
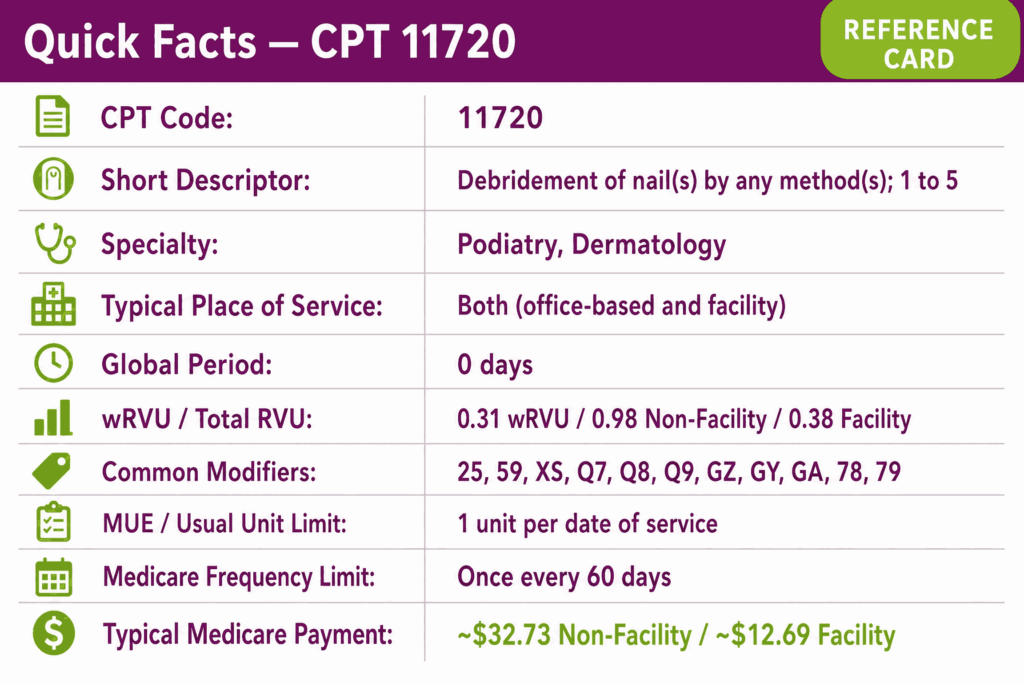
CPT code 11720 reports debridement of one to five nails by any method in a single encounter. It is used when a qualified provider removes thickened, dystrophic, mycotic, or otherwise pathologically altered nail tissue from up to five nails as a medically necessary procedure.
The podiatry code 11720 is used primarily in podiatry, dermatology, and primary care office settings and is subject to strict Medicare coverage criteria, class findings modifier requirements, and frequency restrictions under routine foot care policy. Those coverage criteria make 11720 one of the most denial-sensitive codes in foot care, which is why many groups route it through specialized podiatry billing services.
What Is the Description of CPT Code 11720?
11720 CPT code description as defined by the AMA is: “Debridement of nail(s) by any method(s); 1 to 5.”
This code captures the complete service of debriding between one and five nails, by any method, during a single patient encounter. The “any method” designation includes mechanical reduction, filing, grinding, trimming, or instrumented removal of pathological nail tissue.
Nail debridement code 11720 does not capture nail avulsion, nail matrix destruction, or excision of the nail plate, which are reported under separate codes. The nail count covered by CPT 11720 is 1 to 5. Once six or more nails are debrided in the same session, the CPT 11721 code is the correct code.
What Methods of Nail Debridement Are Covered Under CPT Code 11720?
