
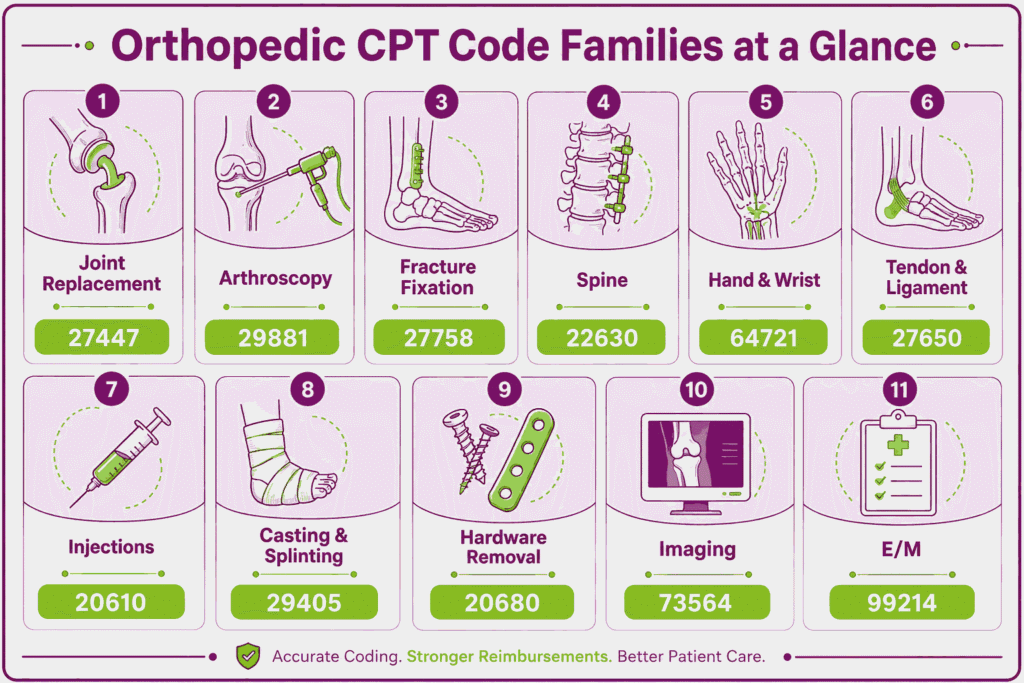
Orthopedic CPT codes report musculoskeletal procedures within the 20000 to 29999 surgical range. They span joint replacement, arthroscopy, fracture fixation, spine, and hand surgery, plus the injection and casting codes billed daily. High volume and strict modifier rules make accuracy hard, so many practices use orthopedic medical billing services to protect reimbursement.
Errors carry measurable cost. An HHS Office of Inspector General audit found 69 of 100 sampled surgical services were billed incorrectly. Most lacked co-surgery or assistant-at-surgery modifiers, and OIG estimated $4.9 million in improper Medicare payments (HHS-OIG, 2022).
Global periods add more exposure. A separate OIG review of 105 global surgeries found that 98 fees did not match the postoperative visits provided (HHS-OIG, 2025). This guide lists the most-used orthopedic CPT codes, modifiers, and global periods for 2026.
What Are the Most Used Orthopedic CPT Codes by Category?
Orthopedic codes split by procedure family, surgical approach, and laterality. The families below cover the codes a coder reaches for most. Each entry gives the descriptor, the documentation rule that supports payment, and the modifier or NCCI trap that most often causes denials.
This page covers the core billing details for each code. Where a dedicated code guide exists, the deeper rules, reimbursement data, and payer scenarios live there.
Which CPT Codes Cover Joint Replacement and Arthroplasty?
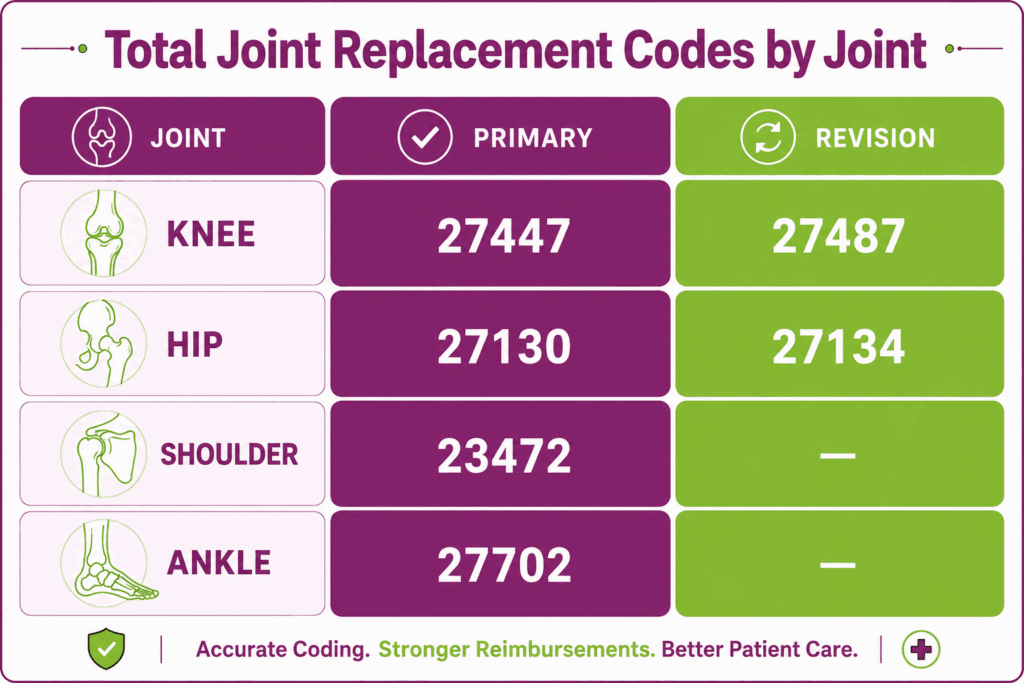
Joint replacement codes carry 90-day global periods and high RVUs. Each one needs the joint, the components, and the side documented. Bilateral cases use modifier 50. Audit exposure is high, so operative detail matters.
CPT 27447: Total Knee Arthroplasty (TKA)
CPT 27447 reports a total knee arthroplasty of the medial and lateral compartments, with or without patellar resurfacing. It is the highest-volume major orthopedic surgical code. Documentation must confirm that both compartments were replaced, since partial replacement uses a different code. Append modifier 50 for a same-session bilateral procedure to the code CPT 27447.
CPT 27130: Total Hip Arthroplasty (THA)
CPT 27130 reports a total hip arthroplasty, including acetabular and femoral components, with or without a bone graft. The operative note must record the surgical approach and the implants used. Bilateral procedures take modifier 50. A revision is never coded as the CPT 27130 code, even when components are exchanged.
CPT 23472: Total Shoulder Arthroplasty
CPT 23472 reports glenohumeral joint replacement, covering both anatomic and reverse total shoulder arthroplasty. The note must state which construct was used, since reverse arthroplasty carries distinct medical-necessity criteria. Many payers require prior authorization. Document the rotator cuff status that supports a reverse build as required by the 23472 CPT code description.
CPT 27702: Total Ankle Arthroplasty
CPT 27702 reports total ankle replacement with a prosthetic implant. It is lower volume and frequently subject to prior authorization and payer coverage policy. Confirm coverage before the procedure for the 27702 code CPT. Document the failed conservative care that supports surgical necessity.
CPT 27487: Revision Total Knee, Both Components
CPT 27487 reports revision knee arthroplasty when both the femoral and tibial components are removed and replaced. Code CPT 27486 applies when only one component is revised. The operative note must document which components were exchanged. Append modifier 22 to CPT code 27487 only when increased complexity is clearly supported.
