CPT code 27447 reports total knee arthroplasty, the replacement of both the medial and lateral compartments of the knee with prosthetic components. It is the highest-volume and one of the highest-value procedures in orthopedic surgery.
CPT 27447 carries a 90-day global period and strict payer controls, including prior authorization and conservative-treatment-failure requirements. Site-of-service rules now allow the procedure in inpatient, hospital outpatient, and ambulatory surgery center settings, which changes both authorization and reimbursement.
These controls make 27447 a frequent denial and recoupment target, which is why many practices route joint replacement claims through dedicated orthopedic billing services.
What Is the Description of CPT Code 27447?
The 27447 CPT code description as defined by the AMA is: “Arthroplasty, knee, condyle and plateau; medial AND lateral compartments with or without patella resurfacing (total knee arthroplasty).”
This code reports a total knee arthroplasty that resurfaces both the medial and lateral compartments of the knee. CPT code 27447 covers the femoral condyle and tibial plateau components together. The phrase “with or without patella resurfacing” means the patellar component is part of the same code, not a separate charge.
The procedure treats end-stage knee disease when the joint surface is destroyed. Procedure code 27447 applies to a primary total knee replacement, distinct from partial replacement and from revision surgery.
What Compartments and Implant Components Define CPT Code 27447 as a Total Knee Arthroplasty?
CPT code 27447 requires replacement of both the medial and lateral compartments to qualify as a total knee arthroplasty. Replacing a single compartment falls under a different code.
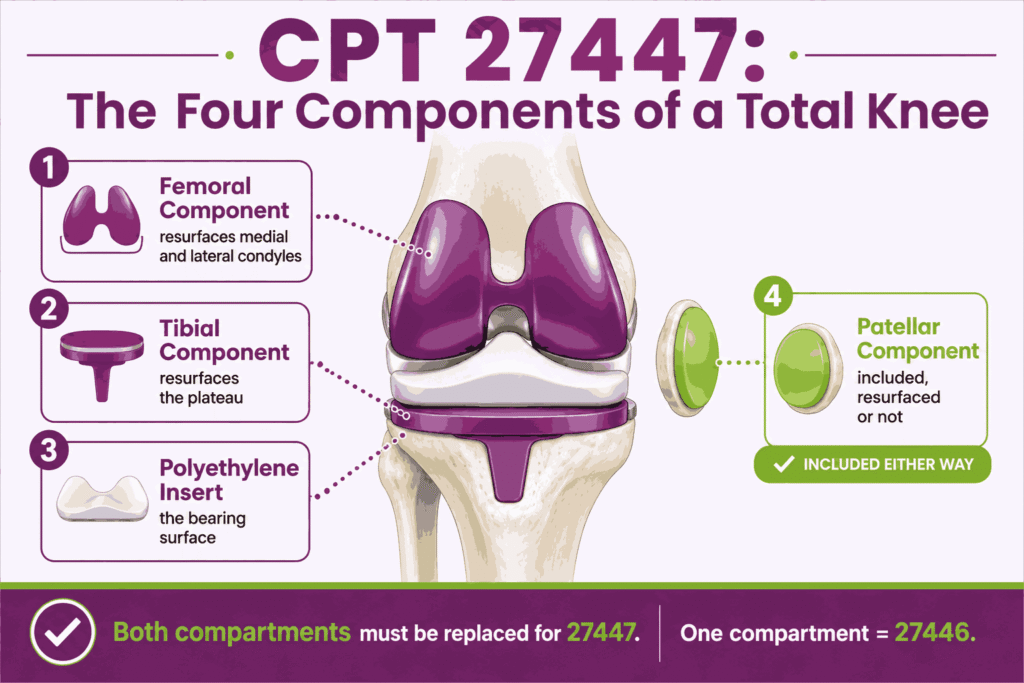
The components that define this total knee replacement include:
- The femoral component that resurfaces the medial and lateral condyles
- The tibial component that resurfaces the tibial plateau
- The patellar component when patella resurfacing is performed
- The polyethylene insert that forms the bearing surface between components
Both the medial and lateral compartments must be replaced for CPT 27447 to apply. Patella resurfacing is included whether or not the surgeon performs it, so it never generates a separate line.
How Does CPT Code 27447 Differ From CPT 27446 (Unicompartmental) and CPT 27445 (Hinged Implant)?
