CPT code 29881 reports a surgical knee arthroscopy with meniscectomy in a single compartment, medial or lateral. The code includes any meniscal shaving and all chondroplasty performed in the same knee, in any compartment.
CPT 29881 carries the most misunderstood bundling rule in knee arthroscopy. Since the 2012 descriptor revision, chondroplasty has been part of the code definition itself, so no modifier and no payer pathway pays it separately.
That single rule, plus payer restrictions on degenerative tears with arthritis, drives most denials and recoupments on this code. Many sports medicine groups route arthroscopy claims through orthopedic billing services to manage them.
What Is the Description of CPT Code 29881?
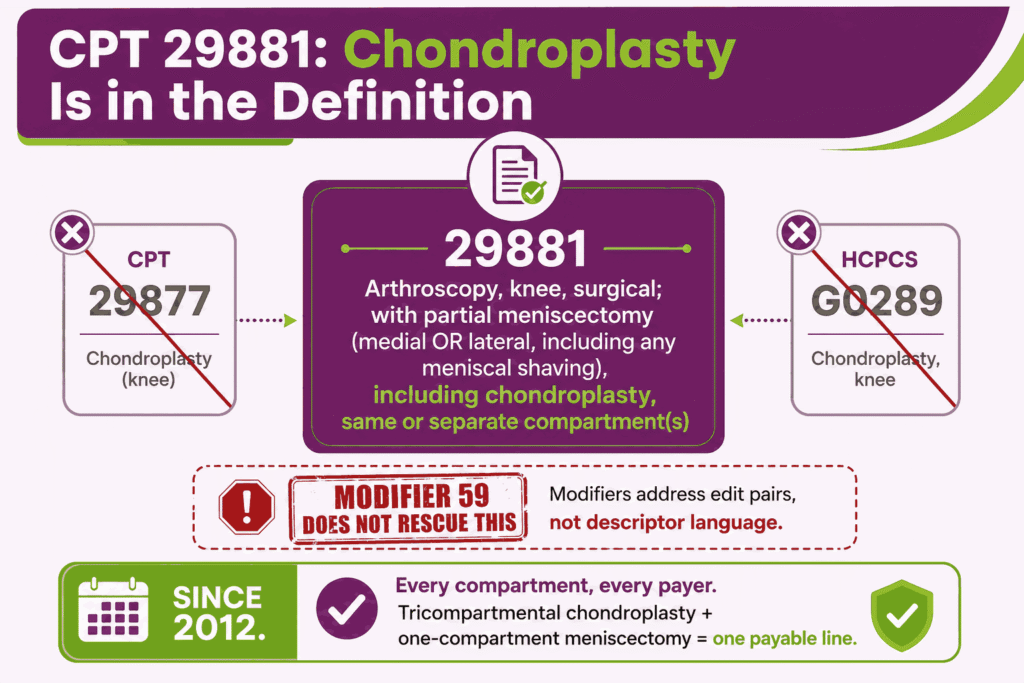
The 29881 CPT code description as defined by the AMA is: “Arthroscopy, knee, surgical; with meniscectomy (medial OR lateral, including any meniscal shaving) including debridement/shaving of articular cartilage (chondroplasty), same or separate compartment(s), when performed.”
This code reports the arthroscopic removal of torn meniscal tissue from one compartment of the knee. CPT code 29881 includes the diagnostic arthroscopy, the meniscectomy with any meniscal shaving, and any chondroplasty performed anywhere in the same knee during the session.
The descriptor language does the heavy lifting on this code. Procedure code 29881 absorbs cartilage debridement by definition, which is why the bundling rules below behave differently from ordinary NCCI edits.
What Does “Single Compartment” Mean for CPT Code 29881 and When Must 29880 Be Used Instead?