CPT 27134: Revision Total Hip, Both Components
CPT 27134 reports revision total hip arthroplasty with replacement of both the acetabular and femoral components. Documentation must record the reason for revision, such as loosening, wear, or infection, and the hardware removed. Coding revision without a documented failure mode invites denial for the 27134 CPT.
CPT 27447 vs 27487: When Is It Primary Versus Revision?
The distinction is whether prior hardware is present. CPT code 27447 reports a first-time total knee replacement. CPT 27487 reports revision when existing components are removed and replaced. Code 27487 covers both femoral and tibial components, while 27486 covers one. Bill revision only when the operative note documents component exchange.
Which CPT Codes Cover Arthroscopy?
Arthroscopy is the most NCCI-sensitive orthopedic family. The diagnostic scope of a joint bundles into any surgical procedure in the same compartment. Most surgical scopes carry 90-day global periods. Compartment and structure details drive correct coding.
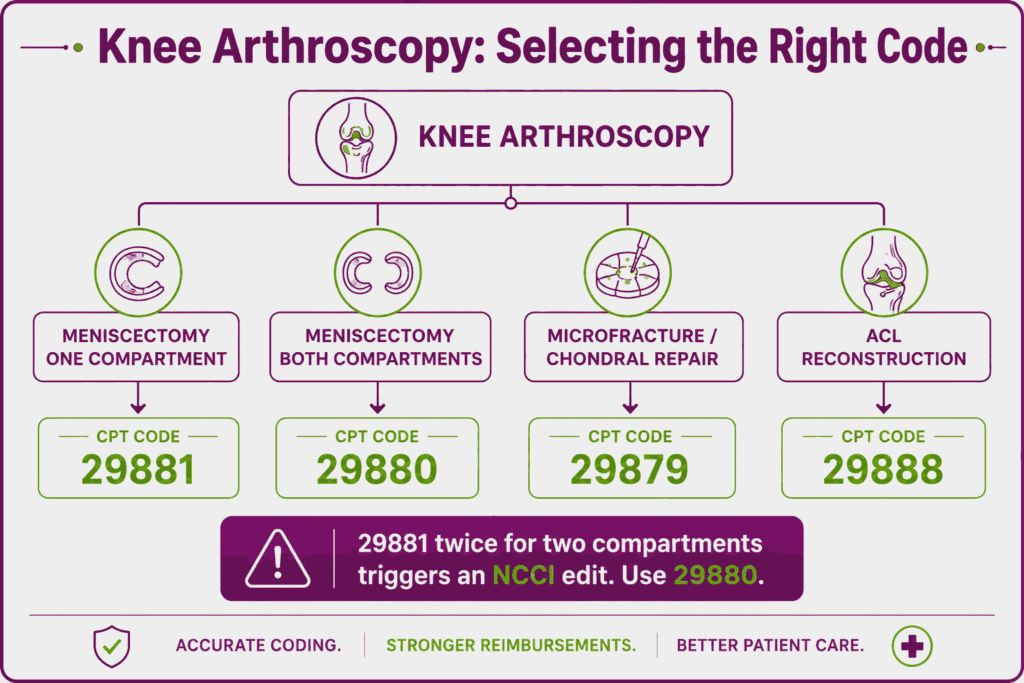
CPT 29881: Knee Arthroscopy With Meniscectomy
CPT 29881 reports knee arthroscopy with meniscectomy in one compartment, medial or lateral. The procedure code 29881 description includes any shaving, debridement, or chondroplasty performed in that same compartment. Reporting a separate debridement code for the treated compartment triggers an NCCI edit. Document which compartment was addressed.
CPT 29880: Knee Arthroscopy, Medial and Lateral Meniscectomy
CPT 29880 reports meniscectomy in both the medial and lateral compartments of the same knee. Use the 29880 CPT instead of reporting 29881 twice, which is a frequent unbundling error. The note must confirm that both compartments were treated. Debridement in either compartment is included.
CPT 29879: Knee Arthroscopy With Microfracture or Abrasion
CPT 29879 reports arthroscopic abrasion arthroplasty or microfracture for a chondral defect. Documentation should record the lesion location and the chondral grade addressed. When performed with a meniscectomy in the same compartment, bundling rules apply to CPT code 29879. Confirm a distinct compartment before separate reporting.
CPT 29888: Arthroscopically Aided ACL Reconstruction
CPT 29888 reports anterior cruciate ligament reconstruction performed with arthroscopic assistance. The operative note must record the graft type and the fixation method. 29888 procedure code carries a 90-day global period. Concurrent meniscal work may be separately reportable when performed in a distinct compartment.
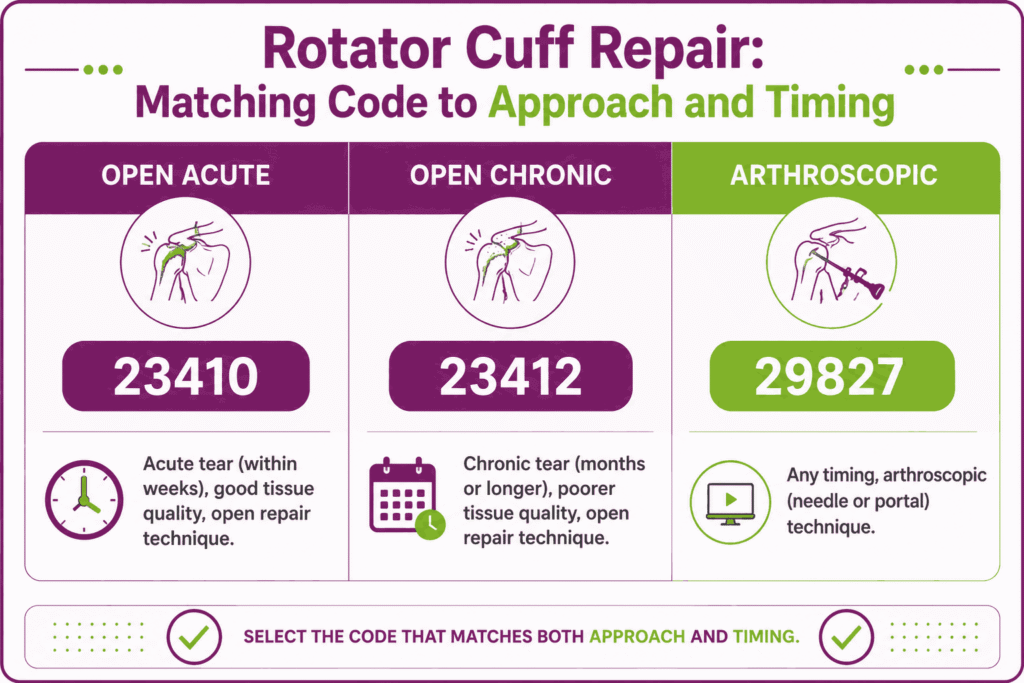
CPT 29827: Shoulder Arthroscopy With Rotator Cuff Repair
CPT 29827 reports arthroscopic rotator cuff repair and is the highest-volume shoulder scope. Documentation must record the tear size and the repair construct. A subacromial decompression performed in the same session is reported with add-on 29826, not separately as a base code. Tear chronicity supports medical necessity.
CPT 29807: Arthroscopic SLAP Repair
CPT 29807 reports arthroscopic repair of a superior labrum anterior-posterior (SLAP) lesion. The note must document the labral pathology and anchor placement. When billed with other shoulder procedures, verify NCCI edits. Distinct structures must be documented to support separate codes.
CPT 29916: Hip Arthroscopy With Labral Repair
CPT 29916 reports hip arthroscopy with labral repair. Payer coverage varies, and prior authorization is common. Document the labral tear and the repair technique. Confirm the coverage policy before the procedure to prevent a medical-necessity denial.
