
CPT code 27130 reports a primary total hip arthroplasty, the first-time replacement of both the acetabular socket and the proximal femur with prosthetic components. It is one of the highest-volume major procedures in orthopedic surgery.
CPT 27130 is restricted to first-time hip replacement. Any prior surgery on the same hip moves the case to the conversion code, and mixing the primary, conversion, and revision codes is the most flagged error in hip arthroplasty audits.
The code also sits inside the new mandatory TEAM episode model, which changes how Medicare reconciles payment at participating hospitals. Many orthopedic groups route joint replacement claims through expert orthopedic billing services to manage these controls.
What Is the Description of CPT Code 27130?
The 27130 CPT code description as defined by the AMA is: “Arthroplasty, acetabular and proximal femoral prosthetic replacement (total hip arthroplasty), with or without autograft or allograft.”
This code reports a first-time total hip replacement, in which the surgeon replaces both the acetabular socket and the proximal femur with prosthetic components. CPT code 27130 includes any bone graft used during the procedure, whether autograft or allograft, so graft work never generates a separate line.
The procedure treats end-stage hip disease when the joint surface is destroyed. Procedure code 27130 applies only to a primary total hip arthroplasty, distinct from partial replacement, conversion, and revision surgery.
What Prosthetic Components Define CPT Code 27130 as a Total Hip Arthroplasty?
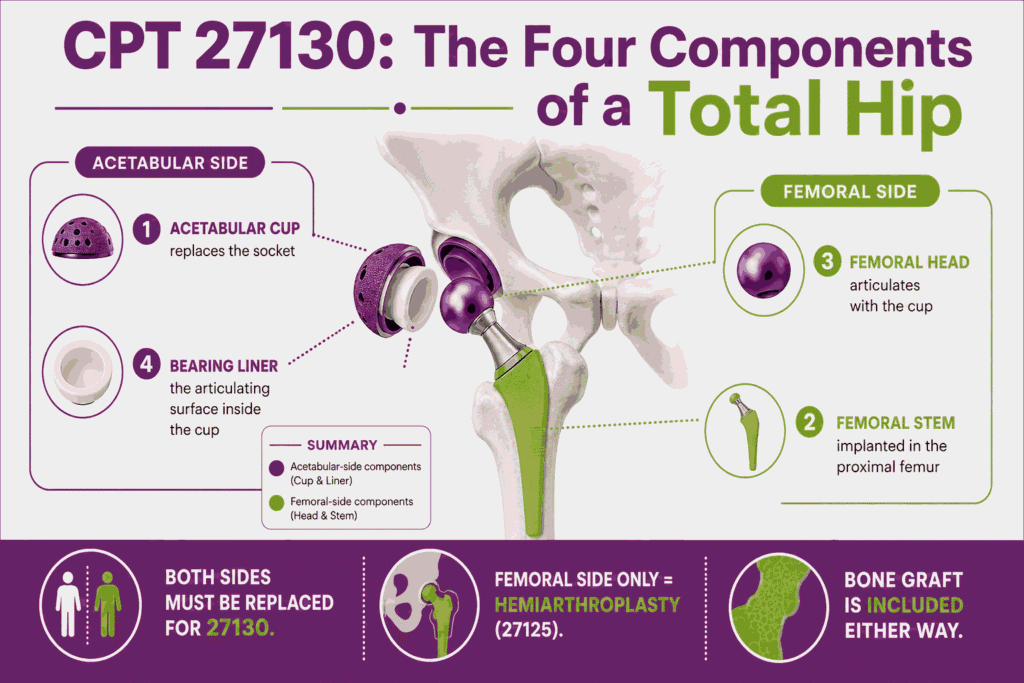
CPT code 27130 requires replacement of both sides of the hip joint. Replacing the femoral side alone is a hemiarthroplasty under a different code.
The components that define this total hip replacement include:
- The acetabular cup that replaces the hip socket
- The femoral stem implanted into the proximal femur
- The femoral head that articulates with the cup
- The bearing liner that forms the articulating surface inside the cup
Both the acetabular and femoral components must be placed for CPT 27130 to apply. Bone graft, when used to address defects, is included in the code under the “with or without autograft or allograft” language.