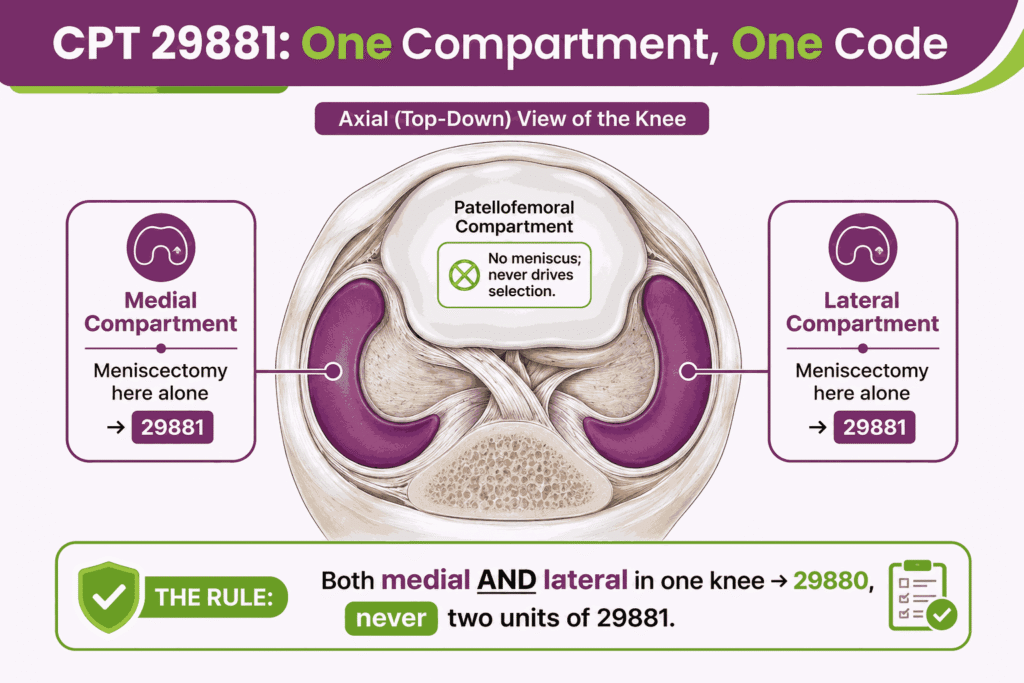
The knee has three recognized compartments: medial, lateral, and patellofemoral. CPT code 29881 reports meniscectomy in one meniscal compartment, either medial or lateral.
The compartment selection rules are:
- Meniscectomy in the medial or the lateral compartment alone is 29881
- Meniscectomy in both the medial and lateral compartments of the same knee is 29880
- Never report 29881 twice for the same knee to capture both compartments
- The patellofemoral compartment has no meniscus, so it never drives meniscectomy code selection
The operative note must identify the compartment treated. A claim reporting two units of CPT 29881 on one knee is a coding error that the bicompartmental code 29880 exists to prevent.
Is Chondroplasty Separately Billable in Any Compartment of the Same Knee When CPT 29881 Is Reported?
No. Chondroplasty is never separately billable with CPT code 29881 on the same knee, in any compartment, for any payer. The 2012 revision of the meniscectomy descriptors placed chondroplasty inside the code definition, same or separate compartment.
The chondroplasty bundle works as follows:
- The bundle is definitional, written into the 29881 descriptor itself, not merely an NCCI edit pair
- Chondroplasty code 29877 is barred with 29881 regardless of the compartment treated
- HCPCS code G0289, the Medicare separate-compartment code, is equally barred for chondroplasty when reported with 29881
- Modifier 59 does not rescue the charge, because a modifier cannot unbundle work the code definition already includes
A tricompartmental chondroplasty performed with a single-compartment meniscectomy still produces one payable line: 29881. Practices that append modifier 59 to 29877 in this situation create recoupment exposure, not revenue.
How Does CPT 29881 Differ From Meniscal Repair Codes 29882 and 29883?
Meniscectomy removes torn tissue, while repair sutures it. The distinction matters for coding because the repair descriptors were never revised to include chondroplasty.