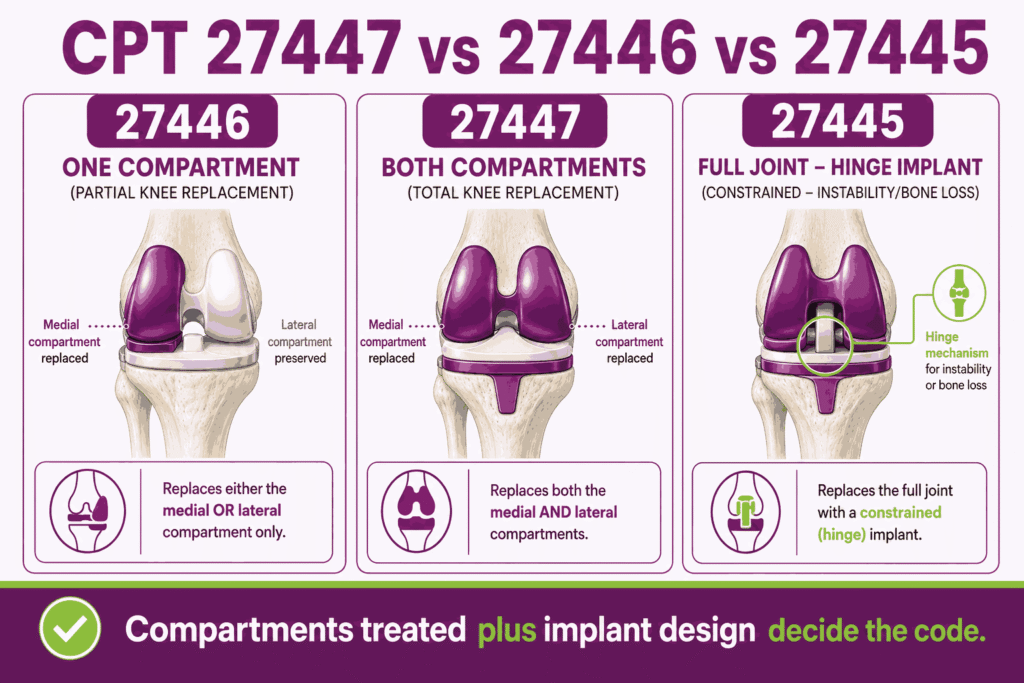
The three codes differ by how much of the knee is replaced and by the implant type. Code selection follows the compartments treated and the prosthesis used.
The knee arthroplasty codes break down as follows:
- 27446 unicompartmental arthroplasty: replaces one compartment, either medial or lateral, not both
- 27447 total knee arthroplasty: replaces both the medial and lateral compartments
- 27445 hinged prosthesis: uses a constrained hinge implant for severe instability or bone loss
The distinction is the extent of replacement and the implant design. A single-compartment replacement is 27446, a two-compartment replacement is CPT code 27447, and a constrained hinge prosthesis is 27445. The knee arthroplasty family sits within the broader set of orthopedic CPT codes where compartment, approach, and implant design drive selection.
Is Patella Resurfacing Separately Billable When Performed With CPT Code 27447?
No, patella resurfacing is not separately billable with CPT code 27447. The descriptor states “with or without patella resurfacing,” so the patellar work is bundled into the code.
The patella rules are:
- The patellar component is included in 27447 whether or not it is resurfaced
- No separate CPT code is reported for resurfacing the patella during the same total knee arthroplasty
- Billing a separate patella code with CPT 27447 on the same knee triggers a bundling denial
- The operative note documents the patellar work as part of the total procedure
How Are Same-Day Bilateral TKA and Staged Bilateral TKA Billed Under CPT Code 27447?
Bilateral total knee arthroplasty is billed differently depending on whether both knees are replaced in one session or on separate dates. CPT code 27447 is inherently a single-knee code, so bilateral cases require specific modifiers.
