials
- Insufficient documentation of labor complexity (straightforward vs. complex) to support the code level selected
- Missing start and stop times for labor management encounters
- No documentation of face-to-face encounter required for labor management codes
- Unclear provider role in multi-provider scenarios (covering, consulting, or attending)
Documentation Requirements for Accurate Coding
Accurate documentation is the foundation of compliant OB/GYN billing under CPT 2027, where each phase of care is reported separately.
What Must Be Documented for Each Phase
| Phase | Required Documentation Elements |
|---|---|
| Antepartum E/M | Medical decision making or total time, problems addressed, data reviewed, risk assessment, and setting of service |
| Labor Management | Complexity level justification, face-to-face encounter confirmation, calendar date, any complications managed, fetal monitoring findings |
| Delivery Care | Time delivery care began, type of delivery, any lacerations and repair level performed, immediate postpartum management |
| Postpartum Care | Assessment findings, ongoing management plan, setting of service, date of service relative to delivery date |
Real-World Coding Scenarios
Scenario 1: Routine Vaginal Delivery
A patient at 39 weeks presents to the hospital in active labor. Her OB manages labor throughout the day. Labor is uncomplicated with singleton vertex presentation and normal fetal monitoring. She delivers vaginally the same day with a first-degree laceration repaired at delivery.
| Service | Code | Notes |
|---|---|---|
| Initial day labor management, straightforward | 59080 | First calendar date, no complications, criteria for initial day met |
| Vaginal delivery | 59431 | Includes laceration repair (first degree) and immediate postpartum care |
| Next-day inpatient postpartum visit | 99231-99233 | Billed on the calendar date after delivery |
Scenario 2: High-Risk Pregnancy with Complications
A patient with hypertension and gestational diabetes is admitted for induction. During labor, she develops preeclampsia and requires additional management. Labor spans two calendar days. Delivery occurs on the second day.
| Service | Code | Notes |
|---|---|---|
| Initial day labor management, complex | 59081 | Hypertension and diabetes requiring additional management during labor |
| Subsequent day labor management, complex | 59083 | Preeclampsia develops; still complex on the delivery date when labor management is also performed |
| Vaginal delivery | 59431 | Delivery code on the date of delivery |
| Postpartum inpatient visits (each subsequent day) | 99231-99233 | Beginning the day after delivery |
Scenario 3: VBAC Attempt Ending in Cesarean
A patient with one prior cesarean presents in labor. She and her provider agree to attempt a VBAC. Labor management is initiated. Labor arrests, and the decision is made to proceed with a repeat cesarean.
| Service | Code | Notes |
|---|---|---|
| Initial day labor management, straightforward or complex | 59080 or 59081 | Depends on clinical complexity; previous cesarean alone makes this complex (59081) |
| Repeat cesarean delivery | 59503 | Report only the cesarean code when a vaginal delivery attempt fails |
| No vaginal delivery code | Do not report 59432 | Vaginal delivery attempt was unsuccessful; cesarean code only |
Scenario 4: Multi-Day Labor Management Case
A patient is admitted for cervical ripening on Day 1. Active labor management continues on Day 2. She delivers on Day 3.
| Day | Code | Rationale |
|---|---|---|
| Day 1 | 59080 or 59081 | Initial day labor management; report the highest level for that date |
| Day 2 | 59082 or 59083 | Subsequent day; not the initial date; report the highest level for Day 2 |
| Day 3 (delivery day) | 59082 or 59083 + 59431 or 59502 | Subsequent labor management (if performed) plus delivery code |
How CPT 2027 Impacts OB/GYN Revenue Cycle
With the elimination of global OB packages, revenue cycle workflows must adapt to a fully component-based billing model that captures every phase of maternity care separately.
Financial Implications of Component-Based Billing
The transition to component-based maternity coding makes it difficult for practices to manage billing manually. Using modern OB GYN EMR software allows providers to document each phase of care accurately, automate charge capture, and maintain compliance with coding guidelines.
At the same time, the documentation burden increases significantly. Billing teams must now account for each calendar date of labor management, each antepartum visit, and each postpartum encounter as an independent claim event.
Workflow Changes for Practices
To support accurate claim generation under CPT 2027, practices must redesign existing billing and clinical workflows.
- Billing systems must be updated to remove deleted global codes and add new labor management codes
- Coding teams need daily tracking of labor management calendar dates to identify initial vs. subsequent day reporting
- Charge capture workflows at the provider level must capture each E/M encounter for antepartum and postpartum care
- Electronic health record templates should be updated to prompt documentation of labor complexity criteria
Best Practices for OB/GYN Billing Teams
To stay compliant and maintain revenue integrity, billing teams must align coding, documentation, and audit processes with the new structure.
