
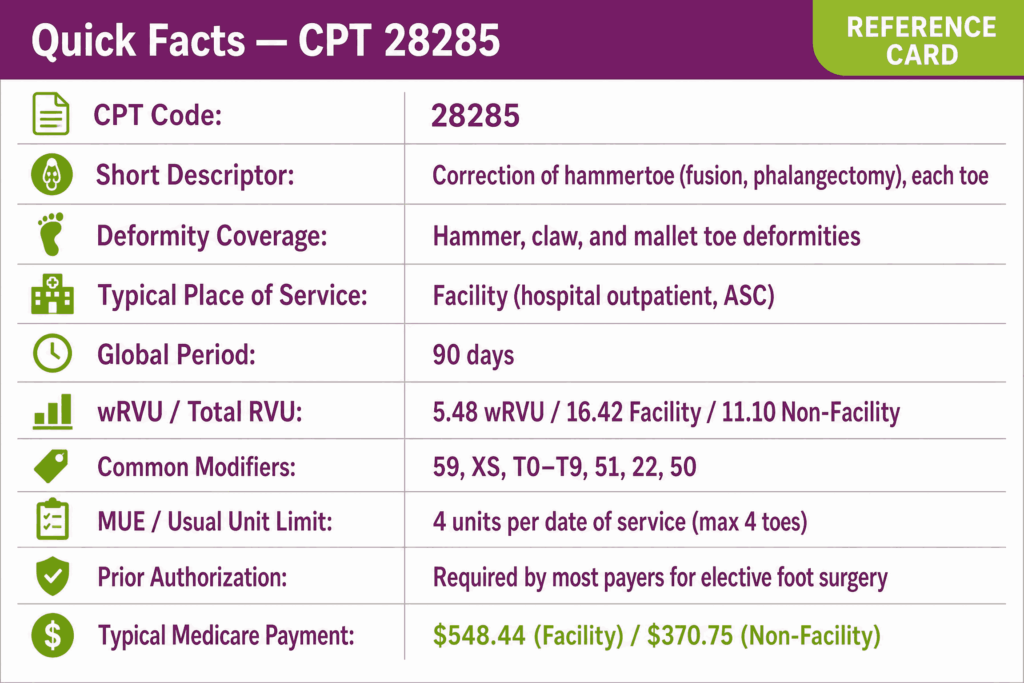
CPT code 28285 is a surgical procedure code used to report correction of hammertoe deformity, which may include interphalangeal joint fusion, partial or total phalangectomy, and related soft-tissue procedures performed on a single lesser toe. Procedure code 28285 is performed in facility settings and covers a range of surgical techniques used to correct rigid or semi-rigid lesser toe deformities when conservative management has failed.
Code 28285 CPT carries a 90-day global period covering all routine postoperative care from the day before surgery through 90 days following the procedure. Prior authorization, facility billing, and multi-toe modifier rules make 28285 a high-denial surgical code best handled by experienced podiatry medical billing services.
What Is the Description of CPT Code 28285?
28285 CPT code description as defined by the AMA is: “Correction, hammertoe (eg, interphalangeal fusion, partial or total phalangectomy).”
The parenthetical descriptor lists examples of covered techniques, such as interphalangeal fusion and phalangectomy, but does not limit the 28285 podiatry CPT code to these approaches only. Any surgical technique used to correct hammertoe, claw toe, or mallet toe deformity of a lesser digit is captured under procedure code 28285 when performed on a single toe.
What Surgical Techniques Are Included Under CPT Code 28285?
CPT code 28285 covers the full range of surgical approaches used to correct lesser toe deformity. These include proximal interphalangeal (PIP) joint resection arthroplasty with removal of the distal head of the proximal phalanx, interphalangeal fusion (arthrodesis) with or without internal fixation such as K-wire, intramedullary implant, or screw, partial or total phalangectomy, and flexor or extensor tendon release or transfer when performed as a component of the hammertoe correction on the same digit.