The bilateral billing rules are:
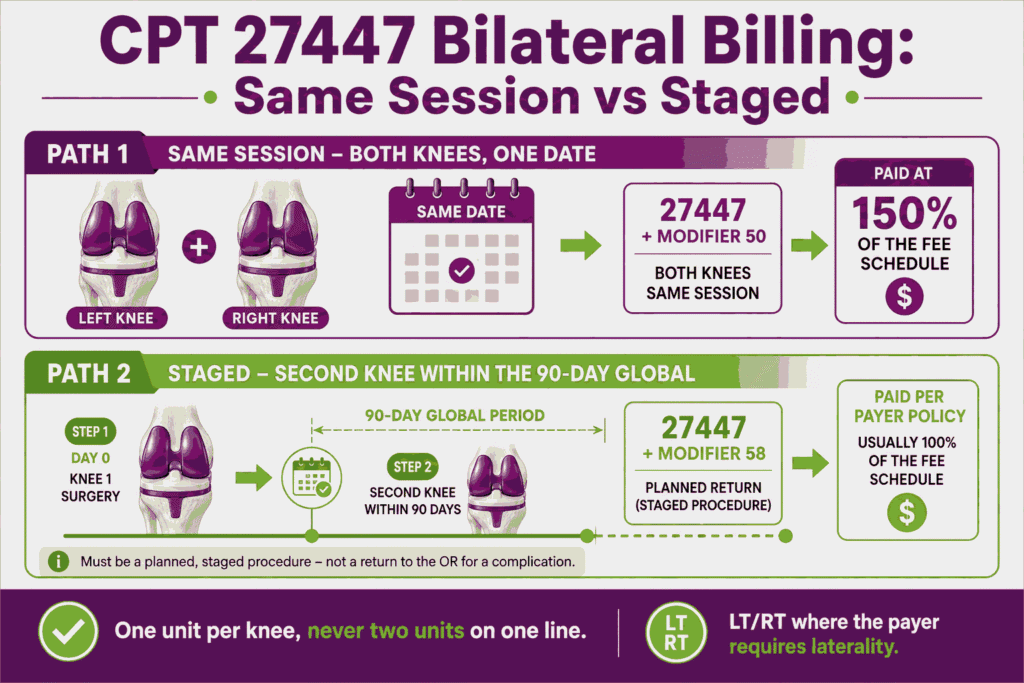
- Same-session bilateral: report 27447 with modifier 50, paid at 150 percent of the fee schedule
- Staged bilateral within the 90-day global: report the second knee with modifier 58 for a staged procedure
- Each knee is one unit, since the code describes a single total knee arthroplasty
- The record must identify the laterality of each procedure with the LT and RT modifiers where the payer requires
Same-session bilateral cases use one line with modifier 50 under most payer rules. Staged cases done during the global period of the first knee use modifier 58 to show the second surgery was planned.
What ICD-10 Codes and Medical Necessity Criteria Support CPT Code 27447?
Medical necessity for CPT code 27447 rests on end-stage knee disease with functional limitation after failed conservative care. When it comes to orthopedic ICD 10 codes for knee arthroplasty, the diagnosis must document advanced joint destruction.
Representative supporting diagnoses include:
- M17.11 and M17.12 (Unilateral primary osteoarthritis of the knee, right and left)
- M17.0 (Bilateral primary osteoarthritis of the knee)
- M05 and M06 codes (Rheumatoid arthritis) for inflammatory joint destruction
- M17.31 and M17.32 (Unilateral post-traumatic osteoarthritis of the knee)
The diagnosis alone does not establish necessity. Payers require documented functional limitation, advanced radiographic findings, and a failed course of conservative management before they authorize procedure code 27447.
What Are the Conservative Treatment Failure Documentation Requirements Before CPT 27447 Can Be Authorized?
Payers require documented failure of conservative management before they authorize CPT code 27447. The typical requirement is a trial of several months of non-surgical care with recorded results.