Why CPT 27130 Is Restricted to Primary (First-Time) Procedures and When Prior Hip Surgery Requires 27132 Instead
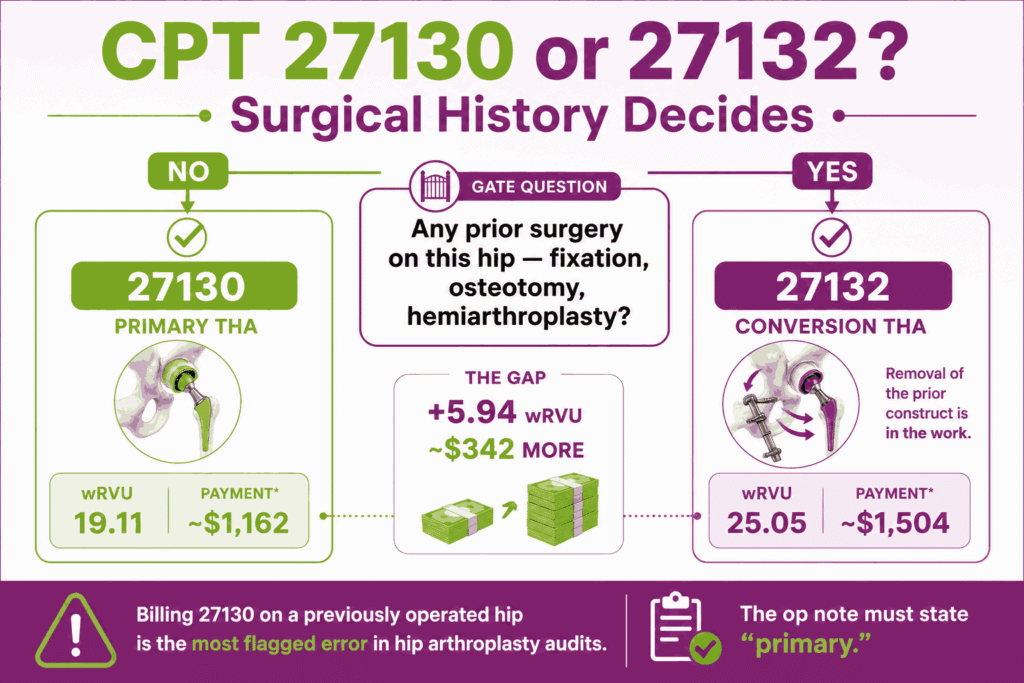
CPT code 27130 applies only when neither hip component has been previously replaced, and the joint has no prior surgical construct being converted. Any prior hip surgery that is now converted to a total hip arthroplasty routes to 27132.
The primary-versus-conversion rules are:
- Use 27130 only for a first-time total hip arthroplasty with no prior surgery on that hip
- Prior hardware in the hip, including internal fixation or a partial replacement, moves the case to conversion code 27132
- Conversion carries a higher work RVU of 25.05, reflecting the removal of the prior construct plus the new prosthesis
- Billing 27130 when prior hip surgery exists is one of the most flagged errors in hip arthroplasty audits
The operative note must state explicitly that the procedure is a primary arthroplasty. The surgical history of the hip decides the code, not the components implanted.
How Does CPT Code 27130 Differ From CPT 27125 (Hemiarthroplasty), 27132 (Conversion), and 27134/27137/27138 (Revision)?
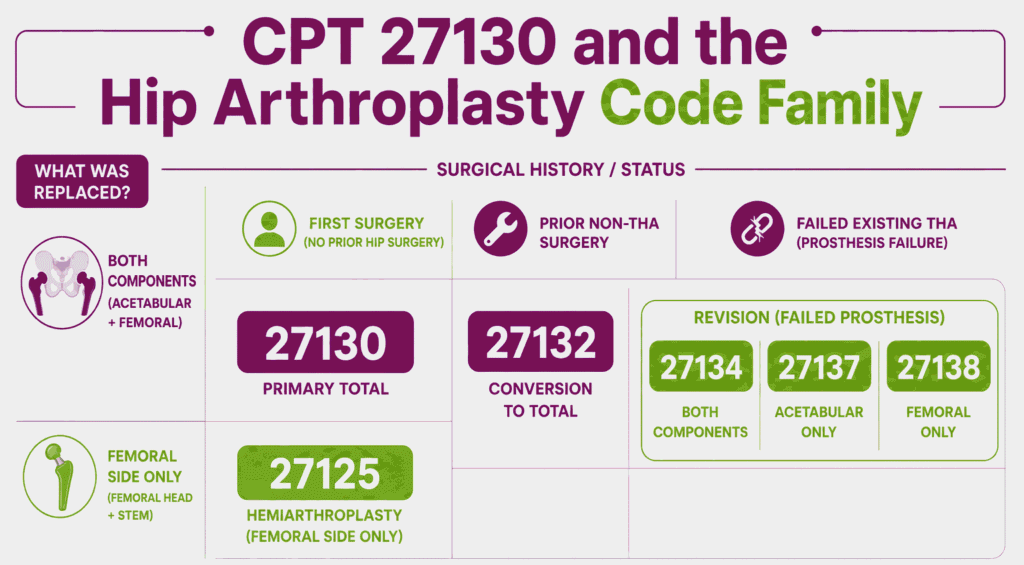
The hip arthroplasty family splits by what is replaced and by the surgical history of the joint. Code selection follows both dimensions.