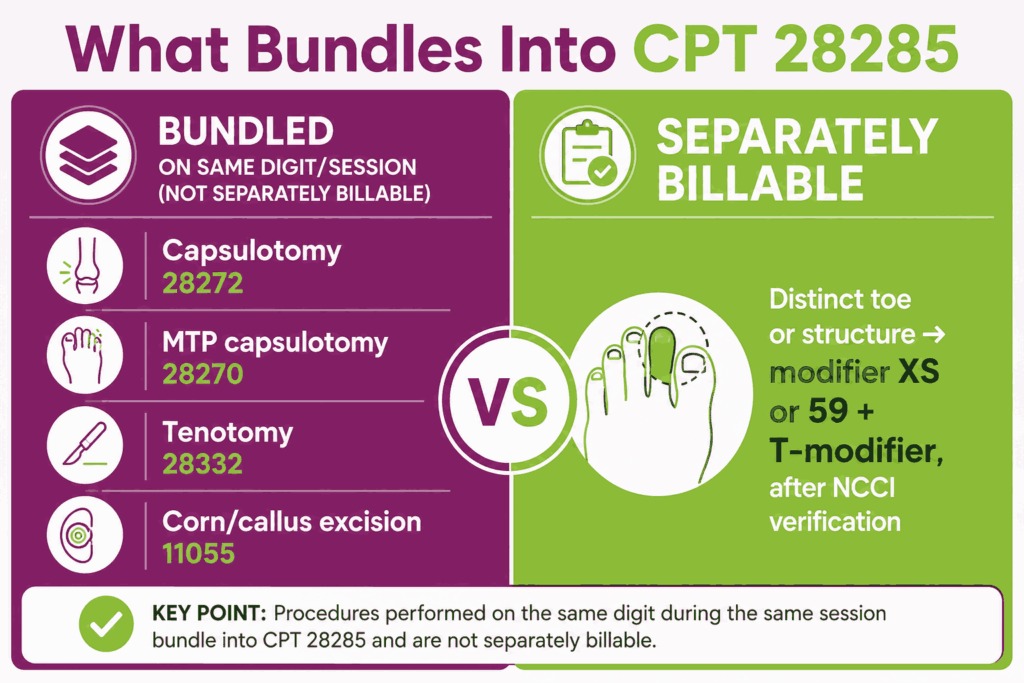
Per CMS RVU26A, all component procedures performed on the same digit, including tenotomy, capsulotomy, phalangectomy, and fixation, are bundled into a single unit of CPT code 28285 and are not separately reportable for the same toe. Documentation must name every component technique performed, even when all are bundled.
Does CPT Code 28285 Cover Claw Toe and Mallet Toe Corrections in Addition to Hammertoe?
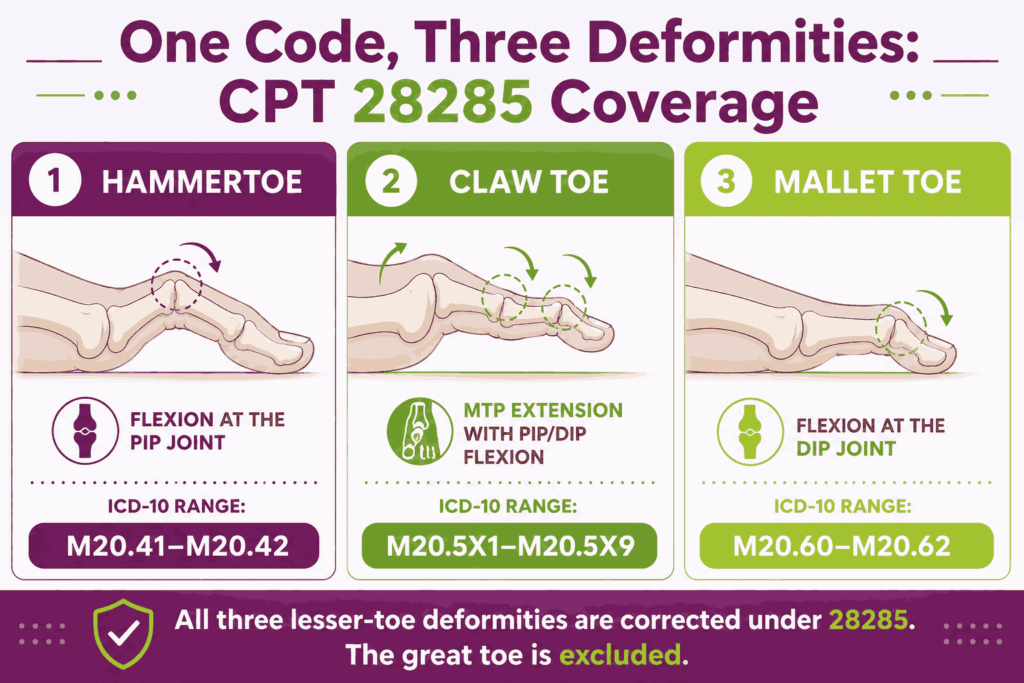
Yes, CPT code 28285 covers correction of hammertoe, claw toe, and mallet toe deformities of the lesser digits. All three deformity types involve abnormal flexion or extension posturing at the interphalangeal joints of the lesser toes and are corrected through the same surgical techniques captured under 28285 CPT code.
