Pain management covers a wide range of acute, chronic, and neuropathic conditions. Low back pain, radiculopathy, complex regional pain syndrome, fibromyalgia, and cancer-related pain each carry distinct coding rules. Each condition maps to a specific ICD-10-CM code, and the wrong code or a missing laterality digit means a denial.
The pain management code set spans two patterns. The G89 category captures pain by type, including acute, chronic, postprocedural, and neoplasm-related pain. Site-specific codes capture pain by anatomical location, such as the M54 spine codes and the M25.5 joint codes.
The scale of the problem explains the billing risks. According to the Centers for Disease Control and Prevention (CDC), an estimated 51.6 million U.S. adults, or 20.9% of the adult population, experienced chronic pain in 2021. Another 17.1 million adults reported high-impact chronic pain that restricted daily activity.
This guide covers the most important pain management ICD-10-CM codes by category. Each section includes the code tables, documentation requirements, sequencing rules, and the denial patterns that drain pain management revenue.
ICD-10-CM Codes for the G89 Pain Category
The G89 category, titled Pain not elsewhere classified, sits at the center of pain management coding. G89 codes capture pain by type rather than by body site. They identify whether pain is acute, chronic, postprocedural, or neoplasm-related.
G89 codes work alongside site-specific pain codes. A coder uses the G89 code to add the acute or chronic detail and the site code to add the location. The sequencing between them depends on the reason for the encounter.
G89 Code Set
The following table presents the billable G89 codes used in pain management billing:
| ICD-10-CM Code | Description |
|---|---|
| G89.0 | Central pain syndrome |
| G89.11 | Acute pain due to trauma |
| G89.12 | Acute post-thoracotomy pain |
| G89.18 | Other acute postprocedural pain |
| G89.21 | Chronic pain due to trauma |
| G89.22 | Chronic post-thoracotomy pain |
| G89.28 | Other chronic postprocedural pain |
| G89.29 | Other chronic pain |
| G89.3 | Neoplasm-related pain (acute) (chronic) |
| G89.4 | Chronic pain syndrome |
The parent codes G89.1 and G89.2 are not billable. Coders select the specific subcode that documents the cause of the acute or chronic pain.
Chronic Pain vs Chronic Pain Syndrome
G89.29 and G89.4 are not interchangeable. This distinction is one of the most common G89 coding errors. The two codes describe different clinical pictures.

- G89.29 (Other chronic pain): persistent pain lasting beyond the expected healing period
- G89.4 (Chronic pain syndrome): chronic pain with documented psychosocial dysfunction
- Documentation rule: G89.4 requires the provider to document the behavioral or functional component
There is no fixed time frame that defines chronic pain in ICD-10-CM. The provider’s documentation guides whether pain is acute or chronic. Code to what the record supports.
ICD-10-CM Codes for Low Back Pain and Sciatica
Low back pain is the highest-volume diagnosis in most pain management practices. ICD-10-CM classifies low back pain under the M54.5 category. The M54.5 parent code became non-billable in October 2021, when three specific subcodes replaced it.
Coders must select among three low back pain codes based on the documented details. Defaulting to the unspecified code when the record supports more detail is a frequent denial trigger.
Low Back Pain Codes (M54.5 Series)
| ICD-10-CM Code | Description | When to Use |
|---|---|---|
| M54.50 | Low back pain, unspecified | No defined cause documented |
| M54.51 | Vertebrogenic low back pain | Vertebral endplate changes, such as Modic changes |
| M54.59 | Other low back pain | Defined pattern not meeting vertebrogenic criteria |
Vertebrogenic low back pain (M54.51) applies when imaging and clinical findings support a vertebral endplate origin. This code captures persistent midline axial pain worsened by sitting or activity.
Sciatica and Lumbago Codes
Sciatica and lumbago with sciatica each require a laterality digit. These codes describe leg pain radiating from the lumbar spine. Bilateral cases require coding both sides separately.
| ICD-10-CM Code | Description |
|---|---|
| M54.30 | Sciatica, unspecified side |
| M54.31 | Sciatica, right side |
| M54.32 | Sciatica, left side |
| M54.40 | Lumbago with sciatica, unspecified side |
| M54.41 | Lumbago with sciatica, right side |
| M54.42 | Lumbago with sciatica, left side |
Excludes1 Rule: When sciatica is caused by a lumbar intervertebral disc disorder, the M51.1 disc code applies instead of M54.4. Coding M54.4 alongside the disc disorder code triggers an edit. A common mistake here is pairing M54.50 or M54.59 with a disc disorder or radiculopathy code that already explains the pain.