The hip arthroplasty codes break down as follows:
- 27125 hemiarthroplasty: replaces the femoral side only, leaving the native acetabulum
- 27130 primary total hip arthroplasty: first-time replacement of both the acetabular and femoral components
- 27132 conversion: converts any prior hip surgery to a total hip arthroplasty
- 27134 revision of both components of an existing total hip prosthesis
- 27137 revision of the acetabular component only
- 27138 revision of the femoral component only
A first-time two-component replacement is CPT code 27130. A prior-surgery hip converted to a total prosthesis is 27132. A failed existing total hip prosthesis is a revision under 27134, 27137, or 27138, depending on the components revised.
How Are Same-Day Bilateral THA and Staged Bilateral THA Billed Under CPT Code 27130?
Bilateral total hip arthroplasty is billed differently depending on whether both hips are replaced in one session or on separate dates. CPT code 27130 describes a single hip, so bilateral cases require modifiers.
The bilateral billing rules are:
- Same-session bilateral: report 27130 with modifier 50, subject to the bilateral payment rules in the fee schedule
- Staged bilateral within the 90-day global: report the second hip with modifier 58 as a staged procedure
- Each hip is one unit, and laterality is identified with LT and RT where the payer requires
- Some payers require one line with modifier 50, while others require two lines with RT and LT, so confirm the payer format
Same-session bilateral total hip arthroplasty is less common than staged bilateral because of the physiologic demand. Staged cases performed during the global period of the first hip carry modifier 58 to show the second surgery was planned.
What ICD-10 Codes and Medical Necessity Criteria Support CPT Code 27130?
Medical necessity for CPT code 27130 rests on end-stage hip disease with documented functional limitation after failed conservative care. The diagnosis must show advanced joint destruction.
Representative supporting diagnoses include:
- M16.11 and M16.12 (Unilateral primary osteoarthritis, right and left hip)
- M16.0 (Bilateral primary osteoarthritis of the hip)
- M87.051 and M87.052 (Osteonecrosis of the femoral head, right and left)
- M05 and M06 codes (Rheumatoid arthritis) for inflammatory hip destruction
- S72.001A series (Displaced femoral neck fracture) for fracture cases treated with primary arthroplasty
The diagnosis alone does not establish necessity. Payers require imaging that corroborates the severity of degeneration, documented functional limitation, and a failed conservative course before authorizing procedure code 27130 for elective cases. From OA laterality to osteonecrosis and fracture coding, the conventions behind these selections are mapped in our ICD-10 codes for orthopedics guide.
What Are the Conservative Treatment Failure and Functional Limitation Documentation Requirements Before CPT 27130 Can Be Authorized?
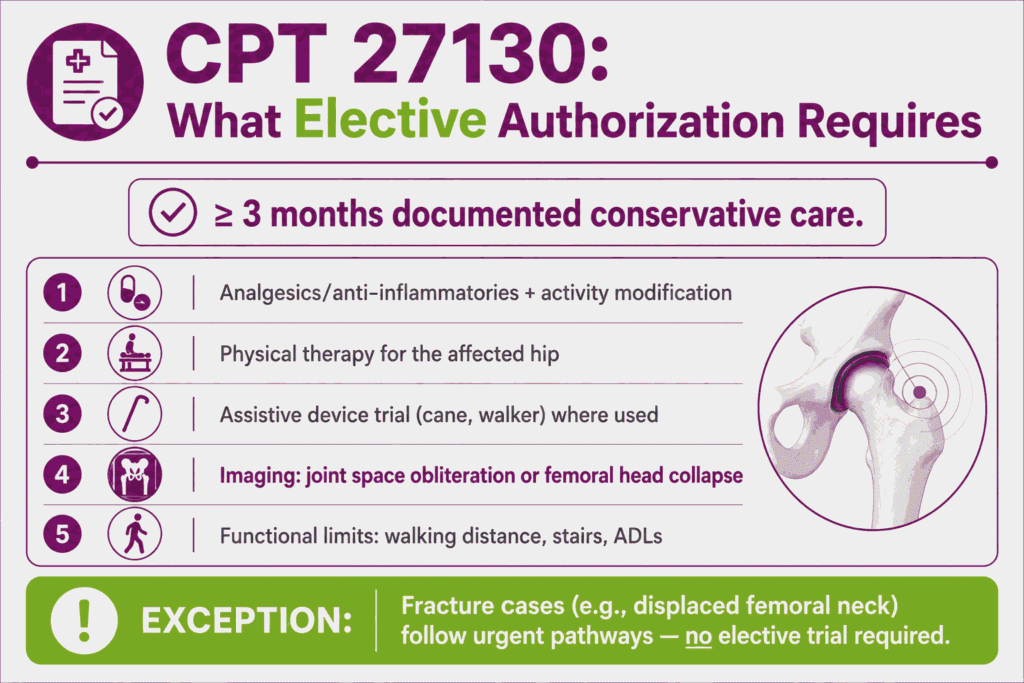
Payers require documented failure of conservative management and a recorded functional limitation before authorizing elective CPT code 27130. Fracture cases follow urgent pathways rather than elective authorization.