The ICD-10 diagnosis code should reflect the specific deformity type, such as M20.41–M20.42 (acquired hammertoe), M20.5X1–M20.5X9 (acquired claw toe), or M20.60–M20.62 (acquired mallet toe) to support accurate code selection and payer medical necessity review.
How Does CPT Code 28285 Differ From CPT Codes 28232, 28272, and 28313?
These codes cover related lesser toe procedures and must not be used interchangeably with procedure code 28285:
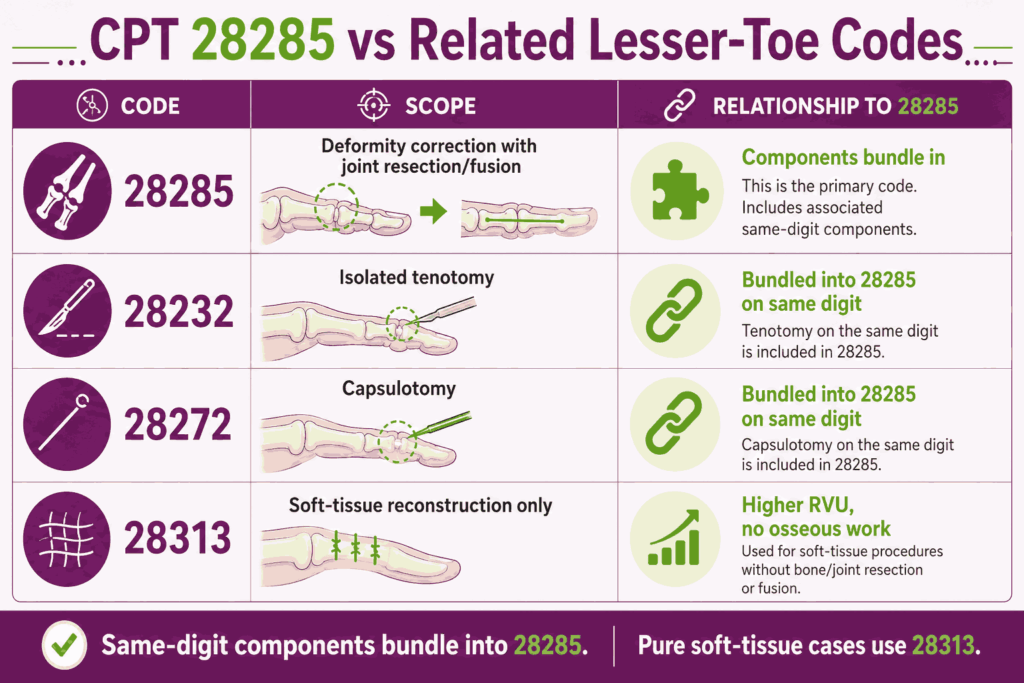
- CPT 28232: Tenotomy, open, toe, single tendon (separate procedure). Covers isolated tendon release without joint resection or fusion; when tenotomy is performed as a component of hammertoe correction on the same digit, it is bundled into CPT code 28285 and must not be reported separately
- CPT 28272: Capsulotomy, interphalangeal joint, including extensor hood apparatus, single joint. Covers isolated joint capsule release; per AAPC and NCCI, when performed on the same digit in the same session as CPT code 28285, it is bundled and not separately reportable
- CPT 28313: Reconstruction, angular deformity of digit, soft tissue procedures only (e.g., overlapping second/fifth digit or cock-up deformity, including skin plasty). Covers soft-tissue reconstruction only, without osseous procedures. It carries higher RVUs than the 28285 CPT code and is the correct code when only soft-tissue correction, not joint resection or fusion, is performed. Providers should review operative reports carefully before defaulting to procedure code 28285 on a purely soft-tissue case
These codes all sit within the broader set of lesser-toe and forefoot podiatry CPT codes, where technique and anatomical structure decide the correct selection.