ICD-10-CM Codes for Neck and Spine Pain
Neck and upper spine pain form a significant portion of the pain management volume. ICD-10-CM codes these conditions across the M54 dorsalgia range. Each code describes pain at a specific spinal region.
The cervical and thoracic spine codes are site-specific symptom codes. They apply when no underlying structural diagnosis has been confirmed as the cause.
Cervical and Thoracic Pain Codes
| ICD-10-CM Code | Description |
|---|---|
| M54.2 | Cervicalgia (neck pain) |
| M54.6 | Pain in the thoracic spine |
| M54.81 | Occipital neuralgia |
| M54.89 | Other dorsalgia |
| M54.9 | Dorsalgia, unspecified |
Cervicalgia (M54.2) captures neck pain without radicular features. When nerve root involvement is documented, the cervical radiculopathy code (M54.12) applies instead, covered in the next section.
Documentation Note: M54.9 (Dorsalgia, unspecified) carries audit risk when the record supports a specific region. Use M54.9 only when the documentation does not specify the spinal level or pain type.
ICD-10-CM Codes for Radiculopathy
Radiculopathy describes pain from compressed or irritated spinal nerve roots. ICD-10-CM classifies radiculopathy under M54.1, with a fifth digit identifying the spinal region. Pain management practices bill these codes daily for epidural and nerve block indications.
The region digit is mandatory. A radiculopathy code without the correct region fails specificity review and slows reimbursement.
Radiculopathy Codes by Region (M54.1 Series)
| ICD-10-CM Code | Description |
|---|---|
| M54.10 | Radiculopathy, site unspecified |
| M54.11 | Radiculopathy, occipito-atlanto-axial region |
| M54.12 | Radiculopathy, cervical region |
| M54.13 | Radiculopathy, cervicothoracic region |
| M54.14 | Radiculopathy, thoracic region |
| M54.15 | Radiculopathy, thoracolumbar region |
| M54.16 | Radiculopathy, lumbar region |
| M54.17 | Radiculopathy, lumbosacral region |
| M54.18 | Radiculopathy, sacral and sacrococcygeal region |
The Disc Disorder Exclusion
The M54.1 codes carry an Excludes1 note that creates a major coding pitfall. Radiculopathy caused by a disc disorder or spondylosis does not use M54.1. A combination code captures both the structural cause and the radiculopathy.
- Cervical disc disorder with radiculopathy: use M50.1, not M54.12
- Lumbar or other disc disorder with radiculopathy: use M51.1, not M54.16
- Spondylosis with radiculopathy: use M47.2, not M54.1
- Neuralgia and neuritis NOS: routes to M79.2, not M54.1
In practice, the documented cause decides the code. When the record names a disc disorder, the combination code replaces the standalone radiculopathy code.
ICD-10-CM Codes for Joint Pain
Joint pain is a frequent pain management presentation across the shoulder, hip, and knee. ICD-10-CM classifies joint pain under M25.5, with laterality digits for each joint. These codes apply when pain is the finding and no joint disease is confirmed.
Laterality drives the code selection. Payers reject claims when the documented side does not match the submitted code.
Pain in Joint Codes (M25.5 Series)
| ICD-10-CM Code | Description |
|---|---|
| M25.50 | Pain in an unspecified joint |
| M25.511 / M25.512 | Pain in right/left shoulder |
| M25.521 / M25.522 | Pain in right/left elbow |
| M25.551 / M25.552 | Pain in the right/left hip |
| M25.561 / M25.562 | Pain in right/left knee |
| M25.571 / M25.572 | Pain in right/left ankle and foot |
| M25.59 | Pain in other specified joint |
Bilateral Rule: ICD-10-CM has no bilateral joint pain code for most joints. Bilateral knee pain reports both M25.561 and M25.562 as two separate codes. The same rule applies across the M25.5 family.
The joint pain code can pair with a G89 code to add the acute or chronic detail. A patient with chronic right knee pain reports M25.561 with the applicable G89 chronic pain code when the encounter supports both.
ICD-10-CM Codes for Complex Regional Pain Syndrome (CRPS)
Complex regional pain syndrome is a chronic neuropathic pain condition managed heavily in pain clinics. ICD-10-CM separates CRPS into two types with different code families. The type and the affected limb both drive the code.
