
Ambulatory Surgery Centers (ASCs) are transforming outpatient healthcare, with billing complexity increasing as well. Today, more than 6,300 Medicare-certified ASCs treat approximately 3.4 million fee-for-service beneficiaries annually. Outpatient settings perform over 80% of the total surgeries. The U.S. ASC market exceeds $50 billion, with nearly 18,000 operating rooms nationwide, with 95% of centers operating as for-profit organizations.
Medicare payments to ASCs have surpassed $6 billion in recent years, as procedure volume has been rising. This is because CMS continues to expand the Covered Procedures List, resulting in more acuity cases being transferred to the ASC setting.
In a payment system driven by strict CPT coding, NCCI edits, and ASC-specific reimbursement rules, even small inaccuracies translate into significant financial loss. This ASC billing guide will help you understand the ASC billing process, commonly used codes, documentation requirements, challenges, and best practices for ASC billing.
What Is ASC Billing, And How Does It Differ From Hospital Billing?
An Ambulatory Surgery Center (ASC) is a licensed, Medicare-certified facility that provides same-day surgical care without requiring an overnight stay. To operate and receive reimbursement, ASCs must comply with the Conditions for Coverage established by the Centers for Medicare & Medicaid Services.
ASC billing refers specifically to the facility component of outpatient procedures. This includes operating room use, nursing services, supplies, and implants. The surgeon and other providers bill their professional services separately under the Medicare Physician Fee Schedule. This split billing structure is what fundamentally differentiates ASC billing from both hospital outpatient departments (HOPDs) and physician billing. This separation is a core concept that top ASC billing providers follow when structuring facility versus professional claims.
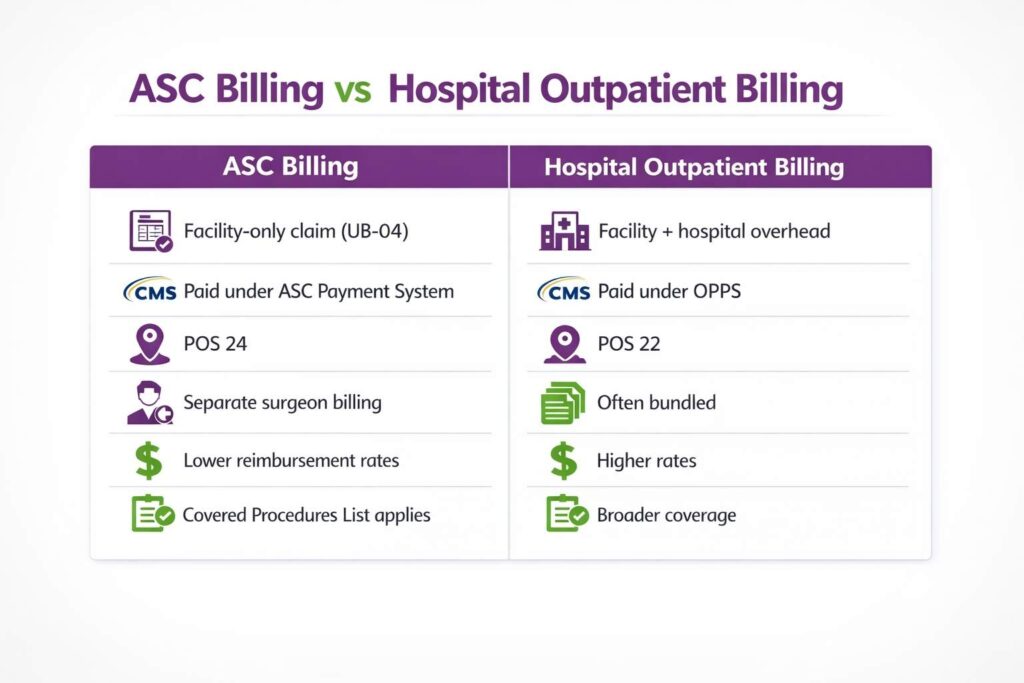
ASC vs HOPD vs Physician Billing
| Component | ASC | HOPD | Physician |
|---|---|---|---|
| Claim Form | CMS-1500 | UB-04 | CMS-1500 |
| Payment System | ASC Payment Groups | APCs | MPFS |
| Place of Service Code | 24 | 22 | Varies |
| Required Medicare Modifier | -SG | N/A | N/A |
| Prior Authorization (Medicare) | Generally not required | Generally not required | Generally not required |
| Reimbursement Rate | Lower than HOPD | Higher than ASC | Separate fee schedule |
Site-of-service decisions directly impact reimbursement: shifting a procedure between ASC and HOPD can materially change payment rates, making accurate classification critical for both compliance and revenue optimization.
What are the Common ASC Procedures?
Ambulatory Surgery Centers (ASCs) perform low-risk outpatient procedures that do not require an overnight hospital stay. Each of these procedures is mapped to standardized ASC CPT codes, which determine how services are grouped for reimbursement. Below are the most common services performed in ASCs:
- Gastroenterology procedures: Colonoscopies and upper endoscopies are commonly performed under the ASC Covered Procedures List with CPT coding.