Common conservative-failure documentation includes:
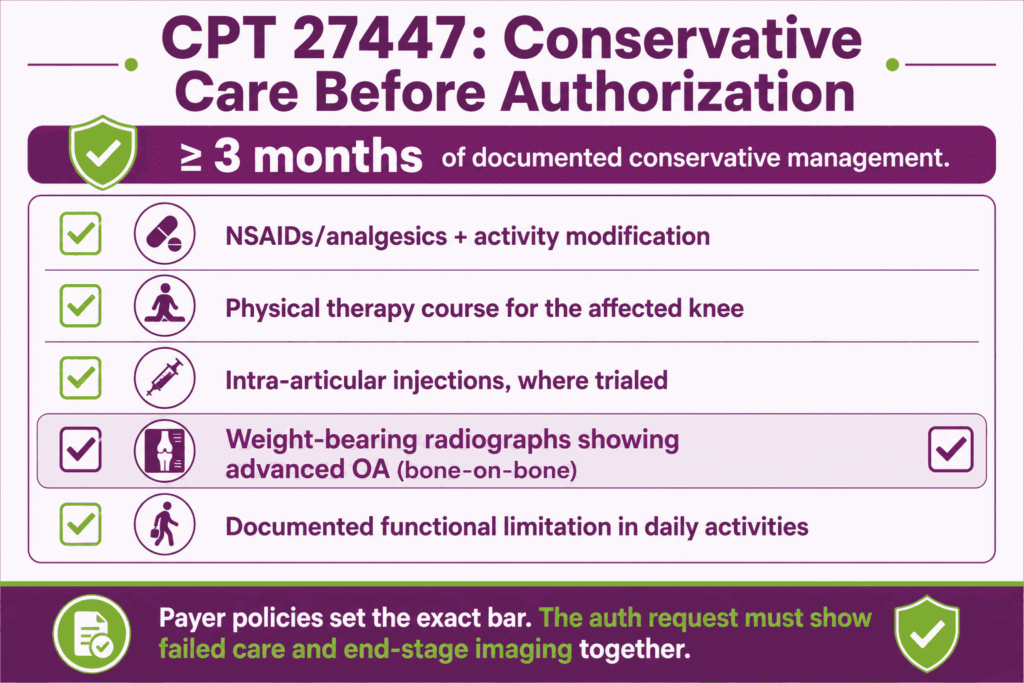
- A trial of at least three months of conservative management with documented outcomes
- Non-steroidal anti-inflammatory drugs or analgesics, and activity modification
- A course of physical therapy addressing the affected knee
- Intra-articular injections such as corticosteroid or viscosupplementation, where trialed
- Weight-bearing radiographs showing advanced osteoarthritis, such as bone-on-bone joint space loss
- Documented functional limitation affecting daily activities
Payer medical policies set the exact requirements, which vary by plan. The authorization request must show that conservative care failed and that imaging supports end-stage disease.
What are the Modifiers for CPT Code 27447?
CPT 27447 uses a wide set of modifiers for laterality, multiple surgeons, assistants, and the global period. The right modifier depends on the setting, the surgical team, and the timing.
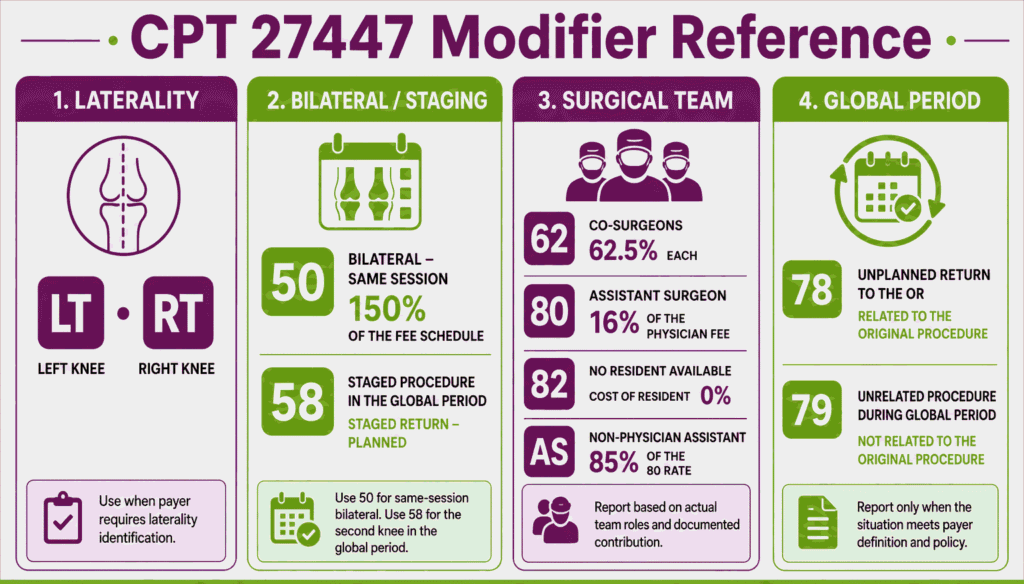
Modifier LT: Left Side Procedure
Modifier LT identifies a procedure performed on the left knee. Append LT to CPT code 27447 when the payer requires laterality on a single-knee claim. The operative note must state the side treated.
Modifier RT: Right Side Procedure
Modifier RT identifies a procedure performed on the right knee. Append RT to 27447 for a right-knee replacement when the payer requires laterality reporting. The record must document the side.
Modifier 50: Bilateral Procedure Same Session (Reimbursed at 150% of MPFS)
Modifier 50 reports both knees replaced in one operative session. Append modifier 50 to CPT code 27447 for same-session bilateral total knee arthroplasty. Medicare pays the bilateral service at 150 percent of the fee schedule amount.