CPT 29898: Ankle Arthroscopy, Debridement
CPT 29898 reports ankle arthroscopy with extensive debridement. The note must specify the extent of synovectomy or debridement performed, since a limited debridement uses a different code. Append RT or LT. Document the structures addressed.
CPT 29880 vs 29881: How Does Compartment Count Change the Code?
Compartment count sets the code. CPT 29881 reports meniscectomy in one compartment, medial or lateral. CPT 29880 reports both compartments in the same knee. A common unbundling error is reporting 29881 twice for a two-compartment case. Use 29880 instead, since 29881 reported twice will trigger an NCCI edit.
Which CPT Codes Cover Fracture Treatment and Fixation?
Fracture codes organize by anatomic region, treatment type, and whether fixation was used. Open treatment codes carry 90-day global periods. Every claim needs laterality and a diagnosis that supports the specific fracture site.
CPT 27236: Femoral Neck Fracture, Open Treatment
CPT 27236 reports open treatment of a femoral neck fracture, by either internal fixation or prosthetic replacement. The note must state which method was used, since both fall under the same code. Append RT or LT. Document the fracture pattern and reduction.
CPT 27244: Intertrochanteric Fracture, Plate and Screw
CPT 27244 reports open treatment of an intertrochanteric or subtrochanteric fracture using a plate and screw construct, such as a sliding hip screw. Document the implant and the reduction. A different code applies when an intramedullary nail is used instead.
CPT 27245: Intertrochanteric Fracture, Intramedullary Nail
CPT 27245 reports the same fracture treated with an intramedullary implant. The note must record the nail type and interlocking screws. Selecting between 27244 and 27245 depends entirely on the construct, not the fracture severity. Match the code to the hardware documented.
CPT 27758: Tibial Shaft Fracture, Open With Plate
CPT 27758 reports open treatment of a tibial shaft fracture with plate and screw fixation. Documentation must specify the fixation hardware and the reduction method. It carries a 90-day global period. Append RT or LT for laterality.
CPT 27759: Tibial Shaft Fracture, Intramedullary Nail
CPT 27759 reports tibial shaft fracture treatment using an intramedullary nail. Document reaming and the interlocking screws placed. As with the femur, the implant type, not the fracture, selects the code. Confirm the construct in the operative note.
CPT 27766: Medial Malleolus Fracture, Open Treatment
CPT 27766 reports open treatment of a medial malleolus fracture. The note must document the fixation hardware and laterality. When multiple malleoli are involved, a combined ankle fracture code applies instead. Confirm which malleoli were treated.
CPT 27814: Bimalleolar Ankle Fracture, Open Treatment
CPT 27814 reports open treatment of a bimalleolar ankle fracture. Document both malleoli and the fixation used on each. Reporting separate single-malleolus codes for the same ankle is an unbundling error. Use the combined code.
CPT 27822: Trimalleolar Ankle Fracture, Open Treatment
CPT 27822 reports open treatment of a trimalleolar fracture, including the posterior lip of the tibia. The note must document posterior fixation when performed. The code captures all three malleoli in one report. Append laterality.
CPT 25607, 25608, 25609: Distal Radius Fracture, Open Treatment
These codes report open treatment of a distal radius fracture by fragment count. CPT 25607 covers extra-articular fixation, 25608 covers a two-fragment intra-articular fracture, and 25609 covers three or more fragments. Document the fragment count, since it is the sole code selector. Append RT or LT.
CPT 23615: Proximal Humerus Fracture, Open With Fixation
CPT 23615 reports open treatment of a proximal humerus fracture with internal fixation. The note must document surgical or anatomical neck involvement. Append laterality. A non-fixation treatment uses a separate code.
CPT 20690 and 20692: External Fixation Systems
CPT 20690 reports application of a uniplane external fixation system, and 20692 reports a multiplane or ring system. Both are reported with the fracture treatment code, not as standalone services. Document the frame type. The fixator application supports separate reporting only per payer rule.
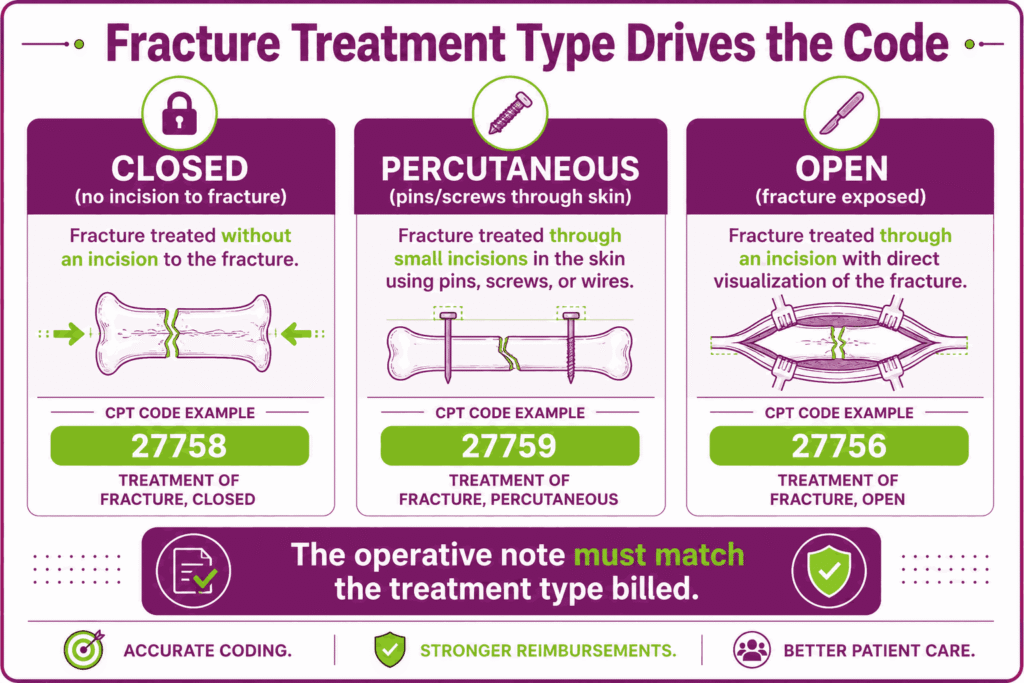
Closed vs Open vs Percutaneous: How Does Treatment Type Drive the Code?
Treatment type is the primary code selector, not fracture severity. Closed treatment means no surgical incision to the fracture. Percutaneous fixation places pins or screws through the skin. Open treatment exposes the fracture directly. The operative note must match the code, since payers audit treatment type against the procedure description.
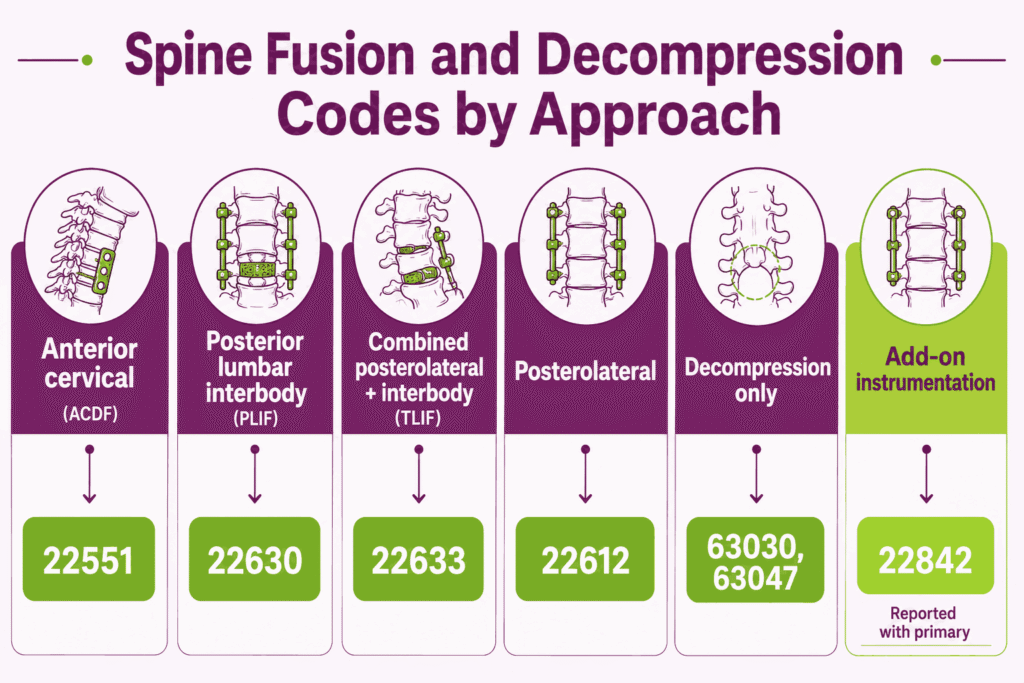
Which CPT Codes Cover Spine Procedures?