Common documentation requirements include:
- A conservative trial of at least three months with documented outcomes
- Analgesics or anti-inflammatory medication and activity modification
- A course of physical therapy addressing the affected hip
- Assistive device use, such as a cane or walker, where trialed
- Imaging confirming advanced degeneration, such as joint space obliteration or femoral head collapse
- Functional limitation records showing impact on walking distance, stairs, or activities of daily living
Medicare Administrative Contractors deny claims that lack evidence of non-operative management. The authorization request must connect the failed conservative course, the imaging severity, and the functional limitation.
What are the Modifiers for CPT Code 27130?
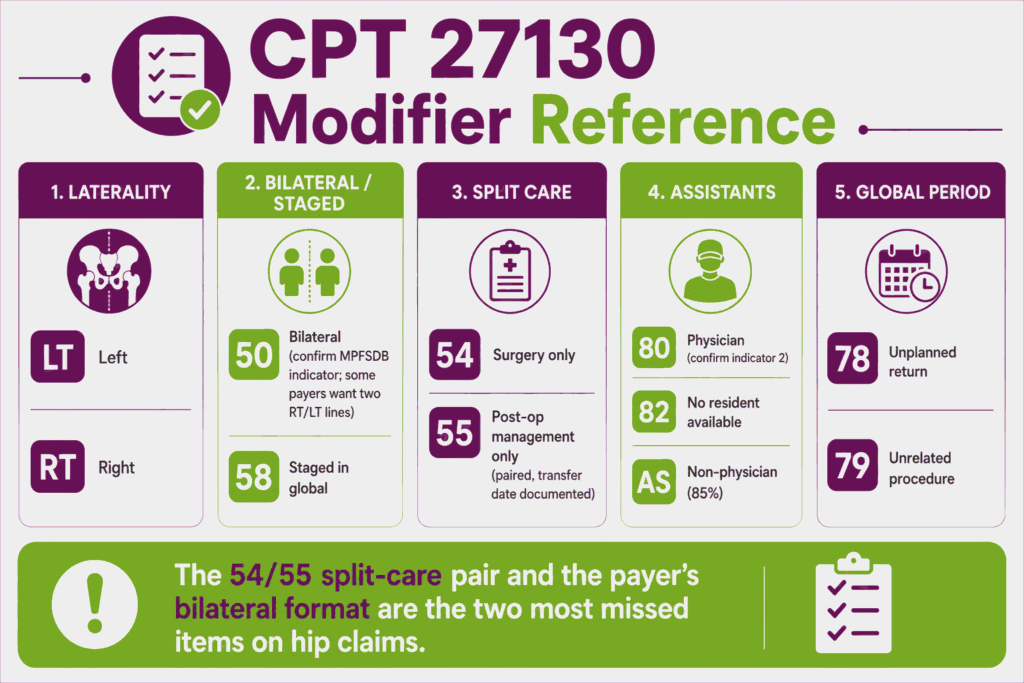
CPT 27130 uses a wide modifier set covering laterality, bilateral cases, split care, staged procedures, assistants, and the global period. The correct modifier depends on the team, the timing, and the payer’s format.
Modifier LT: Left Side Procedure
Modifier LT identifies a procedure on the left hip. Append LT to CPT code 27130 when the payer requires laterality on a single-hip claim. The operative note must state the side treated.
Modifier RT: Right Side Procedure
Modifier RT identifies a procedure on the right hip. Append RT to 27130 for a right-hip replacement when the payer requires laterality reporting. The record must document the side.
Modifier 50: Bilateral Procedure Same Session (Confirm Bilateral Indicator in MPFSDB)
Modifier 50 reports both hips replaced in one operative session. Append modifier 50 to CPT code 27130 for same-session bilateral total hip arthroplasty. Confirm the bilateral surgery indicator for the code in the Medicare Physician Fee Schedule Database before billing, since the indicator controls whether and how the bilateral adjustment applies.
Modifier 22: Increased Procedural Complexity
Modifier 22 reports substantially greater work than the procedure typically requires. Append modifier 22 to 27130 only when the operative note documents the added complexity, such as severe deformity, protrusio, or morbid obesity. Payers require a narrative and often review the claim manually.
Modifier 51: Multiple Procedures Same Session
Modifier 51 identifies multiple procedures in the same session. Append modifier 51 to the secondary procedure when CPT code 27130 is performed with another distinct procedure. The multiple procedure payment reduction applies to the lower-valued service.
Modifier 54: Surgical Care Only (Split Care — Surgeon Performs Procedure, Another Physician Manages Post-Op)
Modifier 54 reports the surgical care only when the operating surgeon transfers post-operative management to another physician. Append modifier 54 to 27130 when the surgeon performs the procedure but does not manage the 90-day recovery. Payment covers the intraoperative portion of the global package.
Modifier 55: Post-Operative Management Only (Split Care — Paired With 54)
Modifier 55 reports the post-operative management only. The physician who assumes the 90-day recovery care appends modifier 55 to CPT code 27130 with the date care was assumed. The 54 and 55 claims together account for the full global package.