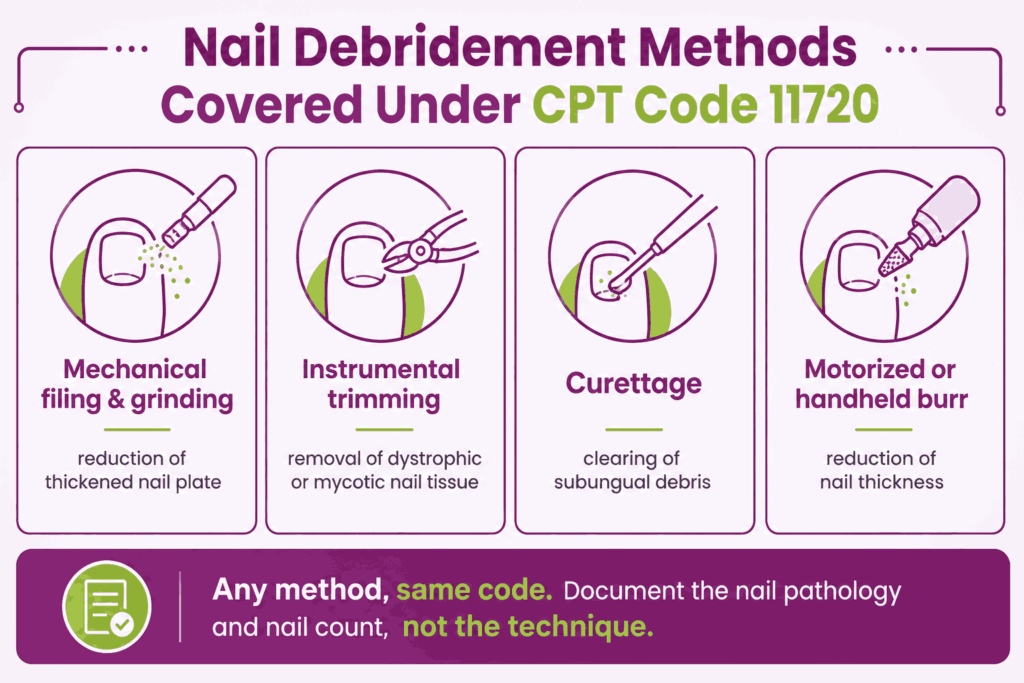
CPT 11720 code applies to debridement by any method, and the descriptor is intentionally broad. Covered techniques include mechanical filing and grinding of thickened nail plate, instrumental trimming and reduction of dystrophic or mycotic nails, curettage of subungual debris, and use of motorized or handheld burrs to reduce nail thickness.
The method does not need to be specified in the procedure note beyond a general description of the debridement performed. What matters clinically and for documentation is the pathological state of the nail, the number of nails treated, and the medical necessity connecting the debridement to the patient’s systemic condition or qualifying diagnosis.
How Does CPT Code 11720 Differ From CPT 11721 and G0127?
The three codes differ by nail count and provider type. The code CPT 11720 covers the debridement of 1 to 5 nails by any method. CPT 11721 covers the debridement of 6 or more nails by any method in the same session. The two codes are mutually exclusive. Procedure codes 11720 and 11721 cannot be billed together on the same date of service. The total number of nails debrided across both feet in a single encounter determines which code applies.
HCPCS code G0127 describes trimming of dystrophic nails performed by a qualified non-physician practitioner. G0127 is a Medicare-specific code that captures the same clinical service as 11720/11721 when performed outside the physician billing context.
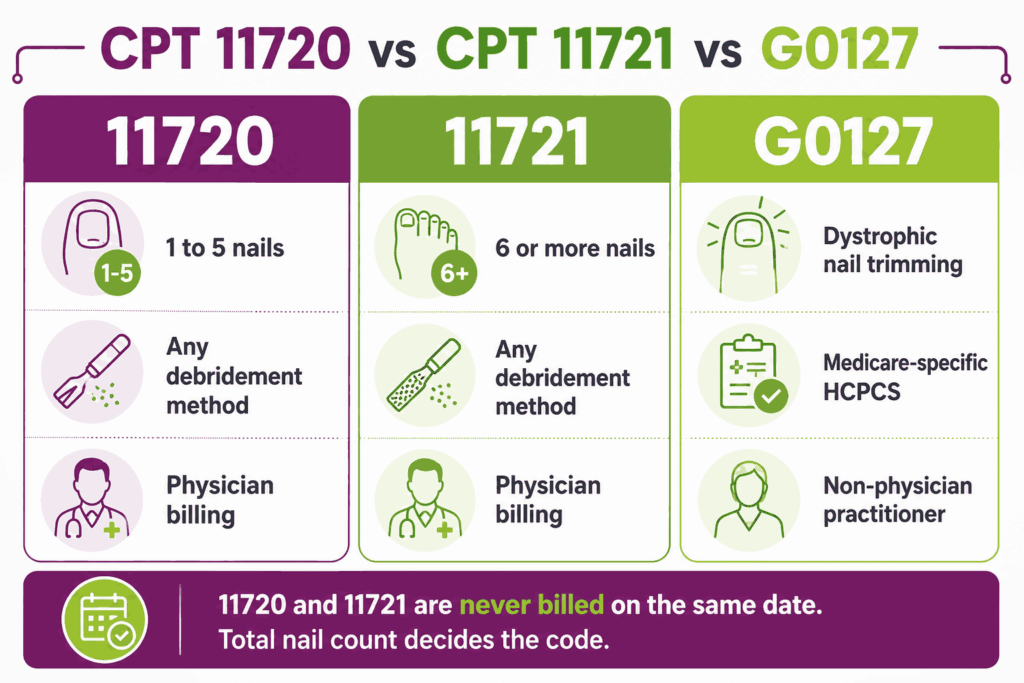
G0127 carries its own RVU valuation and is subject to the same Q modifier and frequency requirements as 11720 and 11721. Physicians typically bill 11720 or 11721. Non-physician practitioners without independent billing authority for 11720/11721 may use G0127 in applicable circumstances. All three codes belong to the wider catalog of podiatry CPT codes spanning routine, surgical, and Medicare-specific foot care reporting.
What Are the Modifiers for CPT Code 11720?
11720 CPT code is reported with several modifiers that are critical for Medicare coverage and claim processing. The class findings modifiers (Q7, Q8, Q9) are unique to routine foot care codes and are among the most denial-sensitive elements in podiatry billing.
Modifier 25: Significant, Separately Identifiable E/M on Same Day
Modifier 25 is appended to the E/M code, not to 11720, when a significant and separately identifiable evaluation and management service is performed on the same date as nail debridement. Per CMS Billing and Coding Article A57759, global surgery rules apply to routine foot care codes, including 11720, meaning an E/M billed on the same day without modifier 25 will not be reimbursed. The E/M must address a problem distinct from the decision to perform the debridement, and documentation must clearly reflect this separate clinical service.