Coding Optimization Tips
Accurate coding starts with consistent documentation and correct E/M selection across all care phases. Here are the coding optimization tips that your practice must follow:
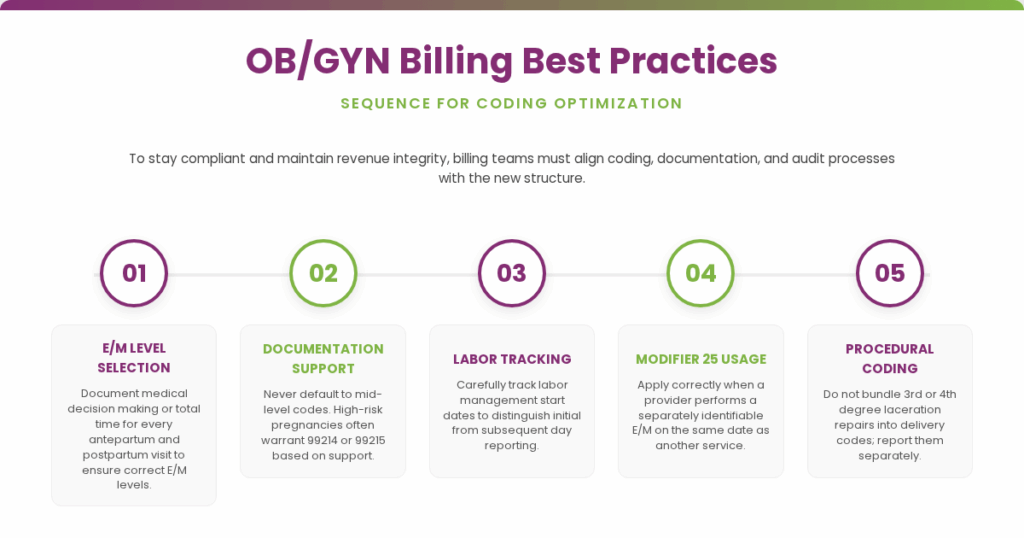
- Use the correct E/M level consistently by documenting medical decision making or total time for every antepartum and postpartum visit
- Never default to a mid-level E/M code without documentation support; high-risk pregnancies often warrant 99214 or 99215
- Track labor management start dates carefully to distinguish initial from subsequent day reporting
- Use Modifier 25 correctly when a provider performs a separately identifiable E/M on the same date as another service
- Do not bundle separately reportable procedures like third- or fourth-degree laceration repair into the delivery code
RCM Strategies to Reduce Denials
Revenue cycle management must become more proactive and audit-driven under the new CPT framework. These structured controls help prevent common billing errors and improve clean claim rates across all maternity care phases:
- Conduct pre-bill audits on all delivery claims to verify that deleted global codes are not appearing
- Implement staff training programs specifically focused on CPT 2027 changes before the January 1, 2027, effective date
- Use specialty-trained OB/GYN coders or hire OB/GYN billing companies who understand the clinical nuances of labor complexity classification
- Build payer-specific edit rules into your billing system to catch same-day conflict combinations before submission.
- Establish a denial tracking workflow to identify patterns related to the new codes and refine submissions accordingly
FAQs on Maternity Care Coding Under CPT 2027
Can You Still Bill Global OB Packages After January 1, 2027?
No, codes 59400, 59510, 59610, and the related global OB codes are deleted effective January 1, 2027. Submitting them will result in claim rejection. All maternity care must be billed in component form using E/M codes, labor management codes, and delivery codes separately.
When Should Labor Management Be Billed?
Labor management is billed on each calendar date the provider performs labor management services for an admitted patient. The first qualifying date uses an initial day code (59080 or 59081). All subsequent dates use subsequent day codes (59082 or 59083). Labor management is not billed when a planned cesarean proceeds without labor.
How do you Code Postpartum Visits?
Postpartum visits are reported with the appropriate E/M code for the setting and date of service. Inpatient visits use hospital E/M codes (99231-99236 or 99238-99239). Outpatient visits use office, telehealth, or home visit codes.
Can Multiple Providers Bill For The Same Patient On The Same Date?
Yes, in some circumstances. A consulting provider who evaluates but does not assume care may report E/M codes, such as inpatient consultation codes or interprofessional telephone or electronic consultation codes. However, providers in the same group practice are treated as a single entity for purposes of labor management and inpatient E/M reporting. Advanced practice nurses and physician assistants working with physicians are considered to be in the exact same specialty.
What Happens When a Continuous Labor Management Encounter Spans Midnight?
A continuous visit requiring continuous personal provider attendance at bedside that spans the transition between two calendar dates is a single service. It is reported once on one of the two calendar dates.
Conclusion
CPT 2027 transforms maternity care coding from a bundled model into a component-based system. Every phase of care now requires accurate, separately documented, and separately billed services.
For OB/GYN billing teams, preparation is essential. The deleted global codes must be removed from billing systems. New labor management codes must be understood and applied correctly. E/M documentation must support each antepartum and postpartum visit independently.
Practices that invest in coder training, documentation improvement, and system updates before January 1, 2027, will be positioned to capture revenue accurately and avoid denials. Those who wait risk claim rejections, compliance exposure, and lost reimbursement. Understanding these changes now gives your team the lead time to prepare, train, and implement before the effective date.