Modifier 58: Staged or Related Procedure by Same Surgeon During 90-Day Global Period
Modifier 58 reports a planned or related procedure during the global period. Append modifier 58 to 27130 for a staged bilateral second hip performed within the first hip’s 90-day global window. The modifier shows the return was anticipated.
Modifier 59: Distinct Procedural Service (Separate Anatomical Structure Same Session)
Modifier 59 identifies a distinct procedural service on a separate anatomical structure in the same session. Append modifier 59, or a more specific X-modifier, only when documentation supports that the second procedure was independent of the total hip arthroplasty. Routine same-session services bundled into CPT code 27130 do not qualify.
Modifier 78: Unplanned Return to OR During Global Period
Modifier 78 reports an unplanned return to the operating room for a related complication during the global period. Append modifier 78 to the second procedure when a complication of 27130, such as dislocation or periprosthetic infection, requires unplanned surgery. Payment covers intraoperative work only.
Modifier 79: Unrelated Procedure During Global Period
Modifier 79 reports an unrelated procedure during the global period. Append modifier 79 to a procedure such as a contralateral joint service unrelated to the 27130 recovery. The modifier starts a new global period for the unrelated procedure.
Modifier 80: Assistant Surgeon — Physician (Confirm Indicator 2 Payable via MPFSDB)
Modifier 80 reports a physician assistant surgeon. Append modifier 80 to CPT code 27130 when a physician assists throughout the procedure. Confirm the assistant-at-surgery indicator for the code in the Medicare Physician Fee Schedule Database, since indicator 2 confirms the assistant is payable.
Modifier 82: Assistant Surgeon When Qualified Resident Not Available
Modifier 82 reports a physician assistant surgeon when a qualified resident is unavailable. Append modifier 82 to 27130 in a teaching setting where no resident could assist. The record must document the resident unavailability.
Modifier AS: Non-Physician Practitioner Assistant at Surgery (PA/NP/CNS)
Modifier AS reports a physician assistant, nurse practitioner, or clinical nurse specialist assisting at surgery. Append AS to CPT code 27130 for a non-physician assistant. Medicare pays the AS service at 85 percent of the physician assistant-at-surgery amount.
Which Documents Are Required For CPT Code 27130?
Documentation for CPT code 27130 must establish that the procedure is primary, medically necessary, and performed in a justified setting. The record connects the authorization, the operative event, and the implant.
The required documentation includes:
- Prior authorization specific to 27130 for the correct hip
- Explicit operative-note confirmation that the arthroplasty is primary, not a conversion or revision
- Conservative-treatment-failure records and imaging corroborating degeneration severity
- Laterality documentation for the hip treated
- Implant records, including manufacturer, model, and lot number
- Graft documentation where autograft or allograft was used
- Site-of-service justification for inpatient, hospital outpatient, or ASC billing
- Assistant, co-surgeon, or split-care documentation supporting the modifiers billed
What Is the Cost of CPT Code 27130?
The cost of CPT code 27130 splits into the surgeon professional fee and the facility fee, which vary sharply by setting. Medicare prices the professional fee through the Physician Fee Schedule.
RVUs & Medicare Payment
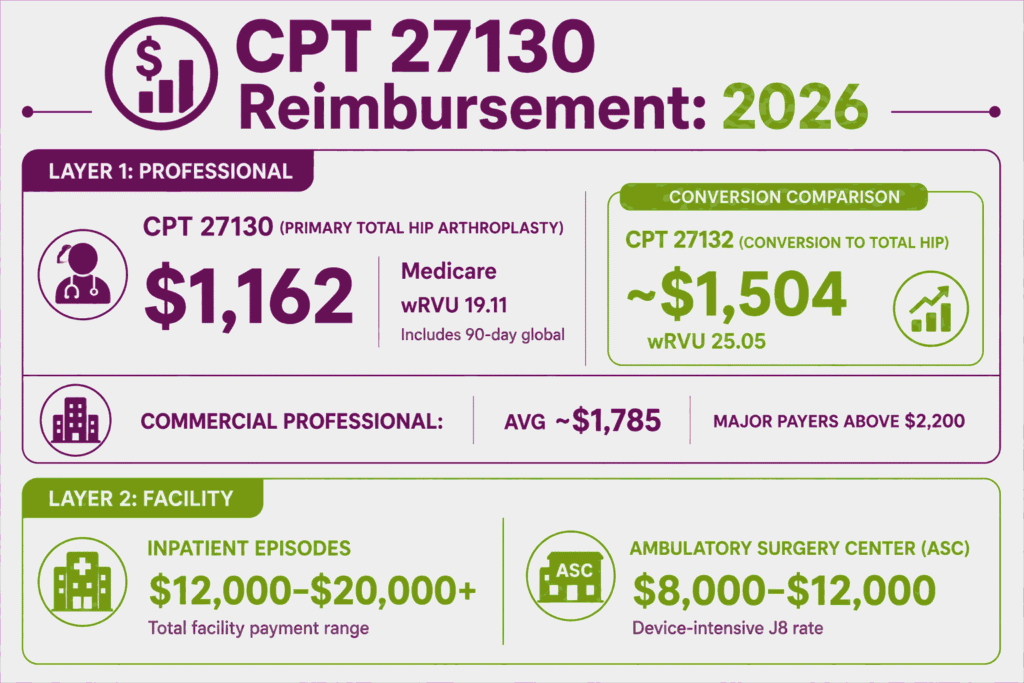
Medicare prices the professional component of CPT code 27130 through the Physician Fee Schedule. The CY2026 values appear below.