Modifier 59: Distinct Procedural Service
Modifier 59 is used when code CPT 11720 is performed as a distinct service from another procedure billed on the same date, where NCCI bundling edits would otherwise apply. Apply only when documentation confirms the services were separate in clinical purpose or anatomical site. Do not use modifier 59 as a routine unbundling tool.
Modifier XS: Separate Structure
Modifier XS is used when nail debridement is performed on a separate anatomical structure from another same-day service. Where payers accept X-modifiers, XS is preferred over modifier 59 as a more specific indicator of a distinct anatomical site.
Modifier Q7: One Class A Finding (Systemic Condition Qualifier)
Modifier Q7 is appended to podiatry code 11720 when one Class A finding is documented in the medical record on the date of service. Per CMS Article A57759, Class A findings include: nontraumatic amputation of a foot or integral skeletal part thereof. Q7 is the least frequently applicable of the three class finding modifiers, given the specificity of the Class A criterion.
Modifier Q8: Two Class B Findings (Systemic Condition Qualifier)
Modifier Q8 is appended to 11720 CPT when two Class B findings are documented. Class B findings include: absent posterior tibial pulse, absent dorsalis pedis pulse, and advanced trophic changes (three of the following: hair growth changes, nail changes, pigmentary changes, skin texture changes, or skin color changes). Q8 is the most commonly used class finding modifier for nail debridement claims, as absent pedal pulses are a common documented finding in patients with peripheral vascular disease and diabetes.
Modifier Q9: One Class B and Two Class C Findings (Systemic Condition Qualifier)
Modifier Q9 is appended to the CPT 11720 code when one Class B finding and two Class C findings are documented. Class C findings include: claudication, temperature changes in the foot (cold feet), edema, paresthesias, and burning. Q9 applies when the patient’s vascular compromise does not fully meet the two-Class-B threshold but shows a combination of Class B and Class C findings meeting the Q9 threshold.
Modifier GZ: Item or Service Expected to Be Denied as Not Medically Necessary
Modifier GZ is used when the provider expects Medicare to deny debridement CPT 11720 as not medically necessary, and no Advance Beneficiary Notice (ABN) has been obtained. Claims submitted with GZ are automatically denied. The patient cannot be billed when GZ is used without an ABN.