Spine codes separate by approach, vertebral level, and whether decompression or fusion was performed. Instrumentation and interbody devices add separate codes. Orthopedic spine surgeons share several of these codes with neurosurgery, so documentation of the exact levels is essential.
CPT 63030: Lumbar Laminotomy and Decompression
CPT 63030 reports a lumbar laminotomy with decompression of a nerve root at one interspace. The note must record the level and the side decompressed. Each additional interspace uses an add-on code. Vague level documentation cannot support multi-level billing.
CPT 63047: Lumbar Laminectomy and Facetectomy
CPT 63047 reports lumbar laminectomy, facetectomy, and foraminotomy at a single segment. Document the nerve roots decompressed and the segment treated. It differs from 63030 in the extent of bone and facet removal. Match the code to the decompression performed.
CPT 22551: Anterior Cervical Discectomy and Fusion (ACDF)
CPT 22551 reports an anterior cervical discectomy with arthrodesis at a single interspace below C2. Each additional level uses add-on 22552. The note must document the interspace and the fusion technique. It carries a 90-day global period.
CPT 22630: Lumbar Posterior Interbody Fusion (PLIF)
CPT 22630 reports lumbar posterior interbody arthrodesis at one interspace. Document the interbody device and the bone graft used. When combined with a posterolateral fusion through one approach, the combined code applies instead. Do not unbundle the components.
CPT 22633: Combined Posterolateral and Interbody Fusion (TLIF)
CPT 22633 reports a combined posterolateral and posterior interbody fusion performed through a single approach at one interspace. Reporting 22630 and 22612 separately for the same level and approach is an unbundling error. Use the combined code. Document both fusion elements.
CPT 22612: Posterolateral Lumbar Arthrodesis
CPT 22612 reports a posterolateral lumbar fusion at a single level. The note must record the bone graft source and any instrumentation. Instrumentation is reported with a separate add-on code. Document the level treated.
CPT 22842: Posterior Segmental Instrumentation
CPT 22842 reports posterior segmental instrumentation spanning three to six vertebral segments. It is an add-on code, reported with the primary fusion procedure. It cannot stand alone. Document the segments instrumented.
How Do Vertebral Level and Approach Change Spine Coding?
Each interspace and each approach changes the code. A single-level fusion and a two-level fusion use different add-on codes. Anterior and posterior approaches carry separate base codes, even at the same level. Document the exact levels treated, since vague language like “lumbar fusion” cannot support multi-level billing.
Managing these intricate software rules is significantly easier when leveraging the top EMRs for Orthopedic billing built to catch multi-level formatting.
Which CPT Codes Cover Hand and Wrist Procedures?
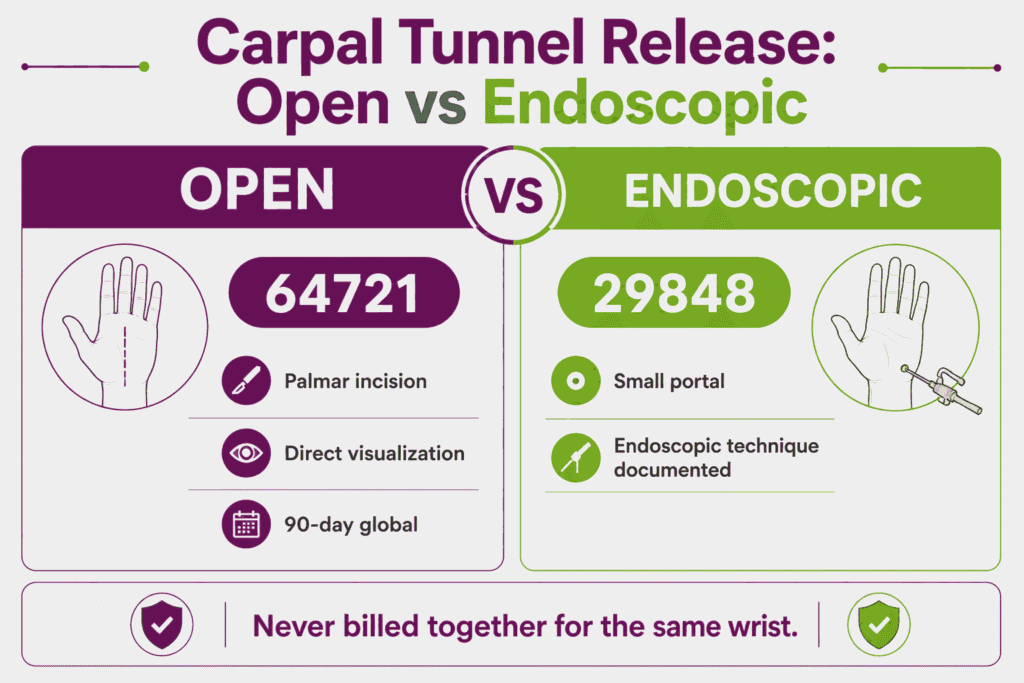
Hand and wrist work is a high-volume orthopedic subspecialty. Many codes carry digit-specific or laterality requirements. Carpal tunnel release is the most common, split by open versus endoscopic technique.
CPT 64721: Open Carpal Tunnel Release
CPT 64721 reports an open carpal tunnel release, a neuroplasty of the median nerve through a palmar incision. It carries a 90-day global period. Append RT or LT. Document the clinical findings and any electrodiagnostic confirmation that supports the necessity.
CPT 29848: Endoscopic Carpal Tunnel Release
CPT 29848 reports an endoscopic carpal tunnel release through a small portal. The note must specify the endoscopic technique, since that is the only basis separating it from 64721. The two are never billed together for the same wrist. Append laterality.
CPT 26055: Trigger Finger Release
CPT 26055 reports a tendon sheath incision for trigger finger release. Document the specific digit treated. Multiple digits on the same hand may require distinct reporting with appropriate modifiers. Confirm payer rules for same-session multiple releases.
CPT 25111: Ganglion Cyst Excision, Wrist
CPT 25111 reports excision of a primary wrist ganglion cyst. Use 25112 for a recurrent ganglion. The note must record whether the cyst is primary or recurrent. Append laterality.
CPT 26600 and 26720: Metacarpal and Phalangeal Fracture, Closed
CPT 26600 reports closed treatment of a metacarpal fracture, and 26720 reports closed treatment of a phalangeal shaft fracture, each without manipulation. Document the bone, the digit, and the manipulation status. Manipulation moves the claim to a different code.
CPT 26356: Flexor Tendon Repair, Zone 2
CPT 26356 reports primary flexor tendon repair in zone 2, with or without a graft, for a single tendon. The note must document the zone and each tendon repaired. Zone 2 repairs carry specific rehabilitation documentation expectations. Report each tendon distinctly.