The excision and repair codes compare as follows:
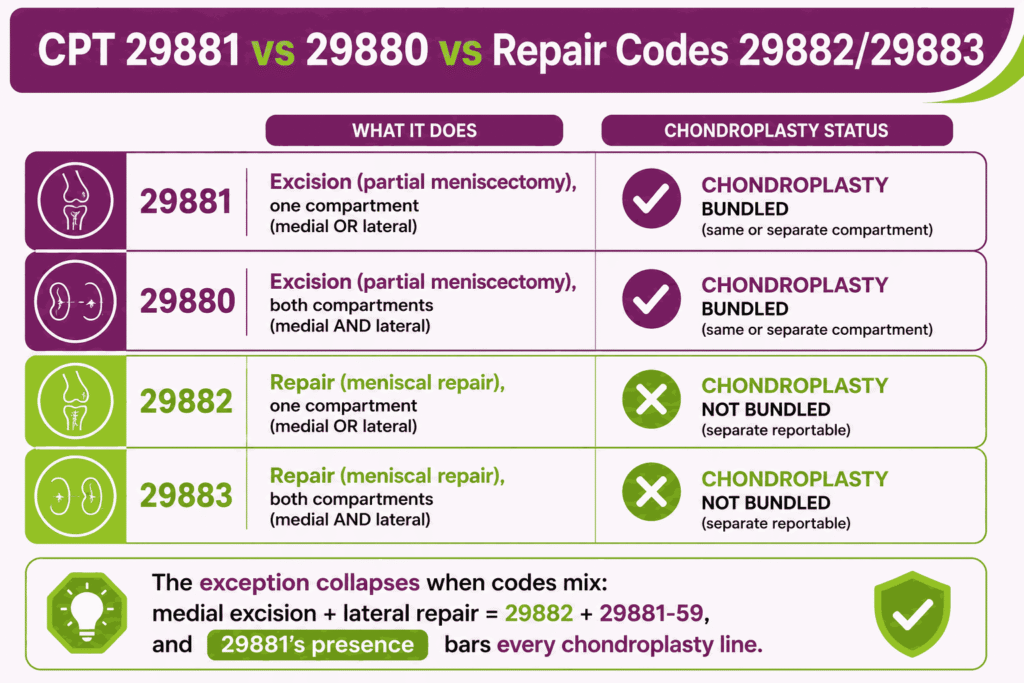
- 29881 meniscectomy, one compartment: chondroplasty bundled in any compartment
- 29880 meniscectomy, both compartments: chondroplasty bundled in any compartment
- 29882 meniscal repair, one compartment: chondroplasty not bundled
- 29883 meniscal repair, both compartments: chondroplasty not bundled
With a repair code, chondroplasty performed in a separate compartment is separately reportable. The exception collapses when a meniscectomy is also performed: a medial meniscectomy with lateral repair reports 29882 and 29881 with modifier 59.
The presence of CPT 29881 on the claim precludes any chondroplasty line, even in the untouched patellofemoral compartment. Descriptor-level details like this separate the meniscectomy and repair families across the orthopedic procedure codes, where a revision year can change what a code absorbs.
What ICD-10 Codes and Medical Necessity Criteria Support CPT Code 29881?
Medical necessity for CPT code 29881 rests on a documented meniscal tear with symptoms that conservative care has not resolved. The tear type and the state of the joint cartilage both matter to payers.
Representative supporting diagnoses include:
- S83.211A through S83.289A (Acute meniscal tear codes, by location and tear pattern)
- M23.203 through M23.269 (Derangement of meniscus due to old tear or injury)
- M23.305 and related codes (Other meniscus derangements) where payer policy accepts them
- Mechanical symptom documentation, such as locking, catching, or giving way, recorded in the note
The diagnosis must reflect the tear the imaging shows. MRI confirmation of the tear, the compartment, and the tear morphology anchors the claim. Selecting between the S83 acute-tear series and the M23 old-injury codes follows the same conventions that run through orthopedic ICD-10 coding generally, where injury timing changes the category.