Modifier GY: Statutorily Non-Covered Service
Modifier GY is used when CPT 11720 is performed as a routine foot care service that is statutorily excluded from Medicare coverage, meaning no qualifying systemic condition or class finding is present. Claims with GY are automatically denied and the limitation of liability provision does not apply.
Modifier GA: Waiver of Liability Statement on File
Modifier GA is used when the provider expects Medicare to deny CPT 11720 as not medically necessary, but has obtained a signed ABN from the patient prior to the service. Modifier GA protects the provider’s right to bill the patient if denied. Confirm the ABN was signed before the date of service.
Modifier 78: Unplanned Return to Operating Room During Global Period
Modifier 78 applies when the provider returns to a procedure room or operating setting during the global period of CPT 11720 to address a complication related to the original debridement. Given the 000-day global period for this code, modifier 78 is rarely applicable but remains a billing option when a same-day return to a procedure setting occurs for a complication.
Modifier 79: Unrelated Procedure During Global Period
Modifier 79 is used when an unrelated procedure is performed by the same provider during the global period of CPT 11720. Again, because 11720 carries a 000-day global period, modifier 79 has limited practical application for this code but applies under standard global surgery billing rules.
Why Medicare Class Finding Modifiers (Q7, Q8, Q9) Are Critical for CPT Code 11720
Medicare classifies routine foot care, including nail debridement, as a statutory exclusion under the Social Security Act. Coverage is an exception, not the default, and it is triggered only by the presence of documented systemic disease and qualifying physical findings meeting the class finding threshold.
Per CMS Billing and Coding Article A57759, one of the Q modifiers must be present on every CPT 11720 code claim when coverage is based on a qualifying systemic condition. This is except when coverage is based solely on peripheral neuropathy without vascular impairment. In which case, class finding modifiers are not required, but the neuropathy must still be documented and meet LCD severity criteria.
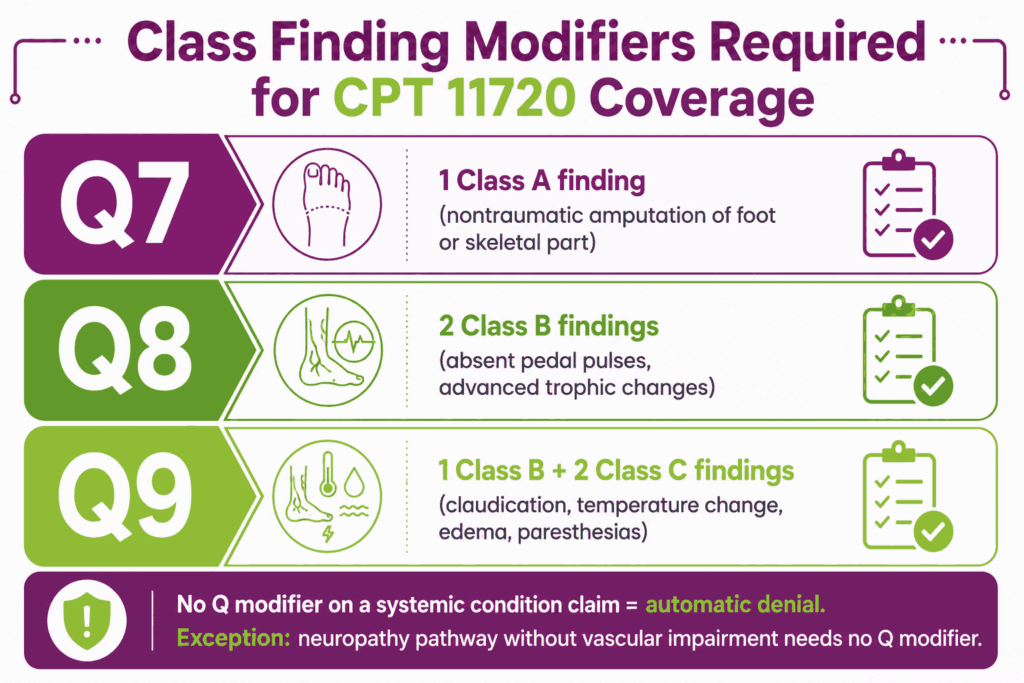
Claims submitted without the appropriate Q modifier when coverage depends on a systemic condition will be automatically denied as routine foot care. This is the most common and costly denial trigger for CPT 11720 claims.