- Orthopedic surgeries: Arthroscopy and minimally invasive joint repairs qualify for ASC payment groups.
- Ophthalmology procedures: Cataract removal and related eye surgeries are among the highest-volume ASC services.
- Pain management procedures: Epidural steroid injections and nerve blocks have payer coverage as ASC procedures.
- ENT surgeries: Sinus surgery and other otolaryngology procedures are suited for outpatient settings and have ASC payment classifications.
- Urology procedures: Cystoscopy and related minimally invasive interventions are commonly approved under ASC reimbursement policies.
These specialties also align with high-volume CPT groupings under the ASC payment system defined by the Centers for Medicare & Medicaid Services, making them key drivers of ASC reimbursement volume and procedure mix.
What Are CY 2026 CMS Payment Updates And How Do They Impact Revenue?
The CY 2026 ASC payment updates from the CMS directly impact reimbursement, compliance exposure, and long-term revenue strategy for Ambulatory Surgery Centers (ASCs), especially under ASC billing rules tied to the ASC Covered Procedures List and ASC Quality Reporting Program (ASCQR).
Key CY 2026 Conversion Factor Change
For CY 2026, the ASC conversion factor is set at:
- $56.322 for ASCQR-compliant ASCs
- $55.224 for non-compliant ASCs
This $1.098 differential per case may appear small, but at the ASC volume scale, it compounds into substantial annual revenue loss. The update is based on a 2.6% hospital market basket adjustment and a wage index neutrality factor, applied to the CY 2025 base rate of $54.895.
ASCQR Compliance Impact
Non-compliance with the ASC Quality Reporting Program results in a 2% payment reduction, not just administrative penalties. This reduction applies across all eligible claims and can translate into six-figure revenue losses annually for high-volume ASCs.
What CY 2026 Policy Updates Affect Billing?
- Measures removed: COVID-19 Healthcare Personnel vaccination coverage measure removed starting CY 2026 payment determination cycle.
- Proposed quality reporting changes: The 9-item post-operative patient survey was not finalized, reflecting regulatory pushback on reporting burden.
- Non-opioid pain management expansion: Separate payment continues for drugs such as Omidria (J1097) and Dextenza (J1096) under provisions of the Consolidated Appropriations Act of 2023 through December 31, 2027.
What is ASC Covered Procedures List?
Only procedures approved under the ASC Covered Procedures List are reimbursable in Ambulatory Surgery Centers. Verifying eligibility before billing is critical to prevent avoidable claim denials and compliance violations under rules set by the Centers for Medicare & Medicaid Services.
The Covered Procedures List is updated annually through the ASC payment system final rule and further refined through quarterly addenda (January, April, July, October). These updates directly impact what ASCs can legally bill and must be continuously reflected in billing software and charge capture workflows.
When a non-listed procedure is performed in an ASC, the claim is typically denied outright. In some cases, the facility may have limited options such as patient self-pay billing, but this introduces financial risk, payer disputes, and potential compliance exposure if medical necessity or site-of-service requirements are not met.
Pre-Scheduling Eligibility Checks Vs. Pre-Billing Checks
A key distinction in high-performing ASC billing workflows is pre-scheduling eligibility checks vs. pre-billing checks. Pre-scheduling validation ensures the procedure is ASC-eligible before booking, while pre-billing scrubbing only identifies issues after the service has already been performed. Eliminating errors at the scheduling stage is what prevents downstream denials entirely.
Why ASC Medical Billing Is Different: Key Components and Challenges
Understanding what makes ASC medical billing different is essential for ASCs to maximize reimbursements. Unlike standard hospital billing, ASC billing focuses on the facility component of outpatient procedures. This requires strict adherence to specialized coding and reimbursement policies for ASCs. Following ASC medical billing guidelines ensures compliance with CMS regulations for ambulatory surgery centers.
- Separate Facility vs. Professional Billing
ASC claims cover only the facility portion, while surgeons bill their professional services separately. Proper coordination helps to prevent coding errors and delayed payments. - ASC Payment System Rules
Reimbursement follows the CMS ASC payment methodology, assigning procedures to payment groups with predetermined rates. Misclassification can cause revenue loss. - Compliance with Covered Procedures List
Only procedures approved under the CMS ASC Covered Procedures List are reimbursable. Verifying eligibility before billing is critical to avoid denials. - Complex Modifiers and Bundling Guidelines
Correct use of CPT/HCPCS modifiers and adherence to NCCI edits ensure that bundled procedures are billed accurately. - High Audit and Regulatory Compliance
Documentation must support medical necessity, device use, and implant billing. Compliance with federal, state, and payer-specific rules reduces the risk of audits.
What is the Step-by-Step Process for ASC Billing?
The ASC billing process follows a step-by-step workflow to ensure that all facility charges for outpatient procedures are properly documented, coded, and submitted. Each step is critical for compliance, revenue optimization, and minimizing claim denials.
The ASC billing process is a structured workflow that ensures facility charges for outpatient procedures are accurately captured, coded, and reimbursed under the rules defined by the Centers for Medicare & Medicaid Services. Each step directly impacts claim acceptance, revenue cycle efficiency, and compliance with ASC-specific billing requirements.