What Are the Conservative Treatment Failure Requirements Before CPT Code 28285 Can Be Billed?
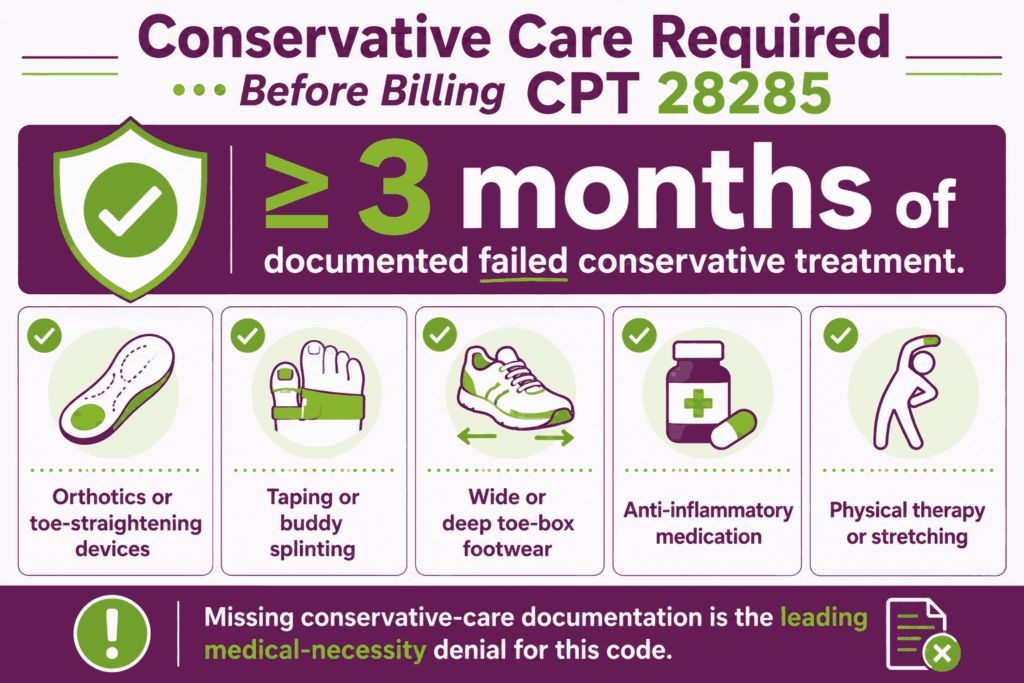
Medicare and most commercial payers require documented failure of conservative treatment before approving CPT code 28285 as medically necessary. Your documentation must reflect at least 3 months of failed conservative management, including one or more of the following: custom or prefabricated orthotics and toe-straightening devices, taping or buddy splinting of the affected digit, shoe modifications including wide or deep toe-box footwear, anti-inflammatory medications, and physical therapy or stretching exercises.
The operative note and pre-surgical evaluation must explicitly document the duration and type of conservative treatment attempted, the patient’s reported persistence of pain and functional impairment despite those efforts, and the clinical examination findings, including rigidity, skin breakdown, footwear interference, or ulceration, justifying surgical intervention.
Claims for 28285 CPT code submitted without evidence of prior conservative treatment failure are among the most frequently denied for medical necessity by both Medicare and commercial payers.
What Are the Modifiers for CPT Code 28285?
CPT code 28285 is reported with digit identification modifiers on every claim and may use additional circumstance modifiers for bilateral procedures, distinct services, and increased complexity.
Modifier 59: Distinct Procedural Service
Modifier 59 is used when CPT code 28285 is performed on a different toe than another procedure billed on the same date, and an NCCI edit would otherwise bundle the codes. Append modifier 59 only when documentation supports a distinct operative service on a separate anatomical structure, and a more specific X-modifier (such as XS) is not available or accepted by the payer.
Modifier XS: Separate Structure
Modifier XS is the preferred, more specific alternative to modifier 59 when procedure code 28285 is performed on a separate toe from another procedure billed on the same date. It provides greater coding specificity and is preferred by CMS and many commercial payers over modifier 59 when the distinct service involves a clearly separate anatomical structure.