| Component | Value (CY 2026) |
|---|---|
| Work RVU | 19.11 |
| Total RVU (facility) | 34.79 |
| Medicare professional payment | $1,162.02 |
| Conversion factor | $33.4009 |
| Global period | 090 |
The professional fee covers the surgeon work plus the 90-day global period. The conversion code 27132 carries a higher work RVU of 25.05 and pays approximately $1,504, which shows why coding the correct primary-versus-conversion status matters. GPCI adjustments change the final amount by locality.
Commercial Payers
Commercial plans reimburse procedure code 27130 well above the Medicare professional rate. National benchmark data places the average commercial professional payment near $1,785, against a Medicare mean of roughly $1,178, with major payers reporting means above $2,200.
Facility charges drive the larger totals. Hospital inpatient episodes commonly run $12,000 to $20,000 or more depending on the diagnosis-related group, while ASC facility rates average roughly $8,000 to $12,000. Commercial site-of-service policies increasingly steer uncomplicated cases away from inpatient stays.
Place-of-Service & Geographic Adjustments
Site of service is the largest cost variable for CPT code 27130, since the facility payment differs across inpatient, hospital outpatient, and ambulatory surgery center settings. Locality adjusts each amount.
Key setting and geographic factors include:
- Inpatient billing pays a facility fee through the inpatient prospective payment system, the highest of the three
- Hospital outpatient billing pays through the outpatient prospective payment system at an APC rate
- Ambulatory surgery center billing pays the lowest facility rate, at the device-intensive adjusted amount
- GPCI values adjust the professional fee by locality, while the surgeon fee stays consistent across settings
What Are Example Clinical Scenarios or Use Cases for CPT Code 27130?
CPT code 27130 applies when end-stage hip disease requires a first-time total replacement of both joint components. The scenarios below show common reporting patterns.
Scenario 1: End-Stage Primary Osteoarthritis of the Hip With Documented Functional Limitation and Failed Conservative Management
ICD-10: M16.11 (Unilateral primary osteoarthritis, right hip)
A patient with advanced osteoarthritis of the right hip has failed three months of physical therapy, anti-inflammatory medication, and activity modification. Imaging shows joint space obliteration, and walking distance is limited to one block. The surgeon performs a primary right total hip arthroplasty. The practice reports CPT code 27130 with modifier RT, supported by the conservative-failure and functional-limitation documentation.
Scenario 2: Avascular Necrosis of the Femoral Head With Advanced Articular Surface Collapse
ICD-10: M87.051 (Osteonecrosis due to idiopathic causes, right femur)
A patient with avascular necrosis of the right femoral head presents with articular surface collapse on imaging. The joint destruction involves both the femoral head and secondary acetabular change. The surgeon performs a primary total hip arthroplasty, replacing both components. The practice reports CPT 27130, with the osteonecrosis diagnosis and collapse imaging supporting medical necessity.
Scenario 3: Rheumatoid Arthritis With Severe Hip Joint Destruction Unresponsive to Disease-Modifying Therapy
ICD-10: M05.751 (Rheumatoid arthritis with rheumatoid factor, right hip)
A patient with rheumatoid arthritis has severe destruction of the right hip joint despite disease-modifying therapy. Imaging shows advanced erosion of the acetabulum and femoral head. The surgeon performs a primary total hip arthroplasty. The practice reports CPT code 27130, with the inflammatory diagnosis, therapy history, and imaging supporting the claim.
Scenario 4: Displaced Femoral Neck Fracture in an Active Elderly Patient Treated With Primary THA
ICD-10: S72.001A (Fracture of unspecified part of neck of right femur, initial encounter)
An active 72-year-old sustains a displaced femoral neck fracture of the right hip. Given the displacement and the patient’s activity level, the surgeon selects a primary total hip arthroplasty over hemiarthroplasty. The practice reports CPT code 27130 with modifier RT. The fracture diagnosis supports urgent medical necessity without an elective conservative-care trial.
What Are the CPT Code 27130 Rules To Ensure Successful Reimbursement?
Follow site-of-service requirements, NCCI bundling rules, bilateral staging rules, the primary-versus-conversion restriction, device billing rules, and the TEAM episode requirements. Meeting these rules reduces denials and recoupment for CPT code 27130.