CRPS type I was formerly called reflex sympathetic dystrophy (RSD). CRPS type II was formerly called causalgia and involves a confirmed nerve injury. The two types are mutually exclusive for the same limb.
CRPS Type I Codes (G90.5 Series)
| ICD-10-CM Code | Description |
|---|---|
| G90.50 | CRPS I, unspecified |
| G90.511 / G90.512 | CRPS I of right/left upper limb |
| G90.513 / G90.519 | CRPS I of upper limb, bilateral/unspecified |
| G90.521 / G90.522 | CRPS I of right/left lower limb |
| G90.523 / G90.529 | CRPS I of lower limb, bilateral/unspecified |
| G90.59 | CRPS I of other specified site |
CRPS Type II Codes (Causalgia)
CRPS type II, or causalgia, routes to the mononeuropathy codes. The fifth digit identifies laterality, matching the right, left, bilateral, and unspecified patterns.
- G56.4- Causalgia (CRPS II) of upper limb
- G57.7- Causalgia (CRPS II) of the lower limb
Excludes1 Rule: CRPS I (G90.5-) and CRPS II (G56.4-, G57.7-) carry an Excludes1 relationship. The two codes never report together for the same limb. The provider’s documentation of nerve injury status decides which type applies.
ICD-10-CM Codes for Neuropathic Pain and Neuralgia
Neuropathic pain arises from nerve damage or dysfunction. Pain management practices code these conditions across several ICD-10-CM chapters. The codes span nerve disorders, postherpetic conditions, and diabetic neuropathy.
The correct code depends on the documented nerve and cause. Generic neuralgia codes apply only when the specific nerve or cause is not identified.
Common Neuropathic Pain Codes
| ICD-10-CM Code | Description |
|---|---|
| M79.2 | Neuralgia and neuritis, unspecified |
| G50.0 | Trigeminal neuralgia |
| G58.0 | Intercostal neuropathy |
| B02.22 | Postherpetic trigeminal neuralgia |
| B02.23 | Postherpetic polyneuropathy |
| B02.29 | Other postherpetic nervous system involvement |
| G54.6 | Phantom limb syndrome with pain |
Diabetic Neuropathy Codes
Diabetic neuropathy is a combination code that binds the diabetes type to the nerve complication. Type 2 diabetes uses the E11.4 subcategory. The neuropathy type drives the fifth digit.
| ICD-10-CM Code | Description |
|---|---|
| E11.40 | Type 2 diabetes with diabetic neuropathy, unspecified |
| E11.41 | Type 2 diabetes with diabetic mononeuropathy |
| E11.42 | Type 2 diabetes with diabetic polyneuropathy |
| E11.43 | Type 2 diabetes with diabetic autonomic (poly)neuropathy |
| E11.49 | Type 2 diabetes with other diabetic neuropathy |
Coding Note: M79.2 is a last-resort code. Its Excludes1 note routes radiculitis to M54.1, sciatica to M54.3 and M54.4, and mononeuropathies to the G56 through G58 range. Query the provider before defaulting to M79.2.
ICD-10-CM Codes for Fibromyalgia and Myalgia
Fibromyalgia and myalgia are muscle-based pain diagnoses common in pain management. ICD-10-CM classifies them under the M79 soft tissue range. Fibromyalgia carries its own dedicated code.
These codes apply to muscle pain without a confirmed inflammatory or structural cause. Documentation of the affected region adds specificity to the myalgia codes.
Fibromyalgia and Myalgia Codes
| ICD-10-CM Code | Description |
|---|---|
| M79.7 | Fibromyalgia |
| M79.10 | Myalgia, unspecified site |
| M79.11 | Myalgia of the mastication muscle |
| M79.12 | Myalgia of auxiliary muscles, head, and neck |
| M79.18 | Myalgia, other site |
Fibromyalgia (M79.7) is a single billable code with no laterality or subcode. It captures widespread musculoskeletal pain with tenderness. The diagnosis rests on the provider’s clinical assessment.
Documentation Note: Myalgia codes are symptom codes. When a confirmed inflammatory myopathy or other definitive diagnosis exists, the disease code replaces the myalgia code.
ICD-10-CM Codes for Headache and Facial Pain
Headache and facial pain disorders appear across pain management and neurology billing. ICD-10-CM splits these conditions into headache syndromes, migraines, and facial nerve pain. The G44 and G43 ranges carry detailed subcodes.