Modifier 22: Increased Procedural Complexity
Modifier 22 reports substantially greater work than the procedure usually requires. Append modifier 22 to 27447 only when the operative note documents the added complexity, such as severe deformity or prior hardware. Payers require a supporting narrative and often review the claim manually.
Modifier 51: Multiple Procedures Same Session
Modifier 51 identifies multiple procedures performed in the same session. Append modifier 51 to the secondary procedure when CPT code 27447 is performed with another distinct procedure. Medicare applies the multiple procedure payment reduction to the lower-valued service.
Modifier 58: Staged or Related Procedure During Global Period
Modifier 58 reports a planned or related procedure during the 90-day global period. Append modifier 58 to 27447 for a staged bilateral second knee, or to a related procedure such as a planned manipulation. The modifier shows the return was anticipated.
Modifier 62: Two Surgeons / Co-Surgery (Reimbursed at 62.5% each; Requires Medical Necessity Documentation)
Modifier 62 reports two surgeons acting as co-surgeons on the same procedure. Append modifier 62 to CPT code 27447 for each surgeon when co-surgery is medically necessary. Each surgeon is paid 62.5 percent of the fee schedule, and both operative notes must justify the co-surgery.
Modifier 80: Assistant Surgeon (MD/DO)
Modifier 80 reports a physician assistant surgeon. Append modifier 80 to 27447 when a physician assists throughout the procedure. Medicare pays the assistant at 16 percent of the fee schedule amount.
Modifier 82: Assistant Surgeon (When Qualified Resident is Unavailable)
Modifier 82 reports a physician assistant surgeon when a qualified resident is unavailable. Append modifier 82 to CPT code 27447 in a teaching setting where no resident could assist. The record must document the resident unavailability.
Modifier AS: Non-Physician Assistant at Surgery (PA/NP/CNS assisting; Reimbursed at 85% of the Modifier 80 amount)
Modifier AS reports a physician assistant, nurse practitioner, or clinical nurse specialist assisting at surgery. Append AS to 27447 for a non-physician assistant. Medicare pays the AS service at 85 percent of the physician assistant surgeon amount under modifier 80.
Modifier 78: Unplanned Return to OR During Global Period
Modifier 78 reports an unplanned return to the operating room for a related complication during the global period. Append modifier 78 to the second procedure when a complication of CPT code 27447 requires unplanned surgery. Payment covers intraoperative work only.
Modifier 79: Unrelated Procedure During Global Period
Modifier 79 reports an unrelated procedure during the global period. Append modifier 79 to a procedure such as a contralateral joint service that is unrelated to the 27447 recovery. The modifier resets the global period for the new procedure.
Which Documents Are Required For CPT Code 27447?
Documentation for CPT code 27447 must support medical necessity, the surgical work, and the site of service. The record connects the authorization to the operative event.
The required documentation includes:
- Prior authorization specific to 27447 for the correct knee
- Conservative-treatment-failure records and weight-bearing radiographs
- The operative report describing both compartments and the components implanted
- Laterality documentation for the knee treated
- Implant and device records, including manufacturer and lot information
- Site-of-service justification for inpatient, hospital outpatient, or ASC billing
- Any assistant or co-surgeon documentation supporting the modifiers billed
What Is the Cost of CPT Code 27447?
The cost of CPT code 27447 splits into the surgeon professional fee and the facility fee, which differ sharply by setting. Medicare sets the professional fee through the Physician Fee Schedule.
RVUs & Medicare Payment
Medicare prices the professional component of CPT code 27447 through the Physician Fee Schedule. The CY2026 values appear below.