Modifiers T0–T9: Toe Digit Identification
HCPCS Level II T-modifiers are required on every claim for CPT code 28285 to identify the specific toe corrected. Each unit of 28285 CPT code in a multi-toe claim must carry its own T-modifier:
- TA: Left foot, great toe
- T1: Left foot, 2nd digit
- T2: Left foot, 3rd digit
- T3: Left foot, 4th digit
- T4: Left foot, 5th digit
- T5: Right foot, great toe
- T6: Right foot, 2nd digit
- T7: Right foot, 3rd digit
- T8: Right foot, 4th digit
- T9: Right foot, 5th digit
Omission of a T-modifier on any line of procedure code 28285 is a primary cause of claim rejection. Note that CPT code 28285 is applied to lesser toes. The great toe is excluded from hammertoe correction coding under this code. Great-toe procedures are reported with hallux-specific codes such as CPT 28755 (great toe interphalangeal arthrodesis) or other hallux correction procedures as appropriate.
Modifier 51: Multiple Procedures
Modifier 51 is appended to each additional unit of CPT code 28285 or other procedure code performed in the same operative session beyond the primary procedure. The highest RVU procedure is listed first without a modifier; subsequent procedures on additional toes receive modifier 51. Under Medicare’s Multiple Procedure Payment Reduction (MPPR) rules, the second through fifth procedures are typically reimbursed at reduced percentages of the allowed amount.
Modifier 22: Increased Procedural Services
Modifier 22 is used when the work required to perform CPT code 28285 substantially exceeds what is typically required. For example, severe deformity with prior failed surgery, extensive scarring, or unusual anatomical complexity requiring significantly increased operative time. Append modifier 22 with a cover letter documenting the basis for the increased effort and total operative time.
Modifier 50: Bilateral Procedure
Modifier 50 is used when the identical hammertoe correction is performed on the same toe of both feet during the same operative session. When performing CPT code 28285 on different toes or on different feet at different digit positions, modifier 50 does not apply. Instead, use the appropriate T-modifiers with modifier 59 or XS instead. Medicare reimburses bilateral procedures billed with modifier 50 at 150% of the single-procedure allowed amount.
Which Documents Are Required For CPT Code 28285?
Per CMS RVU26A and CMS OPPS, documentation for CPT code 28285 must support medical necessity, surgical technique, and digit-specific identification.
Required documents checklist:
- Operative report naming every component procedure performed, like tenotomy, capsulotomy, phalangectomy, fusion, fixation, by technique and implant type
- Pre-surgical evaluation documenting at least 3 months of failed conservative treatment with specific modalities attempted
- Clinical examination findings confirming rigidity, pain, functional impairment, or skin breakdown justifying surgical correction
- Imaging (weight-bearing X-rays) demonstrating the deformity and any bony changes
- ICD-10 diagnosis code linked to the specific toe corrected and deformity type (hammertoe, claw toe, or mallet toe)
- Documentation of the specific digit(s) corrected, matching the T-modifier(s) appended on the claim
- Prior authorization approval where required by the payer
- Postoperative notes within the 90-day global period
- Hardware record (K-wire, implant, or fixation device manufacturer, model, lot number) where applicable
What is the Cost of CPT Code 28285?
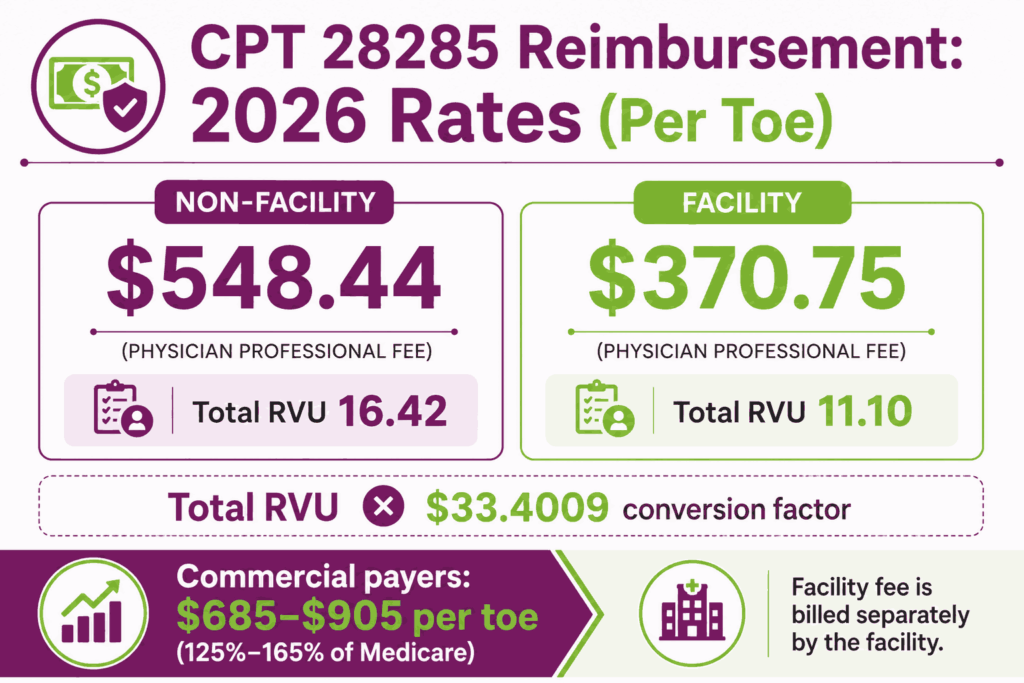
The cost of CPT code 28285 varies by payer, place of service, and geographic location. Note that the physician’s professional fee and the facility fee are billed and reimbursed separately.