Inpatient vs. Outpatient vs. ASC: The Two-Midnight Rule and Site-of-Service Medical Necessity
CPT code 27130 can be performed in inpatient, hospital outpatient, or ambulatory surgery center settings. CMS removed it from the Inpatient-Only list in 2020 and added it to the ASC Covered Procedures List in 2021.
The site-of-service rules are:
- The two-midnight rule governs inpatient admission, requiring an expectation that care crosses two midnights
- The surgeon determines the appropriate setting based on the patient’s clinical characteristics, documented before surgery
- An uncomplicated outpatient case discharged within 24 hours but billed as inpatient creates recoupment exposure
- Some commercial payers still restrict the ASC setting, so confirm site-of-service coverage during authorization
Bundling / NCCI / Same-Day Procedure Rules
NCCI rules bundle several services into CPT code 27130 when performed on the same hip in the same session. These services are not separately reportable.
The core bundling rules are:
- Bone graft, autograft or allograft, is included in the code descriptor and never billed separately
- Intraoperative fluoroscopy to confirm component positioning is included in the primary procedure
- A diagnostic arthroscopy of the same hip in the same session is bundled as a scout procedure
- Run every claim through an NCCI scrubber before submitting 27130 with any other code
Units, MUEs & Bilateral Staging Billing Rules
CPT code 27130 is a single-hip code, so each hip is one unit. Bilateral and staged cases use modifiers rather than additional units.
Unit and staging rules include:
- Report one unit of 27130 per hip, since the code describes a single total hip arthroplasty
- Same-session bilateral cases use modifier 50 or the payer’s required two-line RT and LT format
- Staged bilateral cases within the global period use modifier 58 on the second hip
- Confirm the current Medically Unlikely Edit value through CMS, since the table updates quarterly
Why 27130 Cannot Be Used When Any Prior Hip Surgery Is Present and Which Code Applies Instead
Any prior surgery on the operative hip disqualifies CPT code 27130. The prior construct changes the work performed, and the code must reflect it.
The code-selection rules for prior surgery are:
- Prior internal fixation, osteotomy, or hemiarthroplasty converted to a total hip prosthesis is 27132
- Revision of an existing total hip prosthesis is 27134 for both components, 27137 for the acetabular component, or 27138 for the femoral component
- The conversion and revision codes carry higher RVUs that reflect the removal of the prior construct
- Billing 27130 on a previously operated hip is a leading audit finding that produces recoupment and downcoding exposure
Primary, conversion, and revision distinctions like these run throughout the orthopedic surgery CPT codes, where surgical history changes the code as much as the anatomy does.
Implant Charge Capture and Device-Intensive Rate Billing in Facility vs. ASC Settings
Implant and device charges are captured on the facility claim, not the surgeon professional claim for CPT code 27130. The ASC setting applies a device-intensive payment methodology.
The implant billing rules are:
- The surgeon professional fee for 27130 does not include the implant cost
- Hospital settings capture the implant charge through the inpatient or outpatient facility payment
- In the ASC, the code carries payment indicator J8, a device-intensive adjusted rate that accounts for the implant cost
- The facility record must document the implant manufacturer, model, and lot number for charge capture
How the Mandatory TEAM Episode Model Changes Medicare Payment for 27130 at Participating Hospitals (2026–2030)
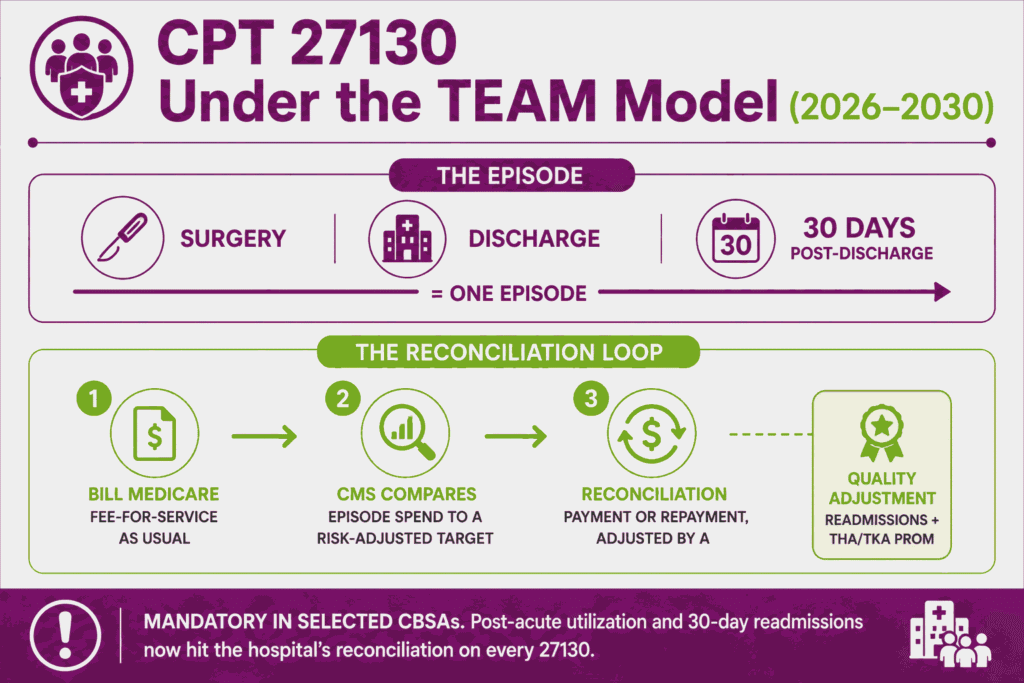
The Transforming Episode Accountability Model (TEAM) is a mandatory episode-based payment model that runs from January 1, 2026, through December 31, 2030. Lower extremity joint replacement, which includes CPT code 27130 in both inpatient and outpatient settings, is one of its five episode categories.