| Component | Value (CY 2026) |
|---|---|
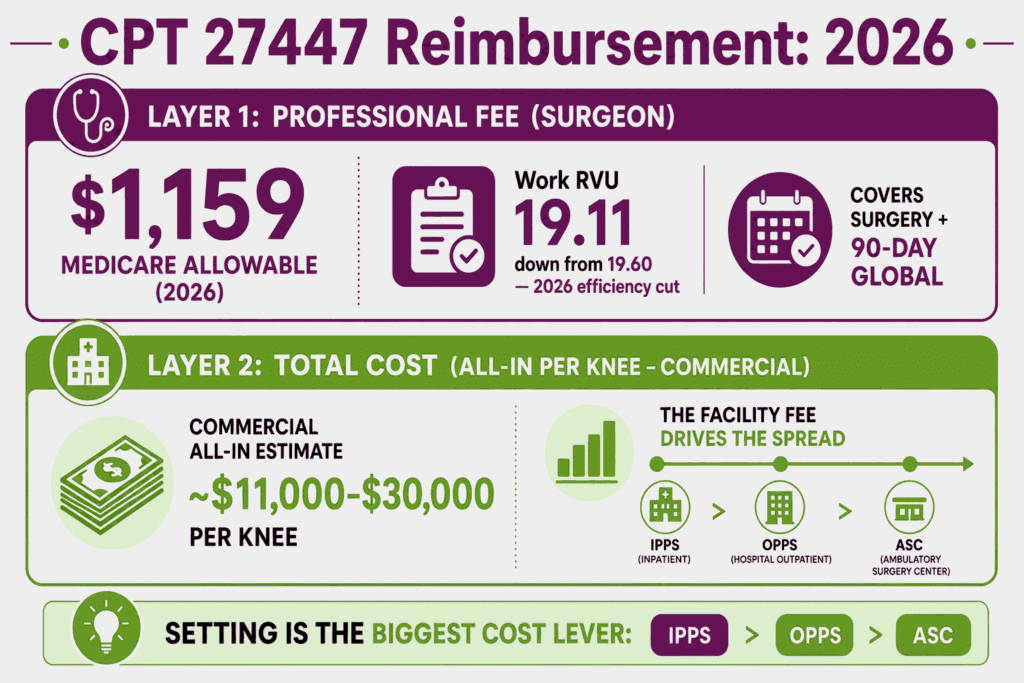
| Work RVU | 19.11 |
| Total RVU (facility) | 34.71 |
| Medicare professional payment | $1,159 |
| Conversion factor | $33.4009 |
| Global period | 090 |
The CY2026 work RVU of 19.11 reflects the 2.5 percent efficiency adjustment applied to non-time-based services, down from 19.60, reflecting how CPT codes are revalued year to year. The professional fee covers the surgeon work plus the 90-day global period. GPCI adjustments change the final amount by locality.
Commercial Payers
Commercial plans reimburse procedure code 27447 at a contracted multiple of the Medicare rate. Total allowed charges for a single knee, including the facility component, commonly range from roughly $11,000 to $30,000 depending on site of service and payer.
The professional fee remains relatively stable across settings, while the facility fee drives most of the variation. Commercial site-of-service policies increasingly deny inpatient stays for uncomplicated cases, which shifts payment to the lower outpatient and ASC facility rates.
Place-of-Service & Geographic Adjustments
Site of service is the largest cost variable for CPT code 27447, since the facility fee differs across inpatient, hospital outpatient, and ambulatory surgery center settings. Locality then adjusts each amount.
Key setting and geographic factors include:
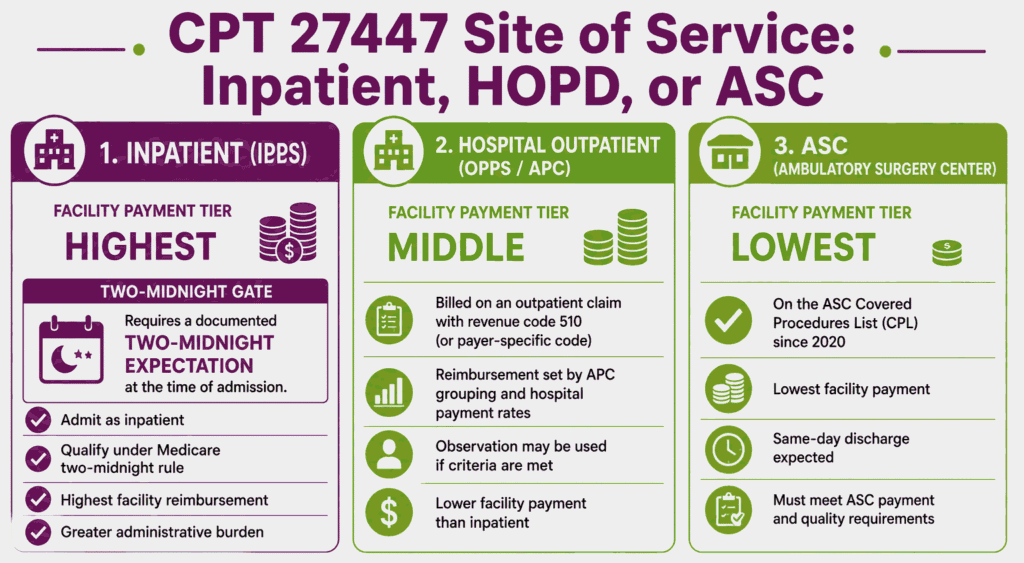
- Inpatient billing pays a facility fee through the inpatient prospective payment system, the highest of the three
- Hospital outpatient billing pays through the outpatient prospective payment system at an APC rate
- Ambulatory surgery center billing pays the lowest facility rate of the three settings
- GPCI values adjust the professional fee by locality, and the surgeon fee stays consistent across settings
What Are Example Clinical Scenarios or Use Cases for CPT Code 27447?