CPT 64721 vs 29848: Open Versus Endoscopic Carpal Tunnel?
Technique sets the code. CPT 64721 reports an open release through a palmar incision. CPT 29848 reports an endoscopic release through a small portal. The two are never billed together for the same wrist. Document the technique used, since the descriptor difference is the only basis for code selection.
Which CPT Codes Cover Tendon and Ligament Repair?
Tendon repair codes separate by anatomic location and timing. Acute and chronic repairs of the same tendon use different codes. Most carry 90-day global periods, and chronicity must appear in the note.
CPT 27650 and 27654: Achilles Tendon Repair
CPT 27650 reports a primary repair of an acute Achilles tendon rupture, and 27654 reports a secondary repair, such as for a chronic or re-ruptured tendon. The note must document the injury timing and the repair technique. Append RT or LT.
CPT 23410: Rotator Cuff Repair, Open, Acute
CPT 23410 reports an open repair of an acute rotator cuff tear. Use it when the tear is repaired soon after injury. The operative note must support the acute timing. Coding acute as chronic, or the reverse, is a frequent denial trigger.
CPT 23412: Rotator Cuff Repair, Open, Chronic
CPT 23412 reports an open repair of a chronic rotator cuff tear, where the tendon has retracted or degenerated. The note must state chronicity to support the code. Document tear size and tissue quality. This is the open counterpart to arthroscopic code 29827.
CPT 23430: Biceps Tenodesis
CPT 23430 reports a biceps tenodesis. It is often performed with a rotator cuff repair, so verify NCCI bundling before separate reporting. Document the tenodesis as a distinct procedure when separately billed. Confirm a distinct indication.
CPT 27380 and 27385: Patellar and Quadriceps Tendon Repair
CPT 27380 reports a primary patellar tendon repair, and 27385 reports a primary quadriceps or hamstring muscle repair. The note must distinguish primary repair from reconstruction. Append laterality. Reconstruction with a graft uses a separate code.
CPT 23410 vs 23412: Acute Versus Chronic, Where Is the Line?
Timing and tissue quality set the code. CPT 23410 reports an acute repair, generally within weeks of injury. CPT 23412 reports a chronic repair where the tendon has retracted or degenerated. The operative note must state chronicity. Coding chronic as acute, or the reverse, is a common downcoding and denial trigger.
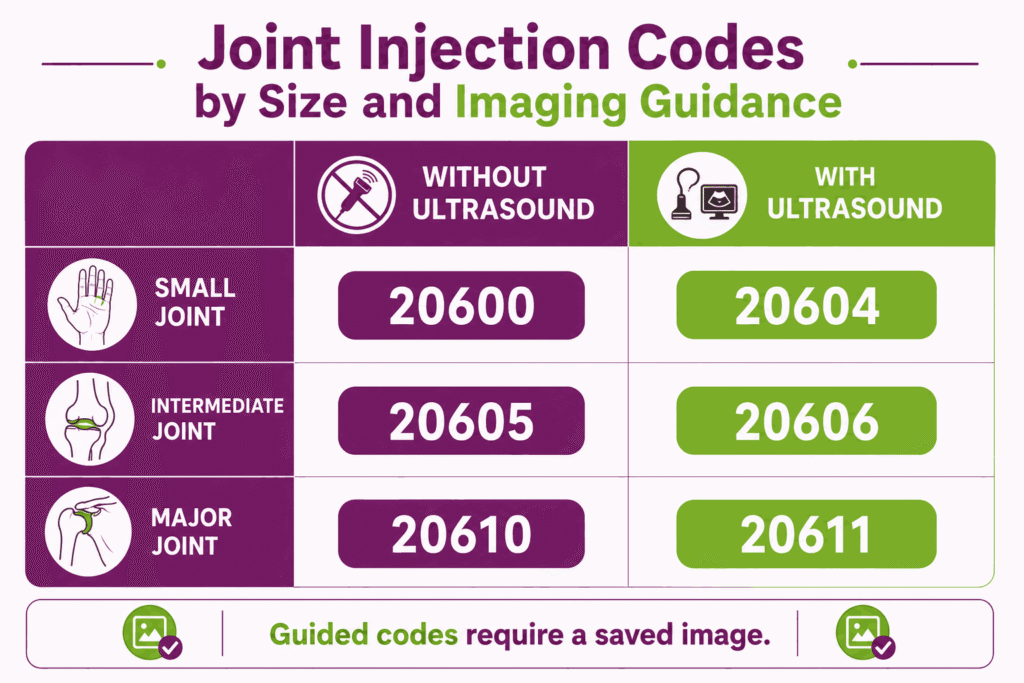
Which CPT Codes Cover Joint and Soft-Tissue Injections?
Injection codes split by joint size and whether imaging guidance was used. Image-guided codes pay more and require a saved imaging record. Modifier 25 applies when a separate E/M is billed the same day. All carry 0-day global periods.
CPT 20610 and 20611: Major Joint Injection or Aspiration
CPT 20610 reports a major joint injection or aspiration by landmark, such as the knee, hip, or shoulder. CPT 20611 reports the same with ultrasound guidance and a permanent recorded image. The image must be saved to support 20611. Document the joint, the drug, and the NDC.
CPT 20605 and 20606: Intermediate Joint Injection
CPT 20605 reports an intermediate joint injection, such as the wrist, elbow, or ankle, and 20606 reports the same with ultrasound guidance. The note must record the joint and the guidance method. A saved image supports the guided code. Append modifier 25 for a same-day separate E/M.
CPT 20600 and 20604: Small Joint Injection
CPT 20600 reports a small joint injection, such as a finger or toe joint, and 20604 reports the same with ultrasound guidance. Document the specific joint and the substance injected. The guided code requires a permanent image. Confirm medical necessity for the injection.
CPT 20550: Tendon Sheath or Ligament Injection
CPT 20550 reports an injection into a single tendon sheath or ligament. Document the anatomic site, the drug, and the NDC. Multiple sites need the modifier 59 or an X-modifier. It differs from a tendon origin injection.
CPT 20551: Tendon Origin or Insertion Injection
CPT 20551 reports an injection at the origin or insertion of a tendon, not the sheath. The note must identify the specific target. It is often confused with 20550, so the documented site must match the code. Confirm the anatomic detail.
CPT 20552 and 20553: Trigger Point Injection
CPT 20552 reports trigger point injection into one or two muscles, and 20553 reports three or more muscles. The code reflects muscle count, not the number of injections. Document each muscle treated. Append modifier 25 when a separate E/M occurs the same day.
When Does Imaging Guidance Change the Injection Code?
Imaging guidance changes the code and the payment. CPT 20610 reports a major joint injection by landmark. CPT 20611 reports the same joint with ultrasound and a saved image. The reimbursement gap is significant, and 20611 is often underused when an ultrasound was performed but not documented. Save the image to support the higher code.