Headache codes require attention to chronicity and intractability. Migraine codes add status migrainosus and intractable modifiers in the final digits.
Headache and Facial Pain Codes
| ICD-10-CM Code | Description |
|---|---|
| R51.9 | Headache, unspecified |
| G44.209 | Tension-type headache, unspecified, not intractable |
| G43.909 | Migraine, unspecified, not intractable, without status migrainosus |
| G44.1 | Vascular headache, not elsewhere classified |
| G50.0 | Trigeminal neuralgia |
| G50.1 | Atypical facial pain |
| M54.81 | Occipital neuralgia |
Sequencing Note: R51.9 is a symptom code for undifferentiated headache. When the provider documents a migraine or tension-type headache, the specific G43 or G44 code replaces R51.9. Headache syndromes route out of the G89 category per the Excludes2 notes.
ICD-10-CM Codes for Postoperative and Cancer-Related Pain
Postoperative and cancer-related pain require careful G89 coding. The distinction between expected pain and complication-related pain changes the code set. Cancer pain carries its own dedicated code.
These scenarios separate routine pain from pain tied to a documented complication. The documentation language decides the path.
Postoperative and Cancer Pain Codes
| ICD-10-CM Code | Description | When to Use |
|---|---|---|
| G89.18 | Other acute postprocedural pain | Expected acute pain after a procedure |
| G89.28 | Other chronic postprocedural pain | Persistent pain after a procedure |
| G89.3 | Neoplasm-related pain | Pain related to a primary or secondary malignancy |
Postoperative Pain Rules
Routine postoperative pain is normal and expected after surgery. It codes to G89.18 for acute pain or G89.28 for chronic pain. The rules change when a complication causes the pain.
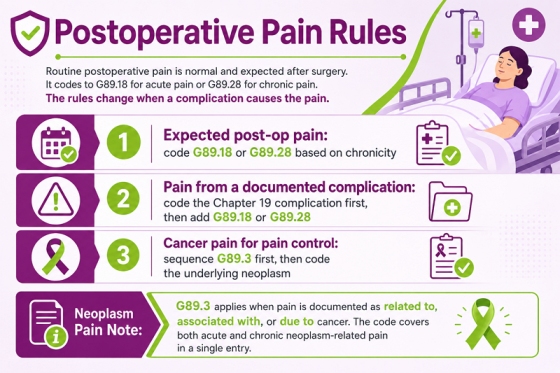
- Expected post-op pain: code G89.18 or G89.28 based on chronicity
- Pain from a documented complication: code the Chapter 19 complication first, then add G89.18 or G89.28
- Cancer pain for pain control: sequence G89.3 first, then code the underlying neoplasm
Neoplasm Pain Note: G89.3 applies when pain is documented as related to, associated with, or due to cancer. The code covers both acute and chronic neoplasm-related pain in a single entry.
ICD-10-CM Codes for Limb, Pelvic, and Other Regional Pain
Pain management practices code limb, pelvic, and regional pain across several ICD-10-CM ranges. These site-specific codes apply when pain is the presenting finding. The location and laterality drive the selection.
The limb pain codes use the M79.6 range with digits for each limb segment. Pelvic and coccyx pain routes to their own codes.
Regional Pain Codes
| ICD-10-CM Code | Description |
|---|---|
| M79.601 / M79.602 | Pain in right/left arm |
| M79.604 / M79.605 | Pain in the right/left leg |
| M79.609 | Pain in an unspecified limb |
| R10.2 | Pelvic and perineal pain |
| M53.3 | Sacrococcygeal disorders (coccydynia) |
| R52 | Pain, unspecified |
R52 Caution: R52 (Pain, unspecified) is a broad symptom code. Use it only when neither the site nor the type of pain is documented. Repeated R52 use across a patient’s claims history raises audit exposure.
The M79.6 limb codes extend to specific segments, including the upper arm, forearm, thigh, and lower leg. Code to the most specific limb segment the documentation supports.
Which G89 Sequencing Rules Every Pain Management Coder Must Know?