CPT code 27447 applies when end-stage knee disease requires replacement of both compartments after failed conservative care. The scenarios below show common reporting patterns.
Scenario 1: End-Stage Tricompartmental Osteoarthritis With Failed Conservative Management
ICD-10: M17.11 (Unilateral primary osteoarthritis, right knee)
A patient with bone-on-bone osteoarthritis of the right knee has failed three months of physical therapy, NSAIDs, and corticosteroid injections. Weight-bearing radiographs confirm advanced joint destruction. The surgeon performs a right total knee arthroplasty. The practice reports CPT code 27447 with modifier RT, supported by the conservative-failure documentation and prior authorization.
Scenario 2: Rheumatoid Arthritis With Severe Bicompartmental Joint Destruction
ICD-10: M06.061 (Rheumatoid arthritis without rheumatoid factor, right knee)
A patient with rheumatoid arthritis has severe destruction of the medial and lateral compartments of the right knee. Conservative management and disease-modifying therapy have not preserved function. The surgeon replaces both compartments in a total knee arthroplasty. The practice reports CPT 27447, with the inflammatory diagnosis and imaging supporting medical necessity.
Scenario 3: Post-Traumatic Arthritis Following Prior Tibial Plateau Fracture
ICD-10: M17.31 (Unilateral post-traumatic osteoarthritis, right knee)
A patient who sustained a tibial plateau fracture years earlier develops post-traumatic arthritis of the right knee. Conservative care has failed, and imaging shows advanced degeneration. The surgeon performs a total knee arthroplasty, and the case involves added complexity from prior hardware. The practice reports CPT code 27447 with modifier 22 and a supporting operative narrative.
What Are the CPT Code 27447 Rules To Ensure Successful Reimbursement?
Follow NCCI bundling rules, bilateral staging rules, site-of-service requirements, code-specific authorization, and global-period billing limits. Meeting these rules reduces denials and recoupment for CPT code 27447.
Bundling / NCCI / Same-Day Procedure Rules
NCCI rules bundle several services into CPT code 27447 when performed on the same knee in the same session. These services are not separately reportable.
The core bundling rules are:
- A diagnostic or surgical arthroscopy on the same knee in the same session is bundled as a scout procedure
- Intraoperative fluoroscopy to confirm component positioning is included in the primary procedure
- A post-operative manipulation within the global period requires modifier 58 to be payable
- Run every claim through an NCCI scrubber before submitting 27447 with any other code
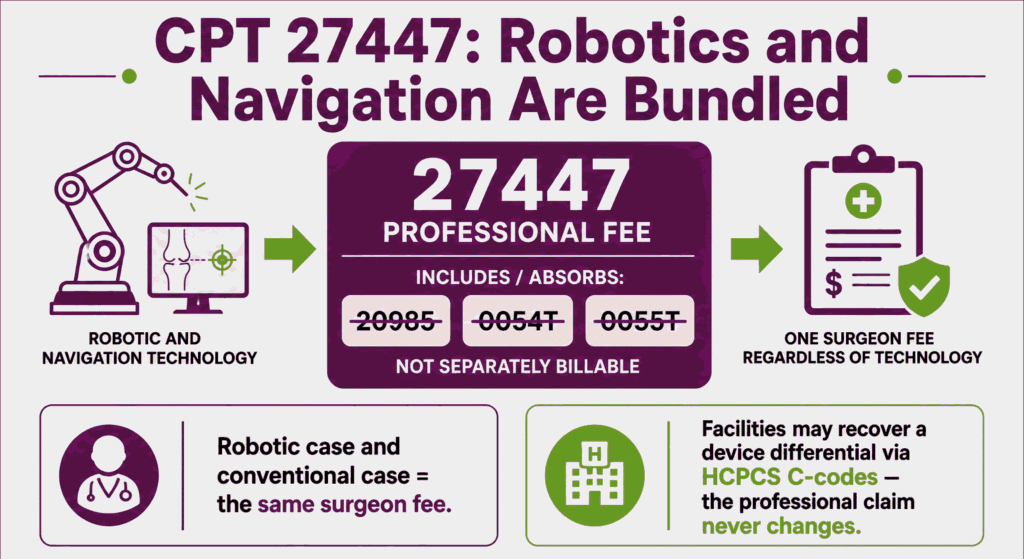
Why Robotic and Computer-Assisted Navigation (20985 / 0054T / 0055T) Are Not Separately Reimbursable
Robotic assistance and computer-assisted navigation are bundled into CPT code 27447 and carry no separate professional payment. There is no distinct professional CPT code for robotic joint replacement.