Which Documents Are Required For CPT Code 11720?
Documentation for CPT 11720 must establish medical necessity, identify the qualifying systemic condition and class findings, and confirm the number of nails debrided.
Required documents checklist:
- Active diagnosis confirming the qualifying systemic condition (e.g., diabetes, peripheral vascular disease, chronic thrombophlebitis, or other Group 1 diagnosis per LCD L33941)
- Physical examination findings documenting the specific class findings present (Class A, B, or C) that support the Q modifier appended to the claim
- Notation that failure to perform professional nail care would be hazardous to the patient, given the underlying condition, language required by CMS A57759
- For neuropathy pathway: documentation of the severity of peripheral neuropathy, including examination findings confirming loss of protective sensation
- Number of nails debrided (1–5 for 11720) with identification of the affected foot and specific digits where applicable
- Description of the nail pathology treated (dystrophic, mycotic, thickened, etc.)
- Date of last nail debridement service if within the 60-day frequency window
- For mycotic nails: primary ICD-10 diagnosis of dermatophytosis plus secondary diagnosis of systemic condition
- Signed ABN if coverage is uncertain
- Provider signature with date and time of service
- Accurate place-of-service designation (POS 11 is most common; see full POS list per CMS Article A57193)
What Is the Cost of CPT Code 11720?
The cost of CPT code 11720 varies by place of service, payer, and geographic location.
RVUs & Medicare Payment
The following figures are sourced from the CMS 2026 National Physician Fee Schedule Relative Value File, as reported by FastRVU (last verified May 1, 2026):
| Component | Non-Facility | Facility |
|---|---|---|
| Work RVU | 0.31 | 0.31 |
| PE RVU | 0.64 | 0.04 |
| MP RVU | 0.03 | 0.03 |
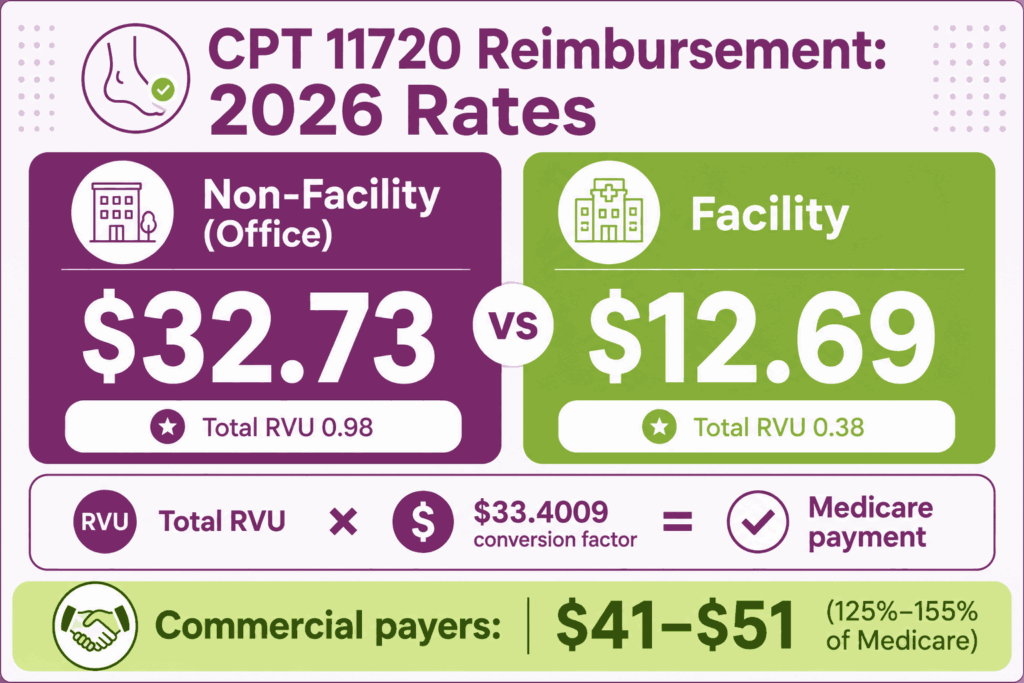
| Total RVU | 0.98 | 0.38 |
| Medicare Payment | $32.73 | $12.69 |
Payment = Total RVU × Conversion Factor ($33.4009).