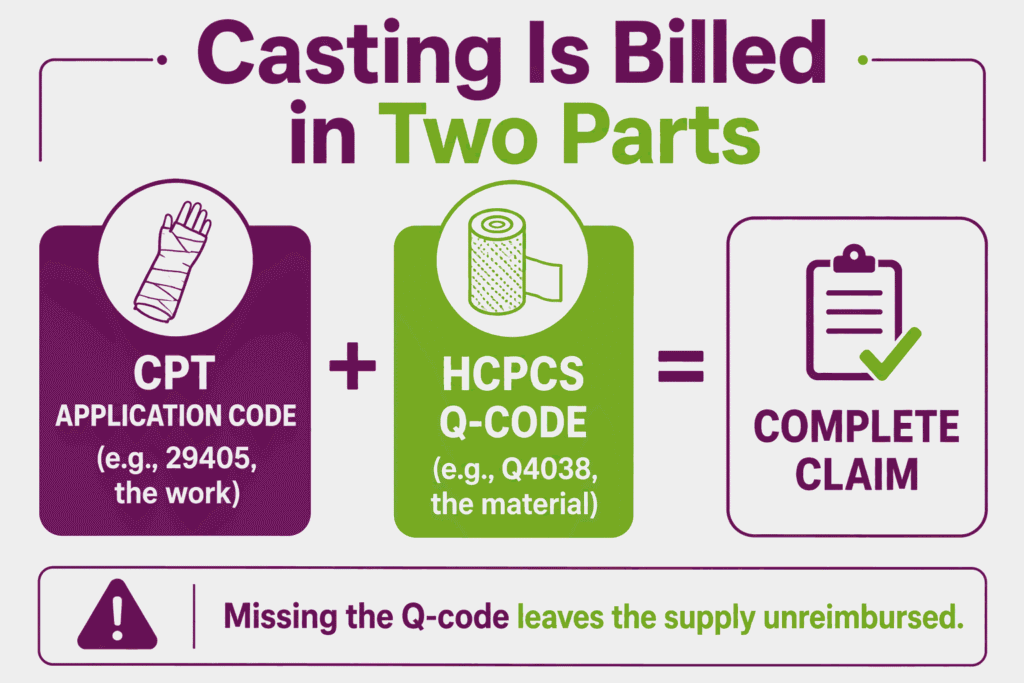
Which CPT Codes Cover Casting, Splinting, and Strapping?
Application codes cover the initial cast or splint placement. They carry 0-day global periods and are billed separately from the supply. Cast supplies are reported under HCPCS Q-codes, which is the step most often missed.
CPT 29405: Short Leg Cast, Non-Weightbearing
CPT 29405 reports application of a short leg cast from below the knee to the toes. Append RT or LT. The cast supply is billed separately under a Q-code. Document the clinical indication for immobilization.
CPT 29425: Short Leg Walking Cast
CPT 29425 reports a short leg walking cast. The note must document weight-bearing status, which distinguishes it from 29405. Append laterality. Bill the supply separately.
CPT 29345: Long Leg Cast
CPT 29345 reports the application of a long leg cast from the thigh to the toes. Document the anatomic extent and the indication. Append laterality. The material is billed under a separate Q-code.
CPT 29515: Short Leg Splint
CPT 29515 reports the application of a short leg splint, common for an acute ankle injury before definitive care. Document the position and indication. Append RT or LT. A splint and a later cast are separately reportable when clinically staged.
CPT 29125 and 29126: Short Arm Splint
CPT 29125 reports a static short arm splint, and 29126 reports a dynamic one. The note must specify static versus dynamic, which is the code selector. Append laterality. Bill the supply separately.
CPT 29105: Long Arm Splint
CPT 29105 reports the application of a long arm splint. Document the anatomic position and clinical indication. Append laterality. The supply is reported under a separate Q-code.
How Are Cast Supplies (Q-Codes) Billed Separately From Application?
Application and supply are two separate charges. The CPT application code, such as 29405, covers the work of placing the cast. The HCPCS Q-code, such as Q4038, covers the cast material itself. Bill both lines when you apply the cast. Missing the Q-code leaves the supply cost unreimbursed.
Which CPT Codes Cover Hardware Removal and Manipulation?
Hardware removal and manipulation codes often fall inside a prior procedure’s global period. When they do, a modifier is required to separate them from the original surgery.
CPT 20680: Deep Implant Removal
CPT 20680 reports the removal of a deep or buried orthopedic implant, such as a plate, screw, or rod. It carries a 90-day global period. When performed inside another procedure’s global window, append modifier 79 for an unrelated procedure or 58 for a staged one. Document the implant removed.
CPT 20670: Superficial Implant Removal
CPT 20670 reports the removal of a superficial implant, such as a pin or wire. The note must document depth to justify 20670 over 20680. Append laterality. Depth is the code selector.
CPT 27570: Knee Manipulation Under Anesthesia
CPT 27570 reports manipulation of a knee under anesthesia, often for arthrofibrosis after surgery. Document the range of motion before and after the manipulation. When performed in the prior surgery’s global period, append the appropriate global-period modifier.
CPT 20680 in the Global Period: When Does Modifier 79 Apply?
Modifier 79 applies when the removal is unrelated to the current global period. Hardware placed during a fracture repair often comes out months later, inside or outside that 90-day window. If removal falls in the original global period and is a planned later stage, modifier 58 may apply instead. Document the timing and intent clearly.
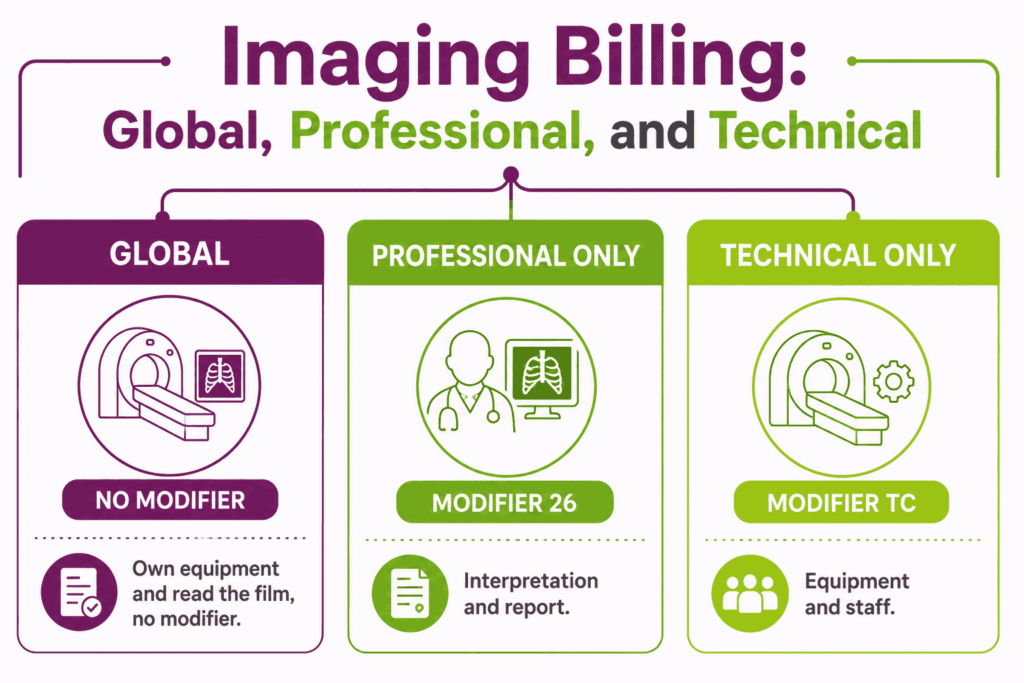
Which CPT Codes Cover In-House Orthopedic Imaging?
Orthopedic groups bill X-rays in-house constantly. When the practice owns the equipment and reads the film, it bills globally. When the components split between entities, modifiers 26 and TC apply.
CPT 73560, 73562, 73564: Knee X-Ray
These codes report a knee X-ray by the number of views. CPT 73560 covers one or two views, 73562 covers three views, and 73564 covers four or more views, a complete study. Document the views obtained, since the count selects the code. Billing a higher view code without the images is an audit risk.
CPT 73610: Ankle X-Ray, Complete
CPT 73610 reports a complete ankle X-ray of at least three views. Document the views performed. Append laterality where the payer requires it. A two-view study uses a different code.
CPT 73130: Hand X-Ray
CPT 73130 reports a hand X-ray of a minimum of three views. Document the views obtained. Confirm laterality per payer rule. Fewer views move the claim to a different code.
CPT 73110: Wrist X-Ray, Complete
CPT 73110 reports a complete wrist X-ray of at least three views. The note should record the views and the clinical indication. A two-view wrist study uses 73100 instead. Match the code to the documented views.