Step 1: Patient Registration and Insurance Verification
The process begins with patient registration and full demographic capture, including insurance details, policy validation, and eligibility verification. This step confirms whether the patient’s plan covers the scheduled procedure under ASC billing rules and identifies any prior authorization requirements before the patient enters the operating schedule.
A critical escalation point in modern ASC billing is Medicare Advantage (MA) plans. Although they are part of the Medicare ecosystem, MA plans follow commercial payer rules, not traditional Medicare ASC payment group logic. For billing purposes, each MA plan must be treated as a commercial insurer, meaning prior authorization, medical necessity criteria, and negotiated fee schedules must be verified individually before scheduling.
In addition, ASCs must confirm that the Place of Service (POS) code 24 is correctly linked to the facility’s National Provider Identifier (NPI) within the payer’s system. If POS 24 is not properly mapped before the first claim submission, even correctly coded claims can be rejected or suspended due to system-level configuration mismatches.
At this stage, eligibility verification should also include confirmation of:
- Active coverage status on the date of service
- Network participation of the ASC facility
- Procedure-specific authorization requirements
- Member cost-sharing obligations (deductibles, coinsurance, copays)
Failing to complete these checks at registration leads to downstream denial risk that cannot be corrected through coding alone, making this step the highest-impact control point in the ASC billing workflow.
Step 2: Prior Authorization
Prior authorization is a separate and critical checkpoint in ASC billing, distinct from eligibility verification. Under ASC billing rules defined by the Centers for Medicare & Medicaid Services, traditional Medicare generally does not require prior authorization for most ASC-covered procedures. However, commercial payers and Medicare Advantage (MA) plans almost always do, and they apply their own medical necessity criteria and documentation standards.
A key complexity in ASC billing is multi-level authorization risk. Many procedures require more than one approval layer:
- The surgical procedure itself
- Implanted devices or biologics
- Post-operative services, such as therapy or injections
Missing even one authorization component can result in a full claim denial, not a partial payment reduction. This makes authorization mapping a revenue-critical step, not an administrative formality.
Practical Example
Suppose a patient’s GI plan requires pre-approval for non-emergency colonoscopies. The ASC front desk should upload the colonoscopy order and patient records to the insurer’s portal before the procedure date. If the insurer denies coverage, the surgery is postponed or billed as a self-pay procedure. Conversely, a properly documented approval means no last-minute denials. See Transcure’s GI Prior Authorization Expansion alert for details on evolving GI pre-auth rules.
Step 3: Procedure Documentation and Coding
After the procedure, all facility-related services such as operating room use, supplies, implants, and anesthesia are carefully documented. This information is then converted into CPT/HCPCS codes, revenue codes, and modifiers in accordance with CMS ASC payment rules and NCCI edits. Modern ambulatory surgery EMR systems integrate operative documentation, coding logic, and charge capture into a single structured workflow. Accurate documentation at this stage directly determines claim accuracy and reimbursement integrity under the ASC billing framework defined by the Centers for Medicare & Medicaid Services.
Op note specificity drives code specificity. Vague or incomplete operative documentation forces coders into generic, lower-paying codes or triggers payer edits. Precise clinical language is what protects reimbursement.
For example, “minor neurolysis” may default to CPT 64721, while “subcutaneous ulnar nerve transposition” supports CPT 64718. The difference is not semantic; rather, it directly impacts RVU valuation, payer grouping logic, and claim acceptance outcomes.
Practical Example
After a knee arthroscopy, the surgeon’s note indicates a meniscectomy. An ASC coder using an integrated EHR will assign CPT 29880 (arthroscopy with meniscectomy) and attach the appropriate ICD-10 code for the diagnosis. The EHR then auto-includes charges for anesthesia and any implants used, reducing manual entry errors. All supporting details (patient history, consent, implants listed) are kept in the chart to substantiate the billing.
See our ASC Coding Guide for procedure-specific code and modifier references by specialty.
Step 4: Claim Preparation and Scrubbing
Claims are prepared using documented services and formatted for submission on the CMS-1500 (HCFA 1500) form with Place of Service code “24” (ASC). Unlike hospital outpatient billing (UB-04/APC), ASC facility claims are submitted on CMS-1500, alongside physician claims where applicable. All claims must also comply with NCCI (National Correct Coding Initiative) edits to ensure correct bundling and prevent unbundling errors under rules enforced by the Centers for Medicare & Medicaid Services.
A critical operational requirement is that NCCI edits must be applied before submission, not after denial. Real-time scrubbing is now the industry standard. Batch scrubbing after submission means the claim has already been filed incorrectly, increasing denial probability and rework costs while delaying reimbursement.
In addition to federal edits, payer-specific edit layers apply on top of CMS rules. Commercial insurers often maintain their own bundling logic, modifier requirements, and medical necessity edits that differ from Medicare’s NCCI framework. This means a claim that is compliant under CMS rules can still be denied if payer-specific logic is not applied during scrubbing.
Effective ASC billing systems, therefore, operate a dual-layer scrubbing model:
- CMS NCCI compliance layer (federal baseline)
- Payer-specific rules engine (commercial and MA plan variation)
Failure to integrate both layers results in predictable denial patterns, especially for high-volume procedures where modifier use, device billing, and bilateral procedures are frequently audited.