GPCI adjustments not applied to these national averages. Code CPT 11720 carries a 000-day global period (minor procedure), meaning postoperative care on subsequent dates is not included in the procedure payment and must be billed separately.
Commercial Payers
Commercial health insurance plans generally price CPT 11720 at a premium over Medicare, typically negotiating fee schedules between 125% and 155% of the federal baseline. This positions average commercial allowable amounts for an office-based procedure between $41 and $51.
Place-of-Service & Geographic Adjustments
The final allowable amount for 11720 is modified regionally by the Geographic Practice Cost Index (GPCI). Non-facility (office) payment at $32.73 is substantially higher than the facility payment of $12.69, reflecting the practice expense differential. The non-facility PE RVU is 0.64 versus 0.04 in the facility setting.
This gap is among the most pronounced of any podiatry-related code on a percentage basis, making office-based billing the appropriate and significantly more remunerative setting for this procedure when clinically appropriate. Per CMS Article A57193, CPT 11720 is payable under Medicare across multiple places of service, including office (11), home (12), assisted living (13), urgent care (20), inpatient hospital (21), hospital outpatient (22), SNF (31/32), and others.
What Are Example Clinical Scenarios or Use Cases for CPT Code 11720?
CPT code 11720 applies in podiatry, dermatology, and primary care encounters where 1 to 5 nails are debrided as a medically necessary procedure in a patient with a qualifying systemic condition or documented neuropathy.
Scenario 1: Single Dystrophic Toenail Debridement in a Patient With Type 2 Diabetes
ICD-10: E11.621 (Type 2 diabetes mellitus with foot ulcer) / B35.1 (Tinea unguium — if mycotic)
A patient with Type 2 diabetes presents with a single severely thickened and dystrophic great toenail with subungual debris and periungual erythema. The podiatrist performs mechanical debridement of the nail plate using an electric burr and curette. Two Class B findings are documented: absent dorsalis pedis pulse and advanced trophic changes, including thin, shiny skin and nail thickening bilaterally. CPT 11720 is reported with modifier Q8. The mycotic nail diagnosis is listed as primary with the diabetes code as secondary.
Scenario 2: Two to Three Fungally Infected Nails in a Patient With Peripheral Vascular Disease
ICD-10: I73.9 (Peripheral vascular disease, unspecified) / B35.1 (Tinea unguium)
A patient with documented peripheral vascular disease presents with three fungally infected toenails on the right foot, second, third, and fourth toes, with significant onychomycotic nail plate thickening and discoloration. The podiatrist debrides all three nails. Physical examination documents one Class B finding (absent posterior tibial pulse, right) and two Class C findings (cold temperature change, right foot; paresthesias reported by patient). CPT 11720 is reported with modifier Q9. The visit note explicitly states that failure to perform professional nail care would be hazardous given the patient’s vascular status.
Scenario 3: Post-Traumatic Nail Debridement in a Patient With Limited Mobility and Neuropathy
ICD-10: E11.40 (Type 2 diabetes mellitus with diabetic neuropathy, unspecified)
An elderly patient with diabetes and documented peripheral neuropathy presents with two post-traumatic thickened toenails on the left foot resulting from repeated microtrauma due to foot deformity and altered gait. The podiatrist performs mechanical debridement of both nails. The patient has confirmed peripheral neuropathy of sufficient severity per monofilament testing, documented in the visit note, without vascular impairment. Because coverage is based on neuropathy without vascular impairment, class finding modifiers Q7, Q8, and Q9 are not required. CPT 11720 is reported with the neuropathy pathway supported by detailed physical examination documentation.
What Are the CPT Code 11720 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for documentation, coding, modifier usage, frequency, and Medicare’s routine foot care exception criteria. Meeting these rules is the single most important factor in reducing denials for this code.