CPT 72100 and 72110: Lumbar Spine X-Ray
CPT 72100 reports a lumbar spine X-ray of two or three views, and 72110 reports a complete study of four or more views. Document the view count, which is the code selector. The complete study requires additional views in the record.
CPT 73721 and 73221: MRI, Lower and Upper Extremity Joint
CPT 73721 reports an MRI of a lower extremity joint without contrast, and 73221 reports an upper extremity joint MRI without contrast. Procedure code 73721 commonly requires prior authorization, as is the case for CPT 73221. Document the joint and the clinical question. Contrast studies use separate codes.
How Do Modifiers 26 and TC Split the Professional and Technical Components?
Modifiers 26 and TC divide a diagnostic service into two billable parts. Modifier 26 reports the physician’s interpretation and written report only. Modifier TC reports the equipment, supplies, and technical staff. A practice that owns the machine and reads the film bills globally, with no modifier. Use 26 or TC only when the components split between entities.
Which Evaluation and Management Codes Do Orthopedic Practices Use?
Orthopedic practices bill heavy office-visit volume alongside procedures. E/M level selection uses medical decision-making or total time. Same-day procedures require modifier 25 on the E/M.
CPT 99202 to 99205: New Patient Visits
These codes report new patient office visits, leveled by medical decision-making or total time on the date of service. A new patient has not been seen by the same specialty in the group within three years. Document the elements that support the selected level. Misclassifying an established patient as new is a common error.
CPT 99211 to 99215: Established Patient Visits
These codes report established patient visits, where 99211 needs no provider presence, and 99215 reflects high complexity. Level selection follows MDM or total time. Document the problems addressed and the data reviewed. Most orthopedic follow-ups land at 99213 or 99214.
CPT 99024: Post-Operative Visit in the Global Period
CPT 99024 reports a post-operative visit during the global period at no charge. It documents the encounter for utilization tracking, which the OIG global surgery audit examined directly. Report it for in-window post-op visits. It carries no separate payment.
CPT 99213 vs 99214: Where Do Most Orthopedic Visits Land?
Most orthopedic visits land between 99213 and 99214 on decision complexity. A 99213 fits a stable follow-up, such as a healing fracture check. A 99214 fits moderate complexity, such as a new injury, an injection decision, or surgical planning. When MDM is borderline, total time can support the higher level if documented.
Which Modifiers Are Most Used in Orthopedic Billing?
Orthopedic modifiers are among the most audited in surgery. A wrong or missing one changes the payment outright. The groups below carry the highest claim impact.
Which Modifiers Handle Laterality and Bilateral Procedures?
Laterality modifiers are mandatory on most orthopedic procedures. Many payers reject claims that omit them.
- RT and LT: identify the right or left side on a unilateral procedure
- 50: reports the same procedure performed bilaterally in one session
- Payer rules vary on whether to use 50 or separate RT and LT lines
Which Modifiers Distinguish Services During the Global Period?
Global period modifiers separate later services from the original surgical package. Each one signals a different relationship to the first procedure.
| Modifier | Meaning | When to Use |
|---|---|---|
| 24 | Unrelated E/M in postop period | Visit for a condition unrelated to the surgery |
| 58 | Staged or related procedure | Planned later stage or a more extensive procedure |
| 78 | Return to OR for a complication | Unplanned return treating a surgical complication |
| 79 | Unrelated procedure in postop period | A separate procedure during the global window |
Which Modifiers Cover Distinct and Multiple Procedures?
Distinct-service modifiers override NCCI bundling edits when procedures are genuinely separate. CMS prefers the specific X-modifiers over the broad 59.
- 59: distinct procedural service, used only with documentation
- XE, XS, XP, XU: specific alternatives for separate encounter, structure, practitioner, or service
- 51: multiple procedures in one session, not used on add-on codes
Which Modifiers Address Complexity, Assistance, and Same-Day E/M?
These modifiers report extra work, surgical assistance, or a separate visit. Each needs supporting documentation in the record.
| Modifier | Meaning | When to Use |
|---|---|---|
| 22 | Increased procedural complexity | Substantially greater work; needs an operative note |
| 25 | Separate, identifiable E/M | E/M distinct from a same-day procedure |
| 57 | Decision for major surgery | E/M where the surgical decision was made |
| 62 | Two surgeons | Each co-surgeon performs a distinct part |
| 80, AS | Surgical assistant | 80 for a physician, AS for a PA, NP, or CNS |
What Are the Global Surgical Periods for Common Orthopedic Procedures?
The global period sets how long post-procedure services bundle into the original payment. Orthopedics is a global-period heavy, since most surgical codes carry 90 days. This is what makes the 24, 58, 78, and 79 modifiers actionable.
| Global Period | Procedure Category | Representative Codes |
|---|---|---|
| 90 Days | Joint replacement and revision | 27447, 27130, 23472, 27487 |
| Open fracture treatment | 27236, 27244, 27758, 25607 | |
| Surgical arthroscopy | 29881, 29827, 29888 | |
| Spine fusion and decompression | 22551, 22630, 63030 | |
| Tendon and cuff repair | 27650, 23410 | |
| Carpal tunnel and hardware removal | 64721, 20680 | |
| 10 Days | Minor hand procedures | 26055, 25111 |
| 0 Days | Joint and trigger point injections | 20610, 20605, 20552 |
| In-house imaging | 73564, 73610, 73721 | |
| Office visits and casting | 99213, 29405, 29515 |
Confirm exact global days in the CMS Physician Fee Schedule, since assignment can change by code and year. Hence, you must fully understand the orthopedic medical billing workflow context for managing these periods.
What Are the Most Common Orthopedic Coding Errors and Denial Reasons?
Most orthopedic denials trace to a small set of recurring errors. Each has a known fix. The patterns below appear most often in payer and federal audits.
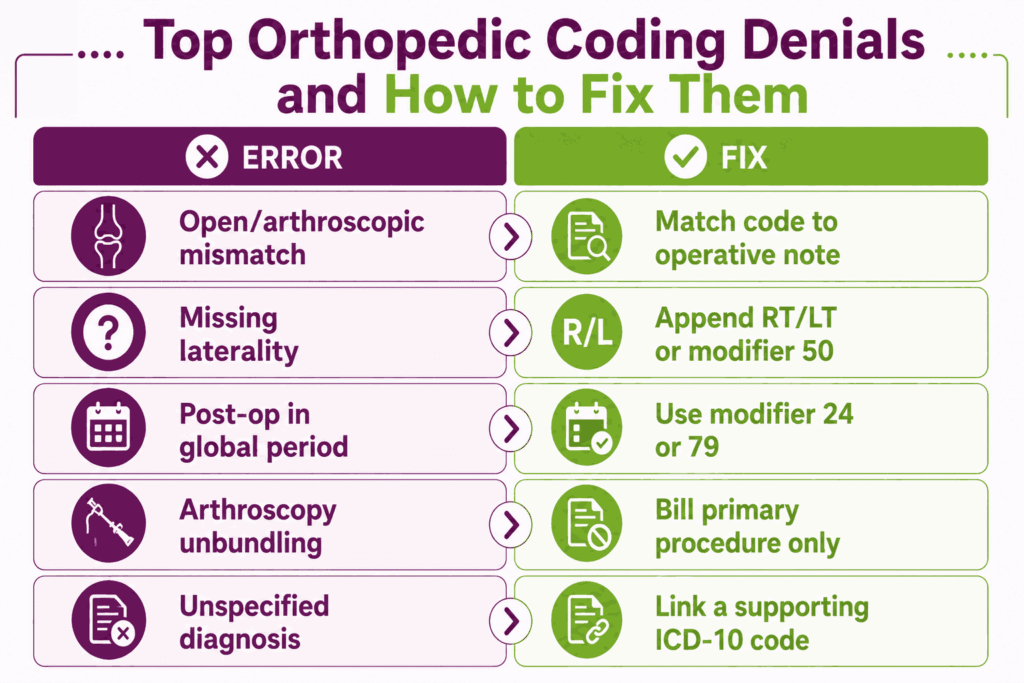
Open Versus Arthroscopic Code Mismatch With the Operative Note
The Error: Billing an open code when the surgeon performed an arthroscopic procedure, or the reverse. The descriptor must match the technique documented.