RVUs & Medicare Payment
Medicare prices every surgical code through RVUs and the annual conversion factor, and 28285 follows that structure. Medicare calculates the baseline physician compensation for 28285 using a dual-track resource scale. For 2026, the Work RVU (wRVU) is firmly established at 5.48, reflecting the clinical time and technical skill required from the surgeon during the 90-day global surgical period.
In a private office setting, the Total Non-Facility RVU is 16.42, which incorporates substantial practice expenses for specialized surgical trays and post-operative monitoring supplies. Multiplied by the standard 2026 conversion factor of $33.4009, this results in a national unadjusted payment of $548.44. If the surgery is performed within a facility, the practice overhead shifts to the institution, dropping the Total Facility RVU to 11.10 and lowering the direct physician allowance to $370.75.
Commercial Payers
Commercial health insurance networks typically reimburse hammertoe corrections at 125% to 165% of the standard Medicare schedule, leading to global private allowable amounts between $685 and $905 per toe. To prevent costly claim rejections from private carriers in 2026, billing teams must strictly manage Medically Unlikely Edits (MUEs), which cap 28285 at 4 units per session. Furthermore, appending specific anatomical T-modifiers (T0–T9) is mandatory when correcting multiple toes on a single foot.
Place-of-Service & Geographic Adjustments
The final allowable baseline for CPT code 28285 is adjusted regionally by the Geographic Practice Cost Index (GPCI). Additionally, the chosen Place of Service (POS) alters the entire institutional cost footprint. In a private clinic (POS 11), the practice captures the full $548.44 global rate. Conversely, when performed in an Ambulatory Surgical Center (POS 24) or a Hospital Outpatient Department (POS 22), the physician receives the scaled professional fee of $370.75, while the facility bills a separate, much larger facility fee.
What Are Example Clinical Scenarios or Use Cases for CPT Code 28285?
CPT code 28285 applies when surgical correction of a lesser toe deformity, like hammertoe, claw toe, or mallet toe, is performed in a facility setting following documented failure of conservative management.
Scenario 1: Rigid Hammertoe of the Second Digit With Failed Conservative Management
ICD-10: M20.411 (Acquired hammertoe of right foot, second toe)
The patient presents with a rigid hammertoe deformity of the right second toe, causing persistent pain, inability to wear standard footwear, and a painful callus overlying the proximal interphalangeal joint. Three months of orthotics and shoe modification have not provided relief. The podiatric surgeon performs PIP joint resection arthroplasty with K-wire fixation. CPT code 28285 is reported with modifier T6.
Scenario 2: Bilateral Claw Toe Deformity Requiring Interphalangeal Fusion on Multiple Toes
ICD-10: M20.5X2 (Acquired clawfoot of left foot)
The patient has bilateral claw toe deformity of the second and third digits of the left foot, causing chronic pain and ulceration risk. Conservative management has failed after 4 months of specialized footwear and orthotics. The surgeon performs interphalangeal fusion on both affected toes in a single operative session. CPT code 28285 is reported twice, with modifier T1 for the second digit and a second unit with modifiers 51 and T2 for the third digit.