Why Payers Deny APM for Degenerative Tears With Moderate-to-Severe OA (KL 3–4)
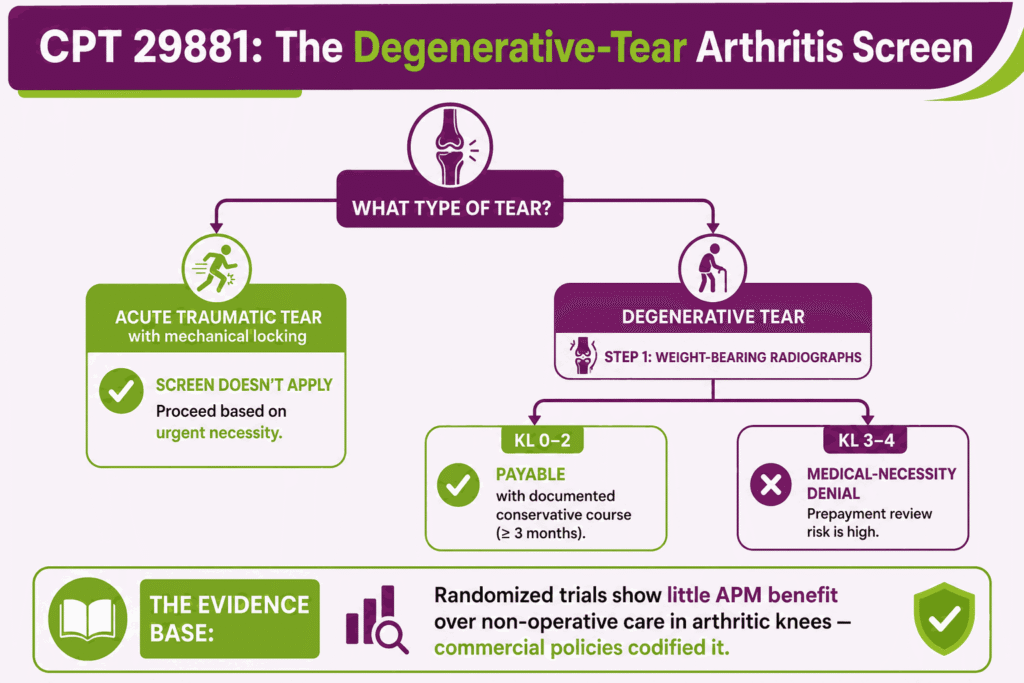
Payers deny arthroscopic partial meniscectomy when the tear is degenerative and the joint shows moderate-to-severe osteoarthritis, typically Kellgren-Lawrence grade 3 or 4. Randomized trial evidence shows little benefit of APM over non-operative care in that population, and commercial medical policies have followed it.
The osteoarthritis screen works like this:
- Weight-bearing radiographs showing KL grade 3 or 4 changes in the operative compartment trigger medical-necessity denial for a degenerative tear
- The policies target degenerative tears, not acute traumatic tears with mechanical locking
- The record must include the imaging and, for degenerative presentations, evidence that arthritis is absent or mild
- Submitting CPT code 29881 for a degenerative tear in an arthritic knee invites prepayment review and denial
What Are the Conservative Treatment Failure Requirements Before CPT 29881 Can Be Authorized?
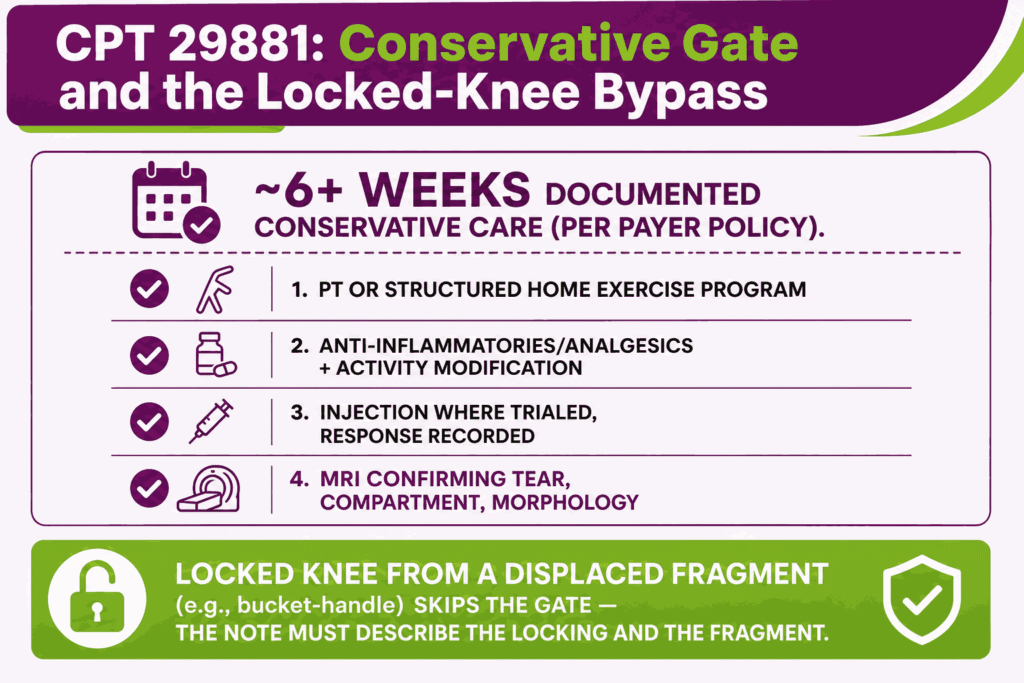
Payers require a documented course of conservative care before authorizing elective CPT code 29881. The common expectation is at least six weeks of non-operative management with recorded outcomes.