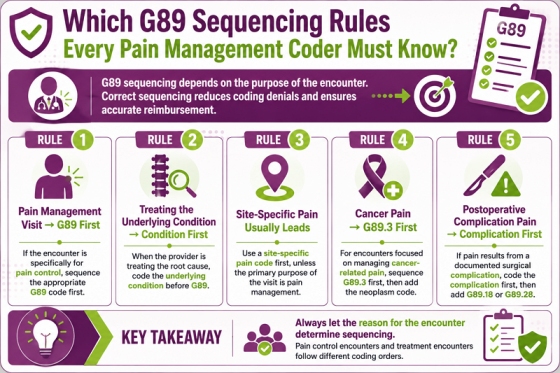
G89 sequencing drives more pain management denials than any other rule. The ICD-10-CM Official Guidelines, Section I.C.6, govern when a G89 code is sequenced first. The reason for the encounter decides the order.
These rules separate a pain control encounter from an encounter to treat the underlying condition. Applying them correctly prevents the most common sequencing denials. For guidance on applying these rules across a full pain management workflow, read this pain management billing guide.
Rule 1: Pain Control Encounters Sequence G89 First
When the encounter is specifically for pain management, the G89 code is sequenced first. The provider is treating the pain, not the condition causing it. A spinal injection visit for pain control lists the G89 code first.
Rule 2: Treating the Underlying Condition Drops G89 from First Position
When the encounter treats the underlying condition, that condition is sequenced first. A kyphoplasty for a vertebral fracture lists the fracture, not the pain. The G89 code is not first-listed in this scenario.
Rule 3: Site Code First Unless the Visit Is for Pain Management
A G89 code can pair with a site-specific pain code to add the acute or chronic detail. The site code is sequenced first unless the purpose is pain management. When pain control is the purpose, the G89 code leads.
Rule 4: Neoplasm Pain Sequences G89.3 First for Pain Control
When the encounter manages cancer pain, G89.3 is the first-listed diagnosis. The neoplasm code is also reported to identify the malignancy. The pain control intent drives the G89.3 sequencing.
Rule 5: Postoperative Complication Pain Codes the Complication First
Pain from a specific postoperative complication codes the Chapter 19 complication first. The G89.18 or G89.28 code is added to identify the acute or chronic pain. Routine post-op pain does not follow this rule.
What are the Common Pain Management ICD-10 Coding Errors and How to Avoid Them?
Pain management claims face a recurring set of coding errors. The table below identifies the most frequent errors and the corrections that prevent them:
| Coding Error | Correct Approach |
|---|---|
| Using M54.50 when the record supports M54.51 or M54.59 | Code the documented detail; reserve M54.50 for undocumented cause |
| Pairing M54.16 radiculopathy with a disc disorder code | Use the M50.1 or M51.1 combination code instead |
| Coding G89.4 for routine chronic pain | Use G89.29 unless psychosocial dysfunction is documented |
| Sequencing the underlying condition first on a pain control visit | Sequence the G89 code first when the visit is for pain management |
| Using unspecified laterality for joint pain (M25.50) | Code the documented side; report bilateral as two codes |
| Reporting CRPS I and CRPS II for the same limb | Code one type per limb per the Excludes1 rule |
| Defaulting to M79.2 for radiculitis or sciatica | Route to M54.1, M54.3, or M54.4 per the Excludes1 note |
| Overusing R52 for site-documented pain | Code the specific site and type when documented |
Why Does Pain Management Billing Demand Precise ICD-10 Coding?
Accurate coding is the foundation of pain management reimbursement. Many practices struggle to keep themselves updated with code changes, payer rules, and documentation standards. This is why many providers partner with specialized pain management billing services to reduce denials and improve collections.
Procedure-Driven Medical Necessity
Pain management is a procedure-heavy specialty. Epidural injections, facet blocks, radiofrequency ablation, and nerve blocks each require a supporting diagnosis. The ICD-10 code establishes the medical necessity for every procedure billed.
- Spinal injection claims require the matching radiculopathy or pain code
- Joint injection claims require the documented joint and laterality
- Nerve block claims require a specific neuropathic pain diagnosis
Sequencing and Combination Rules
Pain management coding relies on G89 sequencing and combination codes. The G89 code may lead or follow the site code based on the encounter. Disc-related radiculopathy uses a combination code rather than two separate codes. Missing these rules creates the denials that disturb pain management revenue.
Laterality and Specificity Requirements
ICD-10-CM requires laterality for joint pain, CRPS, sciatica, and lumbago with sciatica. A claim submitted with an unspecified laterality code when the record documents the side is a coding error. Payers flag repeated unspecified codes for audit.
Coders must pull the documented side and region from the clinical note and match the exact code. Because a single documentation gap can trigger denials, many practices look to external experts. Specialized pain management billing companies manage these laterality, sequencing, and combination rules natively.