Scenario 3: Mallet Toe Correction With Partial Phalangectomy in a Diabetic Patient
ICD-10: M20.6X1 (Acquired mallet toe of right foot)
A patient with type 2 diabetes and peripheral neuropathy presents with a mallet toe deformity of the right third digit, causing a distal subungual ulcer at risk for infection. Following documentation of failed conservative care and confirmation of vascular adequacy, the surgeon performs distal interphalangeal joint partial phalangectomy.
Given the increased complexity of surgical planning and intraoperative management in the setting of diabetes and neuropathy, modifier 22 is appended to CPT code 28285 with modifier T7, supported by documentation of increased operative time and clinical complexity.
What Are the CPT Code 28285 Rules To Ensure Successful Reimbursement?
Follow payer and policy rules for documentation, bundling, global period management, and multi-toe billing. Meeting these rules reduces denials and ensures correct payment for podiatry code 28285.
Bundling / NCCI / Same-Day Procedure Rules
Per AAPC and NCCI, capsulotomy (CPT 28272 code) and MTP capsulotomy (code CPT 28270) performed on the same digit in the same session are bundled into CPT code 28285 and must not be separately reported. Tenotomy (CPT code 28232) performed as a component of the hammertoe correction on the same digit is similarly bundled.
Corn and callus excision (e.g., CPT code 11055) on the same toe at the same session is routinely denied by payers. It is considered caused by the hammertoe and therefore included in procedure code 28285. When distinct procedures are performed on different toes or different anatomical structures in the same session, modifier XS or modifier 59 with the appropriate T-modifier supports separate reimbursement after NCCI edit verification.
Units, MUEs & Multi-Toe Billing Rules Using T-Modifiers
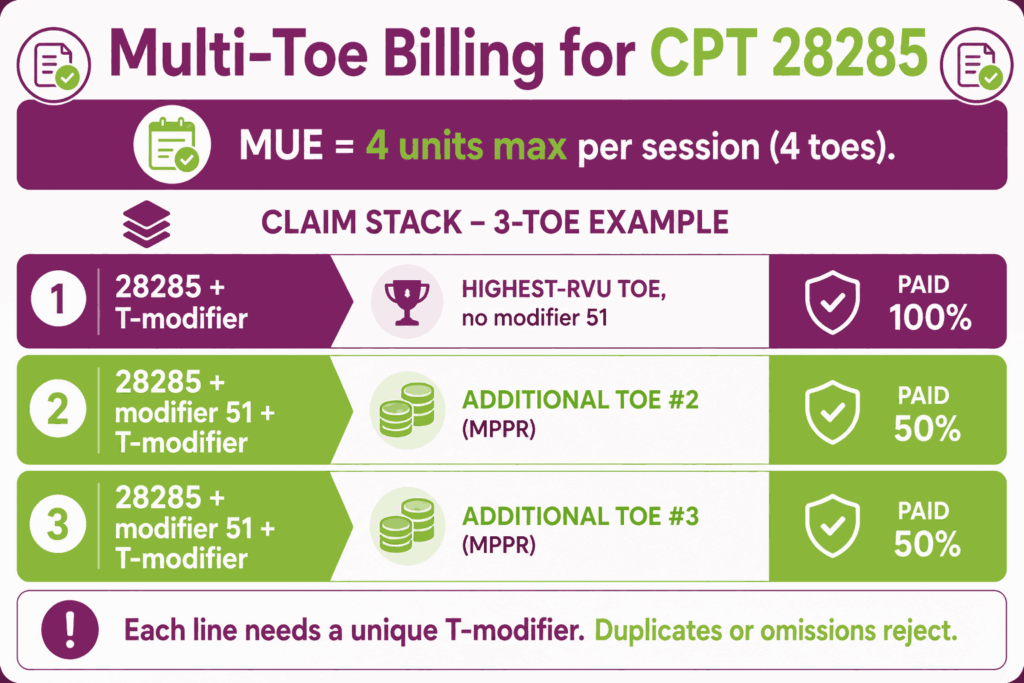
CPT code 28285 has a Medicare MUE of 4 units per operative session, meaning up to four toes may be corrected and billed in a single encounter.