Step 5: Claim Submission
Once verified, claims are submitted to Medicare or commercial payers. ASC billing focuses on facility charges only, submitted under the ASC’s National Provider Identifier (NPI), while the surgeon submits professional services separately under their own NPI. This separation of billing is a core requirement of the ASC billing structure governed by the Centers for Medicare & Medicaid Services.
For Medicare claims, the “-SG” modifier is required on the ASC facility claim line to identify services performed in an Ambulatory Surgery Center. Missing or incorrect use of this modifier is a common trigger for automatic rejections or payment delays.
For Medicare Advantage (MA) plans, the same billing structure applies. “-SG” modifier and POS 24 are still required, but reimbursement is not based on the Medicare ASC payment group methodology. Instead, MA plans process payment using their contracted commercial fee schedules, which may significantly differ from standard CMS rates and require plan-specific allowance verification during contract setup and posting.
Proper submission, therefore, requires dual alignment:
- Structural compliance with CMS billing rules (modifiers, POS, NPI separation)
- Financial compliance with payer-specific reimbursement contracts
Timely and correctly structured submission ensures faster cash flow and reduces rework caused by avoidable front-end configuration errors.
Step 6: Claim Tracking, Denial Management, and Appeals
Submitted claims are continuously monitored for adjudication status, denial codes, and payment outcomes. When denials occur, they must be analyzed, corrected, and appealed based on payer-specific requirements and documentation evidence. Effective denial workflows are a core component of ASC billing performance under rules set by the Centers for Medicare & Medicaid Services.
Practical Example
If a colonoscopy claim is denied due to “no pre-authorization on file,” the billing staff should immediately contact the physician’s office to verify whether pre-authorization was obtained. If it was, submit a reconsideration with the auth approval attached. If not, quickly appeal with clinical justification or arrange for patient self-pay. Over time, tracking these outcomes reduces repeated errors.
Step 7: Payment Posting and Underpayment Detection
Once payments are received, they are posted to the patient account and reconciled against expected reimbursement. A key requirement is an Explanation of Benefits (EOB) review against contracted rates. Underpayments are as common as denials, and payers do not self-correct reimbursement discrepancies.
Payment posting also requires monitoring for recoupments linked to bundling or 72-hour rule violations under NCCI logic, where payers retrospectively adjust payments if services are incorrectly separated or improperly billed across claim lines. These adjustments must be flagged and validated against documentation and coding logic before acceptance.
For Medicare claims, reconciliation must also include validation against ASC payment group rates using CMS quarterly Addenda (AA/BB updates) issued by the Centers for Medicare & Medicaid Services. These updates adjust reimbursement values throughout the year, and outdated fee schedules can result in systematic underpayment if not aligned with current rates.
What are NCCI Edits, MUEs, and the 72-Hour Bundling Rule?
ASC billing compliance is driven by coding rules enforced by the CMS. Among the most important are NCCI edits, Medically Unlikely Edits (MUEs), and the 72-hour pre-operative bundling rule. These rules directly determine whether a claim is payable, bundled, or denied.
What are NCCI Edits and Why do they Matter for ASCs?
The National Correct Coding Initiative (NCCI) is a CMS editing system that identifies code pairs that cannot be billed together unless a modifier supports a distinct procedural service.
NCCI logic is based on Column 1 / Column 2 relationships. Column 2 codes are considered integral to Column 1 and are bundled into it. Billing both without a valid modifier results in automatic denial, even if the documentation is clinically accurate.
NCCI edits are updated quarterly. If an ASC billing system is not aligned with the latest update cycle, claims are submitted using outdated bundling logic, which leads to predictable denials at scale.
Medically Unlikely Edits (MUEs)
MUEs define the maximum number of units of service that are clinically reasonable for a single patient on a single date of service or claim line.
Key operational concepts include:
- MUE Adjudication Indicator (MAI 1): adjudicated per date of service
- MAI 3: adjudicated per claim line and is especially important for complex surgical reporting
MAI 3 edits are critical in ASC billing because they frequently affect bilateral procedures and multi-site surgeries.
Some CPT codes carry an MUE of 1 unit per claim, meaning both sides of a bilateral procedure cannot be billed as separate units unless correctly structured with modifiers. Failure to align units with MUE thresholds results in automatic denials, even when documentation supports medical necessity.