Fix: Read the operative note before coding. Confirm the approach, then select the matching code family. Because these distinctions are heavily audited, many practices hand off this complex oversight to the top companies specializing in orthopedic billing to prevent costly upcoding denials.
Missing Laterality or Bilateral Modifier
The Error: Submitting a procedure on a paired structure without RT, LT, or 50. Automated scrubbers reject these instantly.
Fix: Append RT or LT on every unilateral limb procedure. Use modifier 50 or separate lines for bilateral cases per payer rule.
Billing Post-Op Services Inside the 90-Day Global Period
The Error: Charging follow-up visits or related procedures inside another procedure’s global window without a modifier. Payers bundle them into the original payment.
Fix: Use modifier 24 for unrelated E/M and 79 for unrelated procedures. Document why the service is unrelated.
Unbundling Arthroscopy or Fracture Components Against NCCI Edits
The Error: Reporting the diagnostic scope or a bundled component separately from the primary procedure. This violates NCCI edits.
Fix: Bill the primary surgical code only. Append modifier 59 or an X-modifier only when a genuinely distinct service is documented.
Reporting a Second Base Code Instead of an Add-On
The Error: Using a second base code for additional levels or vessels that require an add-on code. The claim is denied or reduced.
Fix: Apply the correct add-on code, such as 22842, for additional spine instrumentation. Add-on codes cannot stand alone.
Modifier 59 Overuse Without a Distinct Service
The Error: Appending modifier 59 to bypass a bundling edit without a clinically distinct service. The 2026 OIG Work Plan flags modifier 59 overuse on musculoskeletal procedures as an audit focus.
Fix: Use 59 only with documentation of a separate site, encounter, or session. Prefer the specific X-modifiers when they apply.
Missing or Unspecified Diagnosis Breaking Medical Necessity
The Error: Submitting a procedure without a diagnosis that supports it, or using an unspecified code. Medical necessity fails, and the claim denies.
Fix: Link every CPT code to a supporting diagnosis. For correct pairing, see the companion orthopedic ICD-10 codes guide.
What Are the 2026 CPT Code Updates Affecting Orthopedics?
The CPT 2026 code set took effect January 1, 2026. It carries 418 total changes: 288 new codes, 46 revisions, and 84 deletions (American Medical Association, 2025). Most core orthopedic codes for arthroplasty, arthroscopy, fracture care, and E/M were unchanged.
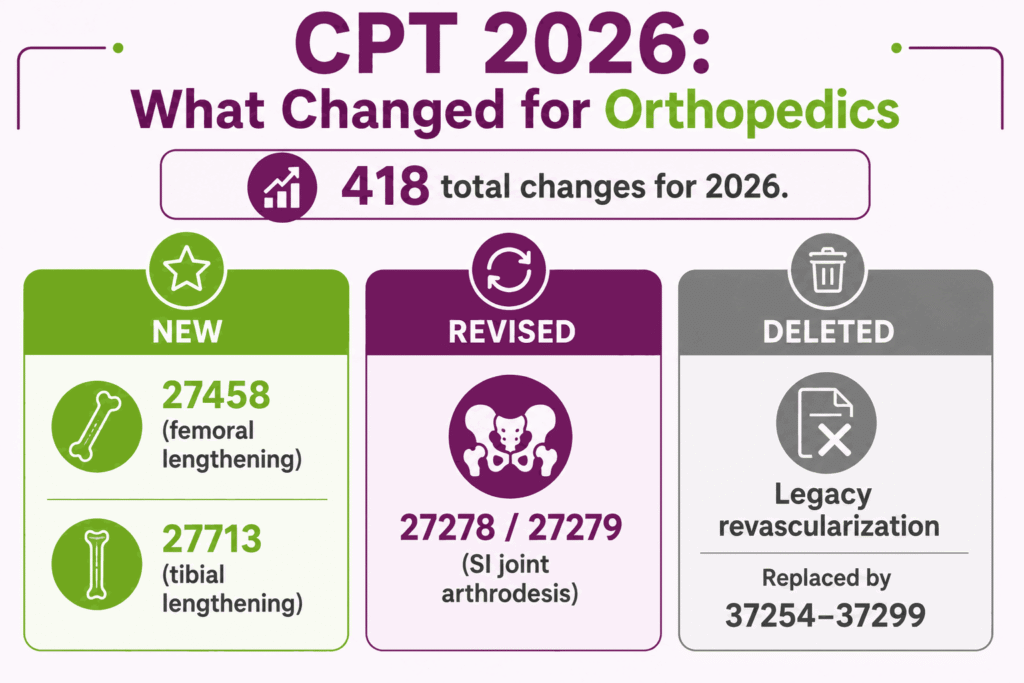
New Codes
The musculoskeletal section added two limb-lengthening reconstruction codes (AAPC, 2025).
- CPT 27458: unilateral femoral osteotomy with an externally controlled intramedullary lengthening device
- CPT 27713: unilateral tibial osteotomy with the same lengthening device
- CPT 99445: remote physiologic monitoring device supply for 2 to 15 days, useful for post-operative tracking
- CPT 99470: first 10 minutes of remote physiologic monitoring treatment management
Revised Codes
Sacroiliac joint arthrodesis coding was refined for the current surgical technique.
- CPT 27278 and 27279: SI joint arthrodesis language and parenthetical notes revised to reflect hybrid fusion constructs that combine percutaneous implants with decortication or grafting
- CPT 99453 and 99454: remote physiologic monitoring descriptors revised for shorter monitoring periods
Deleted Codes
The lower extremity revascularization family was rebuilt, which affects practices billing for peripheral vascular work.
- Legacy revascularization codes were deleted and replaced by 46 territory-based codes (37254 to 37299)
- Verify any deleted code against the AMA CPT 2026 Professional Edition before remapping claims
Orthopedic CPT Codes: Frequently Asked Questions
What Are the Most Common Orthopedic CPT Codes?
The highest-volume codes include 20610 for a major joint injection, 27447 for total knee arthroplasty, and 29881 for knee arthroscopy with meniscectomy. Office visit codes 99213 and 99214 also rank near the top. Exact volume varies by subspecialty and patient mix.
What Is the CPT Code for a Total Knee Replacement?
CPT 27447 reports a total knee arthroplasty, covering the medial and lateral compartments with or without patellar resurfacing. It carries a 90-day global period. Bilateral procedures in the same session use modifier 50.
How Do You Code Bilateral Orthopedic Procedures?
Use modifier 50 to report the same procedure on both sides in one session. Some payers require two separate lines with RT and LT instead. Check the specific payer rule, since reimbursement and formatting differ.
Do Arthroscopy Codes Include Debridement?
Yes, debridement in the same compartment is bundled into the arthroscopy code. For example, 29881 includes shaving and debridement of the treated meniscus. Billing a separate debridement code for the same compartment triggers an NCCI edit.
What Modifier Is Used for a Staged Procedure During the Global Period?
Modifier 58 reports a staged or planned procedure during another procedure’s global period. It applies when the second procedure was anticipated or is more extensive. Modifier 58 also starts a new global period for the staged service.
How Are Cast and Splint Supplies Billed?
Cast application and cast supply are billed separately. The CPT application code covers the work, and an HCPCS Q-code covers the material. Report both lines at the time of application to capture the full charge.