Typical conservative documentation includes:
- A trial of roughly six weeks or more of conservative care, per the payer’s policy
- Physical therapy or a structured home exercise program addressing the knee
- Anti-inflammatory medication or analgesics and activity modification
- An intra-articular injection where trialed, with the response recorded
- MRI confirming the meniscal tear and its compartment
- Persistent pain or mechanical symptoms despite the completed trial
The acute exception matters: a locked knee from a displaced tear, such as a bucket-handle fragment blocking motion, bypasses the conservative-care gate. Urgent mechanical obstruction is its own necessity, and the note must describe the locking and the displaced fragment.
What are the Modifiers for CPT Code 29881?
CPT 29881 uses modifiers for laterality, bilateral sessions, distinct procedures, the surgical decision, and the global period. The correct modifier depends on the anatomy and the timing.
Modifier LT / Modifier RT: Laterality
Modifiers LT and RT identify the left or right knee. Append the correct laterality modifier to CPT code 29881 on every unilateral claim, since most payers require it on knee arthroscopy. The operative note must state the side.
Modifier 50: Bilateral Procedure Same Session
Modifier 50 reports arthroscopic meniscectomy performed on both knees in one session. Append modifier 50 to 29881 when each knee receives a single-compartment meniscectomy on the same date. Confirm whether the payer wants one line with modifier 50 or two lines with RT and LT.
Modifier 22: Increased Procedural Complexity
Modifier 22 reports substantially greater work than the procedure typically requires. Append modifier 22 to CPT code 29881 only when the operative note documents the added difficulty, such as a complex displaced tear with extensive fragment retrieval. A narrative must accompany the claim.
Modifier 51: Multiple Procedures Same Session
Modifier 51 identifies multiple procedures in the same session. Append modifier 51 to the secondary procedure when 29881 is performed with another separately payable procedure. The multiple procedure payment reduction applies to the lower-valued service.
Modifier 57: Decision for Surgery (attaches to the E/M; urgent locked-knee case)
Modifier 57 attaches to the evaluation and management visit at which the decision for major surgery was made, on the day of or the day before the procedure. Append modifier 57 to the E/M code, not to CPT code 29881. The urgent locked-knee presentation is the typical case, where the decision and the surgery fall within a day.
Modifier 58: Staged or Related Procedure During 90-Day Global
Modifier 58 reports a planned or related procedure during the global period. Append modifier 58 to a subsequent procedure that was staged or anticipated at the time of 29881, such as a planned second-look intervention. The modifier shows the return was expected.
Modifier 59 / XS: Distinct Procedural Service
Modifier 59, or the more specific XS, identifies a genuinely distinct procedure at a separate site in the same session. Append it to the qualifying companion code, such as a meniscal repair in the opposite compartment billed alongside CPT code 29881. The modifier never applies to chondroplasty with this code because the bundle is definitional.
Modifier 78: Unplanned Return to OR During Global Period
Modifier 78 reports an unplanned return to the operating room for a related complication during the global period. Append modifier 78 to the second procedure when a complication of 29881, such as a septic joint requiring washout, forces unplanned surgery. Payment covers intraoperative work only.
Modifier 79: Unrelated Procedure During Global Period
Modifier 79 reports an unrelated procedure during the global period. Append modifier 79 to a service unrelated to the 29881 recovery, such as a contralateral knee arthroscopy. The modifier starts a new global period for the unrelated procedure.
Which Documents Are Required For CPT Code 29881?
Documentation for CPT code 29881 must establish the tear, the failed conservative course or acute exception, and the compartment treated. The operative note also protects against the risk of recoupment for chondroplasty.