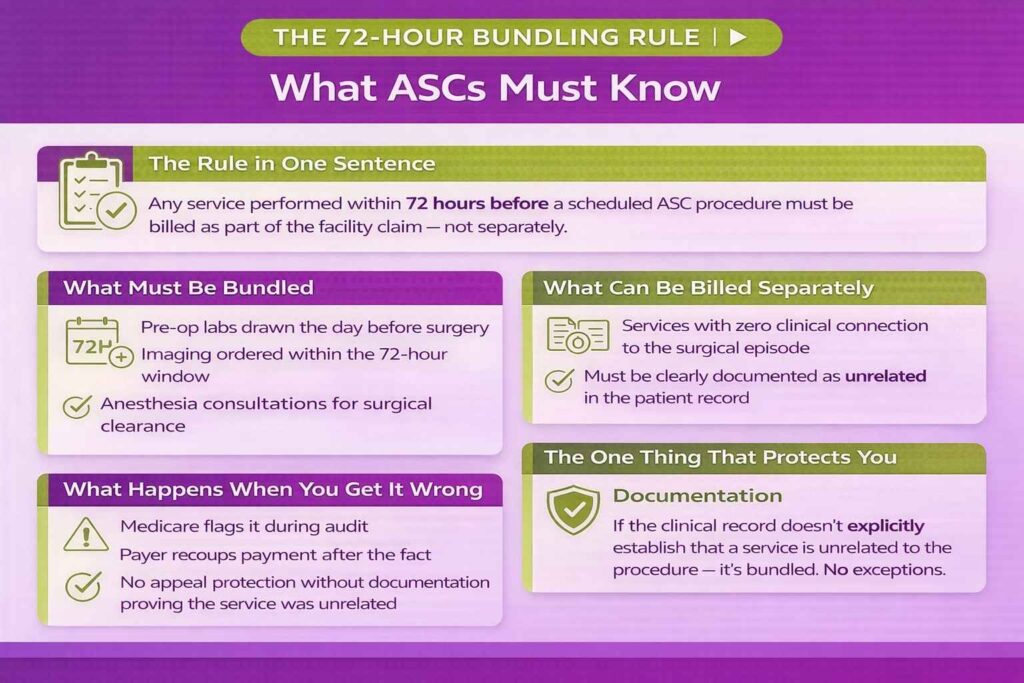
The 72-Hour Pre-Operative Bundling Rule
Any service related to a scheduled ASC procedure and performed within 72 hours prior to surgery must be bundled into the ASC facility claim. It cannot be billed separately. “Related services” include diagnostic, therapeutic, or preparatory interventions directly tied to the surgical episode.
Common violations include pre-operative labs drawn the day before surgery, imaging within the 72-hour window, and anesthesia consultations performed as part of surgical clearance. These are frequently flagged during Medicare audits and often result in post-payment recoupments when billed separately. Unrelated services may be excluded from bundling, but only if the clinical documentation clearly establishes no connection to the surgical episode.
ASC Implant and Device Billing
Most standard surgical supplies and devices are packaged into the ASC facility payment. Attempting to bill them separately typically results in denial.
Separately billable implants require all of the following:
- A device-specific HCPCS code (not generic codes such as L8699)
- Valid invoice documentation attached to the claim record
- Proper linkage to the primary procedure on the same claim
Device specificity has a direct revenue impact. Using a generic HCPCS code instead of a CMS passthrough-listed device code can result in thousands of dollars in lost reimbursement per case.
Commercial payer contracts often differ from Medicare rules. Many allow implant carve-outs, but only if explicitly negotiated. Without contract language, payers default to CMS-style bundling logic.
Operationally, ASCs should maintain a case-level implant log capturing manufacturer, model, and cost data, ensure invoices are attached for audit readiness, and reconcile HCPCS assignments quarterly against CMS passthrough updates.
What Are The Causes For ASC Denials and How Should You Manage Them?
Denial management in ASC billing is a revenue protection function, not a back-office correction process. It directly impacts cash flow, compliance risk, and performance under reimbursement rules set by the Centers for Medicare & Medicaid Services. Most ASC revenue leakage occurs after claims are submitted, making denial prevention and structured appeal workflows essential.
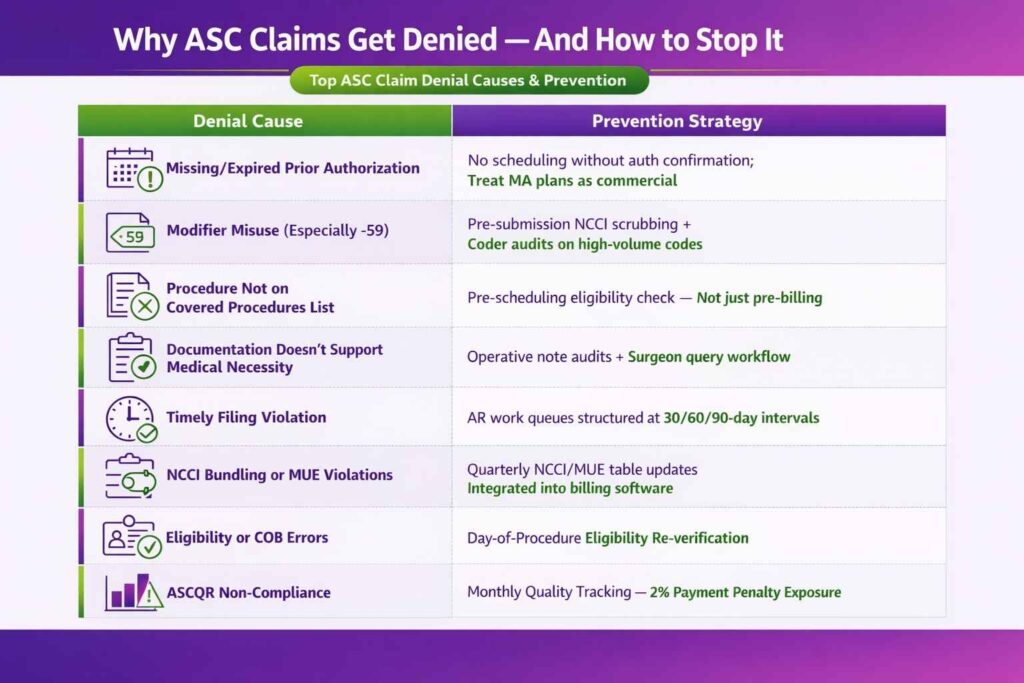
Top Denial Root Causes and Prevention
| Root Cause | Prevention |
|---|---|
| Missing or expired prior authorization | No scheduling without authorization confirmation; treat Medicare Advantage plans as commercial payers |
| Modifier misuse (especially -59) | Pre-submission NCCI scrubbing; coder audits on high-volume procedures |
| Procedure not on Covered List | Pre-scheduling eligibility check, not just pre-billing validation |
| Documentation does not support medical necessity | Operative note quality audits and surgeon query workflow for vague documentation |
| Timely filing violation | AR work queues structured at 30/60/90-day intervals with payer-specific deadlines |
| NCCI bundling or MUE violations | Quarterly NCCI and MUE table updates integrated into billing software |
| Eligibility or coordination of benefits errors | Day-of-procedure eligibility re-verification |