- Each unit of 28285 CPT code in a multi-toe claim must carry a unique T-modifier identifying the specific digit. Claims missing T-modifiers or with duplicate T-modifiers will reject
- The highest RVU procedure is listed first without modifier 51. Each additional unit on subsequent toes receives modifier 51
- Under MPPR, the first procedure is paid at 100% of the allowed amount. The second through fourth procedures are generally reduced to 50% of the allowed amount
- Modifier 50 applies only when the identical procedure is performed on the same digit of both feet in the same session. Use individual T-modifiers for different toes on different feet
- CPT code 28285 carries a 90-day global period. All routine postoperative visits, wound checks, hardware removal planning, and toe splinting within 90 days are bundled. An unplanned return to the OR for a related complication requires modifier 78
Prior Authorization and Medical Necessity Requirements
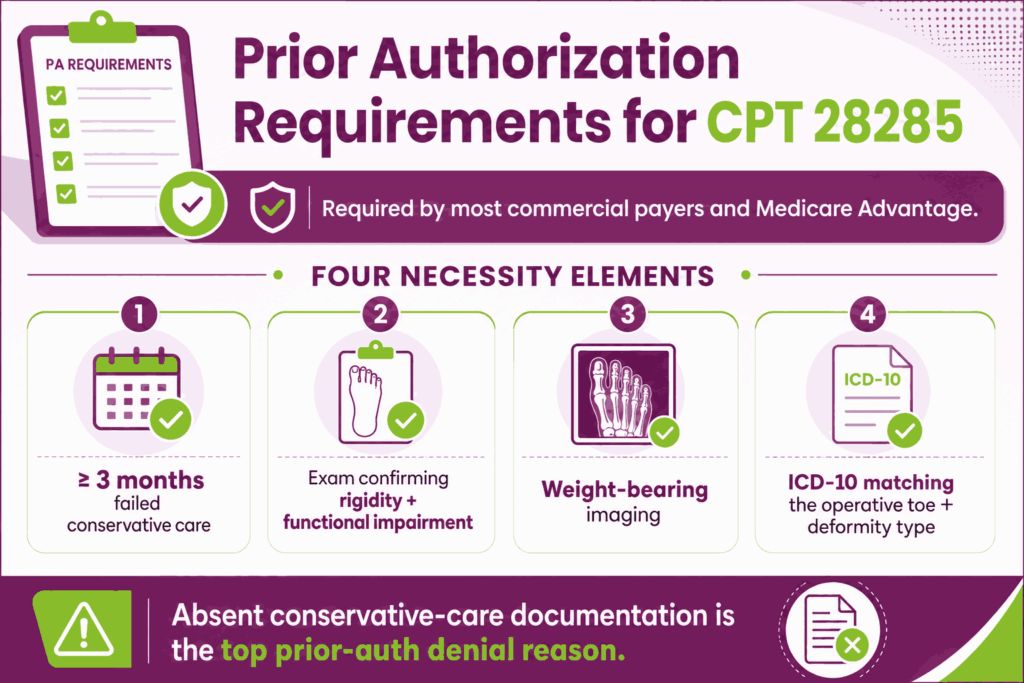
Most commercial payers and Medicare Advantage plans require prior authorization for CPT code 28285. Medical necessity must be supported by documented failure of at least 3 months of conservative treatment, clinical examination confirming deformity rigidity, functional impairment, weight-bearing imaging, and an ICD-10 diagnosis code matching the operative toe and deformity type.
Remember, lack of medical necessity documentation, particularly the absence of documented conservative treatment failure, is the most frequent cause of prior authorization denial and claim denial for procedure code 28285.
Top Reasons For Denials Specific To 28285 & Quick Remedies
- Missing or Wrong T-Modifier: Prevent by appending the correct T-modifier to every unit of CPT code 28285 before submission. Omission or mismatch between the T-modifier and the operative report is a primary cause of automatic claim rejection.
- Bundling Violations (28272 or 28270 Billed Separately for Same Digit): Prevent by confirming NCCI edits. Capsulotomy and tenotomy on the same digit are bundled into the 28285 CPT code and must not be separately reported.
- MUE Exceeded — More Than 4 Units Per Session: Prevent by confirming the number of toes billed does not exceed the MUE of 4 per operative session; claims exceeding the MUE are automatically denied without additional documentation.
- Modifier 51 Omitted on Multi-Toe Claims: Prevent by appending modifier 51 to all procedure lines beyond the first in a multi-toe claim and listing the highest RVU procedure first.