The required documentation includes:
- MRI report confirming the meniscal tear, its compartment, and its morphology
- Conservative-treatment records, or documentation of acute locking that bypasses the gate
- Weight-bearing radiographs establishing the arthritis grade for degenerative presentations
- Prior authorization where the payer requires it, matched to the correct knee
- An operative note identifying the compartment of the meniscectomy and all work performed
- Explicit documentation of any chondroplasty performed, even though it is not separately billed
- Laterality documentation for the knee treated
What Is the Cost of CPT Code 29881?
The cost of CPT code 29881 splits into the surgeon professional fee and the facility fee for the arthroscopy. Medicare prices the professional fee through the Physician Fee Schedule.
RVUs & Medicare Payment
Medicare prices the professional component of CPT code 29881 through the Physician Fee Schedule. The CY2026 values appear below.
| Component | Value (CY 2026) |
|---|---|
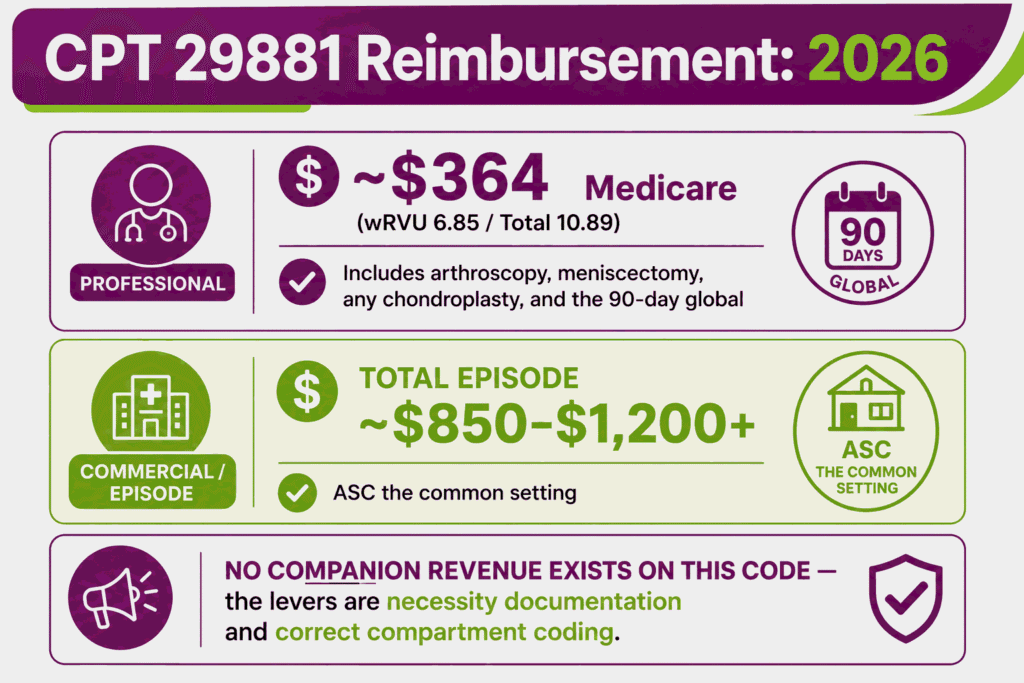
| Work RVU | 6.85 |
| Total RVU | 10.89 |
| Medicare professional payment | ~$364 |
| Conversion factor | $33.4009 |
| Global period | 090 |
The professional fee covers the arthroscopy, the meniscectomy, any chondroplasty performed, and the 90-day global period. The 2026 efficiency adjustment reduced the work component of non-time-based surgical codes by 2.5 percent. GPCI adjustments change the final amount by locality.
Commercial Payers
Commercial plans reimburse procedure code 29881 at a contracted multiple of the Medicare rate. Total episode amounts, including the facility commonly run from roughly $850 to well above $1,200, with the professional fee a fraction of that figure.
Because the chondroplasty bundle applies to every payer, commercial claims gain nothing from a 29877 line. The revenue lever on this code is clean necessity documentation and correct compartment coding, not companion charges.
Place-of-Service & Geographic Adjustments
CPT code 29881 is performed in facility settings, most commonly the ambulatory surgery center. The setting determines the facility payment, and locality adjusts the professional fee.