Bundling / NCCI / Same-Day Procedure Rules
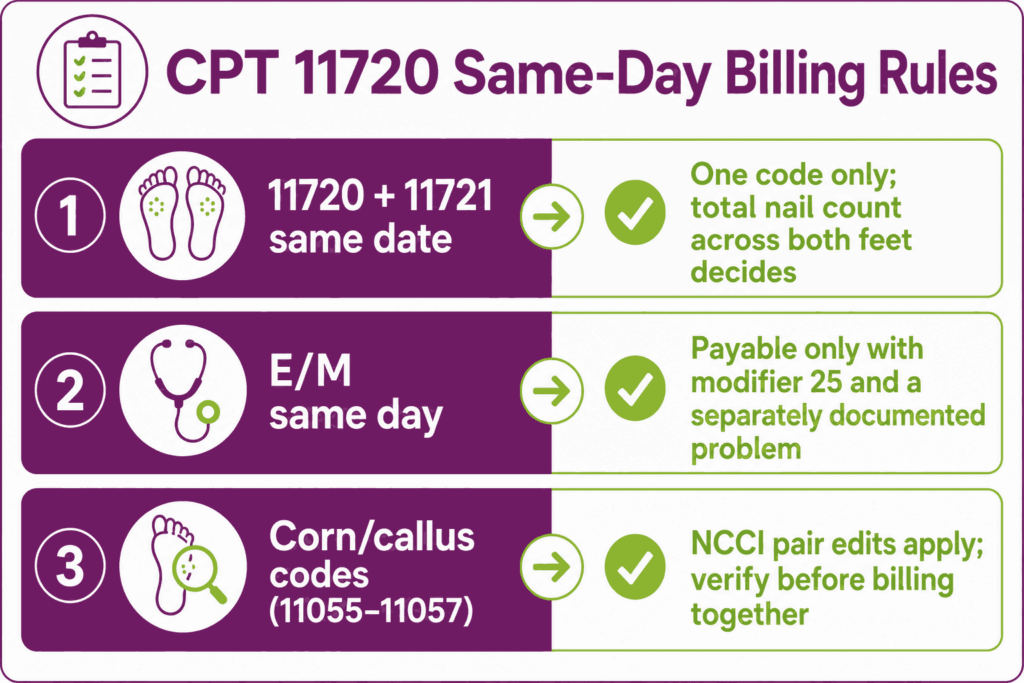
Nail debridement CPT 11720 and CPT 11721 cannot be billed on the same date of service. The nail count across both feet in one encounter is totaled to determine which code applies. If the total is 5 or fewer, use 11720; if 6 or more, use 11721 only. Billing both on the same claim will result in automatic denial of one.
When CPT 11720 is billed on the same date as a corn or callus care code (11055, 11056, 11057), NCCI pair edit relationships apply. Per global surgery rules per CMS Article A57759, an E/M service billed the same day as 11720 is not separately payable unless modifier 25 is appended to the E/M and the documentation clearly reflects a significant, separately identifiable clinical decision beyond the decision to debride nails.
Units, MUEs & Medicare 60-Day Frequency Restrictions
Per CMS Billing and Coding Article A57193, CPT 11720 is billed as 1 unit per date of service, regardless of the number of nails treated. Billing multiple units of 11720 on the same date will be denied. The MUE is 1 unit per date of service.
Medicare’s frequency restriction for routine foot care procedures, including CPT 11720, is once per 60 days. Services billed within 60 days of a prior claim for the same or related routine foot care code will be denied unless documented medical necessity justifies an exception. Verify the date of last service before submitting.
- Document the date of the last nail debridement in the visit note when rebilling within or near the 60-day window
- Some MACs enforce stricter frequency limits at the local level. Verify the applicable LCD and billing article for your MAC before submitting
Unit limits like these are payer rules layered on top of the base CPT code definition, not part of the descriptor itself.