| ASCQR non-compliance | Monthly quality reporting tracking tied to the 2% penalty exposure |
Denial Appeal Workflow
Denial resolution follows a structured escalation process that begins immediately after remittance posting.
- Receipt and categorization
Each denial is logged by reason code, payer, procedure type, and service line to identify systemic patterns rather than isolated errors. - Root cause identification
Denials are classified into coding errors, authorization failures, documentation gaps, or payer processing errors. - Documentation pull
Supporting records are assembled, including operative notes, authorization approvals, medical necessity letters, and implant invoices where applicable. - Appeal submission
Medicare appeals follow strict timelines, including redetermination requests within 120 days of the remittance date. Commercial payer timelines vary by contract and must be tracked individually. - Escalation path
Medicare appeals escalate through redetermination, reconsideration, and Administrative Law Judge (ALJ) hearings. Commercial appeals typically move from internal review to external independent review.
How Can ASCs Ensure Accurate and Compliant ASC Billing?
Ensuring accurate billing in Ambulatory Surgery Centers (ASCs) requires a mix of regulatory knowledge, coding accuracy, and payer rule compliance. The following ASC billing guidelines help ASCs maintain compliance and reduce audit risk:
1. Core Regulatory Framework
The Anti-Kickback Statute and Stark Law govern physician ownership, referrals, and financial relationships in ASCs. Compliance requires structured ownership arrangements, documented fair market value compensation, and strict separation between referral volume and financial incentives.
2. Internal Audit Controls
Internal audits should target high-volume procedures, modifier accuracy (especially -59), and payer-specific billing rules. These are the most common sources of systematic leakage and pre-denial errors in ASC billing workflows.
3. False Claims Act Exposure
False Claims Act risk increases with repeated unbundling patterns and improper modifier use. Modifier -59 misuse is a known audit trigger, particularly when applied inconsistently across high-frequency procedures, signaling potential upcoding or improper separation of bundled services.
4. AI-Assisted Coding Compliance
AI coding tools must include documented human coder attestation for every claim. AI-only coding without clinical or coding review creates audit vulnerability, as payers increasingly flag automated patterns lacking human validation.
5. Audit Cadence Strategy
Run quarterly internal audits focused on the top 10 procedure codes by volume to catch systemic errors early. Supplement this with an annual third-party audit covering high-revenue specialties to validate compliance, reduce cumulative risk, and strengthen payer defense positioning.
ASC Billing by Payer Type
ASC billing rules vary significantly by payer. While the facility workflow remains consistent, reimbursement logic, authorization requirements, and coding enforcement differ across Medicare, Medicare Advantage, commercial insurers, Medicaid, and self-pay patients. These differences are defined and regulated in part by the Centers for Medicare & Medicaid Services.