Key setting and geographic factors include:
- Ambulatory surgery center billing pays the ASC fee schedule rate, the common setting for elective meniscectomy
- Hospital outpatient billing pays through the outpatient prospective payment system at a higher APC rate
- Inpatient admission is rare for this procedure and requires clinical justification
- GPCI values adjust the professional fee components by locality
What Are Example Clinical Scenarios or Use Cases for CPT Code 29881?
CPT code 29881 applies when a symptomatic meniscal tear in one compartment requires arthroscopic excision. The scenarios below show the acute exception, the degenerative screen, and the chondroplasty bundle in practice.
Scenario 1: Acute Medial Meniscal Bucket-Handle Tear With Mechanical Locking and Failed Conservative Management
ICD-10: S83.211A (Bucket-handle tear of medial meniscus, current injury, right knee, initial encounter)
A 28-year-old presents after a twisting injury with a locked right knee that will not fully extend. MRI shows a displaced bucket-handle tear of the medial meniscus. The displaced fragment blocking motion is an urgent mechanical indication, so the conservative-care gate does not apply. The surgeon performs an arthroscopic partial medial meniscectomy, and the practice reports CPT code 29881 with modifier RT. The decision-for-surgery visit carries modifier 57 on the E/M line.
Scenario 2: Degenerative Lateral Meniscal Tear With Persistent Mechanical Symptoms in a Middle-Aged Patient
ICD-10: M23.202 (Derangement of unspecified lateral meniscus due to old tear or injury, left knee)
A 52-year-old has persistent lateral knee pain with catching six months after a minor injury. Weight-bearing radiographs show no moderate-to-severe arthritis, and MRI confirms a degenerative lateral tear. The record documents eight weeks of physical therapy, anti-inflammatory medication, and an injection without relief. The surgeon performs an arthroscopic partial lateral meniscectomy, and the practice reports CPT 29881 with modifier LT. The absent-arthritis imaging and the completed conservative course are what carry this claim past the degenerative-tear screen.
Scenario 3: Medial Meniscal Root Tear With Same-Session Multi-Compartment Cartilage Debridement (Illustrating the Bundled Chondroplasty Rule)
ICD-10: S83.231A (Complex tear of medial meniscus, current injury, right knee, initial encounter)
A patient undergoes arthroscopy for a medial meniscal root tear. During the case, the surgeon also debrides articular cartilage in the medial and patellofemoral compartments. The practice reports one line: CPT code 29881 with modifier RT. The chondroplasty in both compartments is bundled by the code descriptor, so no 29877 or G0289 line is added, and no modifier changes that outcome. The operative note still documents the cartilage work in full.
What Are the CPT Code 29881 Rules To Ensure Successful Reimbursement?
Follow the definitional bundling rules, unit and bilateral limits, the companion-code rules for loose bodies and synovectomy, and the global-period modifiers. Meeting these rules protects CPT code 29881 claims from denial and recoupment.
Bundling / NCCI / Same-Day Procedure Rules
The chondroplasty bundle is the enforcement center of CPT code 29881. It behaves differently from a standard NCCI edit because it lives in the code descriptor.
The core bundling rules are:
- Chondroplasty is bundled into 29881 in every compartment of the same knee, for every payer, since the 2012 descriptor revision
- Modifier 59 does not unbundle it, because the modifier addresses edit pairs, not work the code definition includes
- Diagnostic arthroscopy of the same knee is included and never separately reported
- Appending 59 to a chondroplasty line may slip past an automated edit, and post-payment review then converts the paid line into recoupment exposure with audit risk
The safe rule is structural: when CPT 29881 is on the claim, no cartilage-debridement line joins it. Document the chondroplasty in the note and leave it off the claim. The distinction matters because most bundles in the CPT code system live in NCCI edit tables that modifiers can address, while descriptor-level inclusions like this one sit above them.
Units, MUEs & Bilateral Knee Arthroscopy Billing Rules
CPT code 29881 is billed as one unit per knee per session. Compartment count changes the code, not the units.