The navigation and robotic rules are:
- Computer-assisted navigation codes 20985, 0054T, and 0055T are not separately payable with 27447
- The robotic or navigation technology is part of the surgical service and included in the primary code
- The surgeon professional fee is the same for a robotic case as for a conventional case
- A facility may recover a facility-level differential through HCPCS C-codes, but the professional fee does not change
Units, MUEs & Bilateral Staging Billing Rules
CPT code 27447 is a single-knee code, so each knee is one unit. Bilateral and staged cases use modifiers rather than additional units.
Unit and staging rules include:
- Report one unit of 27447 per knee, since the code describes a single total knee arthroplasty
- Same-session bilateral cases use modifier 50, not two separate units
- Staged bilateral cases within the global period use modifier 58 on the second knee
- Confirm the current Medically Unlikely Edit value through CMS, since the table updates quarterly
Inpatient vs. Outpatient vs. ASC — The Two-Midnight Rule and Site-of-Service Medical Necessity
CPT code 27447 can be performed in inpatient, hospital outpatient, or ambulatory surgery center settings. CMS removed it from the Inpatient-Only list in 2018 and added it to the ASC Covered Procedures List in 2020.
The site-of-service rules are:
- The two-midnight rule governs inpatient admission, which requires an expectation that care crosses two midnights
- The surgeon is the final arbiter of the appropriate setting, documented before surgery
- An uncomplicated outpatient case discharged within 24 hours but billed as inpatient creates recoupment exposure
- The record must justify the chosen setting based on the patient’s clinical characteristics
Implant Charge Capture and Pass-Through Device Billing in Facility vs. ASC Settings
Implant and device charges are captured on the facility claim, not the surgeon professional claim for CPT code 27447. The setting determines how the device cost is reimbursed.
The implant billing rules are:
- The surgeon professional fee for 27447 does not include the implant cost
- Facility settings capture the implant charge through the facility payment system for the setting
- Pass-through device billing follows the OPPS or ASC policy for the specific device
- The facility record must document the implant manufacturer, model, and lot for charge capture
Prior Authorization Specificity Rules — Why a 27447 Auth Does Not Cover 27134
Prior authorization for CPT code 27447 covers only the primary total knee arthroplasty, not a revision. A revision total knee arthroplasty is a different code with its own authorization.
The authorization specificity rules are:
- Authorization for 27447 does not extend to revision code 27134
- A revision total knee arthroplasty requires a separate, code-specific authorization
- The authorized code, laterality, and site of service must match the claim exactly
- A mismatch between the authorized code and the billed code triggers an administrative denial
90-Day Global Period and Related E/M Billing Restrictions
CPT code 27447 carries a 90-day global period that includes routine post-operative care. Related evaluation and management visits during that window are not separately payable.
The global-period rules are:
- Routine post-operative visits within 90 days are included in the 27447 payment
- A related return to the operating room during the global period uses modifier 78
- An unrelated procedure during the global period uses modifier 79
- A staged or planned procedure during the global period uses modifier 58
Top Reasons For Denials Specific To 27447 & Quick Remedies
- Site-of-Service Mismatch: Prevent by documenting the two-midnight expectation before an inpatient admission, and billing uncomplicated same-day cases as outpatient.
- Missing or Wrong-Code Prior Authorization: Prevent by obtaining authorization specific to CPT code 27447 and the correct laterality, and never applying it to revision code 27134.
- Insufficient Conservative-Treatment-Failure Documentation: Prevent by including the full conservative trial and weight-bearing radiographs with the authorization request.
- Separately Billing Bundled Navigation, Robotics, or Scope: Prevent by removing bundled lines such as 20985, 0054T, 0055T, and same-session diagnostic arthroscopy.