Traditional Medicare
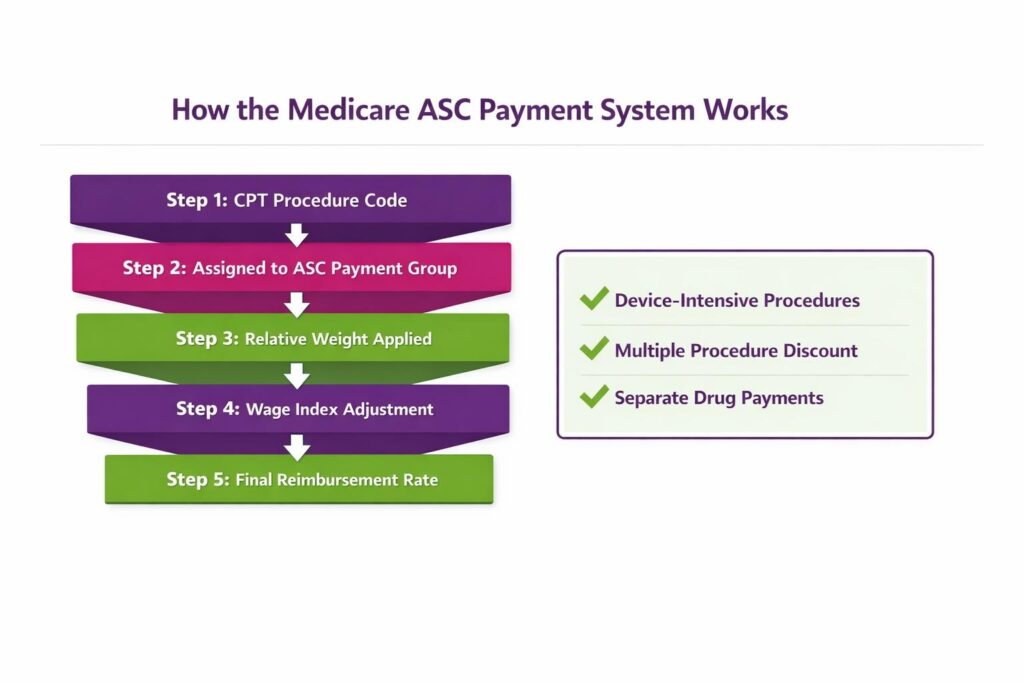
Traditional Medicare reimburses ASCs under the ASC payment system using Ambulatory Payment Classification (APC)-based payment groups, where procedures are assigned to fixed facility fee categories.
Key structural elements include:
- 9 ASC payment groups determine facility reimbursement levels
- Payments are adjusted by the local wage index
- Claims are submitted as “assigned” claims under Medicare rules
- Facility fees do not require Advance Beneficiary Notices (ABNs)
For CY 2026, full reimbursement under the updated conversion factor of $56.322 is contingent on ASCQR compliance, linking quality reporting directly to payment integrity.
Medicare Advantage (Net New)
Medicare Advantage (MA) plans are not bound by traditional Medicare payment logic and are contractually permitted to deviate significantly from CMS ASC rules.
Key operational differences:
- Prior authorization is commonly required, even when traditional Medicare does not require it
- Fee schedules are based on plan-specific contracts, not CMS payment groups
- Commercial-style bundling rules often apply
MA plans must never be treated as traditional Medicare in billing workflows. Each plan’s ASC policy should be verified at credentialing and re-verified annually.
Operationally, “-SG” modifier and POS 24 are still required, but reimbursement is calculated strictly under the MA plan’s contracted terms, not CMS APC or ASC payment group methodology.
Commercial Insurance
Commercial payers require strict contract adherence and prior authorization validation before services are rendered. Each payer applies its own coding edits, bundling logic, and medical necessity criteria.
A key revenue risk in commercial ASC billing is underpayment, not just denial. Every paid claim must be reviewed against contracted rates through Explanation of Benefits (EOB) reconciliation.
Commercial contracting also represents a direct revenue lever: implant carve-out language must be explicitly negotiated, or payers will default to bundling implant costs into the facility fee.
Medicaid
Medicaid billing rules vary by state, with significant differences in reimbursement models and prior authorization requirements.
Some states use Enhanced Ambulatory Patient Groups (EAPG) instead of Medicare-aligned ASC payment structures. ASCs must verify state-specific methodologies to ensure correct coding and reimbursement alignment.
Self-Pay and Out-of-Network
Self-pay and out-of-network billing require transparent financial communication and strict compliance with federal requirements.
Key requirements include:
- Good-faith estimates under the No Surprises Act before scheduled procedures
- Clear itemized cost breakdowns for patients
- Structured payment plans to support collection
Out-of-network claims may use Usual, Customary, and Reasonable (UCR) rate strategies, but reimbursement outcomes depend heavily on payer-specific arbitration and patient liability rules.
What is ASCQR and Its 2% Reimbursement?
The ASC Quality Reporting Program (ASCQR) is a pay-for-reporting framework established by the Centers for Medicare & Medicaid Services. Failure to meet ASCQR requirements reduces the annual payment update by 2 percentage points, directly impacting reimbursement across all Medicare ASC claims.
In CY 2026, this gap becomes financially material. ASCQR-compliant ASCs receive a conversion factor of $56.322, while non-compliant ASCs receive $55.224, creating a $1.098 per-unit differential that compounds significantly across high-volume surgical cases.
For CY 2026 reporting, several measures have been updated:
- The COVID-19 Healthcare Personnel vaccination coverage measure has been removed
- The proposed 9-item post-operative patient survey was not finalized
These changes reflect ongoing recalibration of quality reporting burden versus clinical utility within the ASC payment system.
The broader trajectory is toward value-based reimbursement. The Centers for Medicare & Medicaid Services 2025 Report to Congress outlines early steps toward ASC value-based purchasing (VBP), signaling a shift from pay-for-reporting models toward pay-for-performance frameworks in future rulemaking.
ASC operators should treat ASCQR as a revenue protection system, not a compliance checklist. Core operational controls include maintaining a structured ASCQR submission calendar, tracking measure updates in each annual final rule, and auditing reporting status quarterly rather than at year-end to avoid avoidable payment penalties.