Unit and bilateral rules include:
- One unit of 29881 per knee, since the bicompartmental case routes to 29880
- Never report two units of 29881 on the same knee for two compartments
- Bilateral same-session cases use modifier 50 or the payer’s two-line RT and LT format
- Confirm the current Medically Unlikely Edit value through CMS, since the table updates quarterly
When G0289, CPT 29874, and CPT 29876 Can and Cannot Be Separately Reported Alongside CPT 29881
The companion codes for loose bodies and synovectomy have narrow, compartment-driven rules with CPT code 29881. Each is payable only for distinct work the meniscectomy code does not already include.
The companion-code rules are:
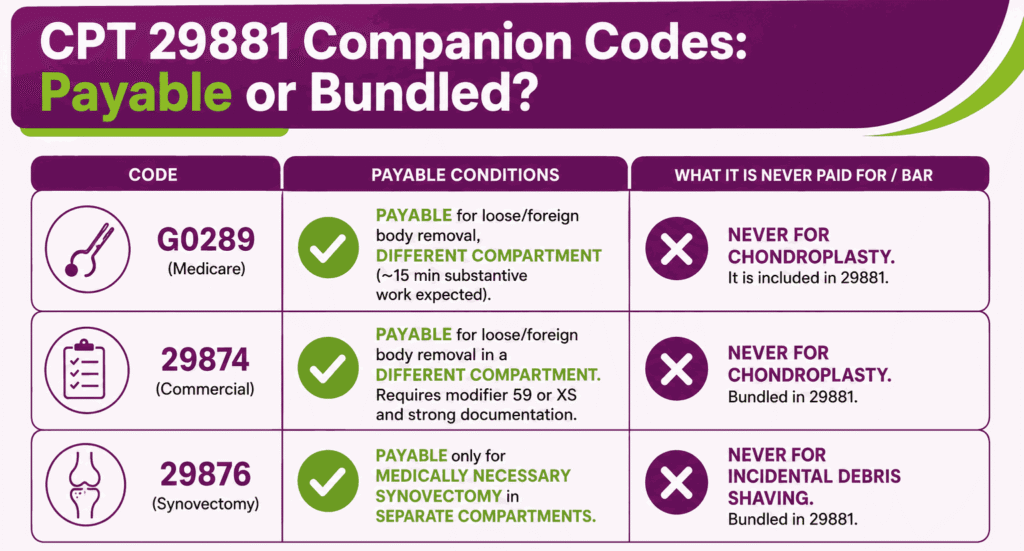
- G0289 is reportable with 29881 for Medicare only for the removal of a loose or foreign body from a different compartment of the same knee, and never for chondroplasty
- Medicare guidance also expects the separate-compartment work to be substantive, on the order of 15 minutes of additional time
- 29874 loose body removal follows the same compartment logic for commercial payers, with modifier 59 or XS and documentation of the distinct compartment
- 29876 major synovectomy is reportable only when performed as medically necessary work in compartments separate from the meniscectomy, not as incidental debris shaving
Same-compartment loose body removal or synovial work is bundled into CPT 29881. The operative note must name the compartments for every companion line billed.
90-Day Global Period, Modifier 58, and Return-to-OR Billing Rules
CPT code 29881 carries a 90-day global period that includes routine post-operative care. Returns and unrelated services during the window each take a specific modifier.
The global-period rules are:
- Routine post-operative visits within 90 days are included in the 29881 payment
- A staged or anticipated procedure during the window uses modifier 58
- An unplanned related return to the operating room uses modifier 78, with payment limited to intraoperative work
- An unrelated procedure uses modifier 79, and an unrelated E/M visit uses modifier 24
Top Reasons For Denials Specific To 29881 & Quick Remedies
- Chondroplasty Billed Alongside the Meniscectomy: Prevent by removing every 29877 and G0289 chondroplasty line when CPT code 29881 is on the claim, in any compartment, for any payer.
- Degenerative Tear in an Arthritic Knee: Prevent by screening weight-bearing radiographs before authorization and reserving surgery requests for knees without moderate-to-severe arthritis, or for acute mechanical indications.
- Missing Conservative-Care Documentation: Prevent by attaching the completed conservative trial, or the locked-knee documentation that bypasses it, to the authorization and the claim.
- Two Units or Two Compartments Miscoded: Prevent by reporting bicompartmental meniscectomy as 29880, never as two units of 29881.
- Missing Laterality or Wrong Bilateral Format: Prevent by appending RT or LT to every unilateral claim and confirming the payer’s bilateral format before submitting.