The TEAM rules that affect this code are:
- Hospitals in selected Core-Based Statistical Areas must participate, and each episode runs from surgery through 30 days after discharge
- Providers continue billing Medicare fee-for-service as usual, and CMS reconciles actual episode spending against a risk-adjusted target price after each performance year
- Reconciliation payments or repayment amounts depend on spending against the target and on a composite quality score that includes readmissions and the THA/TKA patient-reported outcome measure
- Hospitals may enter gain-sharing arrangements with surgeons, which ties surgeon incentives to episode cost and quality performance
TEAM replaces the legacy CJR bundled payment program. For practices at participating hospitals, post-acute utilization and readmissions within 30 days now directly affect the hospital’s reconciliation on every 27130 episode. Episode models layer reconciliation on top of standard fee-for-service, but claims still flow through the CPT coding system line by line before CMS trues up spending.
90-Day Global Period, Modifier 58 Staged-Procedure Rules, and Split Care (54/55) Billing
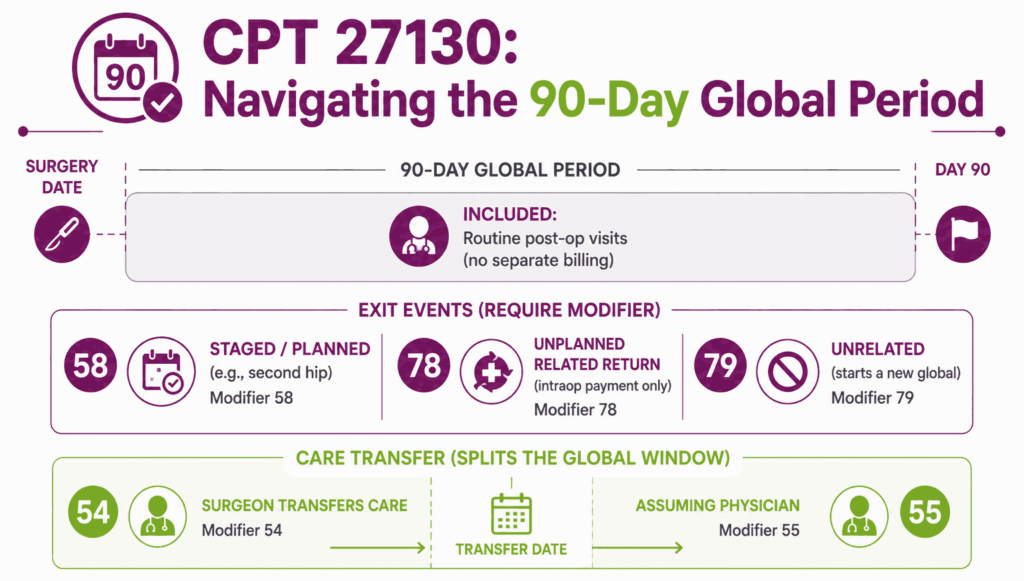
CPT code 27130 carries a 90-day global period that includes routine post-operative care. Global-period returns and transferred care each have a specific modifier.
The global-period rules are:
- Routine post-operative visits within 90 days are included in the 27130 payment
- A staged or planned procedure during the global period, such as a staged bilateral second hip, uses modifier 58
- An unplanned related return to the operating room uses modifier 78, and an unrelated procedure uses modifier 79
- Split care uses modifier 54 for the surgeon and modifier 55 for the physician who assumes post-operative management, with the transfer date documented
Top Reasons For Denials Specific To 27130 & Quick Remedies
- 27130 Billed When Prior Hip Surgery Exists: Prevent by confirming the hip’s surgical history at coding and routing conversions to 27132 and revisions to 27134, 27137, or 27138.
- Missing Conservative-Treatment-Failure Documentation: Prevent by attaching the conservative trial, imaging, and functional-limitation records to elective authorization requests.
- Site-of-Service Mismatch: Prevent by documenting the two-midnight expectation before inpatient admission and billing uncomplicated same-day cases as outpatient.
- Missing or Wrong Laterality or Bilateral Format: Prevent by appending RT or LT per payer rules and confirming whether the payer wants modifier 50 on one line or two RT and LT lines.