Why Should ASCs Outsource Their ASC Billing?
Ambulatory Surgery Centers (ASCs) face complex billing challenges. These include strict compliance requirements, payer-specific rules, and frequent claim denials. Many ASC billing companies specialize in end-to-end revenue cycle management, helping ASCs stay compliant with evolving CMS billing rules. Outsourcing ASC billing has several benefits for ASC, such as:
1. Expertise in ASC-Specific Coding and Compliance
ASCs get access to professionals trained in ICD-10, CPT, HCPCS, and ASC-specific modifiers. Their knowledge of CMS guidelines, commercial payer rules, and state-specific regulations ensures accurate claims, which reduces the risk of denials.
2. Improved Revenue Cycle Management
Outsourced billing providers streamline claim submission, follow-ups, and denial management. With specialized tools and analytics, they can identify missed charges and reduce accounts receivable days, leading to higher revenue collection.
3. Reduced Administrative Burden
ASC billing is time-consuming and requires continuous updates on coding rules and payer policies. By outsourcing, ASC staff can focus on patient care, while experts handle ASC billing and coding.
4. Access to Advanced Technology
Many billing companies use AI-driven billing platforms and automation tools. Such tools minimize errors, track claims in real time, and ensure timely reporting. This reduces human errors and increases billing accuracy.
5. Scalability and Cost Efficiency
Outsourcing provides flexibility as ASCs grow or perform more procedures. Instead of hiring and training additional in-house staff, ASC operators can scale billing resources efficiently, at a lower cost.
Benefits of Outsourcing
Outsourcing ASC billing improves performance across both financial and operational dimensions. High-performing ASC billing services directly impact clean claim rates, denial reduction, and reimbursement accuracy by aligning everything in a single workflow.
- ASC-specific coding and compliance expertise ensures accurate use of CPT, HCPCS, and payer-specific billing rules unique to outpatient surgical settings.
- Stronger revenue cycle management (RCM) improves claim submission accuracy, accelerates follow-ups, and strengthens denial management workflows.
- Reduced administrative burden allows clinical and administrative staff to focus on patient scheduling, coordination, and throughput.
- AI-driven billing platforms and automation enhance claim scrubbing, eligibility checks, and denial prediction, reducing preventable errors.
- Scalability and cost efficiency enable ASCs to handle fluctuating surgical volumes without proportional increases in internal staffing costs.
How to Choose the Right ASC Billing Partner
Selecting an ASC billing partner requires evaluating both operational capability and financial alignment.
- ASC specialization and payer expertise: Ensure the vendor has demonstrated experience with ambulatory surgery centers, including multispecialty coding and payer-specific rules.
- Denial management strength: Look for structured appeal workflows, root-cause denial tracking, and documented recovery performance.
- Technology infrastructure: Prioritize platforms with integrated claim scrubbing, real-time eligibility verification, and reporting dashboards.
- Compliance and update management: The partner should proactively apply CMS updates, payer policy changes, and coding revisions without delays.
- Client support model: Evaluate responsiveness, dedicated account management, and escalation pathways for high-priority issues.
- Transparent KPI reporting: Monthly reporting should include clean claim rate, denial rate, A/R days, and appeal win rate to ensure accountability and performance visibility.
Pricing models should also align with operational goals. Percentage of collections aligns incentives with revenue outcomes, per-claim pricing offers predictability but may not encourage denial prevention, and flat-fee models work best for stable, high-volume ASCs with consistent surgical throughput.
Conclusion
ASC billing requires precise ICD-10, CPT, and HCPCS coding, accurate modifier usage, and strict compliance with CMS ASC payment rules and the Covered Procedures List. A structured ASC billing process reduces errors and improves clean claim rates. By outsourcing to ASC billing experts, ambulatory surgery centers can maximize reimbursements and maintain regulatory compliance.
FAQs
What Is ASC Billing?
ASC billing is the process of submitting facility claims for outpatient procedures performed in an Ambulatory Surgery Center. It includes reporting ASC CPT codes, HCPCS codes, ICD-10 codes, modifiers, and complying with payer-specific reimbursement rules.
How Do ASCs Manage Coding For Multi-Specialty Procedures?
ASCs use accurate CPT, ICD-10, and HCPCS codes with proper modifiers to bill multi-specialty procedures. Clear documentation of each provider’s service ensures compliance, reduces denials, and maximizes reimbursement.
How Do ASCs Handle Out-Of-Network Billing And Coding?
Out-of-network ASC billing requires verifying patient benefits, submitting claims with medical necessity, and communicating patient financial responsibility. Proper coding ensures faster reimbursement and compliance with payer rules.
How Do ASCs Get Paid By Medicare?
Medicare pays ASCs under the ASC payment system, assigning procedures to payment groups with predetermined rates based on Ambulatory Payment Classifications (APCs).
What are the Reasons for ASC Claim Denials?
Common reasons for ASC denials include incorrect modifiers, unbundling, lack of medical necessity documentation, coding errors, and failure to follow payer-specific rules.