Medicare Routine Foot Care Exclusions and How to Establish Medical Necessity
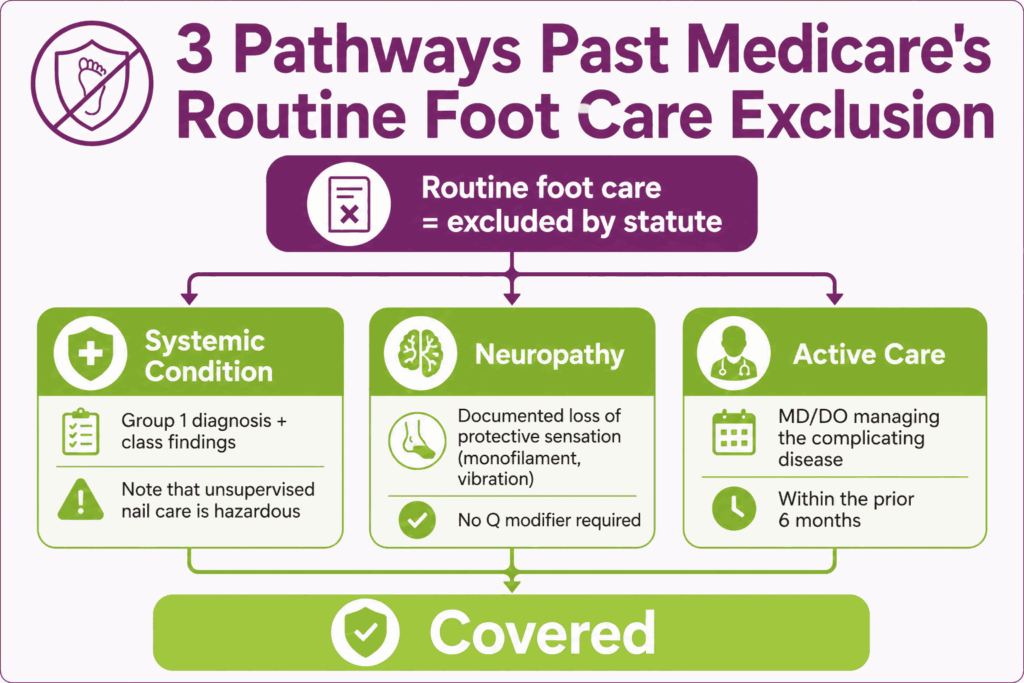
Medicare’s statutory exclusion for routine foot care is the central compliance risk for CPT 11720. The exclusion is overcome only by documenting one of the following pathways, each with specific requirements per CMS LCD L33941 and Billing Article A57759:
Systemic Condition Pathway
The patient must have an active diagnosis from Group 1 of the LCD (diabetes, peripheral vascular disease, arteriosclerosis, chronic thrombophlebitis, Buerger’s disease, etc.) AND documented class findings (Class A, B, or C) meeting the Q7, Q8, or Q9 threshold. The provider must also document that failure to perform professional nail care would be hazardous to the patient’s health, given the underlying condition. Vague language, such as “poor circulation,” is insufficient. Specific findings must be documented.
Neuropathy Pathway
Coverage is available for patients with peripheral neuropathy involving the feet without vascular impairment when the neuropathy is of sufficient severity. Specific neuropathy findings must be documented. Monofilament testing results, vibration testing, or pin-prick findings. Class finding modifiers are not required under this pathway, but neuropathy documentation must be detailed and meet LCD criteria.
Active Care Requirement
For certain systemic conditions, the patient must be under the active care of an MD or DO for the complicating disease during the six-month period prior to the nail care service. Document the name and specialty of the treating physician and the date of the last relevant visit when applicable.
Top Reasons For Denials Specific To 11720 & Quick Remedies
- Missing Q Modifier (Most Common Denial): Prevent by building a pre-submission check that flags every 11720 claim for a Q modifier before it is transmitted. No Q modifier on a systemic condition pathway claim means automatic routine foot care exclusion denial.
- Wrong Q Modifier for Documented Findings: Prevent by mapping documented physical examination findings to the correct class finding threshold before appending the modifier. Q8 requires two distinct Class B findings. Documenting only one pulse absence does not meet the threshold. Train providers to document findings explicitly and bilaterally.
- Frequency Denial (Billed Within 60 Days): Prevent by checking the date of the last same-code or related claim before submission. Mark visit notes with the prior service date and ensure the 60-day window has passed.
- 11720 and 11721 Billed Same Date: Prevent by confirming only one nail debridement code is on the claim per date of service. Total the nail count and select the applicable code. 11720 for 1–5 nails, 11721 for 6 or more.






